
Abstract
Background
Considering the increase in overall life expectancy and the rising incidence of hepatocellular carcinoma (HCC), more elderly patients are considered for hepatic resection. Traditionally, major hepatectomy has not been proposed to the elderly due to severe comorbidities. Indeed, only a few case series are reported in the literature. The present study aimed to compare short-term and long-term outcomes between laparoscopic major hepatectomy (LMH) and open major hepatectomy (OMH) in elderly patients with HCC using propensity score matching (PSM).
Methods
We performed a multicentric retrospective study including 184 consecutive cases of HCC major liver resection in patients aged ≥ 70 years in _8 European Hospital Centers. Patients were divided into LMH and OMH groups, and perioperative and long-term outcomes were compared between the 2 groups.
Results
After propensity score matching, 122 patients were enrolled, 38 in the LMH group and 84 in the OMH group. Postoperative overall complications were lower in the LMH than in the OMH group (18 vs. 46%, p < 0.001). Hospital stay was shorter in the LMH group than in the OMH group (5 vs. 7 days, p = 0.01). Mortality at 90 days was comparable between the two groups. There were no significant differences between the two groups in terms of overall survival (OS) and disease-free survival (DFS) at 1, 3, and 5 years.
Conclusion
LMH for HCC is associated with appropriate short-term outcomes in patients aged ≥ 70 years as compared to OMH. LMH is safe and feasible in elderly patients with HCC.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Hepatocellular carcinoma (HCC) is the most frequent primitive malignant liver tumor, the third leading cause of cancer-related death and the fifth most common type of cancer worldwide [1,2,3].
The management of HCC is rapidly evolving with the advent of new locoregional therapies. However, surgical resection remains the curative treatment due to the current donor shortage in liver transplantation [4, 5].
Since the first laparoscopic wedge resection reported by Reich [6] and the first laparoscopic anatomical liver resection reported by Azagra [7] and Kaneko [8], laparoscopic liver resection (LLR) has been progressively developed, acquiring safety and feasibility [9].
The indications for LLR have been changed substantially with improved laparoscopic techniques. Initially cirrhotic patients were considered a contraindication because cirrhosis made hepatectomy more complex and increased the risk of developing significant postoperative complications. However, nowadays minimally invasive approach has allowed improved postoperative outcomes [10,11,12,13]. Most published studies focus on cirrhotic patients undergoing minor laparoscopic resections, whereas data can rarely be found in the literature for major laparoscopic resections [2].
During the Second International Consensus Conference for Laparoscopic Liver Resection held in Morioka, laparoscopic minor hepatectomy was considered a standard surgical practice, while laparoscopic major hepatectomy was considered in its "exploration" phase since still associated with risks [14].
Progress in laparoscopic major hepatectomy (LMH) has been very slow worldwide but several centers have reported good results after this approach [15, 16].
Advances in surgical techniques and perioperative care have extended the indications for liver resection, especially in older patients requiring major hepatectomy for malignant disease [17].
Considering the increasing life expectancy, the percentage of elderly patients with HCC who will undergo surgery will continue to increase in the future. However, there are insufficient data in the literature to confirm that this approach is safe and feasible in elderly patients.
To date, only a few studies have focused on the potential benefits of laparoscopy in elderly patients requiring liver resection and even fewer studies have focused on the results of LMH in this group of patients specifically [16, 18].
The aim of our study was to evaluate the short- and long-term outcomes of LMH versus open major hepatectomy (OMH) for the treatment of HCC in elderly patients.
Materials and methods
Patient data
We performed a multicentric retrospective study including 184 consecutive cases of HCC liver resection in patients aged ≥ 70 years in 8 European Hospital Centers from January 2009 to January 2019. Centers enrolled were the following: IRCCS San Raffaele Hospital, Milan, Italy; Paul Brousse University Hospital, Villejuif, France; University Hospital Reina Sofía, Córdoba, Spain; Henri Mondor University Hospital, Créteil, France; University Hospital Policlinico of Modena, Modena, Italy; Miulli Hospital, Bari, Italy; Robert Debré University Hospital, Reims, France; Strasbourg University Hospital, IRCAD, Strasbourg, France.
Patients were divided into LMH and OMH groups according to the surgical approach performed.
The laparoscopic group was randomly matched with the open group using a 1-to-many matching of propensity scores.
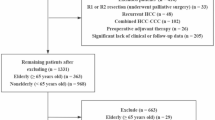
Preoperative, intraoperative, and postoperative data were retrospectively analyzed and compared in both groups. Patients < 70 years of age, with ASA > IV, re-hepatectomy, and R2 resection were excluded from our study. Each center received IRB approval to collect individual patient clinical data.
Preoperative assessment
Patient demographic data and preoperative variables were collected. Patients underwent conventional hemograms and liver function tests, i.e., serum α-fetoprotein (AFP), platelets, bilirubin, coagulation and creatinine.
Preoperative assessment also included the evaluation of surgical risks (ASA score), comorbidities, the presence of portal hypertension, the cause of cirrhosis, the calculation of Child–Pugh and model for end-stage liver disease (MELD) scores.
All patients were staged preoperatively following computer tomography of chest, abdomen, and pelvis, and/or abdominal magnetic resonance, and were discussed in a multidisciplinary team.
Preoperative diagnosis was based on the non-invasive criteria established by the European Association for the study of the Liver (EASL) [19]. Biopsy was used only in the event of inconclusive diagnosis. The number, location, and size of liver nodules were recorded.
All patients received prophylactic antibiotic therapy as well as anticoagulation with low-molecular weight heparin to prevent deep vein thrombosis.
Perioperative assessment
The surgical procedure was performed by expert surgeons with consolidated experience in open liver surgery and advanced laparoscopic surgery and with at least 30 to 60 cases of major liver resections having already developed experience on minor resections. There was a similar management in all centers. The Couinaud classification was used to define liver segmentation and the Brisbane 2000 nomenclature was used to define liver resections [20, 21]. Major hepatectomy was defined when three or more liver segments were removed. An intraoperative Doppler ultrasound was systematically performed to confirm the number and size of the lesions, to search for non-visible lesions, and to define the resection type. Different types of device were used for parenchymal liver transection such as electrocoagulation, ultrasound, radiofrequency or combined energy.
The Pringle maneuver was routinely prepared and used according to the experience of each center.
Postoperative complications were classified according to the Clavien–Dindo grading system [22].
Ninety-day mortality was defined as any death occurring within 90 days from surgery and was considered operative mortality.
The histological examination of the resected specimen analyzed the resection margin width and R0 resection was defined if the neoplasm was more than 1 mm from the resection margin.
Long-term outcomes
A standardized follow-up was adopted, i.e., every four months for the first two years and then every six months. The patients underwent a blood testing including alpha-fetoprotein (AFP) measurement, liver function tests and imaging as well as abdominal ultrasonography, CT, or MRI.
All HCC-related deaths and recurrences were estimated and used to calculate the overall and disease-free survival analyzed in both groups.
Statistical analysis
A propensity score-based analysis was performed to limit selection bias and reduce confusion arising from lack of randomization. The propensity score was estimated using a one-to-many logistic regression regarding the following variables: gender, comorbidity, ASA score, Child–Pugh score, number of tumors, and size of tumors.
All variables were compared before (b-PSM) and after propensity score matching (a-PSM). The Mann–Whitney U test was used for continuous variables expressed as median (range). Instead, the Chi-square test was used for categorical data, presented as numbers with percentages.
Overall survival and disease-free survival were estimated using the Kaplan–Meier method and compared using a log-rank test. A p value of < 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS version 20 software.
Results
Preoperative outcomes b-PSM and a-PSM
Preoperative characteristics of the open and laparoscopic groups are presented in Table 1. During the study period, 184 patients were enrolled and divided into two groups according to the surgical technique performed. Among these, 144 patients were managed with open liver resection and 40 were managed with the laparoscopic approach. After propensity score matching, 84 patients of the open group and 38 patients of the laparoscopic group were compared in each group.
There were no significant differences in sex, age, and BMI between the two groups. The number of comorbidities was higher in the laparoscopic group b-PSM; however, for a-PSM, there was no difference between the two groups. International normalized ration (INR) was statistically lower in the laparoscopic group both before and after PSM. The Child–Pugh score was comparable in each group. Conversely, the MELD score was lower in the laparoscopic group b-PSM and equal between the two groups a-PSM. Patients in the laparoscopic group had a major number of tumors in accordance with the Milan criteria, and this was confirmed even a-PSM. The tumor size of the biggest lesion was lower in the laparoscopic group only b-PSM. Conversely, for a-PSM there was no difference between the two groups. In the open group, it was more necessary to perform a preoperative biopsy both before and after PSM. Patients undergoing laparoscopic surgery had a lower rate of previous abdominal treatments both before and after PSM.
Perioperative outcomes b-PSM and a-PSM
Perioperative characteristics of the open and laparoscopic groups are presented in Table 2. There was a different distribution of hepatectomy types between the two groups only b-PSM (p = 0.03). Operative time was comparable between the two groups both before and after PSM. Intraoperative blood transfusion was significantly lower in the LLR group than in the OLR group (p = 0.03) b-PSM. Conversely, for a-PSM there was no more difference (p = 0.10).
The use of the Pringle maneuver was comparable in each groups both before and after PSM.
Overall postoperative complications were significantly lower in the LLR group than the OLR group, and this was also confirmed in matched groups (p < 0.001).
Major complication rates, i.e., Clavien–Dindo grades III-IV, were significantly lower in the LLR b-PSM group (p = 0.03). After restricting the analysis to propensity score matching, there was no difference between the two groups. A median of hospital stay was significantly shorter in the LLR group than in the OLR group (p < 0.001). The same result was shown in matched groups (p = 0.01).
R0 resection was achieved more in the LLR group than in the OLR group (p = 0.02). Conversely, for a-PSM there was no difference between the two groups. Ninety-day mortality was comparable between the two groups both before and after PSM.
Long-term outcomes b-PSM and a-PSM
Overall survival (OS) and disease-free survival (DFS) were calculated before and after propensity score matching according to the surgical approach performed (Fig. 1). There were no statistically significant differences between each group in terms of OS (b-PSM p = 0.12; a-PSM p = 0.37) and DFS (b-PSM p = 0.78; a-PSM p = 0.33) considering a follow-up of 5 years.

Overall (OS) and disease-free survival (DFS) after laparoscopic major hepatectomy versus open major hepatectomy in elderly patients for hepatocellular carcinoma before (b-PSM) and after propensity score matching (a-PSM). A OS b-PSM; Log Rank (Mantel Cox) = 0.12 B OS a-PSM; Log Rank (Mantel Cox) = 0.38 C DFS b-PSM; Log Rank (Mantel Cox) = 0.78 D DFS a-PSM; Log Rank (Mantel Cox) = 0.33
The median OS b-PSM was 21.3 months in the LLR group and 42.9 months in the OLR group. In the LLR group, the 1-, 3-, and 5-year OS rates b-PSM were 100, 100, and 80%, respectively, as compared to 91, 81, and 73% in the OLR group, respectively.
The median OS a-PSM was 21.3 months in the LLR group and 51.9 months in the OLR group. In the LLR group, the 1-, 3-, and 5-year OS rates were 100, 100, and 77%, respectively, as compared to 95, 88, and 75% in the OLR group, respectively.
The median DFS b-PSM was 11.8 months in the LLR group and 19.9 months in the OLR group. DFS b-PSM at 1-, 3-, and 5 years was 66, 46, and 35% in the LLR group and 76, 51, and 44% in the OLR group, respectively.
The median DFS a-PSM was 11.8 months in the LLR group and 24.5 months in the OLR group. DFS at 1-, 3-, and 5 years was 67, 44, and 29% in the LLR group and 79, 54, and 46% in the OLR group, respectively.
Discussion
To our knowledge, our study represents one of the few series reported in the literature that aims to compare LMH and OMH in elderly patients with HCC.
The old definition of elderly people concerns patients aged over 65 years, but thanks to the improvement in medical care, life expectancy has increased in the elderly. Consequently, the cut-off definition for the elderly population has moved from > 65 years to 70 or 75 years [23].
Elderly patients, defined as fragile, have numerous comorbidities, lower functional reserve, and are characterized by a postoperative high morbidity and mortality rate as compared to younger patients. In general, a morbidity rate of 20% and mortality of 6% have been reported for patients over 70 years of age, with an increase in these rates according to age [16, 24, 25]. Despite of this, surgical resection remains the first-line treatment available with a curative intention for the elderly, due to the age limit overpassed for liver transplantation [26].
There is an increasing number of elderly patients with hepatobiliary tumors requiring major liver resection, this surgical procedure was more frequently performed for multifocal or large HCC and allowed for an adequate resection margin, reducing intrahepatic recurrence. While the safety and feasibility of major hepatectomy in elderly patients has been specifically address, the value of the laparoscopic approach in this setting or in other special clinical populations, such as patients with cirrhosis remains unclear [23, 26,27,28].
In the Second International Consensus Conference for laparoscopic liver resection held in Morioka, laparoscopic minor hepatectomy was considered a standard surgical care. Indeed, several previous studies had already shown that laparoscopic hepatectomy can be feasible for minor, non-anatomical resections, and left lateral sectionectomy. On the other hand, laparoscopic major hepatectomy was considered in its “exploration” phase because it was still associated with high risks [14, 30, 31].
The first major hepatectomy performed laparoscopically was reported by Huscher et al. in 1998 [32].
The progress of LMH has been very slow worldwide due to the technical difficulties with a steep learning curve and the need for experience both in advanced laparoscopic surgery and in hepatobiliary surgery, especially in cirrhotic patients [15, 33, 34]. Advances in laparoscopic devices and experience have gradually expanded the use of LMH in several centers that have reported good results after this approach [15, 16].
During the first European Guidelines Meeting on Laparoscopic Liver Surgery, held in Southampton in 2017, the expert panel highlighted the difference in difficulty and results between left and right laparoscopic hepatectomy. The guidelines also state that the advantages of LMH as compared to OMH can be achieved if the procedure has been performed by expert hands [35].
Several previous studies have shown that minimally invasive techniques guarantee favorable perioperative results, such as lower intraoperative blood loss, shorter hospital stay, and lower postoperative morbidity, for benign and malignant diseases in elderly patients as compared to open hepatectomy. However, there are still limited data available for the use of laparoscopy in elderly patients for major liver resection and these data need to be clarified with new results originating from an improved experience [24].
Our study shows that major liver resections are feasible even in elderly patients and that the laparoscopic approach ensures a better postoperative course.
The progress of laparoscopic liver resection has been progressively developed acquiring safety and feasibility and this was also evidenced in our study, as confirmed by the increasing number of LMHs performed since 2009 (Fig. 2).

Distribution of laparoscopic major hepatectomy (LMH) and open major hepatectomy (OMH) for hepatocellular carcinoma in elderly cirrhotic patients from 2009 to 2019
In our work, the majority of laparoscopic cases have been performed in recent years, with the improvement of surgical technique and pre, peri- and postoperative care, which could potentially have a positive impact on the outcome of the laparoscopic cohort and could represent a limitation of our work.
The year distribution of hepatic resection also showed a reduction in the total number of major liver resections this is in according to parenchymal sparing concept.
Parenchymal sparing surgery has been championed especially for colorectal metastases [36] but several groups have reported that this is a valid technique also for HCC because it is less invasive with surgical and oncological outcomes comparable with those of major hepatectomy [37, 38].
In laparoscopic group, there are a greater number of tumors within Milan criteria, but in our opinion, this does not reduce the superiority of laparoscopic approach because we have compared two groups for kind of surgical technique and not for kind of tumor and we have used a-PSM to make homogeneous the two groups.
In our study, there was no statistically significant difference in operative time between the two groups even after restricting the analysis with propensity score matching. This is corroborated by a recent meta-analysis and a multicentric study [16, 24], which show how the development of surgical instruments and the accumulation of surgical experience and skills have played a key role in reducing operative times for laparoscopic liver resection [39]. This confirms that major liver resections should be attempted only once significant experience in laparoscopic liver resections has been achieved [16]. Conversely, others series showed a higher operative time for LMH because this technique is still being investigated and learned. This is explained by a time-consuming approach to technical difficulties such as liver mobilization, vessel and duct isolation, bleeding control, inability to perform manual palpation and work with the deeper regions of the liver [30, 40, 41].
Our study showed that the two groups had also a comparable rate of blood transfusion a-PSM according to recent studies [15, 40]; however, many authors [24, 30] reported a reduction in blood loss volume in the laparoscopic group. This is explained by the hemostatic effect of the pneumoperitoneum and the magnified view which allowed a precise identification of blood vessels in addition to the development of devices which allow bleeding control [40]. Intraoperative bleeding, and the subsequent need for blood transfusion and fluid infusion have been identified as a risk factor for postoperative morbidity and long-term survival [42, 43]. The inconsistency in reporting blood transfusion rates in different centers may justify the heterogeneity documented in our study, as a result, it cannot be excluded that laparoscopy confers advantages in terms of blood loss and transfusion rate for major liver resections.
Overall postoperative complications were significantly lower in the LMH group than in the OMH group and this benefit persisted even after restricting the analysis to propensity score matching. This is also confirmed by Chen [24] and Komatsu [15].
Conversely, major complication rates, i.e., Clavien–Dindo grades III-IV, were comparable between the two groups a-PSM, and this is also corroborated by many authors [15, 16].
Major liver-related complications such as liver failure, liver dysfunction, and ascites, have not been significantly different, because those complications are much more related to the volume of liver resected and background liver characteristics than to the surgical approach [41]. Generally, laparoscopic surgery allows for a lower abdominal incision with preservation of the venous collateral circulation including the round ligament and the lymphatic flow of the diaphragm, hence reducing the risk of refractory ascites and subsequent potential liver failure [30, 44].
We did not identify any difference in the rate of cardiopulmonary complications between LMH and OMH, and this is corroborated by Chen et al. [24]; however, other authors showed a lower rate of cardiopulmonary complications in the laparoscopic group [16, 45].
Kim et al. [46] reported a high incidence of postoperative pneumonia in older patients because they have a greater predisposition for this complication due to lung structure changes with loss of collagen and parenchyma elasticity.
In accordance with data published in the literature [16, 24, 30], the laparoscopic group, b- and a-PSM, showed a lower hospital stay as compared to the open group. Elderly patients benefit from a quick return to daily activities and they need a postoperative functional recovery with a period of rehabilitation before discharge from hospital as compared to young patients [47].
Conversely, Komatsu [15] and Xu [2] showed that hospital stay is similar between the laparoscopic group and the open group. Menon et al. [48] analyzed outcomes after major hepatectomy between elderly and young patients and showed a similar hospital stay between the two groups.
An appropriate surgical margin is a crucial step in radical hepatic surgery. In our study, R0 resection was comparable between the two groups also after restricting the analysis to propensity score matching, this finding is supported by a recent meta-analysis and a propensity score matching study [2, 24]. In major liver resections, regardless of the surgical technique, a negative margin is more likely to be achieved as there is a greater volume of resected liver than minor or non-anatomic hepatectomy [30]. A precise intraoperative tumor localization is essential in the laparoscopic approach, as a direct tactile evaluation of the liver is not possible. To overcome this limitation, the use of intraoperative ultrasound is recommended by international consensus conferences to improve tumor detection [14, 24, 33].
The rate of mortality at 90 days was comparable between the two groups, and this is also confirmed by many authors [16, 40, 49, 50].
In our study, overall survival (OS) and disease-free survival (DFS) had no statistically significant difference between the two groups b-PSM and a-PSM, and this is in accordance with the literature [29, 36, 47,48,49].
The curve has a steeper trend at exactly 36 months in the laparoscopic group, this may be due to the lower number of patients and a shorter follow-up of the laparoscopic group compared to the open group.
Our work has shown high OS and low DSF at 5 years in both groups, we think that the mechanisms of carcinogenesis are slower in the elderly patients, allowing higher overall survival despite lower disease-free survival. In addition, the selection of elderly patients allows to obtain good survival because patients who are considered for surgery had a certain prognostic advantage, while those who had an oncologically borderline indication and an advanced age are considered for other types of treatments than surgery.
The prognosis of patients with hepatocellular carcinoma could be extremely influenced by the biological behavior of liver tumors rather than by the surgical approach [51, 52]. In addition, there is no superiority in terms of oncological resection between the two approaches. As a result, oncological resection could be performed irrespective of the type of approach [30].
In conclusion, the current study showed than laparoscopic major hepatectomy for HCC in cirrhotic and elderly patients had better results in terms of overall morbidity and length of hospital stay and comparable results in terms of oncological outcomes as compared to the conventional open procedure. Our study revealed how the minimally invasive approach could be considered a valid technique, even in elderly and cirrhotic patients who underwent major liver hepatectomy.
References
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2015) Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. https://doi.org/10.1002/ijc.29210
Xuwei H, Liu F, Li yu H, Weigang Y, Li B (2018) Outcomes following laparoscopic versus open major hepatectomy for hepatocellular carcinoma in patients with cirrhosis: a propensity score-matched analysis. Surg Endosc. https://doi.org/10.1007/s00464-017-5727-2
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A (2015) Global cancer statistics, 2012. CA Cancer J Clin. https://doi.org/10.3322/caac.21262
Dufour JF, Greten TF, Raymond E, Roskams T, De T, Ducreux M, Mazzaferro V, Governing E (2012) Clinical practice guidelines easl—eortc clinical practice guidelines : management of hepatocellular carcinoma european organisation for research and treatment of cancer. J Hepatol. https://doi.org/10.1016/j.jhep.2011.12.001
Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, Christensen E, Pagliaro L, Colombo M, Rodés J, EASL Panel of Experts on HCC (2001) Clinical management of hepatocellular carcinoma. Conclusions of the Barcelona-2000 EASL conference. European Association for the Study of the Liver. J Hepatol
Reich H, McGlynn F, DeCaprio J, Budin R (1991) Laparoscopic excision of benign liver lesions. Obstet Gynecol
Azagra JS, Goergen M, Gilbart E, Jacobs D (1996) Laparoscopic anatomical (hepatic) left lateral segmentectomy - Technical aspects. Surg Endosc. https://doi.org/10.1007/BF00193052
Kaneko H, Takagi S, Shiba T (1996) Laparoscopic partial hepatectomy and left lateral segmentectomy: Technique and results of a clinical series. Surgery. https://doi.org/10.1016/S0039-6060(96)80065-1
Coelho FF (2016) Laparoscopic liver resection: Experience based guidelines. World J Gastrointest Surg. https://doi.org/10.4240/wjgs.v8.i1.5
Kanazawa A, Tsukamoto T, Shimizu S, Kodai S, Yamazoe S, Yamamoto S, Kubo S (2013) Impact of laparoscopic liver resection for hepatocellular carcinoma with F4-liver cirrhosis. Surg Endosc. https://doi.org/10.1007/s00464-013-2795-9
Shehta A, Han HS, Yoon YS, Cho JY, Choi YR (2016) Laparoscopic liver resection for hepatocellular carcinoma in cirrhotic patients: 10-year single-center experience. Surg Endosc. https://doi.org/10.1007/s00464-015-4253-3
Untereiner X, Cagniet A, Memeo R, Cherkaoui Z (2018) Laparoscopic Hepatectomy Versus Open Hepatectomy for the Management of Hepatocellular Carcinoma : A Comparative Study Using a Propensity Score Matching. World J Surg. https://doi.org/10.1007/s00268-018-4827-z
Soubrane O, Goumard C, Laurent A, Tranchart H, Truant S, Gayet B, Salloum C, Luc G, Dokmak S, Piardi T, Cherqui D, Dagher I, Boleslawski E, Vibert E, Sa Cunha A, Belghiti J, Pessaux P, Boelle PY, Scatton O (2014) Laparoscopic resection of hepatocellular carcinoma: A French survey in 351 patients. HPB. https://doi.org/10.1111/hpb.12142
Wakabayashi G, Cherqui D, Geller DA, Buell JF, Kaneko H, Han HS, Asbun H, O’Rourke N, Tanabe M, Koffron AJ, Tsung A, Soubrane O, Machado MA, Gayet B, Troisi RI, Pessaux P, Van Dam RM, Scatton O, Hilal MA, Belli G, Kwon CHD, Edwin B, Choi GH, Aldrighetti LA, Cai X, Cleary S, Chen KH, Schön MR, Sugioka A, Tang CN, Herman P, Pekolj J, Chen XP, Dagher I, Jarnagin W, Yamamoto M, Strong R, Jagannath P, Lo CM, Clavien PA, Kokudo N, Barkun J, Strasberg SM (2015) Recommendations for laparoscopic liver resection: A report from the second international consensus conference held in morioka. Ann Surg. https://doi.org/10.1097/SLA.0000000000001184
Komatsu S, Brustia R, Goumard C, Perdigao F, Soubrane O, Scatton O (2016) Laparoscopic versus open major hepatectomy for hepatocellular carcinoma: a matched pair analysis. Surg Endosc. https://doi.org/10.1007/s00464-015-4422-4
Cauchy F, Fuks D, Nomi T, Dokmak S, Scatton O, Schwarz L, Barbier L, Belghiti J, Soubrane O, Gayet B (2016) Benefits of Laparoscopy in Elderly Patients Requiring Major Liver Resection. J Am Coll Surg. https://doi.org/10.1016/j.jamcollsurg.2015.11.006
Dokmak S, Ftériche FS, Borscheid R, Cauchy F, Farges O, Belghiti J (2013) 2012 Liver resections in the 21st century: We are far from zero mortality. HPB. https://doi.org/10.1111/hpb.12069
Chan ACY, Poon RTP, Cheung TT, Chok KSH, Dai WC, Chan SC, Lo CM (2014) Laparoscopic versus open liver resection for elderly patients with malignant liver tumors: A single-center experience. J Gastroenterol Hepatol. https://doi.org/10.1111/jgh.12539
Galle PR, Forner A, Llovet JM, Mazzaferro V, Piscaglia F, Raoul JL, Schirmacher P, Vilgrain V (2018) EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J Hepatol. https://doi.org/10.1016/j.jhep.2018.03.019
Couinaud C (1980) Definition of hepatic anatomical regions and their value during hepatectomy. Chir - Mem l’Academie Chir
Strasberg SM (2000) Phillips C (2013) Use and Dissemination of the Brisbane. Nomenclature of Liver Anatomy and Resections 257:377–382. https://doi.org/10.1097/SLA.0b013e31825a01f6
Clavien PA, Barkun J, De Oliveira ML, Vauthey JN, Dindo D, Schulick RD, De Santibañes E, Pekolj J, Slankamenac K, Bassi C, Graf R, Vonlanthen R, Padbury R, Cameron JL, Makuuchi M (2009) The clavien-dindo classification of surgical complications: Five-year experience. Ann, Surg
Orimo H (2006) Reviewing the definition of elderly. Japanese J, Geriatr
Chen K, Pan Y, Maher H, Zhang B, Zheng X yong (2018) Laparoscopic hepatectomy for elderly patients Major findings based on a systematic review and meta-analysis. Med. (United States)
Story DA (2008) Postoperative complications in elderly patients and their significance for long-term prognosis. Curr. Opin, Anaesthesiol
Wu FH, Shen CH, Luo SC, Hwang JI, Chao WS, Yeh HZ, Jan YG, Yen Y, Bin CS, Wu CC, Lin YL, P’Eng FK (2019) Liver resection for hepatocellular carcinoma in oldest old patients. World J Surg Oncol. https://doi.org/10.1186/s12957-018-1541-0
Cheung TT, Han HS, She WH, Chen KH, Chow PKH, Yoong BK, Lee KF, Kubo S, Tang CN, Wakabayashi G (2018) The Asia Pacific Consensus Statement on Laparoscopic Liver Resection for Hepatocellular Carcinoma: A Report from the 7th Asia-Pacific Primary Liver Cancer Expert Meeting Held in Hong Kong. Liver Cancer 7:28–39. https://doi.org/10.1159/000481834
Dagher I, O’Rourke N, Geller DA, Cherqui D, Belli G, Gamblin TC, Lainas P, Laurent A, Nguyen KT, Marvin MR, Thomas M, Ravindra K, Fielding G, Franco D, Buell JF (2009) Laparoscopic major hepatectomy: An evolution in standard of care. Ann Surg. https://doi.org/10.1097/SLA.0b013e3181bcaf46
S.K. R, A.S. B, R.S. T, T.C. G, D.A. G, J.W. M, A. T, B.M. C, 2011 Major liver resection in elderly patients: A multi-institutional analysis J. Am. Coll Surg
Chen K, Pan Y, Hu GY, Maher H, Zheng XY, Yan JF (2018) Laparoscopic Versus Open Major Hepatectomy for Hepatocellular Carcinoma: A Meta-Analysis. Surg Laparosc Endosc Percutan Tech. https://doi.org/10.1097/SLE.0000000000000567
Chang S, Laurent A, Tayar C, Karoui M, Cherqui D (2007) Laparoscopy as a routine approach for left lateral sectionectomy. Br J Surg. https://doi.org/10.1002/bjs.5562
Hüscher CG, Lirici MM, Chiodini S (1998) Laparoscopic liver resections. Semin Laparosc Surg 5:204–210. https://doi.org/10.1177/155335069800500308
Buell JF, Cherqui D, Geller DA, O’Rourke N, Iannitti D, Dagher I, Koffron AJ, Thomas M, Gayet B, Han HS, Wakabayashi G, Belli G, Kaneko H, Ker C-G, Scatton O, Laurent A, Abdalla EK, Chaudhury P, Dutson E, Gamblin C, D’Angelica M, Nagorney D, Testa G, Labow D, Manas D, Poon RT, Nelson H, Martin R, Clary B, Pinson WC, Martinie J, Vauthey J-N, Goldstein R, Roayaie S, Barlet D, Espat J, Abecassis M, Rees M, Fong Y, McMasters KM, Broelsch C, Busuttil R, Belghiti J, Strasberg S, Chari RS (2008) (2009) The international position on laparoscopic liver surgery: The Louisville Statement. Ann Surg 250(5):825–830
Cheek SM, Geller DA (2016) The learning curve in laparoscopic major hepatectomy: What is the magic number? JAMA Surg.
MA Hilal ÃL Aldrighetti I Dagher S Aroori ÃÃG Belli M Besselink J Briceno B Gayet MD Hondt M Lesurtel J Santoyo O Scatton O Soubrane R Sutcliffe Dam R Van S White MC Halls ÃF Cipriani Poel M Der Van R Ciria L Barkhatov Y Gomez-luque S Ocana-garcia A Cook J Buell P Clavien C Dervenis G Fusai D Geller H Lang J Primrose ÃM Taylor Gulik T Van G Wakabayashi ÃH Asbun 2017 The Southampton Consensus Guidelines for Laparoscopic Liver Surgery. 10.1097/SLA.0000000000002524
Deng G, Li H, Jia G qing, Fang D, Tang Y yin, Xie J, Chen K fei, Chen Z yu (2019) Parenchymal-sparing versus extended hepatectomy for colorectal liver metastases: A systematic review and meta-analysis. Cancer Med.
Kobayashi K, Kawaguchi Y, Arita J, Akamatsu N, Kaneko J, Sakamoto Y, Hasegawa K, Kokudo N (2018) Parenchyma-sparing liver resection for hepatocellular carcinoma in left lateral section is associated with better liver volume recovery. HPB. https://doi.org/10.1016/j.hpb.2018.03.020
Famularo S, Di Sandro S, Giani A, Lauterio A, Sandini M, De Carlis R, Buscemi V, Romano F, Gianotti L, De Carlis L (2018) Long-term oncologic results of anatomic vs parenchyma-sparing resection for hepatocellular carcinoma. Eur J Surg Oncol A propensity score-matching analysis. https://doi.org/10.1016/j.ejso.2018.05.018
Guro H, Cho JY, Han HS, Yoon YS, Choi YR, Periyasamy M (2016) Current status of laparoscopic liver resection for hepatocellular carcinoma. Clin. Mol, Hepatol
Kasai M, Cipriani F, Gayet B, Aldrighetti L, Ratti F, Sarmiento JM, Scatton O, Kim KH, Dagher I, Topal B, Primrose J, Nomi T, Fuks D, Abu Hilal M (2018) Laparoscopic versus open major hepatectomy: a systematic review and meta-analysis of individual patient data. Surg. (United States)
Chen J, Li H, Liu F, Li B, Wei Y (2017) Surgical outcomes of laparoscopic versus open liver resection for hepatocellular carcinoma for various resection extent. Med (United States). https://doi.org/10.1097/MD.0000000000006460
Nomi T, Fuks D, Govindasamy M, Mal F, Nakajima Y, Gayet B (2015) Risk factors for complications after laparoscopic major hepatectomy. Br J Surg. https://doi.org/10.1002/bjs.9726
Nomi T, Hirokawa F, Kaibori M, Ueno M, Tanaka S, Hokuto D, Noda T, Nakai T, Ikoma H, Iida H, Komeda K, Ishizaki M, Hayami S, Eguchi H, Matsumoto M, Morimura R, Maehira H, Sho M, Kubo S (2019) Laparoscopic versus open liver resection for hepatocellular carcinoma in elderly patients: a multi-centre propensity score-based analysis. Surg Endosc. https://doi.org/10.1007/s00464-019-06812-z
Memeo R, De’Angelis N, Compagnon P, Salloum C, Cherqui D, Laurent A, Azoulay D (2014) Laparoscopic vs open liver resection for hepatocellular carcinoma of cirrhotic liver: A case-control study. World J Surg. https://doi.org/10.1007/s00268-014-2659-z
Fuks D, Cauchy F, Fteriche S, Nomi T, Schwarz L, Dokmak S, Scatton O, Fusco G, Belghiti J, Gayet B, Soubrane O (2016) Laparoscopy decreases pulmonar y complications in patients undergoing major liver resection a propensity score analysis. Ann Surg. https://doi.org/10.1097/SLA.0000000000001140
Kim JM, Cho BI, Kwon CHD, Joh JW, Park JB, Lee JH, Kim SJ, Paik SW, Park CK (2015) Hepatectomy is a reasonable option for older patients with hepatocellular carcinoma. Am J Surg. https://doi.org/10.1016/j.amjsurg.2013.06.010
Wang W, Huang Z, Guo B, Liu S, XiaoLiang W (2018) J Short- and long-term outcomes of laparoscopic hepatectomy in elderly patients with hepatocellular carcinoma. J Buon 23:971–978
Menon KV, Al-Mukhtar A, Aldouri A, Prasad RK, Lodge PA, Toogood GJ (2006) Outcomes after Major Hepatectomy in Elderly Patients. J Am Coll Surg. https://doi.org/10.1016/j.jamcollsurg.2006.07.025
Abu Hilal M, Di Fabio F, Syed S, Wiltshire R, Dimovska E, Turner D, Primrose JN, Pearce NW (2013) Assessment of the financial implications for laparoscopic liver surgery: A single-centre UK cost analysis for minor and major hepatectomy. Surg Endosc. https://doi.org/10.1007/s00464-012-2779-1
Ratti F, Cipriani F, Ariotti R, Giannone F, Paganelli M, Aldrighetti L (2015) Laparoscopic major hepatectomies: current trends and indications A comparison with the open technique. Updates Surg. https://doi.org/10.1007/s13304-015-0312-5
Wang XT, Wang HG, Duan WD, Wu CY, Chen MY, Li H, Huang X, Zhang FB, Dong JH (2015) Pure laparoscopic versus open liver resection for primary liver carcinoma in elderly patients a single-center, case-matched study. Med (United States). https://doi.org/10.1097/MD.0000000000001854
Hou YF, Li B, Wei YG, Yang JY, Wen TF, Xu MQ, Yan LVN, Chen KF (2015) Second hepatectomy improves survival in patients with microvascular invasive hepatocellular carcinoma meeting the Milan criteria. Med (United States). https://doi.org/10.1097/MD.0000000000002070
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Antonella Delvecchio, Maria Conticchio, Francesca Ratti, Maximiliano Gelli, Ferdinando Massimiliano Anelli, Alexis Laurent, Giulio Cesare Vitali, Paolo Magistri, Federica Mereu, Emanuele Felli, Taiga Wakabayashi, Patrick Pessaux, Tullio Piardi, Fabrizio Di Benedetto, Nicola de’Angelis, Javier Briceno, Rene Adam, Daniel Cherqui, Luca Aldrighetti, and Riccardo Memeo declare that they have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Delvecchio, A., Conticchio, M., Ratti, F. et al. Laparoscopic major hepatectomy for hepatocellular carcinoma in elderly patients: a multicentric propensity score‑based analysis. Surg Endosc 35, 3642–3652 (2021). https://doi.org/10.1007/s00464-020-07843-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07843-7