
Abstract
Purpose
To compare the short-term and oncologic outcomes of patients with pancreatic ductal adenocarcinoma (PDAC) undergoing laparoscopic distal pancreatectomy (LDP) and open distal pancreatectomy (ODP).
Methods
Consecutive cases of distal pancreatectomy (DP) (n = 422) were reviewed at a single high-volume institution over a 10-year period (2005–2014). Inclusion criteria consisted of any patient with PDAC by surgical pathology. Ninety-day outcomes were monitored through a prospectively maintained pancreatic resection database. The Social Security Death Index was used for 5-year survival. Two-way statistical analyses were used to compare categories; variance was reported with standard error of the mean; * indicates P value <0.05.
Results
Seventy-nine patients underwent DP for PDAC. Thirty-three underwent LDP and 46 ODP. There were no statistical differences in demographics, BMI, and ASA classification. Intraoperative and surgical pathology variables were comparable for LDP versus ODP: operative time (3.9 ± 0.2 vs. 4.2 ± 0.2 h), duct size, gland texture, stump closure, tumor size (3.3 ± 0.3 vs. 4.0 ± 0.4 cm), lymph node harvest (14.5 ± 1.1 vs. 17.5 ± 1.2), tumor stage (see table), and negative surgical margins (77 vs. 87%). Patients who underwent LDP experienced lower blood loss (310 ± 68 vs. 597 ± 95 ml; P = 0.016*) and required fewer transfusions (0 vs. 13; P = 0.0008*). Patients who underwent LDP had fewer positive lymph nodes (0.8 ± 0.2 vs. 1.6 ± 0.3; P = 0.04*) and a lower incidence of type C pancreatic fistula (0 vs. 13%; P = 0.03*). Median follow-up for all patients was 11.4 months. Long-term oncologic outcomes revealed similar outcomes including distant or local recurrence (30 vs. 52%; P = 0.05) and median survival (18 vs. 15 months), as well as 1-year (73 vs. 59%), 3-year (22 vs. 21%), and 5-year (20 vs. 15%) survival for LDP and ODP, respectively.
Conclusions
The results of this series suggest that LDP is a safe surgical approach that is comparable from an oncologic standpoint to ODP for the management of pancreatic adenocarcinoma.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Pancreatic ductal adenocarcinoma (PDAC) is a known aggressive malignancy for which open pancreatectomy had long been the only method to extirpate the primary lesion. In the last two decades, there has been an increased emphasis on and increased use of minimally invasive techniques in all fields of surgery. Minimally invasive techniques have long been used for benign conditions and have been shown to lead to shorter hospital stays, decreased pain, expedited postoperative recovery, reduced morbidity, and cost savings [1–5]. However, there was a slower adoption of these methods in the setting of malignancy for fear of inferior oncologic outcomes [6–9]—pancreatic malignancies being no exception [10].
The first evidence of equivalent oncologic outcomes in an open versus laparoscopic surgical comparison of the treatment for gastrointestinal malignancies was reported by the Clinical Outcomes of Surgical Therapy Study Group in 2004 [9]. This randomized, controlled clinical trial demonstrated no difference in oncologic outcomes for patients undergoing laparoscopic or open colectomy for colorectal cancer.
Pancreatic surgery is undoubtedly technically challenging due to the close proximity of the pancreas to many critical structures, its retroperitoneal location, and the high association with postoperative complications. Yet, with improvement in tissue sealing energy devices and staplers as well as increasing surgeon comfort level, minimally invasive pancreatic surgery continues to grow in popularity and practice. Multiple studies have reported that laparoscopic distal pancreatectomy (LDP) can be performed safely without increasing operative time while still retaining benefits of the minimally invasive approach such as reduced length of stay, shorter recovery times, earlier return to diet, and reduced blood loss. These studies, however, largely focus on LDP for benign or premalignant lesions [1, 2, 11–14].
Here we report one of the largest, single-institution, North American experiences of LDP for PDAC with direct comparison to a contemporary cohort of open distal pancreatectomy (ODP). The aim of this study was to compare short-term and oncology-specific outcomes of patients with PDAC following LDP and ODP. Our hypothesis was that LDP would have oncologic equivalence while demonstrating a patient safety benefit via improved postoperative morbidity when compared directly to ODP.
Methods
Patient population
Prospectively collected data on 422 consecutive cases of distal pancreatectomy (DP) performed at our tertiary referral center during a 10-year period—between 2005 and 2014—were reviewed. Patients undergoing DP for diagnoses other than PDAC were excluded from our analysis. The remaining patients were grouped by operative approach—minimally invasive (laparoscopic or robotic) versus open. Patients who required conversion from the laparoscopic approach to the open approach were analyzed with the laparoscopic cases under the intention-to-treat principle. All pancreatectomies (100% procedure targeting) were monitored with complete 30-day outcomes through the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). Complete 90-day outcomes were monitored with a prospectively maintained pancreatectomy database. Within this database, we collated and verified the accuracy of all perioperative clinical data combining the ACS-NSQIP data (30 days) and prospectively monitored institutional data (90 days) for all patients undergoing pancreatectomy. Long-term survival was monitored through the review of electronic medical records as well as the Social Security Death Index for median and 5-year survival.
Operative procedures
At our institution, the decision to perform a LDP is guided by clinical judgment, preference, and comfort of the individual surgeon rather than absolute institutional guidelines. However, all hepatopancreatobiliary surgeons utilize similar criteria to determine if a tumor can be resected. Stump closure was addressed in four manners—with sutured, stapled, reinforced stapled, or saline-linked radiofrequency ablation. Surgeon preference determined which method was used. Nevertheless, the pancreatic fistula rate has been previously shown to be identical regardless of stump closure method [15]. Fibrin sealant was very rarely applied to the pancreatic stump in either LDP or ODP. Surgical drain placement near the pancreatic stump in the left upper quadrant was also due to surgeon preference.
ACS-NSQIP
The ACS-NSQIP is a national validated, outcomes-based, risk-adjusted, peer-controlled program for the measurement and enhancement of the quality of surgical care. The sampling strategy, data abstraction procedures, variables collected, and overall structure have been well described [16–19]. One hundred and thirty-six preoperative (patient characteristics), intraoperative (processes of care), and postoperative (adverse outcomes) variables are prospectively collected by trained, certified nurse reviewers in the ACS-NSQIP. Patients younger than 18 years of age are excluded. Outcomes are assessed at 30 days after the index operation (e.g., DP). Definitions are highly standardized and validated. Quality is ensured by inter-rater reliability audits, as well as online decision support, so the level of disagreement is currently only 1.53% for all variables. Surgical clinical nurse reviewers ensure validity of the data by assessing physician documentation and/or contacting patients directly.
Clinical outcomes
Patient demographics such as age, gender, ethnicity, BMI, and ASA were recorded. Operative variables were recorded for approach (LDP vs. ODP), operative time, estimated blood loss, gland texture, duct size, and stump closure method. Surgical pathology was reviewed in all cases. Morbidity and mortality observed within 30 and 90 days of all cases were analyzed. Morbidity included organ space infections, wound disruption, cerebrovascular accident or stroke, myocardial infarction, cardiac arrest, cardiac arrhythmias, pulmonary embolism, ventilator dependence longer than 48 h, bleeding complications, sepsis/septic shock, superficial surgical site infections, pneumonia, unplanned intubations, acute renal failure or progressive renal insufficiency, urinary tract infection, deep vein thrombosis, portal vein thrombosis, pseudoaneurysm, pancreatic fistula, and reoperation.
Surgical complications were assessed and graded using the Clavien–Dindo classification system. In this classification system, grades I–V were assigned to the severity of postoperative complications. Grade I described any complication that deviated from the normal postoperative course, but did not require any intervention or aggressive pharmacologic therapy (aside from antiemetics, analgesics, diuretics, electrolytes, antipyretics, or physiotherapy). Grade II complications required treatment such as blood transfusion, total parenteral nutrition, or specific pharmacologic therapy. Grade III complications required surgical, endoscopic, or radiologic intervention. Grade IV complications were life-threatening. Grade V complications represented patient death [20, 21].
The overall complication pool was composed of approximately two-thirds serious morbidity and one-third minor complications. Any life-threatening event such as (but not limited to) cardiac arrest, hemorrhage, pulmonary embolism, sepsis, or pancreatic fistula were classified as serious morbidity. Events such as urinary tract infection, superficial skin infection, ileus, or transient acute kidney injury were classified as minor complications. If a patient experienced more than one complication, the actual number of complications was counted in the total.
Pancreatic fistula rates were monitored. International Study Group on Pancreatic Fistula (ISGPF) definitions were used for pancreatic fistula: drain output of any volume after postoperative day three with a drain fluid amylase level three times the serum amylase. We also used the ISGPF grading system to further classify the pancreatic fistulae as either Grade A, B, or C Fistulae [22].
Cancer-specific variables were also monitored. These specific variables included tumor size, margin status, lymph node harvest, number of positive lymph nodes, metastasis, TNM stages, adjuvant therapy, and survival.
Statistical analysis
All statistical analyses were performed using SAS 8.2 (Cary, NC). Mann–Whitney U test was used to compare means of continuous variables. Chi squared test was used for non-parametric data. P values of less than 0.05 were considered to represent statistical significance for all comparisons. The Institutional Review Board at Indiana University School of Medicine approved all aspects of this retrospective analysis.
Results
Of the 422 distal pancreatectomies performed over the study period, 79 patients underwent DP for a pathologic diagnosis of PDAC; 33 patients were in the LDP group and 46 in the ODP group. Demographic data can be found in Table 1. The median age of both groups was 66 years (66 ± 2 vs. 66 ± 2). Fifty-six percent of all patients were female (56 vs. 44%). The LDP group had a slightly lower BMI (26.2 vs. 27.8). The median American Society of Anesthesia (ASA) score was three in both groups.
Operative variables can be found in Tables 2 and 3. Operative times were similar in the LDP group (3.9 vs. 4.2 h), with a lower mean estimated blood loss (310 vs. 597 ml; P = 0.016) and subsequent fewer number of patients requiring transfusion (0 vs. 13; P = 0.0008). Drain placement was similar in both groups (74 vs. 89%) as the majority in both groups had a surgical drain placed near the pancreatic stump in the left upper quadrant. Gland texture and duct size were identical in both groups with predominantly soft glands and small duct size (<3 mm) at the site of parenchymal transection. No significant difference was seen in stump closure method (suture, stapler, reinforced stapler, and SLRF) between groups.
Postoperative outcomes are shown in Table 3. Median length of stay was shorter in the laparoscopic group (7.6 vs. 9 days). The 30-day mortality was higher in the LDP group (3 vs. 0%) due to one death secondary to a myocardial infarction. The 90-day mortality was lower in the LDP group (3 vs. 15%). The overall morbidity was lower in LDP but not statistically significant between the groups (52 vs. 70%); the LDP suffered a total of 21 complications in 17 patients (1.2 complications per patient) and ODP suffered a total of 63 complications in 32 patients (2.0 complications per patient).
In regards to the rate of pancreatic fistulae, between the two groups there was no notable variation in the pancreatic duct size, gland texture, and stump closure method. Pancreatic fistula rates (Table 4) were lower in the LDP group; however, this was not statistically significant (24 vs. 35%). The LDP group had three Grade B fistulae requiring additional intervention and five Grade A fistulae which did not require intervention. Grade C pancreatic fistulae were significantly higher in the ODP group (0 (0%) vs. 6 (13%); P = 0.03). As Grade C pancreatic fistulae were seen only in the ODP group, in turn the reoperation rate was higher in the ODP group but not statistically significant between the two groups (1 (3%) vs. 5 (11%); P = 0.19). Overall morbidity from this series is demonstrated in Table 3 via the Clavien–Dindo Grade classifications. As is demonstrated, morbidity was found to be equivalent between the two groups although there were a greater number of Grade II and IV complications in the ODP group.
Cancer-specific outcomes are demonstrated in Table 5. Surgical pathology variables were found to be comparable between LDP and ODP: tumor size (3.3 ± 0.3 vs. 4.0 ± 0.4 cm), tumor stage, and R0 surgical resection margin (77 vs. 87%). Differences were noted between the groups in the number of lymph nodes harvested and also in the number of positive lymph nodes. The ODP group had a higher yield, although not statistically significant, of lymph nodes harvested (17.5 ± 1.2 vs. 14.5 ± 1.1; P = 0.07). The ODP group also had a higher rate of lymph node metastasis which was found to be significant (1.6 ± 0.3 vs. 0.8 ± 0.2; P = 0.04). As demonstrated in Table 5, the overall differences in patient staging were not found to be statistically significant between the two groups.
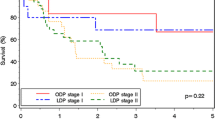
Examination of the postoperative outcomes, follow-up, and oncologic outcomes are demonstrated in Tables 3 and 5. Median follow-up for all patients was 11.4 months. Long-term oncologic outcomes revealed similar survival among both groups, but with a decreased rate of recurrence in the LDP group. The overall survival curve is demonstrated in Fig. 1. Otherwise, median survival (17.9 vs. 15.1 months) and 1-year (73 vs. 59%), 3-year (22 vs. 21%), and 5-year survival (20 vs. 15%) were similar.

Survival curve
Discussion
The laparoscopic approach to oncologic procedures is being used with greater frequency for many gastrointestinal malignancies, yet LDP for pancreatic adenocarcinoma has been slower to gain acceptance. The aim of this study was to compare short-term postoperative morbidity and oncologic outcomes as well as survival of patients with PDAC undergoing LDP and ODP.
Patients who underwent LDP had similar oncologic outcomes and survival as those who underwent ODP for the treatment of PDAC. Overall, there were no significant differences noted in the patient preoperative variables (age, comorbid conditions, or BMI), intraoperative variables (gland texture or pancreatic duct size), or surgical pathology (tumor size, RO status, or lymph node harvest) to suggest any confounding factors that would affect the postoperative outcomes and long-term survival. This study represents the largest single-institution series in North America focusing solely on DP for pancreatic adenocarcinoma; it demonstrated that LDP is not only safe, but also effective as an oncologic procedure in the surgical treatment of pancreatic adenocarcinoma.
At our institution, the open approach to pancreatic surgery was the gold standard until 2005 when the first LDP was performed for benign disease by a single surgeon. However, later that same year the first LDP was also performed for PDAC. Today, one decade later, there are six hepatopancreatobiliary surgeons who all perform LDP for PDAC in addition to ODP. This shift in paradigm has been witnessed elsewhere and adopted by many surgeons worldwide who have accepted LDP as a safe, appropriate, and responsible oncologic procedure in spite of the paucity of data in print to support its use.
Few studies exist that have specifically examined LDP versus ODP in the setting of PDAC. Several published series have reported meaningful data in small numbers [14, 23], while others have reported utilizing LDP for a conglomeration of indications including benign disease, premalignant lesions, and other tumors of the pancreas (neuroendocrine and secondary neoplasms) [3, 11–14, 24]. The first large study was reported by Kooby et al. in 2010 as a multi-institutional, retrospective series which compared outcomes of 23 LDP to 189 ODP and represented a very early laparoscopic experience with the treatment of PDAC. In the study, 212 patients from multiple institutions were included, 23 of which underwent LDP. No difference in intraoperative variables (operative time, blood loss), pathologic characteristics (margin status, lymph node harvest), or mortality was seen [25].
Sharpe et al. published a similar retrospective, yet larger and more modern series, in 2015 using the National Cancer Data Base [1]. These large multi-sourced studies which compiled data from different institutions were important to convey that laparoscopic and open procedures had equivalent mortality, surgical pathology, and survival. Yet they lacked examination of intraoperative variables (gland texture, pancreatic duct size) and postoperative outcomes (morbidity or pancreatic fistula). These concerns of postoperative complications are paramount to understanding the technical aspects that can potentially contribute to morbidity and possibly adversely affect patients who would otherwise be eligible to undergo adjuvant chemotherapy as an integral part of therapy and survival for the diagnosis of PDAC.
The topic of which patients are the best candidates for neoadjuvant and adjuvant chemotherapy is also one that is much studied and debated. Studies have shown that adjuvant therapy offers modest survival benefits, yet many patients do not receive postoperative therapy due to surgery-related morbidity and delayed recovery from surgery, disease progression, and comorbid illnesses [26]. Therefore, as surgeons we must make decisions as to which surgical approach will most benefit our patient and result in the greatest potential for R0 resection and ability to move forward to receive adjuvant therapy. More recently, Katz et al. discussed findings from the multi-institutional Alliance Trial A021101 in which it was demonstrated that there is a subset of patients who may benefit from neoadjuvant chemotherapy and radiation [27]. In our study, we did not focus on the effects of neoadjuvant therapy versus adjuvant therapy alone on survival as only the patients in the ODP underwent neoadjuvant therapy; this is a topic for further investigation and a separate study.
Other factors which must be discussed when examining our reported findings include preoperative oncologic severity (tumor size and vascular involvement) and previous operative history (contributing to excessive adhesions or incisional hernias) that could result in an appropriate selection bias that is neither reflective of disease nor procedure-specific risk—rather more of good clinical judgment. Even though data from this study, and others, demonstrate that LDP is associated with decreased operative time and blood loss, shorter hospital stays, decreased postoperative complications, and faster recovery, LDP likely is not suitable for all patients. Some patients may simply be better candidates for ODP due to their comorbidities and surgical history.
In terms of oncologic severity, no previous study has ever reported a difference in tumor size, R0 resection margin, or lymph node harvest when comparing LDP versus ODP. The ability to obtain an appropriate lymph node harvest via the LDP method was the most commonly cited concern in previous studies comparing LDP to ODP. In our study and others, the number of lymph nodes harvested was equivalent. Similarly, pathologic stage has not varied greatly in these series with the majority being greater than stage IIA, which are the cases that are generally more technically difficult for either laparoscopic or open approach.
Shin et al. published the only other larger single-institution series to date consisting of a propensity-matched study of LDP (n = 70) versus ODP (n = 80) for PDAC. This study reported that LDP had similar mortality, morbidity, and oncologic outcomes as ODP, in addition to a shorter length of stay [2]. This analysis was thorough and comprehensive and the reported findings are nearly identical to the findings reported in our series for postoperative and oncologic outcomes.
Our study does have several limitations. The primary limitation is the low total numbers in the series with 33 and 46 patients in each group. Although Table 6 demonstrates numerous previous reports to date, overall a paucity of patients have been reported having undergone LDP for PDAC. We realize that low numbers result in less reliable statistical comparisons and erroneous associations being made. An example of such a potential erroneous association is in the rate and type of pancreatic fistulae in our study—in the LDP group there were only Grade A and B fistulae, while the ODP group had a statistically significant number of Grade C fistulae in addition to several Grade A fistulae. This finding in reality may not be a function of the technical approach of the procedure but a function of a small sample size. Another important limitation is surgeon selection bias toward possibly resecting larger or locally advanced tumors via the open approach and smaller tumors laparoscopically especially in the earlier years of this study time period. As surgeon experience and comfort improves globally, a more robust comparison will likely occur and more directly identify the merits of either approach.
Conclusions
In summary, these results suggest that LDP appears to be a safe and effective surgical approach for the treatment of pancreatic adenocarcinoma in terms of postoperative morbidity and oncologic outcomes in the properly selected surgical patient. However, future studies are needed and should be in the form of prospective, randomized, multi-institutional clinical trials in order to eliminate surgeon or institutional biases with the stated aim to assess if LDP has improved outcomes and results in a higher rate of adjuvant chemotherapy. However, the overall poor prognosis of pancreatic cancer and the small number of cases may be prohibitive to performing such trials. The question of superiority may become paramount in the future if chemotherapy regimens become more efficacious or if screening methods are able to diagnose pancreatic adenocarcinoma earlier in its course. Despite the many gains made in the surgical treatment of pancreatic tumors in the last two decades, there remains much to be studied.
Abbreviations
- ACS-NSQIP:
-
American College of Surgeons National Surgical Quality Improvement Program
- DP:
-
Distal pancreatectomy
- PDAC:
-
Pancreatic adenocarcinoma
- PF:
-
Pancreatic fistula
References
Sharpe SM, Talamonti MS, Wang E, Bentrem DJ, Roggin KK, Prinz RA, Marsh RDW, Stocker SJ, Winchester DJ, Baker MS (2015) The laparoscopic approach to distal pancreatectomy for ductal adenocarcinoma results in shorter lengths of stay without compromising oncologic outcomes. Am J Surg 209:557–663
Shin SH, Kim SC, Song KB, Hwang DW, Lee JH, Lee D, Lee JW, Jun E, Park KM, Lee YJ (2015) A comparative study of laparoscopic vs open distal pancreatectomy for left-sided ductal adenocarcinoma: a propensity score-matched analysis. J Am Coll Surg 220:177–185
Baker MS, Bentrem DJ, Ujiki MB, Stocker SS, Talamonti MS (2009) A prospective single institution comparison of peri-operative outcomes for laparoscopic and open distal pancreatectomy. Surgery 146:635–643
Sui CJ, Li B, Yang JM, Wang SJ, Zhou YM (2012) Laparoscopic versus open distal pancreatectomy: a meta-analysis. Asian J Surg 35:1–8
Limongelli P, Belli A, Russo G, Cioffi L, D’Agostino A, Fantini C, Belli G (2012) Laparoscopic and open surgical treatment of left-sided pancreatic lesions: clinical outcomes and cost-effectiveness analysis. Surg Endosc 26:1830–1836
Piessen G, Lefevre JH, Cabau M, Duhamal A, Behal H, Perniceni T, Mabrut JY, Regimbeau JM, Bonvalot S, Tiberio GA, Mathonnet M, Regenet N, Guillaud A, Glehen O, Mariani P, Denost Q, Maggiori L, Benhaim L, Manceau G, Mutter D, Bail JP, Meunier B, Porcheron J, Mariette C, Brigand C, AFC and the FREGAT working group, (2015) Laparoscopic versus open surgery for gastric gastrointestinal stromal tumors: what is the impact on postoperative outcome and oncologic results? Ann Surg 262:831–839
Siani LM, Ferranti F, De Carlo A, Quintiliani A (2012) Completely laparoscopic versus open total gastrectomy in stage I-III/C gastric cancer: safety, efficacy and five-year oncologic outcome. Minerva Chir 67:319–326
Siani LM, Ferranti F, Benedetti M, De Carlo A, Quintiliani A (2011) Laparoscopic versus open radical nephrectomy in T1-T2 renal carcinoma: personal 5-year experience about the oncologic outcome. Minerva Chir 66:317–326
The Clinical Outcomes of Surgical Therapy Study Group (2004) A comparison of laparoscopically assisted and open colectomy for colon cancer. N Engl J Med 350:2050–2059
Kooby DA (2006) Laparoscopic surgery for cancer: historical, theoretical, and technical considerations. Oncology 20:317–326
Kim SC, Park KT, Hwang JW, Shin HC, Lee SS, Seo DW, Lee SK, Kim MH, Han DK (2008) Comparative analysis of clinical outcomes for laparoscopic distal pancreatic resection and open distal pancreatic resection at a single institution. Surg Endosc 22:2261–2268
Kooby DA, Gillespie T, Bentrem D, Nakeeb A, Schmidt MC, Merchant NB, Parikh AA, Martin RCG, Scoggins CR, Ahmad S, Kim JH, Park JR, McClaine R, Strasberg SM, Talamonti MS, Staley CA, McMasters KM, Lowy AM, Byrd-Sellers J, Wood WC, Hawkins WG (2008) Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Ann Surg 248:438–446
Rooij TD, Jilesen AP, Boerma D, Bonsing BA, Bosscha K, van Dam RM, van Dieren S, Dijkgraaf MG, van Eijck CH, Gerhards MF, van Goor H, van der Harst E, de Hingh IH, Kazemier G, Klaase JM, Molenaar IQ, van Dijkum EJN, Patijn GA, van Santvoort HC, Scheepers JJ, van der Schelling GP, Sieders E, Vogel JA, Busch OR, Besselink MG (2015) A nationwide comparison of laparoscopic and open distal pancreatectomy for benign and malignant disease. J Am Coll Surg 220:263–270
Zhang Y, Chen XM, Sun DL (2014) Laparoscopic versus open distal pancreatectomy: a single-institution comparative study. World J Surg Oncol 12:327
Ceppa EP, McCurdy RM, Becerra DC, Kilbane EM, Zyromski NJ, Nakeeb A, Schmidt CM, Lillemoe KD, Pitt HA, House MG (2015) Does pancreatic stump closure method influence distal pancreatectomy outcomes? J Gastrointest Surg 19:1449–1456
Khuri SF (2005) The NSQIP: a new frontier in surgery. Surgery 138:837–843
Fink AS, Campbell DA, Mentzer RM, Henderson WG, Daley J, Bannister J, Hur K, Khuri SF (2002) The national surgical quality improvement program in non-veterans administration hospitals: initial demonstration of feasibility. Ann Surg 236:344–353
Khuri SF, Henderson WG, Daley J, Jonasson O, Jones RS, Campbell DA, Fink AS, Mentzer RM, Steeger JE (2007) The patient safety in surgery study: background, study design, and patient populations. J Am Coll Surg 204:1089–1102
Daley J, Khuri SF, Henderson W, Hur K, Gibbs JO, Barbour G, Demakis J, Irvin G 3rd, Stremple JF, Grover F, McDonald G, Passaro E Jr, Fabri PJ, Spencer J, Hammermeister K, Aust JB, Oprian C (1997) Risk adjustment of the postoperative morbidity rate for the comparative assessment of the quality of surgical care: result of the national veterans affairs surgical risk study. J Am Coll Surg 185:328–340
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Casadei R, Ricci C, Pezzilli R, Calculli L, D’Ambra M, Taffurelli G, Minni F (2011) Assessment of complications according to the Clavien-Dindo classification after distal pancreatectomy. J Pancreas 12:126–130
Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, Sarr M, Traverso W, Buchler M (2005) Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 138:8–13
Khaled YS, Malde DJ, Packer J, De Liguori Carino N, Deshpande R, O’Reilly DA, Sherlock DJ, Ammori BJ (2014) A case-matched comparative study of laparoscopic versus open distal pancreatectomy. Surg Laparosc Endosc 25:363–367
Vijan SS, Ahmed KA, Harmsen WS, Que FG, Reid-Lombardo KM, Nagorney DM, Donohue JH, Farnell MB, Kendrick ML (2010) Laparoscopic vs open distal pancreatectomy a single-institution comparative study. Arch Surg 45:616–621
Kooby DA, Hawkins WG, Schmidt CM, Weber SM, Bentrem DJ, Gillespie TW, Sellers JB, Merchant NB, Scoggins CR, Martin RCG, Kim HJ, Ahmed S, Cho CS, Parikh AA, Chu CK, Hamilton NA, Doyle CJ, Pinchot S, Hayman A, McClaine R, Nakeeb A, Staley CA, McMasters KM, Lillemoe KD (2010) A multicenter analysis of distal pancreatectomy for adenocarcinoma: is laparoscopic resection appropriate? J Am Coll Surg 210:779–787
Kagedan DJ, Raju RS, Dixon ME, Shin E, Li Q, Liu N, Elmi M, El-Sedfy A, Paszat L, Kiss A, Earle CC, Mittmann N, Coburn NG (2016) The association of adjuvant therapy with survival at the population level following pancreatic adenocarcinoma resection. HPB 18:339–347
Katz MHG, Shi Q, Ahmad SA, Herman JM, de Wilton Marsh R, Collisson EA, Schwartz LH, Martin RCG, Conway WC, Truty M, Kindler HL, Lowy AM, Philip PA, Sekaii-Saab TS, Cardin BD, LoConte NK, Venook AP (2015) Preoperative modified FOLFIRINOX (mFOLFIRINOX) followed by chemoradiation (CRT) for borderline resectable (BLR) pancreatic cancer (PDAC): initial results from Alliance Trial A021101. J Clin Oncol 33:4008
Fernandez-Cruz L, Cosa R, Blanco L, Levi S, Lopez-Boado MA, Navarro S (2007) Curative laparoscopic resection for pancreatic neoplasms: a critical analysis from a single institution. J Gastrointest Surg 11:1607–1621
Kang CM, Choi SH, Hwang HK, Kim DH, Yoon CI, Lee WJ (2010) Laparoscopic distal pancreatectomy with division of the pancreatic neck for benign and borderline malignant tumor in the proximal body of the pancreas. J Laparoendosc Adv Surg Tech A 20:581–586
Song KB, Kim SC, Park JB, Kim YH, Jung YS, Kim MH, Lee SK, Seo DW, Lee SS, Park DH (2011) Single-center experience of laparoscopic left pancreatic resection in 359 consecutive patients: changing the surgical paradigm of left pancreatic resection. Surg Endosc 25:3364–3372
Mehta SS, Doumane G, Mura T, Nocca D, Fabre JM (2012) Laparoscopic versus open distal pancreatectomy: a single-institution case-control study. Surg Endosc 26:402–707
Rehman S, John SKP, Lochan R, Jaques BC, Manas DM, Charnley RM, French JJ, White SA (2014) Oncological feasibility of laparoscopic distal pancreatectomy for adenocarcinoma: a single-institution comparative study. World J Surg 38:476–483
Magge D, Gooding W, Choudry H, Steve J, Steel J, Zureikat A, Krasinskas A, Daouadi M, Lee KK, Hughes SJ, Zeh HJ 3rd, Moser AJ (2013) Comparative effectiveness of minimally invasive open distal pancreatectomy for ductal adenocarcinoma. JAMA Surg 148:525–531
Acknowledgements
There are no financial disclosures.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Drs. Marita D. Bauman, David G. Becerra, E. Molly Kilbane, RN BSN, Nicholas J. Zyromski, C. Max Schmidt, Henry A. Pitt, Attila Nakeeb, Michael G. House, and Eugene P. Ceppa have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Bauman, M.D., Becerra, D.G., Kilbane, E.M. et al. Laparoscopic distal pancreatectomy for pancreatic cancer is safe and effective. Surg Endosc 32, 53–61 (2018). https://doi.org/10.1007/s00464-017-5633-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-017-5633-7