
Abstract
Objective
To describe outcomes after transanal total mesorectal excision (TaTME) 5 years from implementation at a large-volume colorectal unit, including local recurrence, distant metastasis, and survival.
Background
Transanal total mesorectal excision (TaTME) is a relatively new procedure for mid- and low-rectal cancer, with well-documented safety and feasibility. However, data on long-term results are limited.
Methods
This study was based on a prospective data collection via a maintained database in a large colorectal unit. The database included patients who underwent TaTME from December 2013 through July 2019. We have updated the database through a review of patient charts, including radiology and pathology reports. Data collection included operative details, intraoperative findings, postoperative complications, pathologic results, and oncologic results.
Results
During the study period, two hundred patients underwent TaTME in the study period (men = 147). The mean BMI was 26.7%, and the mean tumor height from the anal verge was 7.86 cm. Neoadjuvant treatment was given to 22% of patients. Anastomotic leakage occurred in 9.3% of patients, and the overall rate of postoperative complications was 24.5%. The TME specimen was incomplete in 11% of patients, and the CRM was positive in 5.5% of patients. Local recurrence (LR) occurred in seven patients with a follow-up of at least 2 years (4.7%). Distant metastasis (DM) occurred in 12% of patients. The overall survival was 90% and disease-free survival was 81%. The operating time was reduced in the later period of our experience.
Conclusions
This study showed that TaTME is feasible, safe, and had acceptable short-term outcomes and an acceptable rate of LR. The study included, however, one group that was non-randomized, and the follow-up was not long enough for most patients. Studies with longer follow-up data are awaited.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
The most recently introduced approach in the treatment of rectal cancer is TaTME, being at this time practiced over a decade. As a “solution to some old problems” [1], it has gained enormous focus, with considerable interest from colorectal surgeons. Most studies have focused on technical tips, risks, safe introduction, complications, and short-term outcomes. The long-term oncologic safety needs, however, to be established before we can consider it as a gold standard.
As a large-volume colorectal unit, we have adopted TaTME as a standard of care for patients with mid- and low-rectal cancer since 2013 [2]. With our growing experience, we aimed in this report to audit our results so far, focusing on long-term outcomes and including all patients operated since 2013.
Methods
We have maintained a prospective TaTME database that includes all patients operated since December 2013. All patients have provided informed written consent for the surgical procedure and the research related to different aspects of their treatment. The institutional review board approved this study and the database. The Danish Data Protection Agency has approved the database, which includes demographics, tumor characteristics, operative details, postoperative results, pathological results, and long-term oncologic results. We have published several papers on different aspects of TaTME [2,3,4,5]. These papers focused on short-term outcomes of our first 150 cases. We have since updated the database regularly to audit the results and detect any tendencies of complications or poor oncologic results. We have reviewed the database recently and present our findings in this study, including data on local recurrence (LR), distant metastasis (DM) and survival. Thus, the present study includes data on cases already published, and an additional 75 patients operated on afterward. The standard variables in the database constituted the source of data collection, in addition to a careful review of patient charts for the period that followed the index operation to the present date. The chart review included all radiological investigations including computerized tomography (CT) and magnetic resonance imaging (MRI) scans, pathology reports from biopsies or specimens (if any), endoscopic procedures and any clinical chart notes indicating the probability of the existence of LR or DM. Our electronic patient chart system is linked to the Central Person Register, allowing the calculation of the date of death for deceased patients. The diagnosis of LR and MD was thus based on either pathology (for patients who underwent surgery for LR or MD), radiologic evidence, or clinical suspicion. We have adopted this method because in some cases, no further diagnostic workup is necessary when it is evident that the patient has LR or MD and radical surgery is not an option. In these cases, we offer palliative chemotherapy based on the radiological evidence and the background of the patient's history of colorectal cancer.
We have previously published our protocol for the diagnostic workup and details of surgery according to our standardized routine at Slagelse Hospital [2, 3]. Besides, the procedure is well described in the literature [6,7,8]. We apply TaTME for all newcomers with rectal cancer at or below 10 cm from the anal verge, including patients where intersphincteric APE would be performed. Indications for TME are tumors at or below the distance of 10 cm, and exceptionally in some cases for a slightly higher tumor up to 12 cm from the anal verge. According to the national guidelines from the Danish Colorectal Cancer Group (DCCG), patients with advanced mid- and low-rectal tumors are offered neoadjuvant chemoradiation [9]. Advanced tumors are defined according to our national guidelines as all T4 tumors and T3 tumors in the lowest five cm of the rectum. In patients with advanced mid-rectal T3 tumors (distance 5–10 cm from the anal verge), the indications for neoadjuvant treatment are a distance of less than five mm from the most profound invasion of the tumor into the mesorectal fat to the mesorectal fascia. This guideline was revised recently, and the most crucial change is the definition of an advanced mid-rectal T3 tumor, which is defined as one with a distance from the most profound invasion in the mesorectal fat to the mesorectal fascia of two mm or depth of invasion into the mesorectal fat of ≥ 5 mm. The radiation dosage is 50.4 Gy, 28 fractions in combination with 5-fluorouracil or equivalent chemotherapy. Patients who receive neoadjuvant chemoradiation undergo surgery after 8–12 weeks from the date of the last radiation dose, preceded by a new radiologic evaluation with CT and MR scans.
We have introduced an enhanced recovery program (ERAS) since 2017. Patients planned for sphincter-saving surgery have received oral mechanical bowel preparation with Moviprep (Norgine Denmark A/S Stamholmen, 2650 Hvidovre, Denmark) plus enema in the morning of surgery.
The usual method of TaTME in our unit is a hybrid method, where TME starts through the abdominal approach, and the transanal part follows. The extent of the abdominal part depended in some cases on the feasibility of dissection from above. We have adopted a routine splenic flexure mobilization in every case of low anterior resection. Splenic flexure was not always mobilized at the beginning of our experience. Our routine for anastomotic technique is a stapled side-end or in some cases end-end. Where possible, we have extracted specimens through the transanal route. A standard laparoscopic or a single port procedure was performed for the abdominal part. A diverting loop ileostomy was performed in all patients who had a colorectal anastomosis (low anterior resection).
Histopathological examination was performed on freshly extracted specimens, based on a standard protocol following the method described by Phil Quirke and colleagues [10,11,12]. The quality of the resected TME specimen was graded as complete, nearly complete or incomplete. The standard pathology report included information about the number of retrieved lymph nodes and the number of nodes involved by cancer, as well as information on the Circumferential and Distal Resection Margins (CRM and DRM). An involved CRM or DRM was defined as a distance of ≤ 1 mm from the tumor to the inked surface of the fixed specimen or from cancer to the distal cut edge of the tissue, respectively.
The primary outcomes in this study were the long-term oncologic results (LR, DM, OS, and DFS), pathologic results (CRM, DRM, quality of TME specimen). As in our previous paper [3], we calculated the surgical success based on a composite based on the quality of TME specimen, CRM, and DRM as described by Fleshman et al. [13]. A successful resection fulfilled the following criteria: (1) clear CRM (defined as a distance > 1 mm between the most profound extent of tumor invasion into the mesorectum and the inked surface on the fixed specimen), (2) clear DRM (defined as the distance > 1 mm between the tumor to the distal cut edge of the tissue), and (3) a TME specimen graded as complete or nearly complete as defined above.
The secondary outcomes included intraoperative details and postoperative complications. Operating time was calculated in minutes from skin incision/insertion of the first laparoscopic port to the last stitch for either skin closure or stoma creation—this included time spent in preparation for the transanal part. The operating time for the transanal part was calculated from the fixation of the Lone Star retractor to the creation of the anastomosis of the last stitch on perineal skin in abdominoperineal excision (APE) procedures. Conversion to open procedure was defined as any skin incision done for purposes other than specimen retrieval. Bowel perforation was defined as any perforation during either the abdominal or the transanal part. Rescue APE was defined as one done in a patient for whom anastomosis was otherwise planned. The decision to perform anastomosis was taken at the outpatient clinic depending on the tumor height, intraoperative complications, patient wishes, and comorbidities. We have a systematic approach in patients who undergo low anterior resection, to inform about low anterior resection syndrome (LARS), followed by information on stomas by a stoma nurse.
Postoperative complications were defined as any complication within 30 days after surgery. Complications were graded as described by Clavien et al. [14]. Anastomotic leakage was defined as one that was clinically suspected, radiologically, or endoscopically proved and actively treated. Urinary dysfunction was defined as an inability of spontaneous voiding at discharge. Stoma complication was defined as any complication related directly to the stoma. The hospital stay was calculated from the day of surgery to discharge. The criteria for discharge were the absence of signs of complications tolerated oral diet and when capable of independent stoma care or help arranged by a home-nurse.
Long-term outcomes were registered in our database according to predefined variables based on chart review. LR was defined as the recurrence of malignancy in the pelvis or perirectally, whether histologically proven (biopsy, surgery or autopsy), radiologically diagnosed or clinically suspected. DM was defined as any histological or radiological sign of metachronous tumor growth outside the pelvis. Time to LR or DM was calculated from the date of surgery to the date of diagnosis of LR or DM. Overall Survival (OS) was defined as the number of patients alive at the end of this study. Disease-free survival (DFS) was defined as the number of patients alive and without signs of LR or DM at the end of this study.
The following variables were analyzed as predictors for anastomotic leakage: gender (female/male), BMI (> 30 vs. < 30 kg/m2), preoperative chemoradiation (yes/no), anastomotic orientation (side-end/end-end), and the size of the circular stapler (32/33 mm). The following variables were analyzed as predictors for incomplete TME specimen, positive CRM and a successful resection: gender (female/male), BMI (> 30 vs. < 30 kg/m2), T4 tumor (T4/not T4), the performed procedure (anastomosis/APE), and intraoperative bowel perforation (yes/no).
The following variables were analyzed as predictors for LR: Gender (female/male), BMI (> 30 vs. < 30 kg/m2), T4 tumor (T4/not T4), tumor height (> 5/ < 5 cm from anal verge), preoperative chemoradiation (yes/no), anastomotic leakage (leak/no leak), quality of TME specimen (incomplete/complete or nearly complete), CRM (±), rates of retrieved positive lymph nodes (pN0/pN1 or pN2), extraction site (transanal or perineal/transabdominal), and the performed procedure (anastomosis/APE).
We have compared the main characteristics and short-term outcomes between two subgroups, representing our first 100 cases versus the last 100 cases. We have chosen this method as a pragmatic and simple way to explore the potential advances, which might have been achieved with time. The first 100 cases were operated on between December 2013 and June 2016; the second 100 cases were operated on between July 2016 and July 2019.
Statistical analysis
Numerical data are presented as means with standard deviation where relevant and categorical data are presented as numbers with percentages. A χ2 test was used to compare nominal categorical variables, and Student’s t-test was used to compare quantitative variables. We conducted a binary logistic regression analysis to define predictors of anastomotic leakage, incomplete TME specimens, CRM positivity, and local recurrence. We have plotted the cumulative sum (CUSUM) charts to determine the learning curve. A P value of < 0.05 for variables in the equation of the analysis was considered statistically significant. We used the statistical software package SPSS version 24 for calculations (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.).
Results
We have performed 200 hybrid TaTME procedures from December 2013 through July 2019. Table 1 shows patient and tumor characteristics. Among 60 APE procedures, five were as rescue procedures in the otherwise planned anastomosis; of these, two were due to intraoperative bleeding and three were due to technical difficulty in the lower part of the pelvis. One urethral injury occurred during the transanal part in a patient who had received neoadjuvant chemoradiation. Transabdominal specimen extraction was done in 38 (19%) patients, of whom five had APE procedures. We performed a side-end anastomosis in 80% of cases. Tables 2 and 3 show the operative details.
Postoperative surgical complications occurred in 49 (24.5%) patients. Among 140 patients with an anastomosis, leakage occurred in 13 (9.3%) patients. Management of anastomotic leakage was as follows: repeated rectal washout (2), endosponge [15] no treatment (10), and colostomy (1). Five patients who had anastomotic leakage ended up having a permanent colostomy. Table 4 shows the postoperative surgical complications, and Table 5 shows the postoperative medical complications, which occurred in 14 (7%) patients.
In the logistic analysis, none of the following variables was significantly associated with anastomotic leakage: gender (P = 086), BMI (P = 0.984), preoperative neoadjuvant treatment (0.664), anastomotic orientation (P = 0.664) ,or the size of the circular stapler (P = 0.586).
Among 140 patients with anastomosis and diverting ileostomy, 113 underwent stoma closure. However, only 104 patients were stoma-free at the end of the follow-up period; eight patients had a permanent colostomy, and one patient underwent a new loop ileostomy formation. Thus, the number of patients with a stoma was 36 (colostomy = 8, ileostomy = 28).
Pathologic outcomes
The TME specimen was incomplete in 22 (11%) patients, and the CRM was positive in 11 patients (5.5), and the DRM was positive in one patient (0.5%). In the logistic regression analysis, the only significant independent factor for incomplete TME specimen was a T4 tumor (P = 0.004). Gender (P = 0264), BMI (P = 0.438), tumor height from the anal verge (P = 0.804), intraoperative bowel perforation (P = 0.055), and the performed procedure (P = 0.824) were not significant predictive factors for incomplete TME specimen. Intraoperative bowel perforation was the only significant positive predictive factor for positive CRM (P < 0.001). A T4 tumor was the only significant independent predictive factor for a non-successful resection (P = 0.003) (Table 6).
Oncologic results and survival
Following a mean follow-up of 29 months (range 1–61, ± SD 15.994), the number of survived patients was 180 (90%), of whom 162 were disease-free (81%). LR occurred in seven patients (3.5%). All these occurred in patients with a minimum length of follow-up of 2 years (n = 150 patients, adjusted percentage of LR = 4.7%). The mean time to LR was 24 months (range 10–45, ± SD 12.632). Metachronous DM occurred in 24 patients (12%), and the mean time to metastasis was 19 months (range 6–45, ± SD 10.185). Four patients who developed distant metastasis had metastatic disease at diagnosis and underwent radical liver surgery before rectal resection. Patients who developed LR had no metastasis at diagnosis.
In the logistic regression analysis, anastomotic leakage was a significant independent factor for the occurrence of LR, among 140 patients who had an anastomosis at the primary surgery (P = 0.019). Gender (P = 0.945), BMI (P = 0.632), preoperative neoadjuvant therapy (P = 0.997), quality of TME specimen (P = 0.820), rates of positive CRM (P = 0.208), T4 tumor (P = 0.999), rates of retrieved positive lymph nodes (P = 0.073), tumor height (P = 0.315), extraction site (P = 0.516), and the performed procedure (P = 0.183) were not positive predictive factors for LR (Table 7).
Comparison of the early versus late period
During the second period of our experience, we performed a low anterior resection in 81% of patients. This was significantly higher than 59% in the first period (P = 0.001). The operating time for the transanal part was significantly shorter in the second period (P < 0.001). We found no statistically significant differences between the two periods for the other main short-term outcomes. Table 8 shows these comparisons.
Learning curve
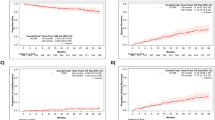
Figure 1 shows the CUSUM chart for the total operating time. The chart shows a decrease in the total operating time in case 140. Prior to that, the operating time tends to lie in the upper limits, with an “out of control” pike at case 133 and 134. Figure 2 shows the CUSUM chart for the transanal part of the procedure, which decreases significantly in case 151 and afterward and falls below the average. The chart shows a steady decrease in the operating time for the transanal part from case 96. The intraoperative blood loss is shown in Fig. 3, where the blood loss was “out of control” on several occasions, the last of which at case 139, after which the blood loss was generally less than that in the previous period. In accordance with findings in Table 8, these results indicate proficiency acquisition in the second half of our experience, translated into stability in some important outcomes.

CUSUM chart for total operating time

CUSUM chart for transanal operating time

CUSUM chart for intraoperative blood loss
Discussion
This was an audit of a single-center experience with a consecutive large number of TaTME procedures. We have shown that the procedure is feasible and safe in accordance with the literature and our own previous experience [2, 3, 16]. The application of such a demanding approach for patients with mid- and low-rectal cancer was in accordance with expert recommendations [17]. The rates of intraoperative complications were in accordance with the literature [16, 18], especially severe complications like urethral injury, which occurred in one patient. No incidence of Carbon Dioxide (CO2) embolism occurred, a complication that was previously reported in association with TaTME [19]. The conversion rate was almost negligible (0.5%). Four patients had an intraoperative bowel perforation. In two cases, the perforation occurred during the transanal phase of the procedure. Perforation is a severe complication and had a predictive effect on the rate of non-radical surgery in this study, but not on LR, and has been identified as a significant risk factor for LR [20].
The rates of postoperative surgical and medical complications were in accordance with the literature [21]. The rate of anastomotic leakage was likewise within the known range in the literature and lower than anastomotic leak rate reported by Penna et al. from the international TaTME registry [22]. Most leaks were mild and treated without the need for anastomosis takedown. Our rate of complete specimens was not very high. However, the rate of complete and nearly complete specimens was 89%. One explanation is our routine transanal extraction whenever this is possible, which could tear the specimens leading to a higher rate of incomplete and nearly complete TME specimens. The rate of positive CRM of 5.5% is to be considered acceptable and in accordance with the literature, and probably slightly higher than selected cases in the international registry [16, 23]. The rate of successful resection was lower in open and laparoscopic rectal surgery, in accordance with our own previous results [3, 13, 24]. One explanation is the relatively high rate of incomplete specimens in this study.
Seven patients in this study had LR, which, for patients with a follow-up length of at least 2 years, is equal to 4.7%. Anastomotic leakage had a predictive effect on LR. This rate is in accordance with the literature. One of these cases was published earlier [25]. There have been improvements in rates of LR and survival. Bill Heald, who introduced TME in the late 1970s and early 1980s, made the most critical change and could show dramatic improvements [26,27,28].
While the minimally invasive approach is the standard way to perform TME in large parts of the globe, the very same original TME principles are applied at this time. It is the oncologic safety of Bill Herald’s TME, which remains the primary outcome to be valued highest when a new procedure is introduced. Minimal invasive laparoscopic and robot-assisted laparoscopic surgery are well established, mainly due to the reproducible results and robust evidence [29,30,31,32]. However, the “non-inferiority” of laparoscopic surgery has been questioned in two recent randomized trials [13, 24, 33]. The main challenges in rectal cancer surgery remain the lowermost part of the operative field, leading to conversion and inferior oncological outcomes [20, 34, 35]. Robot-assisted laparoscopic surgery probably overcomes some of the difficulties and yet to be proved [36]. The critical point is perhaps the direction of dissection and not the way of it, in other words, “from where” and not “by what” we perform the dissection. A very old method that was practiced in over a 100 years that is “dissection from below” is now being explored, utilizing a new technology. Funahashi et al. [37] reported a new procedure in 2009, where some dissection was done through the transanal route, followed by laparoscopic dissection, thus allowing for the most difficult lower part to be done from below where the surgeon is closest to the operative field. The results were quite acceptable. Denost et al. [38] have randomized 100 patients to either transanal or abdominal dissection of the lowermost part of the rectum and found improved short-term pathological outcomes, although this could not be translated to an improvement in local recurrence rate [39].
Since Buess developed his transanal endoscopic microsurgery (TEM) procedure for small rectal lesions in the early 1980s [40], several experimental studies explored the possibility of utilities beyond local excision [41, 42]. These and several other studies showed promising results in terms of feasibility in dissecting through a transanal platform using standard laparoscopic instruments. In the last decade, flexible transanal platforms are used to perform local excisions, and parts of TME procedures, the so-called hybrid procedure TaTME. With hundreds of reports on its feasibility in clinical practice [2, 3, 21, 43, 44] and thousands of patients treated this way [16, 22], the safety and effectivity regarding short-term outcomes are well established.
The oncologic safety of TaTME is, on the other hand, not established yet. Concerns about early recurrence have led to the abandonment of TaTME in at least one country [45]. Hol et al. [46] have reported quite acceptable long-term results. Roodbeen et al. [47] have reported a low recurrence rate after TaTME from expert centers. Thus, no definite alarming data are yet available, and long-term results from centers with the most extensive experience would add more evidence, and clarify whether TaTME is the new gold standard [48]
This study had several limitations. Although it is a prospective study in the sense of data collection and a systematically maintained database, it is not a randomized study. We believe, however, that we had no missing data due to a quite well-established electronic chart system, regular multidisciplinary meetings, and a systematic method of clinical, radiological, and endoscopic controls for patients with rectal cancer. Another limitation is the absence of a control group, though this was done in our previous publication [3]. The follow-up period was probably not long enough, although 150 patients had at least 2 years of follow-up. This is essential as most recurrences occur during the first 2 years after rectal cancer surgery, and even earlier after TaTME [45].
Conclusion
This study showed that TaTME is feasible, safe, and had acceptable short-term outcomes and an acceptable rate of LR. Studies with longer follow-up are to be awaited.
References
Heald RJ (2013) A new solution to some old problems: transanal TME. Tech Coloproctol 17(3):257–258
Perdawood, S.K. and G.A. Al Khefagie, Transanal vs laparoscopic total mesorectal excision for rectal cancer: initial experience from Denmark. Colorectal Dis, 2016. 18(1):51–58.
Perdawood SK, Thinggaard BS, Bjoern MX (2018) Effect of transanal total mesorectal excision for rectal cancer: comparison of short-term outcomes with laparoscopic and open surgeries. Surg Endosc 32(5):2312–2321
Perdawood SK et al (2019) The pattern of defects in mesorectal specimens: is there a difference between transanal and laparoscopic approaches? Scand J Surg 108(1):49–54
Bjoern MX, Nielsen S, Perdawood SK (2019) Quality of life after surgery for rectal cancer: a comparison of functional outcomes after transanal and laparoscopic approaches. J Gastrointest Surg 23(8):1623–1630
Knol JJ et al (2015) Transanal endoscopic total mesorectal excision: technical aspects of approaching the mesorectal plane from below—a preliminary report. Tech Coloproctol 19(4):221–229
Atallah S (2015) Transanal total mesorectal excision: full steam ahead. Tech Coloproctol 19(2):57–61
Atallah S (2014) Transanal minimally invasive surgery for total mesorectal excision. Minim Invasive Ther Allied Technol 23(1):10–16
DCCG (2013) Recommendations of the Danish Colorectal Cancer Group: neoadjuvanttreatment of advanced resectable rectal cancer. https://dccg.dk/wp-content/uploads/2018/10/Str%C3%A5lebehandling-ved-rectum-cancer-v2-2018-10-02.pdf
Quirke, P., et al., Local recurrence of rectal adenocarcinoma due to inadequate surgical resection. Histopathological study of lateral tumour spread and surgical excision. Lancet, 1986. 2(8514):996–999.
Quirke P et al (2009) Effect of the plane of surgery achieved on local recurrence in patients with operable rectal cancer: a prospective study using data from the MRC CR07 and NCIC-CTG CO16 randomised clinical trial. Lancet 373(9666):821–828
Nagtegaal ID et al (2002) Macroscopic evaluation of rectal cancer resection specimen: clinical significance of the pathologist in quality control. J Clin Oncol 20(7):1729–1734
Fleshman J et al (2015) Effect of laparoscopic-assisted resection vs. open resection of stage II or III rectal cancer on pathologic outcomes: the ACOSOG Z6051 randomized clinical trial. JAMA 314(13):1346–1355
Clavien PA et al (2009) The Clavien–Dindo classification of surgical complications: five-year experience. Ann Surg 250(2):187–196
Nerup N et al (2013) Promising results after endoscopic vacuum treatment of anastomotic leakage following resection of rectal cancer with ileostomy. Dan Med J 60(4):A4604
Penna M et al (2017) Transanal total mesorectal excision: international registry results of the first 720 cases. Ann Surg 266(1):111–117
Adamina M et al (2018) St.Gallen consensus on safe implementation of transanal total mesorectal excision. Surg Endosc 32(3):1091–1103
Rouanet P et al (2013) Transanal endoscopic proctectomy: an innovative procedure for difficult resection of rectal tumors in men with narrow pelvis. Dis Colon Rectum 56(4):408–415
Dickson EA et al (2019) Carbon dioxide embolism associated with transanal total mesorectal excision surgery: a report from the international registries. Dis Colon Rectum 62(7):794–801
Bulow S et al (2011) Intra-operative perforation is an important predictor of local recurrence and impaired survival after abdominoperineal resection for rectal cancer. Colorectal Dis 13(11):1256–1264
Bjorn MX, Perdawood SK (2015) Transanal total mesorectal excision—a systematic review. Dan Med J 62(7):5105
Penna M et al (2019) Incidence and risk factors for anastomotic failure in 1594 patients treated by transanal total mesorectal excision: results from the International TaTME Registry. Ann Surg 269(4):700–711
Ma B et al (2016) Transanal total mesorectal excision (taTME) for rectal cancer: a systematic review and meta-analysis of oncological and perioperative outcomes compared with laparoscopic total mesorectal excision. BMC Cancer 16:380
Stevenson AR et al (2015) Effect of laparoscopic-assisted resection vs open resection on pathological outcomes in rectal cancer: the ALaCaRT Randomized Clinical Trial. JAMA 314(13):1356–1363
Perdawood SK (2018) A case of local recurrence following transanal total mesorectal excision: a new form of port-site metastasis? Tech Coloproctol 22(4):319–320
Heald RJ (1979) A new approach to rectal cancer. Br J Hosp Med 22(3):277–281
Heald RJ, Husband EM, Ryall RD (1982) The mesorectum in rectal cancer surgery–the clue to pelvic recurrence? Br J Surg 69(10):613–616
Heald RJ et al (1998) Rectal cancer: the Basingstoke experience of total mesorectal excision, 1978–1997. Arch Surg 133(8):894–899
Bonjer HJ et al (2015) A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 373(2):194
Jeong SY et al (2014) Open versus laparoscopic surgery for mid-rectal or low-rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): survival outcomes of an open-label, non-inferiority, randomised controlled trial. Lancet Oncol 15(7):767–774
Kang SB et al (2010) Open versus laparoscopic surgery for mid or low rectal cancer after neoadjuvant chemoradiotherapy (COREAN trial): short-term outcomes of an open-label randomised controlled trial. Lancet Oncol 11(7):637–645
Fleshman J (2016) Current status of minimally invasive surgery for rectal cancer. J Gastrointest Surg 20(5):1056–1064
Fleshman J et al (2019) Disease-free Survival and local recurrence for laparoscopic resection compared with open resection of stage II to III rectal cancer: follow-up results of the ACOSOG Z6051 randomized controlled trial. Ann Surg 269(4):589–595
Bonjer HJ et al (2015) A randomized trial of laparoscopic versus open surgery for rectal cancer. N Engl J Med 372(14):1324–1332
Nagtegaal ID et al (2005) Low rectal cancer: a call for a change of approach in abdominoperineal resection. J Clin Oncol 23(36):9257–9264
Jayne D et al (2017) Effect of robotic-assisted vs conventional laparoscopic surgery on risk of conversion to open laparotomy among patients undergoing resection for rectal cancer: the ROLARR randomized clinical trial. JAMA 318(16):1569–1580
Funahashi K et al (2009) Transanal rectal dissection: a procedure to assist achievement of laparoscopic total mesorectal excision for bulky tumor in the narrow pelvis. Am J Surg 197(4):e46–50
Denost Q et al (2014) Perineal transanal approach: a new standard for laparoscopic sphincter-saving resection in low rectal cancer, a randomized trial. Ann Surg 260(6):993–999
Denost Q et al (2018) Transanal versus abdominal low rectal dissection for rectal cancer: long-term results of the Bordeaux' randomized trial. Surg Endosc 32(3):1486–1494
Buess G et al (1992) Technique and results of transanal endoscopic microsurgery in early rectal cancer. Am J Surg 163(1):63–69
Whiteford MH, Denk PM, Swanstrom LL (2007) Feasibility of radical sigmoid colectomy performed as natural orifice translumenal endoscopic surgery (NOTES) using transanal endoscopic microsurgery. Surg Endosc 21(10):1870–1874
Telem DA et al (2013) Transanal rectosigmoid resection via natural orifice translumenal endoscopic surgery (NOTES) with total mesorectal excision in a large human cadaver series. Surg Endosc 27(1):74–80
de Lacy FB et al (2018) Transanal total mesorectal excision: pathological results of 186 patients with mid and low rectal cancer. Surg Endosc 32(5):2442–2447
Simillis C et al (2016) A systematic review of transanal total mesorectal excision: is this the future of rectal cancer surgery? Colorectal Dis 18(1):19–36
Larsen SG et al (2019) Norwegian moratorium on transanal total mesorectal excision. Br J Surg 106(9):1120–1121
Hol JC et al (2019) Long-term oncological results after transanal total mesorectal excision for rectal carcinoma. Tech Coloproctol 23:903–911
Roodbeen SX et al (2020) Local recurrence after transanal total mesorectal excision for rectal cancer: a multicenter cohort study. Ann Surg 1:11. https://doi.org/10.1097/SLA.0000000000003757
Atallah S, Sylla P, Wexner SD (2019) Norway versus the Netherlands: will taTME stand the test of time? Tech Coloproctol 23(9):803–806
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosure
Drs. Sharaf Karim Perdawood, Jens Krøigaard, Marianne Eriksen, and Pauli Mortensen have no conflicts of interest or financial ties to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Perdawood, S.K., Kroeigaard, J., Eriksen, M. et al. Transanal total mesorectal excision: the Slagelse experience 2013–2019. Surg Endosc 35, 826–836 (2021). https://doi.org/10.1007/s00464-020-07454-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-020-07454-2