
Abstract
Background
Radical resection is the only curative option for patients with hilar cholangiocarcinoma (HCCA) to achieve long-term survival. However, due to the fact that radical resection of HCCA has high technical requirements, the safety and efficacy of laparoscopic resection for HCCA remains controversial.
Method
From January 2015 to December 2018, 23 cases of HCCA underwent radical resection in our center. Clinical data of those patients were collected and analyzed retrospectively.
Results
14 patients underwent laparoscopic resection and 9 cases received open resection. 2 patients in laparoscopic group were converted to laparotomy. Operation time in laparoscopic group was significantly longer than that in open group (519.4 ± 155.4 min vs 366.7 ± 93.1 min). Estimated blood loss (620.0 ± 681.2 ml vs 821.4 ± 713.8 ml) and incidence of intraoperative blood transfusion (5/9 vs 8/14) did not differ significantly between two groups. Pathological outcomes were comparable between two groups. Length of postoperative hospital stay (23.4 ± 13.4 days vs 17.8 ± 7.1 days), severe postoperative morbidity (3/9 vs 5/14), bile leakage of Grade A or B (5/9 vs 5/14), intra-abdominal bleeding (0/9 vs 1/14), intra-abdominal abscess (1/9 vs 0/14), wound infection (0/9 vs 1/14), pulmonary infection (2/9 vs 0/14), and liver failure (0/9 vs 0/14) did not differ significantly between two groups. One patient in laparoscopic group died (1/14) at 21 postoperative days due to intra-abdominal bleeding, while no 30-day mortality was observed in open group.
Conclusion
Our results demonstrate that laparoscopic radical resection of HCCA is safe and feasible in experienced hands. Although laparoscopic resection for HCCA, which is still in initial and exploratory stage, fails to show any advantage over open resection in this study, we are optimistic with its wide application in future with the improvement of surgical techniques and experience.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Surgical resection of HCCA remains one of the greatest challenges for hepatobiliary surgeons [1]. Radical resection of HCCA has high technical requirements that encompass lymph nodes dissection, extended hepatectomy with caudate lobe, cholangiojejunostomy, and vascular reconstruction if necessary. Minimally invasive operations, including laparoscopic and robotic operations, have been commonly performed for the treatment of benign hepatobiliary diseases and result in faster recovery and less postoperative complication. However, due to the high technical requirements, laparoscopic approach has limited application in radical resection of HCCA. Only limited publications reported this minimally invasive approach for HCCA. Here we reported the experience and data in our center regarding the safety and feasibility of laparoscopic radical resection for HCCA.
Methods
Patients’ cohort and data collection
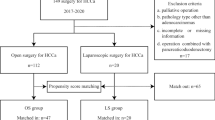
From January 2015 to December 2018, 23 cases of HCCA received radical resection in our center, of which 14 underwent laparoscopic surgery. No patient was explored and deemed unresectable during this time period. Clinical data were collected and analyzed retrospectively. The protocol of this study was approved by the ethics committee of Zhejiang Provincial People’s Hospital.
Preoperative management
Ultrasonography, computed tomography, and magnetic resonance imaging were routinely performed to evaluate the resectability of HCCA including tumor size, the involvement of surrounding blood vessels, and the extent of longitudinal involvement. CT scan for the calculation of future liver volume was carried out. The function of future liver remnant was assessed by liver function test and indocyanine green assay. For patients with elevated total serum bilirubin level (> 100 μmol/l), percutaneous trans-hepatic biliary drainage (PTBD) was performed prior to operation to relieve the obstruction of biliary tract.
Surgical procedure
Laparoscopic and open radical resections of HCCA were performed following the same principles and procedures. For HCCA patients of type I, resection of extrahepatic bile ducts and dissection of lymph nodes were performed. For cases of type II, resection of extrahepatic bile ducts and caudate lobe along with the dissection of lymph nodes was performed. For those classified as type III or type IV, resection of hepatic segments, caudate lobe, and extrahepatic bile ducts along with the dissection of lymph nodes was performed. For laparoscopic approach, a five-port method was used and the position of trocars is shown in Fig. 1. Intraoperative ultrasound was routinely performed to determine and evaluate the potential intrahepatic metastasis. Subsequent to Kocher maneuver for duodenum mobilization, dissection of regional lymph nodes (No. 16 a2/b1 and No. 13, Fig. 2) and transection of the bile duct at the upper border of the pancreatic head were performed. Lymph nodes in suprapancreatic area were then dissected (Fig. 3). After cholecystectomy, the inflow of the right or left liver was occluded and divided. The right or left lobes and caudate lobe were completely mobilized and transected in an en bloc manner (Fig. 4). Lastly, the biliary-enteric reconstruction was performed using end-to-side anastomosis between segmental ducts and Roux-en-Y jejunal loop without any stent. Before intrahepatic cholangiojejunostomy, ductoplasty of intrahepatic bile ducts was performed if necessary (Fig. 5). Surgical view after laparoscopic cholangiojejunostomy was demonstrated in Fig. 6.

The schematic diagram of distribution of trocar pores for HCCA

Dissection of regional lymph nodes (No. 16 a2/b1 and No. 13) after Kocher maneuver. BD bile duct, UP uncinate process, IVC Inferior vena cava, LRV left renal vein

Dissection of lymph nodes in suprapancreatic area. RHA right hepatic artery, MHA middle hepatic artery, LHA left hepatic artery, PV portal vein, GDA gastroduodenal artery

Left hemi-liver and total caudate lobe were completely removed. RHA right hepatic artery, RPV right portal vein, IVC Inferior vena cava, MHV middle hepatic vein

Ductoplasty of intrahepatic bile ducts after left hemi-hepatectomy. Here the bile duct orifices of segment VI, VII, and VIII were joined together to prepare for a cholangiojejunostomy between right hepatic duct and jejunum. B5 bile duct of segment V, B6+7+8 bile duct of segment VI, VII, and VIII

Surgical view after laparoscopic cholangiojejunostomy. Bile ducts of segment of VI–VIII were subjected to ductoplasty and anastomosed with the jejunum. Bile duct of segment V was anastomosed with jejunum. B5 bile duct of segment V, B6+7+8 bile duct of segment VI, VII, and VIII
Postoperative treatment
Postoperative total parenteral nutrition (TPN) was administered before restoring oral intake. Patients usually restored oral diet at 2 to 3 days after operation. Enhanced CT was examined 3 to 5 days after operation to evaluate the intra-abdominal condition. Severe complications were defined as those of Clavien–Dindo grade III and IV [2]. Bile leakage was evaluated and graded according to the definition of international study group of liver surgery [3].
Adjuvant therapy
Gemcitabine alone or gemcitabine plus S-1 (tegafur–gimeracil–oteracil potassium) [4] was recommended to patients as adjuvant therapy after radical resection. No patients received postoperative radiation in our study.
Statistical analysis
Statistical analysis was performed using SPSS 13.0 statistical software (SPSS Inc, Chicago, IL). χ2 or Fisher exact test and Mann–Whitney U test were used to evaluate the statistical difference between groups for categorical variables and continuous variables, respectively. Kaplan–Meier method and log rank test were employed to compare the overall survival between two groups. Difference with P values < 0.05 was considered to be statistically significant.
Results
Preoperative characteristics
A total of 23 HCCA patients was enrolled in this study, of which 14 underwent laparoscopic procedure and 9 underwent open procedure. 2 Patients in laparoscopic group were converted to laparotomy due to the fact that the portal vein was invaded by the tumor. Preoperative data was presented in Table 1. There were 3 male and 6 female patients in open group versus 7 male and 7 female patients in laparoscopic group (P = 0.67). The mean age was 65.4 ± 6.9 and 65.4 ± 8.9 years in open and laparoscopic group (P > 0.99), respectively. BMI of patients did not differ significantly between two groups (22.8 ± 1.9 vs 23.1 ± 3.1, P = 0.75). The level of total Bilirubin (231.4 ± 153.1 vs 139.0 ± 115.7, P = 0.11) and the incidence of preoperative PTBD (6/9 vs 7/14, P = 0.67) were comparable between groups. The distributions of Bismuth types of HCCA were 0/0/8/1 and 5/0/8/1 for type I/II/III/IV in open and laparoscopic group (P = 0.37), respectively.
Intraoperative data
HCCA patients of type IIIa, IIIb, and IV underwent extended hemi-hepatectomy combined with caudate lobectomy in two groups. Intraoperative data for laparoscopic group and laparotomy group was presented in Table 2. Operation time was significantly longer in laparoscopic group than that in open group (366.7 ± 93.1 min vs 519.4 ± 155.4 min, P = 0.01). Estimated blood loss was comparable between two groups (620.0 ± 681.2 ml vs 821.4 ± 713.8 ml, P = 0.50). 6 patients had intraoperative blood transfusion in open group, while the number was 8 in laparoscopic group (6/9 vs 8/14, P > 0.99). Pathological outcomes including the incidence of microscopically R0 margins (7/9 vs 14/14, P = 0.14), tumor diameter (2.82 ± 2.04 cm vs 2.26 ± 0.79 cm, P = 0.35), and the number of dissected lymph nodes (6.13 ± 5.96 vs 9.73 ± 6.76, P = 0.21) did not differ significantly between two groups.
Postoperative outcomes
The comparison of postoperative outcomes between two groups was demonstrated in Table 3. The length of postoperative stay (23.4 ± 13.4 days vs 17.8 ± 7.1 days, P = 0.20), the incidence of severe morbidity which was defined as Clavien–Dindo grade III–V (3/9 vs 5/14, P > 0.99), bile leakage of Grade A or B [3] (5/9 vs 5/14, P = 0.42), intra-abdominal bleeding (0/9 vs 1/14, P > 0.99), intra-abdominal abscess (1/9 vs 0/14, P = 0.39), wound infection (0/9 vs 1/14, P > 0.99), pulmonary infection (2/9 vs 0/14, P = 0.14), and liver failure (0/9 vs 0/14, P > 0.99) did not differ significantly between the open and laparoscopic group. One patient (1/14) died at 21 postoperative days in laparoscopic group. This patient had intra-abdominal bleeding and underwent relaparotomy. Unfortunately, this patient died of abdominal infection subsequent to relaparotomy. No 30-day mortality was observed in the open surgery group (P > 0.99).
OS rate of patients treated with open surgery was relatively higher than those who underwent laparoscopic surgery (P = 0.191, Fig. 7), with 1-, 2-year OS rate of 75% and 62.5% for open surgery group versus 62.5% and 25% for laparoscopic group, respectively.

Comparison of Overall survival (OS) for patients in laparoscopic group and laparotomy group
Discussion
With the development of laparoscopic devices, accumulated experience of laparoscopic surgery, and improvement of surgical techniques, laparoscopic approach has been widely used in various abdominal operations. Recently, surgeons began to explore laparoscopic approach for the radical resection of HCCA. Among 12 HCCA cases who underwent laparoscopic resection reported by Yu et al. [5], 7 cases were type I and 5 cases were type II. Li et al. [6] reported 9 cases of patients who underwent laparoscopic resection of HCCA, with 1 case of type I, 3 of type II, 2 of type IIIb, and 3 of type IV. Lee et al. [7] reported 5 cases of HCCA who underwent laparoscopic resection, with 1 case of type I, 1 of type II, 1 of type IIIa, and 2 of type IIIb. In addition to these studies, there were several case reports describing laparoscopic resection of HCCA [8,9,10]. However, in these publications, hepatic caudate lobe resection was not performed, which was believed to be crucial for radical resection of HCCAs of Bismuth type IIIa, IIIb, and IV [11]. In 2013, Cho et al. [12] performed extended laparoscopic resection of HCCA including left hepatectomy, caudate lobectomy, and pylorus-preserving pancreaticoduodenectomy for an 80-year-old patient with advanced HCCA, which was considered as the first case of laparoscopic extended hepatectomy combined with caudate lobectomy. Lee et al. [7] reported extended hepatectomy combined with caudate lobectomy for HCCAs of Bismuth IIIa and IIIb. In 2017, we also reported a HCCA case of Bismuth IIIa and performed laparoscopic right hemi-hepatectomy combined with caudate lobe resection [10]. In the present study, caudate lobe resection was performed in all HCCAs of type III and IV. These patients showed acceptable short-term outcomes and postoperative survival. Therefore, we believe that laparoscopic radical resection for HCCA is technically safe and feasible and can achieve satisfactory oncological adequacy in surgeons with rich laparoscopic experience.
Since the experience of laparoscopic radical resection of HCCA is very limited, there is no consensus on the indications of this procedure which vary between different centers and these indications are influenced by laparoscopic techniques and surgical experience in each center. In our department, the indications for laparoscopic resection for HCCA are basically the same as those for open resection. Laparoscopic approach is not chosen for HCCA cases who may need vascular reconstruction based on preoperative evaluation.
There is no doubt that laparoscopic radical resection of HCCA is still a technically challenging operation. Technical difficulties include extended hepatectomy combined with caudate lobe resection, meticulous dissection of peri-hilar structures, and biliary-enteric reconstruction under laparoscopy. With accumulated experience of laparoscopic resection of hepatic caudate lobe, pancreatoduodenectomy, and other laparoscopic procedures which showed satisfactory safety and efficacy [13, 14], we believe that the required surgical techniques during laparoscopic resection of HCCA have been mature and reliable. The data in our study which showed non-inferior feasibility and safety of laparoscopic approach compared with open approach also supported this notion.
It is encouraging to mention that laparoscopic surgery was associated with relatively higher lymph nodes yield and shorter postoperative hospital stay in our study. But the differences between groups did not reach statistical significance due to the small number of included cases. There was no statistical difference regarding the OS between the two groups, with relatively lower two-year survival in laparoscopic group. We started laparoscopic surgery for HCCA in 2017. Therefore, the follow-up length for these cases were mostly less than 2 years which could lead to a decreased 2-year survival. On the other hand, our data revealed that laparoscopic procedures were associated with prolonged operation time. Intraoperative bleeding was relatively higher in laparoscopic group. We believe that these disadvantages are probably due to the fact that laparoscopic approach for HCCA is still at its initial stage. With the improvement of surgical techniques and accumulation of laparoscopic experience, operation time as well as intraoperative bleeding of laparoscopic resection of HCCA will gradually decrease. This progress is commonly observed in the development process of other laparoscopic surgeries. These opinions can be further confirmed by comparative studies with a larger number of enrolled cases in the future.
It is worth to note here that one patient encountered postoperative bleeding in laparoscopic group. The reason for the postoperative bleeding was found to be hepatic artery pseudoaneurysm during relaparotomy. We speculated that an excessive dissection of lymph nodes around the hepatic artery, which resulted in the mechanical injury of vessel, was probably the reason for the occurrence of hepatic artery pseudoaneurysm.
Although laparoscopic cholecystectomy was not widely accepted and failed to show any advantage over open surgery in its initial stage, it has now become the gold standard for cholecystectomy. Similar progresses can also be observed in other laparoscopic surgeries including laparoscopic hepatectomy and laparoscopic pancreatoduodenectomy, which are now been gradually accepted. Laparoscopic resection of HCCA is currently at the initial stage with rapid development. Our data reveals that laparoscopic resection of HCCA showed acceptable efficacy in most perioperative outcomes compared with open surgery. With the improvement of surgical techniques and experience in the future, laparoscopic radical resection for HCCA can promisingly become the routine approach in experienced centers and surgeons.
References
Nagino M (2012) Perihilar cholangiocarcinoma: a surgeon’s viewpoint on current topics. J Gastroenterol 47:1165–1176
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Koch M, Garden OJ, Padbury R, Rahbari NN, Adam R, Capussotti L, Fan ST, Yokoyama Y, Crawford M, Makuuchi M, Christophi C, Banting S, Brooke-Smith M, Usatoff V, Nagino M, Maddern G, Hugh TJ, Vauthey JN, Greig P, Rees M, Nimura Y, Figueras J, DeMatteo RP, Buchler MW, Weitz J (2011) Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the International Study Group of Liver Surgery. Surgery 149:680–688
Miyata T, Okabe H, Chikamoto A, Yamao T, Umezaki N, Tsukamoto M, Kitano Y, Arima K, Nakagawa S, Imai K, Hashimoto D, Yamashita YI, Baba H (2017) A long-term survivor of hilar cholangiocarcinoma with resection of recurrent peritoneal dissemination after R0 surgery: a case report. Surg Case Rep 3:110
Yu H, Wu SD, Chen DX, Zhu G (2011) Laparoscopic resection of Bismuth type I and II hilar cholangiocarcinoma: an audit of 14 cases from two institutions. Dig Surg 28:44–49
Li J, Zhao L, Zhang J, Li Z, Li A, Wei Y, Xu J (2017) Application of the laparoscopic technique in perihilar cholangiocarcinoma surgery. Int J Surg 44:104–109
Lee W, Han HS, Yoon YS, Cho JY, Choi Y, Shin HK, Jang JY, Choi H (2015) Laparoscopic resection of hilar cholangiocarcinoma. Ann Surg Treat Res 89:228–232
Machado MA, Makdissi FF, Surjan RC, Mochizuki M (2012) Laparoscopic resection of hilar cholangiocarcinoma. J Laparoendosc Adv Surg Tech Part A 22:954–956
Puntambekar S, Sharma V, Kumar S, Mitkare S, Joshi G, Parikh H (2016) Laparoscopic management of hilar cholangiocarcinoma: a case report. Indian J Surg 78:57–59
Zhang CW, Liu J, Hong DF, Wang ZF, Hu ZM, Huang DS, Shang MJ, Yao WF (2017) Pure laparoscopic radical resection for type IIIa hilar cholangiocarcinoma. Surg Endosc 32(3):1581–1582
Nimura Y, Hayakawa N, Kamiya J, Kondo S, Shionoya S (1990) Hepatic segmentectomy with caudate lobe resection for bile duct carcinoma of the hepatic hilus. World J Surg 14:535–543 (discussion 544)
Cho A, Yamamoto H, Kainuma O, Muto Y, Yanagibashi H, Tonooka T, Masuda T (2014) Laparoscopy in the management of hilar cholangiocarcinoma. World J Gastroenterol 20:15153–15157
Wang M, Peng B, Liu J, Yin X, Tan Z, Liu R, Hong D, Zhao W, Wu H, Chen R, Li D, Huang H, Miao Y, Liu Y, Liang T, Wang W, Cai Y, Xing Z, Cheng W, Zhong X, Zhao Z, Zhang J, Yang Z, Li G, Shao Y, Lin G, Jiang K, Wu P, Jia B, Ma T, Jiang C, Peng S, Qin R (2019) practice patterns and perioperative outcomes of laparoscopic pancreaticoduodenectomy in China: a retrospective multicenter analysis of 1029 patients. Ann Surg. https://doi.org/10.1097/SLA.0000000000003190
Salloum C, Lahat E, Lim C, Doussot A, Osseis M, Compagnon P, Azoulay D (2016) Laparoscopic isolated resection of caudate lobe (segment 1): a safe and versatile technique. J Am Coll Surg 222:e61–e66
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
All authors including Yuhua Zhang, Changwei Dou, Weiding Wu, Jie Liu, Liming Jin, Zhiming Hu, and Chengwu Zhang have no conflicts of interest or financial ties to disclose.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Zhang, Y., Dou, C., Wu, W. et al. Total laparoscopic versus open radical resection for hilar cholangiocarcinoma. Surg Endosc 34, 4382–4387 (2020). https://doi.org/10.1007/s00464-019-07211-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-019-07211-0