
Abstract
Background
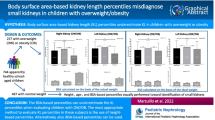
Obesity in the pediatric population is a severe public health problem and is associated with various comorbidities. Renal length is an important clinical parameter for the diagnosis and follow-up of renal diseases. The aim of this study was to determine the relationship between renal length (measured ultrasonographically) and body mass index (BMI) in obese children, and to develop nomograms for renal length according to BMI.
Methods
Renal ultrasound was performed in 368 children without renal disease. Each child’s age, gender, weight, height, and BMI (kg/m2) were recorded. The children were divided into three groups according to BMI percentiles: obese group: BMI ≥ 95th percentile; overweight group: BMI 85th–94th percentile; normal weight group: BMI 5th–84th percentile.
Results
Weight, height, BMI, and right and left renal length differed significantly between the three groups (p = 0.001). There were significant correlations between renal length with age, weight, height, and BMI. Measurement of renal length was independently associated with BMI, age, and height. BMI was used to create renal length nomograms for obese children, based on multiple regression analysis (R2 = 0.32 and p = 0.0001). Mean renal length was highest in the obese group (96.9 ± 13.4 mm) and lowest in the normal weight group (88.3 ± 12.9 mm).
Conclusions
Ultrasonographic measurement of the renal length according to BMI in children can be a useful method in evaluating these children. Smaller-than-normal kidneys can easily remain undiagnosed in obese and overweight children and this nomogram offers an additional method to evaluate the renal size in obese children.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Obesity is increasing dramatically worldwide, and is considered to be among the most serious public health issues both in the pediatric and adult populations. It was reported in the Turkish Nutrition and Health Research Report 2010 that obesity prevalence in 6–18-year-old children was 8.2% overall [1]. Alper et al. reported that the prevalence of childhood obesity in Turkey increased 11.6-fold between 1990 and 2015 [2]. Early childhood obesity has led to the emergence of such multiple serious obesity-related comorbidities as diabetes mellitus, hypertension, and obesity-related glomerulopathy. Each of these comorbidities can negatively affect renal function, with the most serious outcome being end-stage kidney disease (ESKD).
Renal length in children is an important clinical marker of renal development and abnormalities (such as atrophy, hypoplasia, and hypertrophy). Ultrasonography is commonly used to measure renal length because the technique is non-invasive, does not use radiation, is inexpensive, and is easy to perform [3]. Nomograms of normal renal length in healthy children were first published in 1977 by Tay et al. [4]. In most instances, age-specific nomograms are used to evaluate renal length in children [5]. In addition to age, renal length in children is affected by several other factors, including gender, height, weight, and ethnicity [6]. Recent studies on the development of nomograms for assessing renal length in children have highlighted the effects of age and height [7,8,9]. As such, the present study aimed to determine the relationship between renal length and BMI in obese children based on ultrasonography, and to subsequently develop nomograms for renal length according to BMI.
Methods
The study included children aged 5–18 years who presented to Başkent University, Dr. Turgut Noyan Training and Research Center, Pediatrics, Pediatric Endocrinology, and Pediatric Nephrology Departments, Adana, Turkey, for ultrasonography between January 2014 and March 2018. Ultrasonographic measurements of renal length were evaluated retrospectively. Each participant’s age, gender, weight, and height were obtained from their hospital files, and BMI (kg/m2) calculated. The children were divided into 3 groups according to the BMI percentiles listed in the Centers for Disease Control and Prevention (CDC) 2000 growth charts, as follows: obesity group: BMI ≥ 95th percentile; overweight group: BMI 85th–94th percentile; normal weight group: BMI 5th–84th percentile [10].
Children, whose renal ultrasonographic findings showed pathological disorders (cortical scarring, increased echogenicity, agenesis, dysplasia, cysts, pelvic dilation, ureteral duplication, or stones), vesicoureteral reflux, or neurogenic bladder, and/or those with a history of urological surgery, endocrine disorder, steroid use, and malignancy or other systemic illness, were excluded from the study. Measurement of renal length was performed with children in the lateral decubitus position; the renal length was considered the maximum longitudinal length of the kidney. Measurements were performed using an Antares 5 (Siemens Medical Solutions, Issaquah, WA) ultrasound device, and a 4–1 MHz convex or 9–4 MHz linear probe, according to each participant’s renal length. To standardize the sensitivity of the measurements and eliminate radiologist-related differences, all renal measurements were performed by the same radiologist who had 10 years of pediatric radiology experience. The study protocol was approved by the Başkent University Institutional Review Board and Ethics Committee.
Statistical analysis
Data were analyzed using IBM SPSS Statistics for Windows v.23.0 (IBM Corp., Armonk, NY). Categorical data are expressed as number and percentage, whereas continuous data are expressed as mean ± SD, median, and range. Categorical variables were compared using the chi-square test or Fisher’s exact test. To compare continuous variables between groups, their distribution was analyzed; one-way analysis of variance (ANOVA) was used to examine variables that were parametrically distributed and the Kruskal-Wallis test was used for variables that were not parametrically distributed. For pairwise comparisons between groups, normally distributed parameters were analyzed via post hoc analysis, whereas the Mann-Whitney U test was used for parameters that were not normally distributed. Multiple linear regression analysis was employed to identify factors affecting renal length. The level of statistical significance was set at p = 0.05.
Results
The mean age of the 222 female and 146 male children was 10.04 ± 3.30 years (range 5–18 years). Distribution of the 368 children was as follows: obese group n = 130; overweight group n = 98; normal weight group n = 140. Weight, height, BMI, right renal length, and left renal length differed significantly between all three groups (p = 0.001), whereas age (p = 0.089) and gender (p = 0.729) did not (Table 1). Renal length was highest in the obese group (96.9 ± 13.4 mm) and lowest in the normal group (88.3 ± 12.9 mm). There was not a significant difference in left or right renal length between all groups (p = 0.073); however, according to pairwise comparison of the groups, renal length differed significantly between the groups (obese-overweight: p = 0.005; obese-normal: p = 0.0001; overweight-normal: p < 0.05).
Correlations between renal length and anthropometric characteristics are shown in Table 2. There was a positive correlation between renal length, and weight and height.
Multiple linear regression analysis showed that renal length was independently associated with age (β = 0.22, p < 0.001), height (β = 0.47, p < 0.001), and BMI (β = 0.16, p < 0.001) in all participants (Table 3, Fig. 1). The results of the regression model showed that renal length could be estimated using the formula, renal length (mm) = 62.79 + (1.36 × BMI) (R2 = 0.32; p = 0.0001). Since there was no statistical difference between right and left renal length, it was formulated as a single renal length.

Renal length nomograms based on BMI created for the a obese group, b overweight group, and c normal weight group
Discussion
The present study aimed to determine the effect of obesity on renal length (measured ultrasonographically) in healthy children and to subsequently create an ideal renal nomogram. Renal length is of particular importance for the diagnosis, treatment, and follow-up of kidney disease. In patients with smaller-than-normal kidneys based on ultrasonography, renal scintigraphy, voiding cystography, or other more advanced and invasive imaging techniques are employed to determine its etiology. Small kidneys are known to be related to atrophy secondary to congenital hypoplastic and dysplastic kidneys, or vesicoureteral reflux. One of the most common causes of chronic kidney disease and ESKD in children is renal hypodysplasia [11]. Renal hypodysplasia can be associated with such long-term consequences as an increased risk of hypertension or the development of chronic kidney disease following a second renal insult in childhood or as an adult.
Organ development proportional to a child’s overall growth is directly related to the functioning of organs. Height and weight are significant factors used to assess the growth and development of children. It is well known that renal size is positively associated with age, height, and weight. Many studies have shown that height correlates best with renal length in children [12,13,14]. Renal length in our study increased along with age, height, weight, and BMI, and the strongest correlation was observed between renal length and height. Also, our results show that renal length was independently associated with age, height, and BMI.
Obesity affects renal morphology and function. Zuzuarregui et al. [13] studied 204 children and reported that renal size was greater in obese children than in those with normal weight. They also observed that obesity, height, and age were independent predictors of renal length, and as height was most strongly correlated with renal length, they created a nomogram for renal length based on height. Similarly, Soheilipour et al. [14], using linear regression analysis, observed that height and age were independent predictors of renal length in children. In this study, children were divided into 3 groups according to age (1–72 months, 6–12 years, and 12–19 years) and it was determined that renal length in obese children was greater than in children of the same age and height. Zuzuarregui et al. and Soheilipour et al. both used linear regression analysis to produce a nomogram for renal length based only on height [13, 14]. In our study, we found that age and height as well as BMI have a positive effect on renal length in accordance with the literature, and rather than basing our nomograms on height, we created renal length nomograms based on BMI.
Today, renal nomograms created without taking into account the steady increase in the prevalence of obesity continue to be used and there is a lack of nomograms specific to obese children. As such, there is a great need for obese children-specific renal length nomograms based on BMI. The present study used polynomial regression analysis to explore the correlation between BMI and renal length by calculating estimated renal length. The analysis results led us to a formula for estimating renal length according to BMI: renal length (mm) = 62.79 + (1.36 × BMI). In addition to the adverse effects of obesity on the kidneys, the creation of such nomograms will facilitate easier detection of renal abnormalities (hypoplasia, atrophy, and dysplasia) that are not associated with an increase in BMI and thus supposed to be normal. To the best of our knowledge, the present study is the first to produce an obese children-specific renal length nomogram based on BMI.
There are several limitations of this study that should be mentioned. In this study, we evaluated the size of kidney with ultrasonographic length measurement. We think that if we evaluated the size of kidney with renal volume instead of renal length, we may have found a stronger relationship between BMI and renal volume. A new prospective study to investigate the relationship between renal volume and anthropometric values could be planned in obese children. In addition, this study was not prospective and therefore does not provide evidence that using the obese or non-obese child’s BMI or height as a means to assess the status of renal size is superior since a “gold standard” for true distribution of normal dimensions in these populations is lacking.
In conclusion, ultrasonographic measurement of the renal length according to BMI in children can be a useful method in evaluating these children. Smaller-than-normal kidneys can easily remain undiagnosed in obese and overweight children and this nomogram offers an additional method to evaluate the renal size in obese children. Whereas earlier studies have observed nephromegaly in obese children, clinicians must be aware that hypoplastic and dysplastic kidneys are not always detected [13, 14]. Children with these renal conditions must be monitored closely, as they are at risk of chronic kidney disease. Advanced imaging technologies must be used in all children with smaller-than-normal kidneys.
References
(2014) Ministry of Health. Turkey Nutrition and Health Research Report 2010: Assessment of Nutritional Status and Habits [article InTurkish]
Alper Z, Ercan İ, Uncu Y (2018) A meta-analysis and an evaluation of trends in obesity prevalence among children and adolescents in Turkey: 1990 through 2015. J Clin Res Pediatr Endocrinol 10:59–67
Weisenbach J, Horvath M, Jeges S, Adamovich K, Huszar T (2001) Normal percentiles of kidney size in children as measured by ultrasonography. Orv Hetil 142:71–74
Tay JS, Vellayappan K, Tan LKA (1977) Pediatric ultrasonography: the accuracy of the ultrasound scan in the estimation of renal size in children. J Singapore Pediatr Soc 19:234–237
Rosenbaum DM, Korngold E, Teele RL (1984) Sonographic assessment of renal length in normal children. AJR Am J Roentgenol 142:467–469
Chen JJ, Pugach J, Patel M, Luisiri A, Steinhardt GF (2002) The renal length nomogram: a multivariable approach. J Urol 168:2149–2152
Kim JH, Kim MJ, Lim SH, Kim J, Lee MJ (2013) Length and volume of morphologically normal kidneys in Korean children: ultrasound measurement and estimation using body size. Korean J Radiol 14:677–682
Otiv A, Mehta K, Ali U, Nadkarni M (2012) Sonographic measurement of renal size in normal Indian children. Indian Pediatr 49:533–536
Kim BW, Song MK, Chung S, Kim KS (2012) Evaluation of kidney size in children: a pilot study of renal length as a surrogate of organ growth. Korean J Pediatr 55:54–57
Centers for Disease Control and Prevention/National Center for Health Statistics (CDC/NCHS). CDC growth charts: United States, 2000. http://www.cdc.gov/growthcharts
Seikaly MG, Ho PL, Emmett L, Fine RN, Tejani A (2003) Chronic renal insufficiency in children: the 2001 Annual Report of the NAPRTCS. Pediatr Nephrol 18:796–804
Ece A, Gözü A, Bükte Y, Tutanç M, Kocamaz H (2007) The effect of malnutrition on kidney size in children. Pediatr Nephrol 22:857–863
Pantoja Zuzuarregui JR, Mallios R, Murphy J (2009) The effect of obesity on kidney length in a healthy pediatric population. Pediatr Nephrol 24:2023–2027
Soheilipour F, Jesmi F, Rahimzadeh N, Pishgahroudsari M, Almassinokian F, Mazaherinezhad A (2016) Configuring a better estimation of kidney size in obese children and adolescents. Iran J Pediatr 26:e4700. https://doi.org/10.5812/ijp.4700
Acknowledgements
Nurcan Dinler Cengiz has been working at Muğla Sıtkı Koçman University Faculty of Medicine, Pediatric Nephrology Department, since April 2016.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study protocol was approved by the Başkent University Institutional Review Board and Ethics Committee.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Parmaksız, G., Kekeç, Ş.D., Cengiz, N.D. et al. The relationship between body mass index and renal length in obese children. Pediatr Nephrol 35, 901–905 (2020). https://doi.org/10.1007/s00467-019-04464-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-019-04464-8