
Abstract
Background
Neurobiological feedback in surgical training could translate to better educational outcomes such as measures of learning curve. This work examined the variation in brain activation of medical students when performing laparoscopic tasks before and after a training workshop, using functional near-infrared spectroscopy (fNIRS).
Methods and procedures
This single blind randomised controlled trial examined the prefrontal cortex activity (PFCA) differences in two groups of novice medical students during the acquisition of four laparoscopic tasks. Both groups were shown a basic tutorial video, with the “Trained-group” receiving an additional standardised one-to-one training on the tasks. The PFCA was measured pre- and post-intervention using a portable fNIRS device and reported as mean total oxygenated hemoglobin (HbOµm). Primary outcome of the study is the difference in HbOµm between post- and pre-intervention readings for each of the four laparoscopic tasks. The pre- and post-intervention laparoscopic tasks were recorded and assessed by two blinded individual assessors for objective scores of the performance.
Results
16 Trained and 16 Untrained, right-handed medical students with an equal sex distribution and comparable age distribution were recruited. Trained group had an attenuated left PFCA in the “Precision cutting” (p = 0.007) task compared to the Untrained group. Subgroup analysis by sex revealed attenuation in left PFCA in Trained females compared to Untrained females across two laparoscopic tasks: “Peg transfer” (p = 0.005) and “Precision cutting” (p = 0.003). No significant PFCA attenuation was found in male students who underwent training compared to Untrained males.
Conclusion
A standardised laparoscopic training workshop promoted greater PFCA attenuation in female medical students compared to males. This suggests that female and male students respond differently to the same instructional approach. Implications include a greater focus on one-to-one surgical training for female students and use of PFCA attenuation as a form of neurobiological feedback in surgical training.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
With technological advances, minimally invasive surgery has since become the preferred surgical approach due to reduced surgical trauma by using smaller incisions. Unlike open surgical approaches, laparoscopic surgery is considered technically difficult due to its learning curve. Although 3-dimensional imaging is available, most commonly used laparoscopes have 2-dimensional imaging. The surgeon has poorer depth perception from 2-dimensional images produced by the laparoscope and manipulation of tissue involves the use of tools that are difficult to handle and provide poorer tactile feedback. Consequently, the acquisition of laparoscopic skills is considered to be more challenging.
Historically, the evaluation of surgical skill is assessed by quantitative and qualitative feedbacks which can be subjective. The lack of neurobiological understanding of the effects of surgical training provided the impetus for this study. The prefrontal cortex is responsible for various cognitive processes including: executive functions, motor planning, decision-making, judgment, working memory and ability to sustain attention [1]. It has also been implicated in the ability to utilise feedback and to deal with novelty [2]. We elected to use the Functional Near-Infrared Spectroscopy (fNIRS), which is a novel non-invasive optical brain imaging tool, to study hemodynamic changes within the prefrontal cortex. Based on neurovascular coupling, local neuronal activation can be inferred from increased blood flow to activated regions of the brain. This allows us to measure the activation of prefrontal cortex during the performance of various motor tasks. Its portability allows the participants to be scanned in standing or sitting position, facilitating the assessment of the participants’ prefrontal cortex function while doing laparoscopic tasks.
While the prefrontal cortex is known to be vital for acquisition of visuomotor skills, its role in the attainment of complex technical skills which comprise both perceptual and motor components, such as those associated with laparoscopic surgery, remains poorly understood. The literature has shown differences in PFC activity patterns between surgeons of varying skills [3,4,5]. In a previous study which was based on simple suturing, Leff et al. [3] demonstrated that similar prefrontal cortex hemodynamic responses were found in registrars and consultants, in whom technical performance could not be discriminated. In contrast, distinctly different patterns of cortical hemodynamics and significantly poorer knot-tying performance were observed in surgical novices. Shetty et al. [4] examined prefrontal cortex engagement of participants during laparoscopic tasks and found superior technical performance in experts compared with residents, who in turn outperformed novices. An inverse association was also noted between the grade of surgeon and prefrontal cortex attenuation. Apart from attenuation of the PFC with mastery, Andreu-Perez et al. [6] also demonstrated a disparity in frontal lobe connectivity during complex bimanual motor task aids, with novices depending on the interactions between associative and motor cortical networks more so than experts.
Foregoing studies did not compare the prefrontal cortex activation patterns of male and female medical students who underwent laparoscopic surgical training to those without training. The changes in various areas of prefrontal cortex activation between Trained participants and Untrained participants could reveal how surgical training streamlines the learning process and causes activation of specific areas that may correlate with learning pathways.
The aim of our study herein was to examine the neurophysiological basis underlying these learning processes which may spark more rigorous refinement of the curricula in medical surgical education with the assistance of functional neuroimaging. We hypothesised that the group of students who underwent an additional surgical training workshop would have a greater attenuation in PFCA after training.
Methods
This is a prospective, parallel randomised controlled pilot study examining the effects of how laparoscopic workshops changes areas of brain activation using fNIRS brain imaging in medical students. Approval was obtained, National University of Singapore’s Institutional Review Board (NUS IRB No: S-18–140). We adhered to principles of reporting of results as suggested by the CONSORT 2010 Statement.
Study participants
The study recruited 32 first to fourth year medical students from the Yong Loo Lin School of Medicine (Singapore) from June to August 2018. Only right-handed individuals with no previous laparoscopic surgery experience were included in the study. Participants were healthy, with no psychiatric or neurological medical history and were not on any chronic medication. They also had normal or corrected to normal vision and were able to provide written consent prior to participation in the study.
Study interventions
All participants were shown a short 20-min video tutorial on how to perform the 4 basic laparoscopic tasks (Peg transfer, Precision cutting, Suture insertion and Intracorporeal knotting) and were given 5 min to familiarise themselves with the laparoscopic simulator (Endo Trainer).
Following which the participants began their pre-intervention assessment. PFCA was recorded using a fNIRS device, the “NIRSIT” model from OBELAB (Korea), as seen in Fig. 1. There was a mandatory 2-min resting period before each laparoscopic task, in which the participants were instructed to regard a cross on the wall while repeating the phrase “ABCDE” in their heads. The resting period gives participants adequate rest and reduces cognitive activity in the prefrontal cortex to a baseline before each task begins. Participants were then given 3 min to complete each of the 4 tasks in a sequential order as demonstrated by Fig. 2. Participants were only required to complete one trial for each task.

A participant wearing the OBELAB NIRSIT device

Example of pre/post-intervention assessment (total time 22 min)
The start and end of each task corresponded to time synchronisation markers for each task, helping to extract fNIRS data accurately.
Participants were then randomly assigned to either intervention groups.
In the “Trained” group, participants were randomly assigned to receive one-to-one training by either of two consultants of general surgery (1 male and 1 female tutor) for 45 min. During the training workshop, participants were given the opportunity to clarify any questions that they had and could practice all 4 tasks again under supervision.
In the “Untrained” group, participants were given a 45-min break and were prohibited from practicing with the Endo Trainer and from watching any laparoscopic related videos or materials.
Following the intervention, participants from both groups completed their post-intervention assessment (identical to pre-intervention assessment) while the NIRSIT device recorded their fNIRS data.
During the laparoscopic tasks, to ensure uniformity amongst participants, the camera’s field of vision was centred and fixed, participants were not allowed to move the camera during the various trials. A Prolene 4–0 suture was used for the Suture insertion and Intracorporeal knotting tasks.
Laparoscopic tasks
In Peg transfer (Task 1) participants used 2 graspers to perform a mid-air transfer of 6 pegs, placed on the left side of the pegboard, onto the corresponding right side of the pegboard. The task was considered complete when participants finished transferring all 6 pegs from left to right. Any pegs which fell out of the field of view resulted in a penalty and the task was not considered to have been completed. This exercise tests eye-hand coordination, ambidexterity and depth perception.
In Precision cutting (Task 2), a 7.5 cm × 7.5 cm non-woven, 4 ply gauze swab had a circle pattern marked out on it with a black marker and positioned pattern face up, such that the open edge of the gauze is secured in the clip. Participants had to use a grasper and scissors to cut out the black circle as quickly and precisely as possible. The task was considered complete when the entire circle was cut out from the gauze swab. This exercise requires one to use both hands in a complementary manner, using one hand to resent the other hand in the best possible way for the other hand to cut.
In Suture insertion (Task 3), participants used a needle holder to hold onto the suture thread before inserting it into the Endo trainer box. Within the Endo trainer, participants had to ensure proper holding of the needle (one third from the end where the suture is attached) using the needle holder before driving the needle through two “black dots” marked on either side of a slit made longitudinally on a Penrose drain. The task was considered complete once the participant was able to insert the suture through both sides of the Penrose drain. This exercise requires proper holding of the needle in the needle holder, needle transferring and suture insertion precision.
In Intracorporeal knotting (Task 4), the suture is already inserted through the longitudinally slit Penrose drain for them and participants had to use 2 needle holders to perform an intracorporeal knot. The participants needed to perform a “surgeons knot” first followed by 2 square knots. The task was considered complete once all three throws were achieved. This exercise is complex requiring several skills such as depth perception, eye-hand coordination, ambidexterity and transferring skills.
The order of the tasks was arranged in an ascending order of technical difficulty level, loosely based off the Fundamentals of Laparoscopic Surgery (FLS) program. The Intracorporeal suturing task in the FLS program was divided into 2 tasks in our study; Suture insertion and Intracorporeal knotting. This was due to concerns that medical students may not be able to complete the entire Intracorporeal suturing task within the 3-min time limit.
Randomization
Upon recruitment of participants, a quick eligibility screen was done. Participants received verbal and written information regarding the study as approved by NUS IRB. After obtaining informed written consent, the participant was then randomly assigned a unique randomization code obtained from a randomization schedule. The randomization schedule was created prior to study activation using a random number generator. As sex differences in response to various surgical teaching approaches were noted in prior studies [7, 8], the randomization schedule was also stratified by sex with a 1:1 allocation using fixed block sizes of 6 and 10. Within each fixed randomisation block, participants were allocated unique randomisation codes sequentially. The intervention status of the participants was only revealed by an investigator with no direct contact with participants after complete recruitment of a block to prevent allocation bias. As the primary outcome is entirely assessed by the fNIRS machine, only the data analysts were blinded to the allocation. All investigators, staff and participants were kept masked to outcome measurements and trial results.
Signal processing and study outcomes
To determine differences in prefrontal cortex activation between Trained and Untrained groups, the fNIRS device used was of the “NIRSIT” model from OBELAB (Korea), which obtained medical device approval from the Korea Food and Drug Administration in April 2017. The ability to transfer fNIRS data wirelessly to laptops facilitated ease of access for analysis and feedback on training.
The NIRIST device has a comprehensive 48 channel system which allows the mapping of each channel to the various Brodmann areas. The main regions of prefrontal cortex analysed were the Dorsolateral prefrontal cortex, Ventrolateral prefrontal cortex and Frontopolar cortex.
The fNIRS data for each laparoscopic task were extracted wirelessly, using time synchronisation markers during the experiment. This system utilises 24 laser source (780/850 nm; maximum power under 1 mW) and 32 photo detectors [9]. The detected signals were filtered by low pass filter (DCT 0.05 Hz) and high pass filter (DCT 0.005 Hz) to minimise ambient light noise and motion artefact. The bad quality channels decided by signal to noise ratio as 30 dB are rejected before further analysis. Hemodynamic changes for each of the 48 channels during each trial and task were calculated separately using the Modified Beer Lambert Law (MBLL) [10]. The individual results are block averaged by multiple trials in each task and grand averaging was conducted to calculate representative result in each group. These data times were baseline corrected with respect to the start of the trial. The final output of each optode was then reported as mean total oxygenated hemoglobin (HbO µm).
As all participants included in the study were right-hand dominant with a presumed left sided cerebral dominance, the Left region channels (#33–48) were the focus of analysis. Grouping of the NIRSIT channels is illustrated in Fig. 3. This correlates anatomically to the left anterior PFC containing the Dorsolateral PFC cortex, Ventrolateral PFC cortex and Frontopolar cortex. The Centre region (#17–32) was omitted from analysis as previous literature has shown the medial PFC to be commonly engaged by social and emotional processes in adolescents aged up to 23 years old [11]. As the mean age of our participants fell within the adolescent category, the activation of the medial PFC due to adolescent-motivated social behaviour lacked relevance in this study.

48 Channels and the manner of grouping during data analysis. Left region channels (#33–48.)
The PFCA recorded during the pre-intervention assessment serves as a baseline to which the PFCA recorded during the post-intervention assessment can be compared against. The primary outcome of the study is therefore the difference in HbOµm between post- and pre-intervention readings (ΔHbOµm = (Post-intervention HbOµm) − (Pre-intervention HbOµm)) for each of the four laparoscopic tasks.
To demonstrate the differences in PFCA, prefrontal topographical maps are used to represent the various areas of prefrontal cortex activation during task performance. The intensity of red colour represents increased oxygenated hemoglobin levels detected in that region of the prefrontal cortex, and thus correlates with increased activation and cognitive effort. The converse holds true with a dark blue colour representing reduced oxygenated hemoglobin levels and hypo-activation of the region.
The participants’ performance during each of the four tasks pre- and post-intervention were recorded into a video. The video recorded only the hand movements and manipulation of the laparoscopic simulator to allow blinding of the assessors to the identities of the participants. The videos was assessed in a random order by two independent consultants that were not involved in the training of the intervention group. The pre- and post-intervention performance was graded using a Likert scale on a originally designed marking scheme (Objective Structured Assessment of Technical Skills Scores) (Table 1).
Sample size and statistical analysis
As this is a pilot study, a sample size of 30 or more is deemed adequate [12]. To investigate the PFC hemodynamic changes, the representative value (\(\Delta {HbO}_{2}\upmu \mathrm{m}\)) was extracted by averaging the block averaged HbO2µm in each channels depending on individual left and right separation. The right region refers to channels 1–16 and left region channels 33–48, as shown in Fig. 3. Since the specific location of each channels in MNI coordinates are different within subject, regional grouping can robustly calculate regional representative value at left and right region. The Kolmogorov–Smirnov test and the Shapiro–Wilk test was used to test normality of \((\Delta {HbO}_{2} \upmu \mathrm{m}\)) Trained and Untrained groups and tasks as well as each sex. Between-groups differences were evaluated using unpaired t tests. We also conducted pre-specified subgroup analyses by sex. All statistical analyses were performed using IBM SPSS Statistics 21 (SPSS Inc., Chicago, Ill., USA). The criterion for statistical significance was set at p < 0.05.
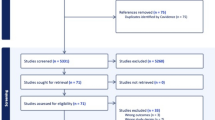
The CONSORT diagram for randomization is illustrated in Fig. 4.

CONSORT diagram of prospective, parallel randomised controlled trial to compare PFCA attenuation between “Trained-group” and “Untrained-group”
Results
32 participants were assessed for eligibility and all consented to participate. They were randomised to ‘Trained’ and ‘Untrained’ group, with 16 participants in each group. Data from 1 male participant in the ‘Untrained’ group was excluded due to technical issues during the fNIRS recording. A total of 15 participants from the ‘Untrained’ group and 16 participants from the ‘Trained’ group were studied, and the results were analysed. Participant baseline demographic information studied showed no significant difference (Table 2).
No significant statistical difference was noted upon analysis of the right region channels (#1–16) across all tasks between Trained and Untrained and on subgroup analysis. This is in keeping with the participant’s right-hand dominance and presumed left sided cerebral dominance.
Figure 5 shows the statistical difference in ΔHbOµm between Trained and Untrained individuals during Precision cutting (p = 0.007). During the Precision cutting task, Trained individuals demonstrated an attenuation in left PFCA, whereas Untrained individuals had a greater increase in left PFCA.

Difference in PFC activation (HbOµm) between post- and pre-intervention readings of Trained and Untrained individuals during the Precision cutting task
No statistically significant difference was observed between the 2 groups during Peg transfer, Suture insertion and Intracorporeal knotting.
Subgroup analysis by sexes showed statistically significant differences in ΔHbOµm between Trained and Untrained females during the first two tasks: Peg transfer (p = 0.005) and Precision cutting (p = 0.003). Figure 6 and Fig. 7 shows Trained females consistently demonstrating an attenuation in left PFCA, whereas Untrained females had a greater increase in left PFCA while performing Peg transfer and Precision cutting, respectively. No statistically significant difference was observed during Suture insertion and Intracorporeal knotting.

Difference in PFC activation (HbOµm) between post- and pre-intervention readings of Trained and Untrained females during the Peg transfer task

Difference in PFC activation (HbOµm) between post- and pre-intervention readings of Trained and Untrained females during the Precision cutting task
No statistically significant difference in ΔHbOµm was observed between Trained and Untrained males during all four tasks.
Table 3 demonstrates a summary of the significance testing on the Objective Structured Assessment of Technical Skills Scores. Across all 4 tasks, there was significant improvement in objective scores amongst Untrained participants during their post-intervention performance as noted during the assessment of the videos (p < 0.05). In Trained participants, an increase in objective scores during their post-intervention performance was only observed across the first two tasks: Peg transfers (p = 0.002) and Precision cutting (p < 0.000), However, there is no statistically significant difference observed between Trained versus Untrained participants in their objective scores for their performance. We also did not observe a difference of scores between Trained versus Untrained females.
Discussion
The purpose of the study was to examine the effects of a one-to-one laparoscopic surgical training workshop on student’s PFC cortex activity. Using an Endo Trainer with a fixed set of laparoscopic tasks and fNIRS device to record cortical hemodynamic activity. Secondary objectives included examining any sex differences that might be present.
The underlying basis of measuring PFCA during each laparoscopic task is based on the premise that with sufficient practice and attainment of proficiency, a motor task would require progressively less cognitive load (visuomotor integration, visuospatial working memory, performance monitoring etc.). Correspondingly, PFC activation would decrease as the actions becomes more “automatic” to the participant. This is based on previous studies where expert surgeons were found to have a significantly attenuated PFCA levels as compared to novice surgeons performing simple suturing [4]. Leff et al. [3] examined cortical correlates of technical skills acquisition and found that PFC processing across five knot-tying trials is influenced by the level of experience on a task, with relative decreases in HBO2 with successive trials. After getting participants to perform simple tasks like sequence keypresses and go-no-go key pressing tasks, Lage et al. [13] similarly observed that “the consecutive repetition of a motor task resulted in decreased DLPFC (Dorsolateral PFC cortex) activity”. Thus, these studies have observed predictable attenuation in PFC response alongside improvement in technical performance; and we seek to examine if a similar effect is seen in students acquiring laparoscopic skills.
Difference between Trained and Untrained individuals and sexes
We report that a one-to-one laparoscopic workshop appears to cause a significant PFC attenuation in the Precision cutting task only, compared to Untrained individuals. While this is in line with our hypothesis that increased training would lead to automation of task and decreased PFC activation, it was unusual that amongst the four tasks completed, only the second task yielded significant results. We expect the least cognitively challenging task, Peg transfer, to have yielded significant results instead. This, along with differences between sexes noted in prior studies, prompted a subgroup analysis on sexes and led to further insight into our preliminary results.
Here, for the first time, we report that one-to-one laparoscopic training results in significant differences in PFC attenuation between female and male medical students. Significant PFC attenuation was observed amongst female medical students for the first two laparoscopic tasks. On the contrary, this phenomenon was not observed in the Trained male students for any of the four tasks. Therefore, sex is a confounder in our analysis of Trained versus Untrained individuals and may explain the initial paucity of statistically significant results observed.
In female medical students the surgical training workshop caused a comparatively lower absolute activation of the Left PFC for the first two tasks, which are found to be less technically challenging and easier to complete. This is in keeping with our hypothesis, as these motor tasks would be easier to master, and hence Trained participants would require lesser activation of the PFC during the completion of each task during their post-intervention assessment.
The lack of decreased PFC activation found in the Suture insertion and Intracorporeal knotting task is expected. These tasks requires the participant to attain proficiency in depth perception, eye-hand coordination, ambidexterity and transferring skills. A tall task to ask of a novice medical student.
The literature explains this pattern of attenuation. Firstly, laparoscopic tasks are generally considered to be more technically challenging than simple knot tying or suturing. Ohuchida et al. [5] demonstrated that without training, novices failed to exhibit PFC responses during challenging laparoscopic tasks, affording them a pattern of brain activation similar to experts. Tasks that are too difficult may preclude novices from developing a cognitive strategy for successful motor performance, requiring them to rely more on luck rather than skill during initial attempts. Secondly, while the laparoscopic surgical training was provided by an expert consultant with individual attention granted, 45 min might have been too short of a duration. Previous studies had a greater amount of time dedicated to training or greater number of practice trials, e.g. Crewther et al. [14] had novices practice set sequences of intracorporeal suturing and knot tying for a baseline of 120 min, Shewokis et al. [15] had participants perform 108 acquisition trials using a laparoscopic simulator over 3 days (acquisition phase of 60–90 min of training) and Shetty et al. [4] had participants practice suturing skills for 2 h on the first session. The combination of technical complexity and insufficient training time might have resulted in the failure of participants to gain “automaticity” in intracorporeal knotting. Philipp Romero et al. had students and surgical residents undergo a 3 h training session for intracorporeal knot tying (ICKT) and that while students and residents improved in all categories for both ICKT techniques after training, they did not achieve expert level for task times and accuracy [16]. Felix Nickel et al. similarly found that medical students assigned to the simultaneous learning arm required approximately 91.1 min to obtain proficiency in laparoscopic suturing and knot tying with the C-loop technique [17].
Crewther et al. [14] observed no significant difference in PFC activation for intracorporeal knot tying, even after 8hrs of training and attributed the consistent PFC response to “The greater complexity of the laparoscopic tasks.” Shetty et al. [4] similarly observed a lack of attenuation in a group of novice surgeons despite progression towards near expert levels of suturing skill, noting that additional training failed to lead to progressive PFC attenuation.
The 4 tasks can be broadly grouped into 2 categories: Tasks 1 & 2(Peg transfer and Precision cutting) are considered “technically easy” while Tasks 3 & 4 (suture insertion and intracorporeal knotting) are considered “technically challenging”. Hence with the time constraints of a single training workshop, the benefits of basic skills (grasping and simple maneuvering) acquired in the completion of the various laparoscopic tasks, would feature more prominently in Tasks 1 & 2. Task 2 may seem to have a more significant difference between the “Trained” and “Untrained” group as the additional skills taught during the training workshop might have a greater value add in the completion of the 2nd task compared to the 1st task.
Interestingly, the Untrained group showed a slight increased HbO level in PFC in their post-intervention trials for the above-mentioned tasks. As the Untrained group would not be expected to obtain mastery without training, one would expect the pre- and post- intervention PFC activation levels to be similar. This could be explained by the fact that for tasks which are challenging, but achievable, i.e. Peg transfer and Precision cutting, Untrained participants had to struggle more to develop a cognitive strategy, requiring them to recruit more heavily from the PFC initially, whereas Trained participants had the experience required for relative attenuation of PFC compared to their counterparts [18]. Leff et al. [19] showed during intraoperative decision-making, novices had increased activation of PFC during “unprimed” intraoperative decisions”, where solutions were not apparent and they had to use effortful decision-making processes that require increased attention and concentration. While PFC was deactivated during “primed” intraoperative decisions, with acceptance of the observed decision and prefrontal disengagement. Such a pattern was similarly not observed in expert surgeons.
The difference in PFC responses to one-to-one laparoscopic training between males and females, is a phenomenon observed by other studies such as that of Donnon et al. [7] who studied the impact of cognitive imaging and sex differences on the development of laparoscopic suturing skills. While obtaining feedback on the preferred instructional approaches of teaching, one-to-one instruction was the preferred and only instructional technique ranked higher by female than male medical students. Strandbygaard et al. [8] also determined instructor feedbacks to have increased the efficiency regarding the amount of time and number of repetitions needed to reach a predefined proficiency level by medical students for a complex simulated operation. An additional sex specific difference includes the greater influence feedback had on women’s performance than that of men. Males outperformed females when instructor feedback was not given, while both males and females performed equally when instructor feedback was given.
Our study sheds light on the differing neurobiological responses during laparoscopic skill acquisition in females compared to males. It has also reaffirmed the significant benefits of a personal one-to-one laparoscopic tutorial in female medical students. The growing emphasis on laparoscopic proficiency, prompts us to acknowledge sex specific differences in laparoscopic education, to refine the current surgical education curriculum and give personalised training opportunities to each student. In addition, this study has shown that analysis of left region channels would be sufficient for right-handed individuals.
Our study also suggest that one-to-one laparoscopic training may improve performance as supported by the improvement seen in the objective scores from the assessment of the individual videos of the participants pre- and post-intervention performances; however, this was not statistically significant. We assume that this is likely due to the limited training time allocated during the study.
One could explore the use of a fNIRS device as a learning aid in assessing a student’s progress in the acquisition of laparoscopic technical skills, with an increased PFC attenuation possibly reflecting the extent of a student’s increased proficiency. This prospect is bolstered by Nemani et al. [20] study, which used fNIRS results to successful distinguish Trained and Untrained subjects in motor skill transfer from simulation to ex vivo environment, proving that fNIRS metrics are an objective means of classifying different levels of surgical motor skill transfer more accurately than alternative metrics such as checklists and task completion times.
There were several limitations in this study: First, the intervention group did not have any rest after their training. This may result in higher PFC baseline due to residual cognitive activity from the training. Second, there were limitations due to the nature of the fNIRS device used. PFC activation is inferred based on hemodynamic coupling and blood flow to various regions of the PFC. Blood flow is affected by gravity and despite instructions to keep their head level, participants inevitably tilted their heads during performance of each laparoscopic task, potentially affecting the recording of data. Third, while our study has proven that analysis of the left region channels is sufficient for right-handed individuals, our study did not include left-hand dominant individuals with possibly varied PFCA patterns. Fourth, the laparoscopic training provided was not standardised and instead tailored to each individual. While this improves external validity, with tutors commonly teaching students according to their varying aptitudes, individualised training makes it difficult to pinpoint which aspect of training resulted in the decreased cognitive load. Fifth, the training was conducted in only 45 min which may be insufficient for training a novice laparoscopic surgeon to perform four different laparoscopic tasks. Sixth, the assessment was also done in an artificial simulated environment such that the laparoscopic camera’s field of vision was fixed and centred within the Endo trainer. This prevented participants from adjusting the camera and reduces the generalizability of our results to surgical tasks in the operating theatre. Lastly, this is a pilot study with a small sample size of 32 participants, making the results susceptible to Type I error. While the absolute number is small, the sample size of this study is comparable to similar published studies [3,4,5, 7, 14,15,16,17]. This study nonetheless provides a foundation upon which future studies can be built upon, with the authors of this paper intending for a follow up study including surgical residents with a larger sample size.
Implications
The application of fNIRS devices as an adjunct tool in surgical laparoscopic education of medical students could prove beneficial. fNIRS devices may be used as a measure of progress in a student’s acquisition of laparoscopic technical skills, with attenuated PFC levels a reflection of mastery and an indicator for tutors to move onto the next skill. An observation of real time PFCA during laparoscopic tasks could also allow tutors to give immediate feedback to students, based on aspects of the surgical task student may find most cognitively challenging. Female medical student would also benefit from personalised one-to-one surgical training, which allows us to maximise the potential of each surgical trainee. Future studies should be performed to examine the relationship between repeated training sessions on medical student’s PFCA levels and its correlation to objective surgical performance. This could provide greater insight into the degrees of PFC attenuation and its correspondence to objective surgical clinical outcomes.
References
Yuan P, Naftali R (2014) PFC cortex and executive functions in healthy adults: a meta-analysis of structural neuroimaging studies. Neurosci Biobehav Rev 42:180–192. https://doi.org/10.1016/j.neubiorev
Chan RC, Shum D, Toulopoulou T, Chen EY (2008) Assessment of executive functions: review of instruments and identification of critical issues. Arch Clin Neuropsychol. https://doi.org/10.1016/j.acn.2007.08.010
Leff DR, Elwell CE, Orihuela-Espina F, Atallah L, Delpy DT, Darzi AW, Yang GZ (2008) Changes in PFC cortical behaviour depend upon familiarity on a bimanual co-ordination task: an fNIRS study. Neuroimage. https://doi.org/10.1016/j.neuroimage.2007.09.032
Shetty K, Leff DR, Orihuela-Espina F, Yang GZ, Darzi A (2016) Persistent PFC engagement despite improvements in laparoscopic technical skill. JAMA Surg 151:682e–e684. https://doi.org/10.1001/jamasurg.2016.0050
Ohuchida K, Kenmotsu H, Yamamoto A, Sawada K, Hayami T, Morooka K, Takasugi S, Konishi K, Ieiri S, Tanoue K, Iwamoto Y, Tanaka M, Hashizume M (2009) The frontal cortex is activated during learning of endoscopic procedures. Surg Endosc. https://doi.org/10.1007/s00464-008-0316-z
Andreu-Perez J, Leff DR, Shetty K, Darzi A, Yang GZ (2016) Disparity in frontal lobe connectivity on a complex bimanual motor task aids in classification of operator skill level. Brain Connectivity 6(5):375–388
Donnon T, DesCoteaux JG, Violato C (2005) Impact of cognitive imaging and sex differences on the development of laparoscopic suturing skills. Can J Surg 48:387–393
Strandbygaard J, Bjerrum F, Maagaard M, Winkel P, Larsen CR, Ringsted C, Gluud C, Grantcharov T, Ottesen B, Sorensen JL (2013) Instructor feedback versus no instructor feedback on performance in a laparoscopic virtual reality simulator: a randomized trial. Ann Surg 257:839–844
Choi J, Kim J, Hwang G, Yang J, Choi M, Bae H (2016) Time-divided spread-spectrum code-based 400 fW-detectable multichannel fNIRS IC for portable functional brain imaging. IEEE J Solid-State Circuits 51(2):484–495
Delpy DT, Cope M, van der Zee P, Arridge S, Wray S, Wyatt J (1988) Estimation of optical pathlength through tissue from direct time of flight measurement. Phys Med Biol 33(12):1433–1442
Somerville LH, Jones RM, Ruberry EJ, Dyke JP, Glover G, Casey BJ (2013) Medial prefrontal cortex and the emergence of self-conscious emotion in adolescence. Psychol Sci 24(8):1554–1562
Lancaster GA, Dodd S, Williamson PR (2004) Design and analysis of pilot studies: recommendations for good practice. J Eval Clin Pract 10(2):307–312
Lage GM, Ugrinowitsch H, Apolinario-Souza T, Vieira MM, Albuquerqe MR, Benda RN (2015) Repetition and variation in motor practice: a review of neural correlates. Neurosci Biobehav Rev 57:132–141
Crewther BT, Shetty K, Jarchi D, Selvadurai S, Cook CJ, Leff DR, Darzi A, Yang GZ (2961e) Skill acquisition and stress adaptations following laparoscopic surgery training and detraining in novice surgeons. Surg Endosc 30:2961e–2968
Shewokis PA, Shariff FU, Liu Y, Ayaz H, Castellanos A, Lind DS (2017) Acquisition, retention and transfer of simulated laparoscopic tasks using fNIR and a contextual interference paradigm. Am J Surg 213:336–345
Philipp R, Felix N, Maisha M, Giovanni F, Alina R, Karl-FK BPMS, Patrick G (2017) Intracorporal knot tying techniques—which is the right one? J Pediatric Surg 52:633–638
Hendrie JD, Nickel F, Bruckner T et al (2016) Sequential learning of psychomotor and visuospatial skills for laparoscopic suturing and knot tying—study protocol for a randomized controlled trial “the shoebox study”. Trials 17:1–7. https://doi.org/10.1186/s13063-015-1145-8
Modi HN, Singh H, Yang GZ, Darzi A, Leff DR (2017) A decade of imaging surgeons' brain function (part II): a systematic review of applications for technical and nontechnical skills assessment. Surgery 162(5):1130–1139
Leff DR, Yongue G, Vlaev I, Orihuela-Espina F, James D, Taylor MJ et al (2017) Contemplating the next maneuver: functional neuroimaging reveals intraoperative decision-making strategies. Ann Surg 265:320–330
Nemani A, Kruger U, Cooper CA, Schwaitzberg SD, Intes X, De S (2018) Objective assessment of surgical skill transfer using non-invasive brain imaging. Surg Endosc. https://doi.org/10.1007/s00464-018-6535-z
Author information
Authors and Affiliations
Contributions
Conceptualisation: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne, Davide Lomanto, Ho Pei, Roger C.M. Ho. Data curation: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne, Hrishikesh Salgaonkar. Formal analysis: Choi JK, JiYeong Baek, Howard C.H. Khoe, Jun Wei Low, Wilson W. Tam. Investigation: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne, Roger C.M. Ho. Methodology: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne, Davide Lomanto, Ho Pei, Roger C.M. Ho. Project administration: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne, Roger C.M. Ho. Resources: Sujith Wijerathne, Davide Lomanto, Ho Pei, Roger C.M. Ho. Software: Choi JK, JiYeong Baek. Supervision: Sujith Wijerathne, Davide Lomanto, Ho Pei, Roger C.M. Ho, Lui Su Ann. Validation: Wilson W. Tam. Writing—original draft preparation: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne. Writing—review & editing: Howard C.H. Khoe, Jun Wei Low, Sujith Wijerathne, Davide Lomanto, Ho Pei, Roger C.M. Ho, Lui Su Ann. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Disclosure
Dr Howard C.H. Khoe, Dr Jun Wei Low, Dr Sujith Wijerathne, Dr Hrishikesh Salgaonkar, Dr Davide Lomanto, Mr Choi JK, Ms JiYeong Baek, Dr Wilson W. Tam, Dr Ho Pei, Dr Roger C.M. Ho, Dr Lui Su Ann have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Khoe, H.C.H., Low, J.W., Wijerathne, S. et al. Use of prefrontal cortex activity as a measure of learning curve in surgical novices: results of a single blind randomised controlled trial. Surg Endosc 34, 5604–5615 (2020). https://doi.org/10.1007/s00464-019-07331-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07331-7