
Abstract
The association between ear and kidney abnormalities has long been recognized; however, the connection between these two disparate organs is not always straightforward. Although Alport syndrome is the most well-known, there are over 20 disorders that need to be considered in the differential diagnosis of patients with both ear and kidney abnormalities. Commonalities are present between the kidney and ear in a number of structural proteins, developmentally important transcription factors, ciliary proteins, and channel proteins, and mutations in these pathways can lead to disease in both organ systems. This manuscript reviews the congenital disorders with both hearing and kidney manifestations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The association between ear and kidney abnormalities has long been recognized; however, the connection between these two disparate organs is not always straightforward. Although Alport syndrome (AS) is the most well-known, there are over 20 disorders that need to be considered in the differential diagnosis of patients with both ear and kidney abnormalities. Kidney diseases associated with ear abnormalities can include a wide variety of disorders, including glomerulopathies, congenital anomalies of the kidney and urinary tract (CAKUT), ciliopathies, and tubulopathies.
Normal hearing
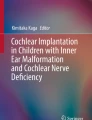
Normal hearing requires multiple steps to convert sound waves to nerve signals that the brain can recognize as sound [1]. Sound waves enter the outer ear and cause vibrations of the tympanic membrane that are then amplified via the middle ear bones. Next, the vibrations are transferred to the fluid-filled, spiral-shaped cochlea, which is divided into three compartments: the scala vestibuli (vestibular duct) and scala tympani (tympanic duct), which both contain perilymph, and the scala media (cochlear duct), which contains endolymph (Fig. 1). The stria vascularis is an epithelium that lines the outer wall of the scala media and secretes potassium-rich (157 mM) and sodium-poor (1.3 mM) endolymph fluid compared with the perilymph (potassium 4.2 mM and sodium 148 mM) [2]. The organ of Corti lies on the basilar membrane and is responsible for converting physical sound waves into electrical nerve stimuli. Within the organ of Corti are inner hair cells and outer hair cells. Vibrations within the cochlear fluid are sensed by stereocilia on top of the hair cells, which are stimulated to bend, and lead to the opening of channels that allow movement of potassium across the cell membrane and electrical signal transmission through the auditory nerve to the brain. Abnormalities at any step of this process can lead to hearing loss. Commonalities are present between the kidney and ear in a number of structural proteins, developmentally important transcription factors, ciliary proteins, and channel proteins, and mutations in these pathways can lead to disease in both organ systems.

Cochlear structures involved in normal hearing. For more detail, see the text
Glomerulopathies
Alport syndrome
Alport syndrome (AS) is an inherited disorder that leads to progressive chronic kidney disease, sensorineural deafness, and ocular abnormalities. It is caused by mutations in COL4A3, COL4A4, and COL4A5 that encode type IV collagen proteins required for maintenance of the glomerular basement membrane (GBM), cochlear basement membranes, and specific basement membranes in the eye [3, 4]. Affected children present with isolated microscopic hematuria followed by proteinuria and decline in glomerular filtration rate. Affected male subjects with X-linked AS and male and female subjects with autosomal recessive AS develop end-stage kidney disease (ESKD) at a median age of 25 years [5, 6]. Individuals with autosomal dominant AS have a slower progression, with only 50% requiring renal replacement therapy by the age of 50 years [7]. Females with X-Linked AS have a wide variability in outcomes, with some women demonstrating only isolated microscopic hematuria, whereas up to 30% of others develop ESKD by the age of 60 years [8, 9]. Treatment of kidney disease with angiotensin-converting enzyme inhibitors is recommended once proteinuria develops and may slow the progression to ESKD [10, 11].
Newborn hearing screening is normal in individuals with AS; however, high frequency hearing loss becomes apparent in late childhood by audiometry and later progresses into the frequency range of conversational speech. Hearing loss is present in 50% of males with X-linked AS by the age of 15 years and 90% by the age of 40 years [5]. Women with X-linked AS are at a lower risk of hearing loss, with 10% affected by the age of 40 years and 20% by the age of 60 years [9]. The hearing loss in AS has been localized to the cochlea [12]. Within the cochlea, type IV collagen is expressed in the spiral limbus, the spiral ligament, stria vascularis, and in the basement membrane situated between the organ of Corti and the basilar membrane [13,14,15].
MYH9-related disorders
MYH9-related disorders are rare autosomal dominant macrothrombocytopenias caused by mutations in MYH9, the gene encoding nonmuscle myosin IIA. These include Epstein syndrome, Fechtner syndrome, May–Hegglin anomaly, and Sebastian syndrome, which were originally classified as separate disorders, but appear to be more appropriately classified as MYH9-related disorders with variable phenotypes of hearing loss, chronic kidney disease, leukocyte Dӧhle-like bodies, and cataracts [16].
Renal disease in MYH9-related disorders manifests as microscopic hematuria and proteinuria in approximately 30–70% of affected individuals, with a majority diagnosed before the age of 35 years [17]. Renal biopsy findings can be similar to those in AS and these disorders can be misdiagnosed owing to the similarities in clinical presentations and pathological findings. Biopsies early in the disease course demonstrate focal foot process effacement in areas of focal thickening of the GBM. At more advanced stages of disease, GBM thickening is more widespread, with areas of GBM lamellation. Isolated GBM thinning has also been reported [18].
Sensorineural hearing loss may be present in up to 58% of affected families at a mean age of 31 years, although some present in their adolescent years [19]. Although the exact mechanism by which mutations in MYH9 cause hearing loss are unknown, nonmuscle myosin IIA is known to be expressed in several structures of the inner ear that are important for hearing, including the organ of Corti, the spiral ligament, and the spiral limbus [20].
Fabry disease
Fabry disease is a rare X-linked disorder characterized by accumulation of globotriaosylceramide (Gb3) in lysosomes of various cell types owing to deficiency of the lysosomal enzyme alpha-galactosidase A caused by mutations in the GLA gene. This accumulation causes thrombotic and ischemic complications including stroke, cardiac disease, and progressive chronic kidney disease. Additional findings may include hypohidrosis, angiokeratomas, pain in the hands and feet, and corneal opacities. Renal involvement presents as proteinuria, hematuria, and isosthenuria with progressive chronic kidney disease leading to ESKD predominantly in the 3rd to 5th decades of life.
Hearing loss is present in 18–55% of patients with Fabry disease and is predominantly sensorineural [21]. High-frequency hearing loss is detectable in a small percentage of children with Fabry disease [22]. The etiology of hearing loss is unclear. Human autopsy studies and mouse studies have demonstrated atrophy of the stria vascularis and spiral ligament, hair cell loss, and a decrease in the number of spiral ganglion cells [23, 24]. Enzyme replacement therapy does not reverse hearing loss; however, it is unknown whether or not early treatment prevents hearing loss [21].
Other glomerular disorders
A number of disorders may manifest as nephrotic syndrome (NS) or proteinuria and hearing loss. Charcot–Marie–Tooth disease is a constellation of inherited neuropathies with variable phenotypes and genetic causes [25]. Mutations in INF2, an actin regulatory protein found in podocytes and Schwann cells, cause Charcot–Marie–Tooth disease with focal segmental glomerulosclerosis (FSGS) [26]. INF2 interacts with diaphanous-related formins (mDia), inhibiting mDia-mediated actin polymerization in response to Rho signaling. Affected patients develop steroid-resistant FSGS and peripheral nerve dysfunction at a median age of 18 and 13 years respectively. Hearing loss is an inconsistent phenotype, with ~33% affected by mild to moderate sensorineural hearing loss [26]. The etiology of hearing loss is unclear; however, mDia1 is required for actin cytoskeletal maintenance in the inner ear hair cells [27].
Mutations in several genes associated with the biosynthesis of coenzyme Q10 have been associated with steroid-resistant NS including COQ2 and COQ6 [28,29,30]. Mutations in these genes lead to decreased coenzyme Q10 levels and reduced mitochondrial respiratory enzyme activity. COQ6 is located in podocyte cell processes, Golgi apparatus, stria vascularis, and spiral ligament cells of the inner ear [29]. Mutations in COQ2 cause collapsing FSGS predominantly in the first decade of life, with increased numbers of mitochondria on EM and variable manifestation of hearing loss [28]. Additional findings may include encephalopathy, hypertrophic cardiomyopathy, and seizures [31]. Mutations in COQ6 cause onset of steroid resistant NS due to FSGS or diffuse mesangial sclerosis within the first few years of life frequently associated with sensorineural hearing loss [29]. Early diagnosis of mutations in the coenzyme Q10 biosynthetic pathway is important, as early supplementation with coenzyme Q10 may be beneficial.
Mutations in MTTL1 encoding tRNA-LEU, a mitochondrial-specific transfer RNA, can present with FSGS and sensorineural hearing loss [32, 33]. Patients are variably affected with MELAS syndrome (mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes). Mutations in mitochondrial DNA are one of the most common causes of inherited deafness [34]. It is hypothesized that increased reactive oxygen species might cause damage to inner ear hair cells and cochlear neurons, leading to hearing loss. The pathogenesis of renal injury in individuals with MTTL1 mutations is unclear.
Cockayne syndrome is a rare autosomal recessive disorder arising from mutations in genes involved in DNA nucleotide excision repair (ERCC6 and ERCC8). It is characterized by growth retardation, cognitive deficits, premature aging, hearing loss, cataracts, retinopathy, sun sensitivity, and dental caries [35]. Renal involvement may include hypertension, proteinuria, and NS or hypoplasia/dysplasia in about 10% of patients, associated with diffuse, homogeneous GBM thickening on EM; however, the pathogenesis is unclear [36]. Sensorineural and/or conductive hearing loss may be present at birth and affects 60–80% of affected individuals [37]. Hearing loss is due to cell loss at multiple sites along the auditory pathways and mimics loss seen in normal aging [35].
Mutation in CD151 have been reported in several families with sensorineural deafness, nephrotic range proteinuria, and renal failure, epidermolysis bullosa, and beta-thalassemia minor [38]. CD151 is an integral cell membrane protein and forms complexes with integrin α3β1 and α6β1 in the kidney and is required for glomerular and tubular basement membrane assembly [39].
Muckle–Wells syndrome is a rare auto-inflammatory disorder caused by NLRP3 mutations, leading to overproduction of interleukin-1β, that is characterized by recurrent fever, arthralgias, fatigue, conjunctivitis, and urticarial rash. Sensorineural hearing loss and renal amyloidosis (<10%) are typically late manifestations of this disease [40]. Hearing loss is thought to be due to chronic inflammation of the inner ear and may improve with interleukin-1 blockade [41].
Congenital anomalies of the kidney and urinary tract
Branchio-oto-renal syndrome
Branchio-oto-renal syndrome is a relatively common (estimated incidence of 1:40,000) autosomal dominant disorder with hearing loss, outer ear malformations, and renal anomalies, with a variable penetrance caused by mutations in EYA1, SIX1, and SIX5 [42,43,44,45]. Causative genes encode transcription co-activators with an effect on a wide array of downstream target genes [46]. EYA1 expression in the developing metanephros is restricted to condensing mesenchymal cells [47]. Congenital anomalies of the kidney and urinary tract can be identified in ~67% and include renal agenesis, hypoplasia/dysplasia, ureteropelvic junction obstruction, and vesicoureteral reflux (VUR) [48]. Hearing impairment is present in over 70% of affected individuals and may be sensorineural, conductive, or mixed [49]. During ear development, EYA1 expression is observed in differentiating hair cells and in the associated ganglia and appears to be required for differentiation and survival of inner ear cells [47]. Additional phenotypic features may include cleft palate, retrognathia, facial nerve paresis, nonrotation of the gastrointestinal tract, and pancreatic duplication cyst [49].
Townes–Brocks syndrome
Townes–Brocks syndrome is an autosomal dominant disorder due to mutations in SALL1 (encoding a zinc finger protein thought to act as a transcriptional repressor) that is characterized by the triad of imperforate anus, dysplastic ears, and thumb malformations [50]. SALL1 is expressed in the metanephric mesenchyme in the developing kidney and is required for ureteric bud invasion in kidney development [51]. Approximately 42% of affected individuals have renal anomalies that may include renal agenesis, hypoplasia/dysplasia, or cystic kidneys [52]. Hearing loss or dysplastic outer ears are observed in 65% of individuals with Townes–Brocks syndrome. Malformations in the malleus and incus have been identified in some patients with Townes–̄Brocks syndrome, leading to conductive hearing loss [53]. SALL1 mutations also frequently lead to inner ear dysfunction and sensorineural hearing loss; however, the mechanisms are unclear [54]. Additional clinical findings may include club feet, toe malformations, genitourinary anomalies, and congenital heart disease.
CHARGE syndrome and Abruzzo–Erickson syndrome
The CHARGE syndrome is a rare disorder including coloboma, heart defects, choanal atresia, retardation of growth or development, genitourinary malformations, and ear anomalies due to a mutation in CHD7, a transcriptional regulator required for normal neural crest migration [55]. One patient with this phenotype has also been reported with a mutation in SEMA3E, encoding developmental neural guidance molecules [56]. Significant renal anomalies are uncommonly associated, but may include dysplasia, renal agenesis, or horseshoe/ectopic kidney. Genital hypoplasia occurs in 50–70% of individuals [57]. Either conductive or sensorineural hearing loss can occur in CHARGE syndrome. Typically, the lateral semicircular canals are absent; however, dysplasia of all semicircular canals and the cochlea can be observed [57].
Abruzzo–Erickson syndrome has been referred to as X-linked CHARGE syndrome and is caused by mutations in TBX22, a transcription factor [58]. Additional findings may include cleft palate and radial synostosis [59].
Other syndromes
A number of mutations in other genes are associated with very rare syndromes, with hearing loss, and with congenital anomalies of the kidney and urinary tract, and are summarized in Table 1.
Ciliopathies
Cilia are membrane-enclosed hair-like cell organelles that are found on the apical surface of many cells, including renal tubular cells. The broad range of phenotypes observed in ciliopathies demonstrates the presence of cilia in all organ systems. They function as chemo-, mechano- and osmosensors and mediate many pathways essential for organ development, including left–right organization of the internal organs [60]. Genetic disorders of primary cilia are a frequent cause of childhood renal disease, which is frequently cystic in nature. Primary cilium dysfunction alters spatial organization of the cells (planar cell polarity) and therefore cellular growth and development, possibly via deranged Wnt signaling [61]. This leads to cystic kidneys and often many extra-renal defects. Examples of renal ciliopathies include autosomal recessive and dominant polycystic kidney disease, von Hippel–Lindau disease, tuberous sclerosis, and the medullary cystic kidney disease–nephronophthisis complex. The Bardet–Biedl and Alstrom syndromes are ciliopathies causing renal disease and deafness in addition to sharing other phenotypic characteristics, such as retinitis pigmentosa, obesity, and diabetes mellitus. In addition to primary cystic kidney disease, affected individuals may develop secondary renal dysfunction due to diabetes and hypertension.
Bardet–Biedl syndrome
Bardet–Biedl syndrome (BBS) is characterized by polydactyly, learning difficulties, and hypogonadism in addition to the features listed above. Polydactyly (and perhaps brachydactyly and syndactyly) may be the only early feature; thus, diagnosis is often delayed until later in childhood. Obesity is particularly common and most develop blindness by the second or third decade because of an atypical retinitis pigmentosa with early macular involvement [62]. Data on deafness in BBS is often incomplete, although a series of 109 cases reported hearing loss in 21% of patients, mostly because of a conductive pattern (chronic otitis media), although 3 patients had unexplained sensorineural deafness [63]. Up to 50% of adults with BBS had subclinical sensorineural deafness in another series [64]. The renal phenotype is variable, with structural malformations common, although a cystic tubulopathy similar to nephronophthisis is typical. It is a rare disorder with a variable prevalence, ranging from 1 in 13,500 among the Bedouin peoples of Kuwait to 1 in 100,000 and 1 in 160,000 in North America and Switzerland respectively [6]. It is a heterogenous genetic condition, generally inherited in an autosomal recessive pattern. Mutations in at least 19 genes are associated with the syndrome, with those in BBS1 the most common, followed by BBS10 (Table 1) [63, 65]. The BBS proteins form a complex, the BBSome, which is involved in cilia targeting and assembly. MKKS (BBS6) is expressed in inner hair cells and outer hair cells of the cochlea and mutations may impair function of the kinocilium, which is important for cochlear development [64, 66]. A study of 350 cases of BBS from a UK registry found that 31% of children and 42% of adults had CKD. It also noted that a severe phenotype was likely with the presence of two truncating mutations and a BBS10 (versus BBS1) mutations [65].
Alstrom syndrome
Alstrom syndrome is an autosomal recessive disorder caused by mutations in the ALMS1 gene, the protein of which is found in the cilium basal body. It shares many clinical features of BBS including cone–rod dystrophy and childhood obesity, although there is no polydactyly, hypogonadism or learning difficulty [67]. The hearing loss in individuals with Alstrom syndrome is sensorineural in origin. It is recognized that altered planar cell polarity in the inner ear disrupts orientation of the stereociliary bundles, mechanosensing organelles of hair cells, which may explain the pathogenesis of the deafness in Alstrom syndrome [68]. A myriad of urological problems are frequently reported. Consistent with BBS, the renal disease appears to be predominantly due to interstitial fibrosis in cases in which biopsies are performed [69]. Life expectancy is often greatly reduced because of dilated cardiomyopathy, liver disease, and restrictive lung disease.
Tubulopathies
There are several rare genetic syndromes that share the phenotypes of deafness and renal tubular dysfunction. These syndromes are mostly due to co-localization of electrolyte channels in the cochlea and renal tubular cells. In contrast to ciliopathies, where renal impairment may occur because of tubulointerstitial fibrosis, these syndromes feature various metabolic phenomena caused by altered tubular cell function (Fig. 2).

Localization of tubular channels affected in renal and hearing syndromes. a Abnormalities in barttin, critical for function of the basolateral chloride channels in the thick ascending limb of the loop of Henle, cause Bartter syndrome. b Abnormalities in Kir4.1, an inward rectifying potassium channel in the distal convoluted tubule, cause EAST syndrome. c Abnormalities in pendrin, a sodium-independent chloride–bicarbonate exchanger on the apical membrane of β-intercalated cells of the distal nephron, cause Pendred syndrome. d Abnormalities in the B1 and a4 subunits of H+-ATPase in α-intercalated cells cause distal renal tubular acidosis with deafness. TAL thick ascending limb, ROMK renal outer medullary potassium channel, DCT distal convoluted tubule, NCC sodium-chloride co-transporter, CaSR calcium sensing receptor
Bartter syndrome
Bartter syndrome (BS) is a group of autosomal recessive disorders caused by mutations in various ion transport mechanisms of the thick ascending limb of the loop of Henle. It is characterized by hypokalemia, metabolic alkalosis, often hypercalciuria and hyperreninemia due to hyperplasia of the juxtaglomerular apparatus. These metabolic features mimic those seen with the chronic use of loop diuretics. In types I, II, and III BS respectively, the altered channels are the Na-K-2Cl co-transporter (coded by SLC12A1), the luminal potassium channel ROMK (coded by KCNJ1), and the basolateral chloride channel ClC-Kb (coded by CLCNKB) [70]. Deafness is not a feature of these conditions.
Bartter syndrome with sensorineural deafness (BS type IV) is due to the loss of function mutations in BSND [71,72,73], coding Barttin, a protein that co-localizes to the basolateral membrane of the loop tubular cells and the inner ear epithelia [73]. Barttin is critical for both the ClC-Ka and ClC-Kb channels. These channels have an overlapping function; thus, the complete phenotype requires defects in both the ClC-Ka and ClC-Kb channels, explaining the milder disease seen in BS type III (preserved ClC-Ka activity). Aside from BSND mutations affecting barttin, simultaneous mutations of genes coding ClC-Ka and ClC-Kb cause a similar phenotype [74], termed BS type IVb. This also explains why deafness is not a feature of BS type III (only ClC-Kb is affected). The phenotype of BS type IV is generally that of severe salt-losing nephropathy and early sensorineural deafness. There is often an antenatal presentation with polyhydramnios in the mother and neonatal volume depletion in the infant. Type IV disease may also demonstrate progressive renal dysfunction more commonly than other BS subtypes. This phenotypic variability may be modified by the particular causative mutation in BSND [71].
EAST syndrome
The EAST syndrome is an autosomal recessive condition caused by mutation in the KCNJ10 gene, coding for an inward rectifying potassium channel. This channel, Kir4.1, is expressed on the basolateral membrane of the distal nephron, from the macula densa to the early cortical collecting duct. It is expressed in the spinal cord and brain, where it may maintain membrane resting potential and modulate cell excitability [75]. It is also found in the cochlea, where it is involved in the generation of endolymph. Loss of function mutations in KCNJ10 are characterized by epilepsy, ataxia, moderate sensorineural deafness, and tubulopathy leading to a salt-losing nephropathy similar to BS (with hypokalemia, metabolic alkalosis, and normal blood pressure) [76]. It was described by Scholl et al. as SESAME syndrome with features of seizures, sensorineural deafness, ataxia, mental retardation, and electrolyte imbalance [77]. Neurological features include generalized seizures in infancy, delayed psychomotor development, ataxia with a progressive axonal neuropathy, and hypomyelination [77]. The salt-wasting and hypokalemic state may be explained by impaired function of the distal convoluted tubular cells due to mutant Kir4.1, as basolateral potassium recycling is critical for Na-Cl reabsorption [78].
Combined oxidative phosphorylation deficiency-11
Combined oxidative phosphorylation deficiency is a group of rare autosomal recessive disorders with multisystemic features. Loss-of-function mutations in mitochondrial translation genes cause the syndrome, with the RMND1 gene being responsible for combined oxidative phosphorylation deficiency-11 [78]. Features include seizures, encephalopathy, hypotonia, liver disease, lactic acidosis, and death in infancy. Additionally, hearing loss and renal failure in the context of a tubulopathy have also been described [78, 79]. Other renal phenotypes reported include dysplastic kidneys and renal tubular acidosis [79], but the pathogenesis of the renal involvement remains unclear given the rarity of the condition.
Distal renal tubular acidosis with progressive nerve deafness
Distal renal tubular acidosis (RTA) with progressive nerve deafness is another rare autosomal recessive condition caused by mutations in the ATP6B1 gene. This gene codes for the B1 subunit of H+-ATPase, which co-localizes to the apical surface of α-intercalated cells of the distal nephron and the endolymphatic sac of the cochlea. The deafness is presumably caused by impairment of endolymphatic pH homeostasis with alkalinization of endolymph leading to altered hair cell function [80]. The presentation is usually in childhood with failure to thrive and a tubulopathy manifested by hyperchloremic metabolic acidosis (type 1 distal RTA), hypokalemia and hypercalciuria, often with nephrocalcinosis and stone disease [80]. Although alkali therapy may help the systemic pH, it has no impact on hearing loss.
Mutations in the ATP6N1B gene, coding for the a4 subunit of H+-ATPase, also cause distal RTA, but deafness was not thought to be a consequence [81]. However, reports have emerged of later onset deafness occurring with ATP6N1B mutations when individuals were followed up into adulthood [82, 83]. In some cases, childhood deafness has also been reported, demonstrating the genetic and phenotypic variability of distal RTA with progressive nerve deafness [83].
Pendred syndrome
Pendrin is a sodium-independent chloride–bicarbonate exchanger found in the inner ear and thyroid, where it regulates acid/base in the endolymphatic sac and iodide transport respectively. It is also found on the apical membrane of β intercalated cells in the distal nephron, where it mediates bicarbonate secretion and chloride absorption [84]. Pendred syndrome is an autosomal recessive disorder caused by mutation in the SLC26A4 gene, which encodes pendrin. The phenotype is that of sensorineural deafness and goiter, as described by Vaughan Pendred [85].
Pendrin is upregulated in metabolic alkalosis, which attenuates the alkalosis by secreting bicarbonate. However, patients with Pendred syndrome generally have no electrolyte or acid/base disturbance at baseline, possibly because pendrin and the Na-Cl co-transporter (NCC) cross-compensate for each other. Pendrin appears to have minimal influence on Na-Cl reabsorption in the steady state, but may be critical when NCC is inactivated. This explains why patients with Pendred syndrome may develop profound hypovolemia, hypokalemia, and hypochloremic metabolic alkalosis if exposed to thiazide diuretics [86] or an alkali load. It also explains why mice with double pendrin/NCC gene knockouts display a similar phenotype [87].
It is notable that mutations in SLC26A4 may cause isolated deafness often with an enlarged vestibular aqueduct. Moreover, many patients with the Pendred phenotype lack a mutation in SLC26A4, suggesting additional undiscovered genetic causes. Cases of Pendred syndrome have also been described with homozygous mutations in SLC26A4 and in FOXI1, a gene that regulates SLC26A4, again highlighting the genetic heterogeneity of the condition [88].
Multiple choice questions (answers are provided following the reference list)
-
1.
A 17-year-old boy has sensorineural hearing loss, hematuria, and proteinuria with GBM thickening on electron microscopy, and thrombocytopenia. Mutation in which of the following genes is the most likely cause of his symptoms?
-
a)
COL4A5
-
b)
COL4A3
-
c)
MYH9
-
d)
COQ2
-
e)
CD151
-
a)
-
2.
A 1-year-old boy has small dysplastic kidneys, triphalangeal thumbs, and a history of imperforate anus corrected in the neonatal period. What is the child’s most likely underlying diagnosis?
-
a)
Townes–Brocks syndrome
-
b)
Branchio-oto-renal syndrome
-
c)
CHARGE syndrome
-
d)
Abruzzo–Erickson syndrome
-
e)
Wolfram syndrome
-
a)
-
3.
A 5-year-old has sensorineural deafness, hypokalemia, metabolic alkalosis, and polyuria. Mutation in which of the following genes is likely to be the cause of his symptoms?
-
a)
SLC12A1 (Na-K-2Cl co-transporter)
-
b)
KCNJ1 (ROMK potassium channel)
-
c)
KCNJ10 (Kir4.1 potassium channel)
-
d)
BSND (Barttin)
-
e)
ATP6B1 (B1 subunit of H+-ATPase)
-
a)
-
4.
A 16-year-old boy with recently diagnosed X-linked Alport syndrome has proteinuria (1.5 g/day), normal blood pressure, and eGFR of 85 ml/min/1.73 m2. What treatment should be initiated to slow the progression of chronic kidney disease?
-
a)
Calcineurin inhibitor
-
b)
Calcium channel blocker
-
c)
Beta blocker
-
d)
Thiazide diuretic
-
e)
ACE inhibitor
-
a)
-
5.
An 8-year-old girl has steroid-resistant nephrotic syndrome and FSGS on kidney biopsy. Treatment with coenzyme Q10 should be initiated if a mutation is identified in which of the following genes?
-
a)
COQ2
-
b)
MTTL1
-
c)
INF2
-
d)
CD151
-
e)
COL4A5
-
a)
References
Sliwinska-Kowalska M (2015) Hearing. Handb Clin Neurol 131:341–363
Lang F, Vallon V, Knipper M, Wangemann P (2007) Functional significance of channels and transporters expressed in the inner ear and kidney. Am J Physiol Cell Physiol 293(4):C1187–C1208
Barker DF, Hostikka SL, Zhou J, Chow LT, Oliphant AR, Gerken SC, Gregory MC, Skolnick MH, Atkin CL, Tryggvason K (1990) Identification of mutations in the COL4A5 collagen gene in Alport syndrome. Science 248(4960):1224–1227
Mochizuki T, Lemmink HH, Mariyama M, Antignac C, Gubler MC, Pirson Y, Verellen-Dumoulin C, Chan B, Schroder CH, Smeets HJ, Reeders ST (1994) Identification of mutations in the alpha 3(IV) and alpha 4(IV) collagen genes in autosomal recessive Alport syndrome. Nat Genet 8(1):77–81
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Verellen C, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schroder C, Sanak M, Krejcova S, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC (2000) X-linked Alport syndrome: natural history in 195 families and genotype- phenotype correlations in males. J Am Soc Nephrol 11 (4):649-657
Storey H, Savige J, Sivakumar V, Abbs S, Flinter FA (2013) COL4A3/COL4A4 mutations and features in individuals with autosomal recessive Alport syndrome. J Am Soc Nephrol 24(12):1945–1954
Marcocci E, Uliana V, Bruttini M, Artuso R, Silengo MC, Zerial M, Bergesio F, Amoroso A, Savoldi S, Pennesi M, Giachino D, Rombola G, Fogazzi GB, Rosatelli C, Martinhago CD, Carmellini M, Mancini R, Di Costanzo G, Longo I, Renieri A, Mari F (2009) Autosomal dominant Alport syndrome: molecular analysis of the COL4A4 gene and clinical outcome. Nephrol Dial Transplant 24 (5):1464–1471
Rheault MN (2012) Women and Alport syndrome. Pediatr Nephrol 27(1):41–46
Jais JP, Knebelmann B, Giatras I, De Marchi M, Rizzoni G, Renieri A, Weber M, Gross O, Netzer KO, Flinter F, Pirson Y, Dahan K, Wieslander J, Persson U, Tryggvason K, Martin P, Hertz JM, Schroder C, Sanak M, Carvalho MF, Saus J, Antignac C, Smeets H, Gubler MC (2003) X-linked Alport syndrome: natural history and genotype-phenotype correlations in girls and women belonging to 195 families: a “European Community Alport syndrome concerted action” study. J Am Soc Nephrol 14(10):2603–2610
Kashtan CE, Ding J, Gregory M, Gross O, Heidet L, Knebelmann B, Rheault M, Licht C (2013) Clinical practice recommendations for the treatment of Alport syndrome: a statement of the Alport syndrome research collaborative. Pediatr Nephrol 28(1):5–11
Gross O, Licht C, Anders HJ, Hoppe B, Beck B, Tonshoff B, Hocker B, Wygoda S, Ehrich JH, Pape L, Konrad M, Rascher W, Dotsch J, Muller-Wiefel DE, Hoyer P, Knebelmann B, Pirson Y, Grunfeld JP, Niaudet P, Cochat P, Heidet L, Lebbah S, Torra R, Friede T, Lange K, Muller GA, Weber M (2012) Early angiotensin-converting enzyme inhibition in Alport syndrome delays renal failure and improves life expectancy. Kidney Int 81(5):494–501
Wester DC, Atkin CL, Gregory MC (1995) Alport syndrome: clinical update. J Am Acad Audiol 6:73–79
Kleppel MM, Santi PA, Cameron JD, Wieslander J, Michael AF (1989) Human tissue distribution of novel basement membrane collagen. Am J Pathol 134:813–825
Cosgrove D, Samuelson G, Meehan DT, Miller C, McGee J, Walsh EJ, Siegel M (1998) Ultrastructural, physiological, and molecular defects in the inner ear of a gene-knockout mouse model of autosomal Alport syndrome. Hearing Res 121:84–98
Harvey SJ, Mount R, Sado Y, Naito I, Ninomiya Y, Harrison R, Jefferson B, Jacobs R, Thorner PS (2001) The inner ear of dogs with X-linked nephritis provides clues to the pathogenesis of hearing loss in X-linked Alport syndrome. Am J Pathol 159(3):1097–1104
Seri M, Pecci A, Di Bari F, Cusano R, Savino M, Panza E, Nigro A, Noris P, Gangarossa S, Rocca B, Gresele P, Bizzaro N, Malatesta P, Koivisto PA, Longo I, Musso R, Pecoraro C, Iolascon A, Magrini U, Rodriguez Soriano J, Renieri A, Ghiggeri GM, Ravazzolo R, Balduini CL, Savoia A (2003) MYH9-related disease: May-Hegglin anomaly, Sebastian syndrome, Fechtner syndrome, and Epstein syndrome are not distinct entities but represent a variable expression of a single illness. Medicine (Baltimore) 82(3):203–215
Singh N, Nainani N, Arora P, Venuto RC (2009) CKD in MYH9-related disorders. Am J Kidney Dis 54(4):732–740
Naito I, Nomura S, Inoue S, Kagawa M, Kawai S, Gunshin Y, Joh K, Tsukidate C, Sado Y, Osawa G (1997) Normal distribution of collagen IV in renal basement membranes in Epstein’s syndrome. J Clin Pathol 50(11):919–922
Pecci A, Klersy C, Gresele P, Lee KJ, De Rocco D, Bozzi V, Russo G, Heller PG, Loffredo G, Ballmaier M, Fabris F, Beggiato E, Kahr WH, Pujol-Moix N, Platokouki H, Van Geet C, Noris P, Yerram P, Hermans C, Gerber B, Economou M, De Groot M, Zieger B, De Candia E, Fraticelli V, Kersseboom R, Piccoli GB, Zimmermann S, Fierro T, Glembotsky AC, Vianello F, Zaninetti C, Nicchia E, Guthner C, Baronci C, Seri M, Knight PJ, Balduini CL, Savoia A (2014) MYH9-related disease: a novel prognostic model to predict the clinical evolution of the disease based on genotype-phenotype correlations. Hum Mutat 35 (2):236-247
Mhatre AN, Li J, Kim Y, Coling DE, Lalwani AK (2004) Cloning and developmental expression of nonmuscle myosin IIA (Myh9) in the mammalian inner ear. J Neurosci Res 76(3):296–305
Suntjens EB, Smid BE, Biegstraaten M, Dreschler WA, Hollak CE, Linthorst GE (2015) Hearing loss in adult patients with Fabry disease treated with enzyme replacement therapy. J Inherit Metab Dis 38(2):351–358
Suntjens E, Dreschler WA, Hess-Erga J, Skrunes R, Wijburg FA, Linthorst GE, Tondel C, Biegstraaten M (2017) Hearing loss in children with Fabry disease. J Inherit Metab Dis. doi: 10.1007/s10545-017-0051-5
Sakurai Y, Suzuki R, Yoshida R, Kojima H, Watanabe M, Manome Y, Ohashi T, Eto Y, Moriyama H (2010) Inner ear pathology of alpha-galactosidase A deficient mice, a model of Fabry disease. Auris Nasus Larynx 37(3):274–280
Schachern PA, Shea DA, Paparella MM, Yoon TH (1989) Otologic histopathology of Fabry’s disease. Ann Otol Rhinol Laryngol 98(5 Pt 1):359–363
Rossor AM, Polke JM, Houlden H, Reilly MM (2013) Clinical implications of genetic advances in Charcot-Marie-Tooth disease. Nat Rev Neurol 9(10):562–571
Boyer O, Nevo F, Plaisier E, Funalot B, Gribouval O, Benoit G, Huynh Cong E, Arrondel C, Tete MJ, Montjean R, Richard L, Karras A, Pouteil-Noble C, Balafrej L, Bonnardeaux A, Canaud G, Charasse C, Dantal J, Deschenes G, Deteix P, Dubourg O, Petiot P, Pouthier D, Leguern E, Guiochon-Mantel A, Broutin I, Gubler MC, Saunier S, Ronco P, Vallat JM, Alonso MA, Antignac C, Mollet G (2011) INF2 mutations in Charcot-Marie-Tooth disease with glomerulopathy. N Engl J Med 365(25):2377–2388
Muller U, Littlewood-Evans A (2001) Mechanisms that regulate mechanosensory hair cell differentiation. Trends Cell Biol 11(8):334–342
Diomedi-Camassei F, Di Giandomenico S, Santorelli FM, Caridi G, Piemonte F, Montini G, Ghiggeri GM, Murer L, Barisoni L, Pastore A, Muda AO, Valente ML, Bertini E, Emma F (2007) COQ2 nephropathy: a newly described inherited mitochondriopathy with primary renal involvement. J Am Soc Nephrol 18(10):2773–2780
Heeringa SF, Chernin G, Chaki M, Zhou W, Sloan AJ, Ji Z, Xie LX, Salviati L, Hurd TW, Vega-Warner V, Killen PD, Raphael Y, Ashraf S, Ovunc B, Schoeb DS, McLaughlin HM, Airik R, Vlangos CN, Gbadegesin R, Hinkes B, Saisawat P, Trevisson E, Doimo M, Casarin A, Pertegato V, Giorgi G, Prokisch H, Rotig A, Nurnberg G, Becker C, Wang S, Ozaltin F, Topaloglu R, Bakkaloglu A, Bakkaloglu SA, Muller D, Beissert A, Mir S, Berdeli A, Varpizen S, Zenker M, Matejas V, Santos-Ocana C, Navas P, Kusakabe T, Kispert A, Akman S, Soliman NA, Krick S, Mundel P, Reiser J, Nurnberg P, Clarke CF, Wiggins RC, Faul C, Hildebrandt F (2011) COQ6 mutations in human patients produce nephrotic syndrome with sensorineural deafness. J Clin Invest 121(5):2013–2024
Salviati L, Sacconi S, Murer L, Zacchello G, Franceschini L, Laverda AM, Basso G, Quinzii C, Angelini C, Hirano M, Naini AB, Navas P, DiMauro S, Montini G (2005) Infantile encephalomyopathy and nephropathy with CoQ10 deficiency: a CoQ10-responsive condition. Neurology 65(4):606–608
Doimo M, Desbats MA, Cerqua C, Cassina M, Trevisson E, Salviati L (2014) Genetics of coenzyme q10 deficiency. Mol Syndromol 5(3–4):156–162
Kurogouchi F, Oguchi T, Mawatari E, Yamaura S, Hora K, Takei M, Sekijima Y, Ikeda S, Kiyosawa K (1998) A case of mitochondrial cytopathy with a typical point mutation for MELAS, presenting with severe focal-segmental glomerulosclerosis as main clinical manifestation. Am J Nephrol 18(6):551–556
Yorifuji T, Kawai M, Momoi T, Sasaki H, Furusho K, Muroi J, Shimizu K, Takahashi Y, Matsumura M, Nambu M, Okuno T (1996) Nephropathy and growth hormone deficiency in a patient with mitochondrial tRNA(Leu(UUR)) mutation. J Med Genet 33(7):621–622
Ding Y, Leng J, Fan F, Xia B, Xu P (2013) The role of mitochondrial DNA mutations in hearing loss. Biochem Genet 51(7–8):588–602
Karikkineth AC, Scheibye-Knudsen M, Fivenson E, Croteau DL, Bohr VA (2017) Cockayne syndrome: clinical features, model systems and pathways. Ageing Res Rev 33:3–17. https://doi.org/10.1016/j.arr.2016.08.002
Hirooka M, Hirota M, Kamada M (1988) Renal lesions in Cockayne syndrome. Pediatr Nephrol 2(2):239–243
Wilson BT, Stark Z, Sutton RE, Danda S, Ekbote AV, Elsayed SM, Gibson L, Goodship JA, Jackson AP, Keng WT, King MD, McCann E, Motojima T, Murray JE, Omata T, Pilz D, Pope K, Sugita K, White SM, Wilson IJ (2016) The Cockayne syndrome natural history (CoSyNH) study: clinical findings in 102 individuals and recommendations for care. Genet Med 18(5):483–493
Kagan A, Feld S, Chemke J, Bar-Khayim Y (1988) Occurrence of hereditary nephritis, pretibial epidermolysis bullosa and beta-thalassemia minor in two siblings with end-stage renal disease. Nephron 49(4):331–332
Karamatic Crew V, Burton N, Kagan A, Green CA, Levene C, Flinter F, Brady RL, Daniels G, Anstee DJ (2004) CD151, the first member of the tetraspanin (TM4) superfamily detected on erythrocytes, is essential for the correct assembly of human basement membranes in kidney and skin. Blood 104(8):2217–2223
Tran TA (2017) Muckle-Wells syndrome: clinical perspectives. Open Access Rheumatol 9:123–129
Kuemmerle-Deschner JB, Koitschev A, Tyrrell PN, Plontke SK, Deschner N, Hansmann S, Ummenhofer K, Lohse P, Koitschev C, Benseler SM (2015) Early detection of sensorineural hearing loss in Muckle-Wells-syndrome. Pediatr Rheumatol Online J 13(1):43
Fraser FC, Sproule JR, Halal F (1980) Frequency of the branchio-oto-renal (BOR) syndrome in children with profound hearing loss. Am J Med Genet 7(3):341–349
Abdelhak S, Kalatzis V, Heilig R, Compain S, Samson D, Vincent C, Weil D, Cruaud C, Sahly I, Leibovici M, Bitner-Glindzicz M, Francis M, Lacombe D, Vigneron J, Charachon R, Boven K, Bedbeder P, Van Regemorter N, Weissenbach J, Petit C (1997) A human homologue of the drosophila eyes absent gene underlies branchio-oto-renal (BOR) syndrome and identifies a novel gene family. Nat Genet 15(2):157–164
Ruf RG, Xu PX, Silvius D, Otto EA, Beekmann F, Muerb UT, Kumar S, Neuhaus TJ, Kemper MJ, Raymond RM Jr, Brophy PD, Berkman J, Gattas M, Hyland V, Ruf EM, Schwartz C, Chang EH, Smith RJ, Stratakis CA, Weil D, Petit C, Hildebrandt F (2004) SIX1 mutations cause branchio-oto-renal syndrome by disruption of EYA1-SIX1-DNA complexes. Proc Natl Acad Sci U S A 101(21):8090–8095
Hoskins BE, Cramer CH, Silvius D, Zou D, Raymond RM, Orten DJ, Kimberling WJ, Smith RJ, Weil D, Petit C, Otto EA, Xu PX, Hildebrandt F (2007) Transcription factor SIX5 is mutated in patients with branchio-oto-renal syndrome. Am J Hum Genet 80(4):800–804
Mutsuddi M, Chaffee B, Cassidy J, Silver SJ, Tootle TL, Rebay I (2005) Using drosophila to decipher how mutations associated with human branchio-oto-renal syndrome and optical defects compromise the protein tyrosine phosphatase and transcriptional functions of eyes absent. Genetics 170(2):687–695
Kalatzis V, Sahly I, El-Amraoui A, Petit C (1998) Eya1 expression in the developing ear and kidney: towards the understanding of the pathogenesis of branchio-oto-renal (BOR) syndrome. Dev Dyn 213(4):486–499
Chang EH, Menezes M, Meyer NC, Cucci RA, Vervoort VS, Schwartz CE, Smith RJ (2004) Branchio-oto-renal syndrome: the mutation spectrum in EYA1 and its phenotypic consequences. Hum Mutat 23(6):582–589
Kochhar A, Fischer SM, Kimberling WJ, Smith RJ (2007) Branchio-oto-renal syndrome. Am J Med Genet A 143A(14):1671–1678
Powell CM, Michaelis RC (1999) Townes-Brocks syndrome. J Med Genet 36(2):89–93
Nishinakamura R, Matsumoto Y, Nakao K, Nakamura K, Sato A, Copeland NG, Gilbert DJ, Jenkins NA, Scully S, Lacey DL, Katsuki M, Asashima M, Yokota T (2001) Murine homolog of SALL1 is essential for ureteric bud invasion in kidney development. Development 128(16):3105–3115
Botzenhart EM, Bartalini G, Blair E, Brady AF, Elmslie F, Chong KL, Christy K, Torres-Martinez W, Danesino C, Deardorff MA, Fryns JP, Marlin S, Garcia-Minaur S, Hellenbroich Y, Hay BN, Penttinen M, Shashi V, Terhal P, Van Maldergem L, Whiteford ML, Zackai E, Kohlhase J (2007) Townes-Brocks syndrome: twenty novel SALL1 mutations in sporadic and familial cases and refinement of the SALL1 hot spot region. Hum Mutat 28(2):204–205
Ferraz FG, Nunes L, Ferraz ME, Sousa JP, Santos M, Carvalho C, Maroteaux P (1989) Townes-Brocks syndrome. Report of a case and review of the literature. Ann Genet 32(2):120–123
Kohlhase J, Wischermann A, Reichenbach H, Froster U, Engel W (1998) Mutations in the SALL1 putative transcription factor gene cause Townes-Brocks syndrome. Nat Genet 18(1):81–83
Janssen N, Bergman JE, Swertz MA, Tranebjaerg L, Lodahl M, Schoots J, Hofstra RM, van Ravenswaaij-Arts CM, Hoefsloot LH (2012) Mutation update on the CHD7 gene involved in CHARGE syndrome. Hum Mutat 33(8):1149–1160
Lalani SR, Safiullah AM, Molinari LM, Fernbach SD, Martin DM, Belmont JW (2004) SEMA3E mutation in a patient with CHARGE syndrome. J Med Genet 41(7):e94
Hsu P, Ma A, Wilson M, Williams G, Curotta J, Munns CF, Mehr S (2014) CHARGE syndrome: a review. J Paediatr Child Health 50(7):504–511
Pauws E, Peskett E, Boissin C, Hoshino A, Mengrelis K, Carta E, Abruzzo MA, Lees M, Moore GE, Erickson RP, Stanier P (2013) X-linked CHARGE-like Abruzzo-Erickson syndrome and classic cleft palate with ankyloglossia result from TBX22 splicing mutations. Clin Genet 83(4):352–358
Abruzzo MA, Erickson RP (1977) A new syndrome of cleft palate associated with coloboma, hypospadias, deafness, short stature, and radial synostosis. J Med Genet 14(1):76–80
Bergmann C (2012) Educational paper: ciliopathies. Eur J Pediatr 171(9):1285–1300
Hildebrandt F, Benzing T, Katsanis N (2011) Ciliopathies. N Engl J Med 364(16):1533–1543
Forsythe E, Beales PL (2013) Bardet-Biedl syndrome. Eur J Hum Genet 21(1):8–13
Beales PL, Elcioglu N, Woolf AS, Parker D, Flinter FA (1999) New criteria for improved diagnosis of Bardet-Biedl syndrome: results of a population survey. J Med Genet 36(6):437–446
Ross AJ, May-Simera H, Eichers ER, Kai M, Hill J, Jagger DJ, Leitch CC, Chapple JP, Munro PM, Fisher S, Tan PL, Phillips HM, Leroux MR, Henderson DJ, Murdoch JN, Copp AJ, Eliot MM, Lupski JR, Kemp DT, Dollfus H, Tada M, Katsanis N, Forge A, Beales PL (2005) Disruption of Bardet-Biedl syndrome ciliary proteins perturbs planar cell polarity in vertebrates. Nat Genet 37(10):1135–1140
Forsythe E, Sparks K, Best S, Borrows S, Hoskins B, Sabir A, Barrett T, Williams D, Mohammed S, Goldsmith D, Milford DV, Bockenhauer D, Foggensteiner L, Beales PL (2017) Risk factors for severe renal disease in Bardet-Biedl syndrome. J Am Soc Nephrol 28(3):963–970
Katsanis N, Beales PL, Woods MO, Lewis RA, Green JS, Parfrey PS, Ansley SJ, Davidson WS, Lupski JR (2000) Mutations in MKKS cause obesity, retinal dystrophy and renal malformations associated with Bardet-Biedl syndrome. Nat Genet 26(1):67–70
Marshall JD, Hinman EG, Collin GB, Beck S, Cerqueira R, Maffei P, Milan G, Zhang W, Wilson DI, Hearn T, Tavares P, Vettor R, Veronese C, Martin M, So WV, Nishina PM, Naggert JK (2007) Spectrum of ALMS1 variants and evaluation of genotype-phenotype correlations in Alstrom syndrome. Hum Mutat 28(11):1114–1123
May-Simera H (2016) Evaluation of planar-cell-polarity phenotypes in Ciliopathy mouse mutant cochlea. J Vis Exp 108:53559
Marshall JD, Bronson RT, Collin GB, Nordstrom AD, Maffei P, Paisey RB, Carey C, Macdermott S, Russell-Eggitt I, Shea SE, Davis J, Beck S, Shatirishvili G, Mihai CM, Hoeltzenbein M, Pozzan GB, Hopkinson I, Sicolo N, Naggert JK, Nishina PM (2005) New Alstrom syndrome phenotypes based on the evaluation of 182 cases. Arch Intern Med 165(6):675–683
Koulouridis E, Koulouridis I (2015) Molecular pathophysiology of Bartter’s and Gitelman’s syndromes. World J Pediatr 11(2):113–125
Janssen AG, Scholl U, Domeyer C, Nothmann D, Leinenweber A, Fahlke C (2009) Disease-causing dysfunctions of barttin in Bartter syndrome type IV. J Am Soc Nephrol 20(1):145–153
Birkenhager R, Otto E, Schurmann MJ, Vollmer M, Ruf EM, Maier-Lutz I, Beekmann F, Fekete A, Omran H, Feldmann D, Milford DV, Jeck N, Konrad M, Landau D, Knoers NV, Antignac C, Sudbrak R, Kispert A, Hildebrandt F (2001) Mutation of BSND causes Bartter syndrome with sensorineural deafness and kidney failure. Nat Genet 29(3):310–314
Estevez R, Boettger T, Stein V, Birkenhager R, Otto E, Hildebrandt F, Jentsch TJ (2001) Barttin is a Cl- channel beta-subunit crucial for renal Cl- reabsorption and inner ear K+ secretion. Nature 414(6863):558–561
Schlingmann KP, Konrad M, Jeck N, Waldegger P, Reinalter SC, Holder M, Seyberth HW, Waldegger S (2004) Salt wasting and deafness resulting from mutations in two chloride channels. N Engl J Med 350(13):1314–1319
Doupnik CA, Davidson N, Lester HA (1995) The inward rectifier potassium channel family. Curr Opin Neurobiol 5(3):268–277
Bockenhauer D, Feather S, Stanescu HC, Bandulik S, Zdebik AA, Reichold M, Tobin J, Lieberer E, Sterner C, Landoure G, Arora R, Sirimanna T, Thompson D, Cross JH, van’t Hoff W, Al Masri O, Tullus K, Yeung S, Anikster Y, Klootwijk E, Hubank M, Dillon MJ, Heitzmann D, Arcos-Burgos M, Knepper MA, Dobbie A, Gahl WA, Warth R, Sheridan E, Kleta R (2009) Epilepsy, ataxia, sensorineural deafness, tubulopathy, and KCNJ10 mutations. N Engl J Med 360(19):1960–1970
Scholl UI, Choi M, Liu T, Ramaekers VT, Hausler MG, Grimmer J, Tobe SW, Farhi A, Nelson-Williams C, Lifton RP (2009) Seizures, sensorineural deafness, ataxia, mental retardation, and electrolyte imbalance (SeSAME syndrome) caused by mutations in KCNJ10. Proc Natl Acad Sci U S A 106(14):5842–5847
Janer A, van Karnebeek CD, Sasarman F, Antonicka H, Al Ghamdi M, Shyr C, Dunbar M, Stockler-Ispiroglu S, Ross CJ, Vallance H, Dionne J, Wasserman WW, Shoubridge EA (2015) RMND1 deficiency associated with neonatal lactic acidosis, infantile onset renal failure, deafness, and multiorgan involvement. Eur J Hum Genet 23(10):1301–1307
Ravn K, Neland M, Wibrand F, Duno M, Ostergaard E (2016) Hearing impairment and renal failure associated with RMND1 mutations. Am J Med Genet A 170A(1):142–147
Karet FE, Finberg KE, Nelson RD, Nayir A, Mocan H, Sanjad SA, Rodriguez-Soriano J, Santos F, Cremers CW, Di Pietro A, Hoffbrand BI, Winiarski J, Bakkaloglu A, Ozen S, Dusunsel R, Goodyer P, Hulton SA, Wu DK, Skvorak AB, Morton CC, Cunningham MJ, Jha V, Lifton RP (1999) Mutations in the gene encoding B1 subunit of H+−ATPase cause renal tubular acidosis with sensorineural deafness. Nat Genet 21(1):84–90
Smith AN, Skaug J, Choate KA, Nayir A, Bakkaloglu A, Ozen S, Hulton SA, Sanjad SA, Al-Sabban EA, Lifton RP, Scherer SW, Karet FE (2000) Mutations in ATP6N1B, encoding a new kidney vacuolar proton pump 116-kD subunit, cause recessive distal renal tubular acidosis with preserved hearing. Nat Genet 26(1):71–75
Stover EH, Borthwick KJ, Bavalia C, Eady N, Fritz DM, Rungroj N, Giersch AB, Morton CC, Axon PR, Akil I, Al-Sabban EA, Baguley DM, Bianca S, Bakkaloglu A, Bircan Z, Chauveau D, Clermont MJ, Guala A, Hulton SA, Kroes H, Li Volti G, Mir S, Mocan H, Nayir A, Ozen S, Rodriguez Soriano J, Sanjad SA, Tasic V, Taylor CM, Topaloglu R, Smith AN, Karet FE (2002) Novel ATP6V1B1 and ATP6V0A4 mutations in autosomal recessive distal renal tubular acidosis with new evidence for hearing loss. J Med Genet 39(11):796–803
Vargas-Poussou R, Houillier P, Le Pottier N, Strompf L, Loirat C, Baudouin V, Macher MA, Dechaux M, Ulinski T, Nobili F, Eckart P, Novo R, Cailliez M, Salomon R, Nivet H, Cochat P, Tack I, Fargeot A, Bouissou F, Kesler GR, Lorotte S, Godefroid N, Layet V, Morin G, Jeunemaitre X, Blanchard A (2006) Genetic investigation of autosomal recessive distal renal tubular acidosis: evidence for early sensorineural hearing loss associated with mutations in the ATP6V0A4 gene. J Am Soc Nephrol 17(5):1437–1443
Wall SM, Lazo-Fernandez Y (2015) The role of pendrin in renal physiology. Annu Rev Physiol 77:363–378
Pendred V (1896) Deaf-mutism and goitre. Lancet 148(3808):532
Pela I, Bigozzi M, Bianchi B (2008) Profound hypokalemia and hypochloremic metabolic alkalosis during thiazide therapy in a child with Pendred syndrome. Clin Nephrol 69(6):450–453
Soleimani M, Barone S, Xu J, Shull GE, Siddiqui F, Zahedi K, Amlal H (2012) Double knockout of pendrin and Na-Cl cotransporter (NCC) causes severe salt wasting, volume depletion, and renal failure. Proc Natl Acad Sci U S A 109(33):13368–13373
Yang T, Vidarsson H, Rodrigo-Blomqvist S, Rosengren SS, Enerback S, Smith RJ (2007) Transcriptional control of SLC26A4 is involved in Pendred syndrome and nonsyndromic enlargement of vestibular aqueduct (DFNB4). Am J Hum Genet 80(6):1055–1063
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they have no conflicts of interest.
Additional information
Answers
1. c; 2. a; 3. d; 4. e; 5. a
Rights and permissions
About this article

Cite this article
Phelan, P.J., Rheault, M.N. Hearing loss and renal syndromes. Pediatr Nephrol 33, 1671–1683 (2018). https://doi.org/10.1007/s00467-017-3835-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00467-017-3835-9