
Abstract
Background
Lateral pelvic lymph node (LPLN) dissection is becoming increasingly important in the treatment of advanced low rectal cancer patients. However, the surgery has several disadvantages, including its technical complexity and high risk of urinary dysfunction. Herein, we report a new technique for robotic lateral pelvic lymph node dissection for advanced low rectal cancer with emphasis on en bloc resection and inferior vesical vessel preservation.
Methods
Robotic LPLN dissection was performed in 12 consecutive patients between April 2020 and December 2021. Six surgical ports were placed in the abdomen under general anesthesia. Fascia-oriented LPLN dissection of the internal iliac region and obturator region was performed using the ureterohypogastric nerve fascia, vesicohypogastric fascia, and internal obturator muscles as anatomical landmarks. Lymph nodes were resected en bloc via the caudal side of the inferior vesical vessels. The inferior vesical vessels were spared to prevent urinary dysfunction.
Results
The median patient age was 62 years (range, 43–82 years), and eight patients were male. The median operative time was 498 min (range, 424–661 min), the median bleeding volume was 56 ml (range, 13–467 ml), and the median number of harvested LPLN was 16 (range, 1–70). The conversion rate to open surgery was 0%. Clavien–Dindo Grade ≥ II urinary dysfunction rated was not observed.
Conclusion
A new technique for robotic LPLN dissection for advanced low rectal cancer with emphasis on en bloc resection and inferior vesical vessel preservation can be safely performed, making it a promising surgical procedure.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Lateral pelvic lymph node (LPLN) metastasis occurs in 13.9–20.1% of advanced low rectal cancer patients [1,2,3]. Treatment for advanced low rectal cancer differs between Eastern and Western countries. In Eastern countries, especially in Japan, the standard therapy is total mesorectal excision (TME) and LPLN dissection [3]. The addition of LPLN dissection to TME was found to significantly decrease local recurrence from 13 to 7% (P = 0.02) in the JCOG0212 study, a joint multicenter randomized controlled trial conducted in Japan [4]. Meanwhile, TME plus neoadjuvant chemoradiotherapy (CRT) is the gold standard treatment for advanced low rectal cancer in Europe and America. This is based on reports that local recurrence rates are reduced when CRT is combined with TME [5, 6]. However, a certain percentage of patients treated by TME and CRT experience lateral local recurrence [7, 8]. Thus, the importance of LPLN dissection is gradually gaining recognition. A recent multicenter study of low rectal cancer patients showed that adding LPLN dissection to TME significantly reduced the 5-year lateral local recurrence rate of nodes having pre-CRT short-axis diameter ≥ 7 mm from 19.5 to 5.7% [9].
However, the complex anatomy of the deep pelvis presents a major technical obstacle to LPLN dissection [10]. Conventional surgical approaches for LPLN dissection include open and laparoscopic procedures. Robotic surgery that has superior operability deep in the pelvic cavity owing to its greater range of motion, three-dimensional view, and rock-stable tractions has also been introduced in recent years. This modality has achieved excellent short-term outcomes [11]. Our team performs robotic LPLN dissection by specifying the surgical field with respect to the pelvic fasciae [12]. Moreover, reports have highlighted a need to resect all lymph nodes en bloc to achieve cure [13]. We believe that resecting the lymph nodes of the obturator region en bloc with, not separately from, those of the internal iliac region also offers an oncological advantage in LPLN dissection. Furthermore, our procedure preserves the inferior vesical vessels given the high risk of postoperative urinary dysfunction originating from the complex anatomy of the pelvic autonomic nerves surrounding these vessels.
The purpose of this study was to clarify the efficacy and safety of a new technique for robotic lateral pelvic lymph node dissection for advanced low rectal cancer with emphasis on en bloc resection and inferior vesical vessel preservation.
Materials and methods
Study design and patients
This single-center retrospective study included 12 clinical stage III patients with advanced rectal cancer in the low rectum who had undergone TME and LPLN dissection after neoadjuvant chemotherapy at Tokyo Medical University Hospital between April 2020 and December 2021. CRT was not performed as a preoperative treatment. Low rectal cancer was defined as located within 60-mm distance from the anal verge, histologically diagnosed as adenocarcinoma. One patient who had multiorgan cancer was excluded.
This study was approved by the Tokyo Medical University Ethics Committee (approval no. T20-0054). Informed consent was obtained from all patients after explaining the procedure.
Surgical technique
Under general anesthesia, six ports are implanted in the abdominal region, centered around a camera port in the umbilical region (Fig. 1). The procedure begins with the patient in the Trendelenburg position. Once TME is completed, the internal iliac region lymph nodes are dissected first, followed by the obturator region lymph nodes.

Positions of the six surgical ports implanted in the abdomen; R robotic port, C camera port, A assistant port
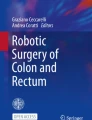
Understanding the anatomy of the fasciae that bound the dissection range is crucial for accurate LPLN dissection. For reference, we define the ureterohypogastric nerve fascia as the fascia enclosing the ureter and hypogastric nerve [14] and the vesicohypogastric fascia as the fascia enclosing the branch of the internal iliac artery supplying the bladder [15]. Lymph nodes are dissected from the internal iliac region present between these two structures. Next, the lymph nodes in the obturator region are dissected. It is crucial to ensure that all lymph nodes present between the vesicohypogastric fascia and internal obturator muscle are dissected. Normally, lymph nodes in these two regions are dissected independently. However, given their high risk of metastasis, we contend that relocating the lymph nodes on the distal side of the internal iliac region to the obturator region via the caudal side of the inferior vesical vessels first (Fig. 2). Then, they are dissected en bloc without separation (Fig. 3) to achieve greater oncological advantage. The inferior vesical vessels are spared, in principle, to avoid urinary dysfunction and prioritize blood supply to the bladder. However, if a metastatic lymph node is present in the vicinity, the closest of the several inferior vesical vessels is resected to prioritize oncological curability. A detailed demonstration of the surgical technique can be viewed in the accompanying video.

Left lateral pelvic region. Once dissected loose, the lymph nodes in the internal iliac region are relocated to the obturator region via the caudal side of the inferior vesical vessels. LPLN dissection is then performed en bloc. To prevent urinary dysfunction, the inferior vesical vessels are spared

Lymph nodes in the internal iliac region are resected en bloc with those in the obturator region, instead of separately, because the metastasis risk is greatest in the distal side of the internal iliac region
Results
The median age of the patients was 62 years (range, 43–82 years), and eight patients were male. The median operative time was 498 min (range, 424–661 min); median bleeding volume, 56 ml (range, 13–467 ml); and median number of harvested LPLN, 16 (range, 1–70). The conversion rate to open surgery was 0%. Clavien–Dindo Grade ≥ II urinary dysfunction was not observed. Ileus was the only Clavien–Dindo Grade II intraoperative or postoperative complication, and only 1 patient was affected (8.3%). No surgery-related or in-hospital deaths occurred.
Discussion
We developed this technique with the aim of improving oncological curability and preserving urinary function. Our surgical technique is based on three key concepts. The first is fascia-oriented dissection [12]. The ureterohypogastric nerve fascia and vesicohypogastric fascia are useful landmarks for determining the lymph node dissection range. Early identification of these structures allows surgeons to dissect LPLNs rapidly and thoroughly. If the unique rock-stable tractions of the robotic system are continuously maintained between the fascia and adipose tissue containing the lymph node(s), loose connective tissue can be cut away easily deep into the pelvic cavity without serious bleeding.
The second key concept is en bloc LPLN dissection. The location of LPLNs can be subdivided into six regions: the aortic bifurcation area, common iliac area, internal iliac areas proximal and distal to superior vesical artery, obturator area, and external iliac area [16]. En bloc resection without separating the lymph nodes of the internal iliac region and obturator region—corresponding to the internal iliac area proximal and distal to superior vesical artery and obturator area [16]—is a vital component of our approach, conferring survival benefit because these regions are at greatest risk of LPLN metastasis. Open LPLN dissection makes it difficult to get a good surgical view of the deep pelvic cavity. Although laparoscopic LPLN dissection permits a magnifying view, en bloc resection is difficult to perform using laparoscopic forceps as they can only be manipulated by linear movements. In contrast, robotic LPLN dissection permits en bloc resection of the lymph nodes of the internal iliac region, instead of separately from, those of the obturator region, connected on the caudal side of the inferior vesical vessels located in the deepest part of the pelvic cavity. Robotic surgery provides operators with a three-dimensional view to perceive depth to identify 3D structures. The articulated robotic arms offer them superior handling in the narrow spaces of the deep pelvic cavity.
Finally, the third key concept is preservation of the inferior vesical vessels. Resecting the inferior vesical vessels allows easier en bloc resection [17]. However, preserving them is expected to reduce the risk of urinary dysfunction because doing so also spares the pelvic autonomic nerves, as branches of the pelvic splanchnic trunk and pelvic plexus run through the periphery of the inferior vesical vessels [15]. Once intraoperative bleeding occurs, it becomes difficult for operators to correctly identify the dissection layer. Losing their anatomical orientation can lead to further accidental bleeding and complicate the preservation of the inferior vesical vessels. The efficient use of the robotic range of motion allows the area to be dissected sensitively, despite diverse variation in vascular vessels in the deep pelvic cavity. Thus, the inferior vesical vessels can be safely preserved. However, when a metastatic lymph node is present in the area, as in the case shown in our demonstration video, the operator should resect one of the several inferior vesical vessels present to prioritize oncological curability. Our study’s findings are equivalent or superior to those previously reported for robotic LPLN dissection, that is, the median number of harvested LPLN ranged from 6 to 15, and the incidence of urinary dysfunction ranged from 7.1 to 15% [18,19,20].
Our preliminary results show acceptable intraoperative and postoperative outcomes and intact urinary function. However, our study has some limitations, including the small case size and single-institution design. Additionally, long-term oncological outcomes could not be examined, and sexual function was not evaluated. The effect of the procedure on urinary function should be verified in further investigations. In addition, the oncological utility of en bloc resection should be investigated in multicenter prospective studies with larger cohorts.
In conclusion, our new technique for robotic lateral pelvic lymph node dissection with emphasis on en bloc resection and inferior vesical vessel preservation is safe and is thus a promising surgical procedure for the treatment of advanced low rectal cancer.
References
Sugihara K, Kobayashi H, Kato T, Mori T, Mochizuki H, Kameoka S, Shirouzu K, Muto T (2006) Indication and benefit of pelvic sidewall dissection for rectal cancer. Dis Colon Rectum 49:1663–1672
Ueno M, Oya M, Azekura K, Yamaguchi T, Muto T (2005) Incidence and prognostic significance of lateral lymph node metastasis in patients with advanced low rectal cancer. Br J Surg 92:756–763
Hashiguchi Y, Muro K, Saito Y, Ito Y, Ajioka Y, Hamaguchi T, Hasegawa K, Hotta K, Ishida H, Ishiguro M, Ishihara S, Kanemitsu Y, Kinugasa Y, Murofushi K, Nakajima TE, Oka S, Tanaka T, Taniguchi H, Tsuji A, Uehara K, Ueno H, Yamanaka T, Yamazaki K, Yoshida M, Yoshino T, Itabashi M, Sakamaki K, Sano K, Shimada Y, Tanaka S, Uetake H, Yamaguchi S, Yamaguchi N, Kobayashi H, Matsuda K, Kotake K, Sugihara K, Japanese Society for Cancer of the Colon and Rectum (2020) Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2019 for the treatment of colorectal cancer. Int J Clin Oncol. 25:1–42
Fujita S, Mizusawa J, Kanemitsu Y, Ito M, Kinugasa Y, Komori K, Ohue M, Ota M, Akazai Y, Shiozawa M, Yamaguchi T, Bandou H, Katsumata K, Murata K, Akagi Y, Takiguchi N, Saida Y, Nakamura K, Fukuda H, Akasu T, Moriya Y, Colorectal Cancer Study Group of Japan Clinical Oncology Group (2017) Mesorectal excision with or without lateral lymph node dissection for clinical stage II/III lower rectal cancer (JCOG0212): a multicenter, randomized controlled, noninferiority trial. Ann Surg. 266:201–207
Kapiteijn E, Marijnen CA, Nagtegaal ID, Putter H, Steup WH, Wiggers T, Rutten HJ, Pahlman L, Glimelius B, van Krieken JH, Leer JW, van de Velde CJ, Dutch Colorectal Cancer Group (2001) Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med 345:638–646
Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, Martus P, Tschmelitsch J, Hager E, Hess CF, Karstens JH, Liersch T, Schmidberger H, Raab R, German Rectal Cancer Study Group (2004) Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351:1731–1740
Kim NK, Kim MJ, Park JK, Park SI, Min JS (2000) Preoperative staging of rectal cancer with MRI: accuracy and clinical usefulness. Ann Surg Oncol 7:732–737
Kim TG, Park W, Choi DH, Park HC, Kim SH, Cho YB, Yun SH, Kim HC, Lee WY, Lee J, Park JO, Park YS, Lim HY, Kang WK, Chun HK (2014) Factors associated with lateral pelvic recurrence after curative resection following neoadjuvant chemoradiotherapy in rectal cancer patients. Int J Colorectal Dis 29:193–200
Ogura A, Konishi T, Beets GL, Cunningham C, Garcia-Aguilar J, Iversen H, Toda S, Lee IK, Lee HX, Uehara K, Lee P, Putter H, van de Velde CJH, Rutten HJT, Tuynman JB, Kusters M, Lateral Node Study Consortium (2019) Lateral nodal features on restaging magnetic resonance imaging associated with lateral local recurrence in low rectal cancer after neoadjuvant chemoradiotherapy or radiotherapy. JAMA Surg. 154:e192172
Ogura A, Konishi T, Cunningham C, Garcia-Aguilar J, Iversen H, Toda S, Lee IK, Lee HX, Uehara K, Lee P, Putter H, van de Velde CJH, Beets GL, Rutten HJT, Kusters M, Lateral Node Study Consortium (2019) Neoadjuvant (chemo)radiotherapy with total mesorectal excision only is not sufficient to prevent lateral local recurrence in enlarged nodes: Results of the multicenter lateral node study of patients with low cT3/4 rectal cancer. J Clin Oncol. 37:33–43
Kim HJ, Choi GS, Park JS, Park SY, Lee HJ, Woo IT, Park IK (2018) Selective lateral pelvic lymph node dissection: a com- parative study of the robotic versus laparoscopic approach. Surg Endosc 32:2466–2473
Matsumoto A, Arita K (2017) A technique of laparoscopic lateral pelvic lymph node dissection based on vesicohypogastric fascia and ureterohypogastric nerve fascia for advanced low rectal cancer. Surg Endosc 31:945–948
Lynch ML, Brand MI (2005) Preoperative evaluation and oncologic principles of colon cancer surgery. Clin Colon Rectal Surg 18:163–173
Kinugasa Y, Murakami G, Suzuki D, Sugihara K (2007) Histological identification of fascial structures posterolateral to the rectum. Br J Surg 94:620–626
Yabuki Y, Sasaki H, Hatakeyama N, Murakami G (2005) Discrepancies between classic anatomy and modern gynecologic surgery on pelvic connective tissue structure: harmonization of those concepts by collaborative cadaver dissection. Am J Obstet Gynecol 193:7–15
Kanemitsu Y, Komori K, Shida D, Ochiai H, Tsukamoto S, Kinoshita T, Moriya Y (2017) Potential impact of lateral lymph node dissection (LLND) for low rectal cancer on prognoses and local control: A comparison of 2 high-volume centers in Japan that employ different policies concerning LLND. Surgery 162:303–314
Nakamura T, Watanabe M (2013) Lateral lymph node dissection for lower rectal cancer. World J Surg 37:1808–1813
Peacock O, Limvorapitak T, Bednarski BK, Kaur H, Taggart MW, Dasari A, Holliday EB, Minsky BD, You YN, Chang GJ (2020) Robotic lateral pelvic lymph node dissection after chemoradiation for rectal cancer: a Western perspective. Colorectal Dis 22:2049–2056
Song SH, Choi GS, Kim HJ, Park JS, Park SY, Lee SM, Choi JA, Seok HA (2021) Long-term clinical outcomes of total mesorectal excision and selective lateral pelvic lymph node dissection for advanced low rectal cancer: a comparative study of a robotic versus laparoscopic approach. Tech Coloproctol 25:413–423
Morohashi H, Sakamoto Y, Miura T, Kagiya T, Ogasawara K, Takahashi Y, Sato K, Hara Y, Ogasawara H, Hakamada K (2021) Short-term outcomes of robotic-assisted laparoscopic versus laparoscopic lateral lymph node dissection for advanced lower rectal cancer. Surg Endosc 35:5001–5008
Acknowledgements
We would like to thank Editage (https://www.editage.jp) for English language editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
Study conception and design: TI, ME, and KK; Data acquisition: TI and JM; Data interpretation: TI, RU, TT, KK, and HK; Drafting the manuscript: TI; Supervision of the manuscript: YN; Critical review and approval of the manuscript: TI and JM.
Corresponding author
Ethics declarations
Disclosures
All the authors (Tetsuo Ishizaki, Junichi Mazaki, Masanobu Enomoto, Ryutaro Udo, Tomoya Tago, Kenta Kasahara, Hiroshi Kuwabara, Kenji Katsumata, Yuichi Nagakawa) declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file1 (MP4 958636 KB)
Rights and permissions
About this article

Cite this article
Ishizaki, T., Mazaki, J., Enomoto, M. et al. A new technique for robotic lateral pelvic lymph node dissection for advanced low rectal cancer with emphasis on en bloc resection and inferior vesical vessel preservation. Surg Endosc 36, 7789–7793 (2022). https://doi.org/10.1007/s00464-022-09275-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-022-09275-x