
Abstract
Background
Esophageal achalasia can be classified on the grounds of three distinct manometric patterns that correlate well with final outcome after laparoscopic Heller-Dor myotomy (LHM). No analytical data are available, however, on the postoperative picture and its possible correlation with final outcome. The aims of this study were: (a) to investigate whether manometric patterns change after LHM for achalasia; (b) to ascertain whether postoperative patterns and/or changes can predict final outcome; and (c) to test the hypothesis that the three known patterns represent different stages in the evolution of the disease.
Methods
During the study period, we prospectively enlisted 206 consecutive achalasia patients who were assessed using high-resolution manometry (HRM) before undergoing LHM. Symptoms were scored using a detailed questionnaire. Barium swallow, endoscopy and HRM were performed, before and again 6 months after surgery.
Results
Preoperative HRM revealed the three known patterns with statistically different esophageal diameters (pattern I having the largest), and patients with pattern I had the highest symptom scores. The surgical treatment failed in 10 cases (4.9%). The only predictor of final outcome was the preoperative manometric pattern (p = 0.01). All patients with pattern I preoperatively had the same pattern afterward, whereas nearly 50% of patients with pattern III before LHM had patterns I or II after surgery. There were no cases showing the opposite trend.
Conclusions
Neither a change of manometric pattern after surgery nor a patient’s postoperative pattern was a predictor of final outcome, whereas preoperative pattern confirmed its prognostic significance. The three manometric patterns distinguishable in achalasia may represent different stages in the disease’s evolution, pattern III and pattern I coinciding with the early and final stages of the disease, respectively.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
Achalasia is a primary esophageal motility disorder of unclear etiology. It is characterized by the absence of esophageal peristalsis and a defective relaxation of the lower esophageal sphincter (LES), resulting in an impaired bolus transit through the gastroesophageal junction [1, 2]. Achalasia has an incidence of 1.6 cases per 100,000 population a year [3]. Current treatments include surgical or endoscopic myotomy, pneumatic dilation and botulinum toxin injection for the purpose of relieving dysphagia by weakening the functional outflow obstruction, but they are only palliative measures [4, 5]. Laparoscopic Heller’s myotomy with a partial fundoplication is the treatment of choice at present because it achieves a symptom relief that persists after 5 years in 85 to 95% of patients [6,7,8,9,10,11].
In recent years, a classification based on the results of high-resolution manometry (HRM) has changed the diagnostic approach to esophageal achalasia. The disease reveals three distinct patterns: pattern I, achalasia with minimal esophageal pressurization; pattern II, achalasia with esophageal compression; and pattern III, achalasia with spasm [1, 12]. Our group and other recent studies have demonstrated that a patient’s preoperative manometric pattern predicts the outcome of laparoscopic Heller–Dor myotomy (LHM) and pneumatic dilation [12, 13]. No analytical data are available on patients’ postoperative manometric patterns, however, or on their possible correlation with patients’ final outcomes. When preoperative assessments and final outcomes are compared in patients treated for esophageal achalasia, the role and etiology of pattern III are still unclear [1, 12]. It is also still not known whether the three manometric patterns identified in achalasia patients represent three different diseases, or different manifestations (or stages) of the same disease, with the possibility of transitions from one to another.
The aims of the present study were: a) to investigate whether achalasia patients’ manometric patterns change after LHM; b) to examine whether the postoperative manometric pattern, or a change in manometric pattern after surgery, can predict a patient’s final outcome; and c) to test the hypothesis that the three manometric patterns seen in achalasia represent different phenotypes or different stages in the evolution of the same disease.
Materials and methods
The study population consisted of achalasia patients consecutively treated with LHM from January 2011 to December 2015 who underwent HRM both pre- and postoperatively. Their diagnosis of primary achalasia was established on the basis of accepted esophageal motility characteristics (i.e., no peristalsis in the esophageal body and impaired LES relaxation on swallowing) [1, 4]. Patients who had already been treated for achalasia with endoscopic or surgical myotomy, pneumatic dilations or botulinum toxin injections were ruled out.
Patients’ demographic and clinical data, preoperative assessment, surgical details and postoperative follow-up were prospectively recorded in a dedicated database.
Since this was an observational study and all the procedures were routinely performed for the diagnosis and the follow-up of patients with esophageal achalasia, IRB approval was not required. The study was approved by the Research Committee of the Department of Surgical, Oncological, and Gastroenterological Sciences—University of Padova.
Preoperative assessment
Demographic and clinical data were collected on each patient using a dedicated questionnaire. The scores for dysphagia, regurgitation and chest pain were calculated by combining the severity of each symptom (0 = none, 2 = mild, 4 = moderate, 6 = severe) with its frequency (0 = never, 1 = occasionally, 2 = once a month, 3 = every week, 4 = twice a week, 5 = daily). The symptom score was the sum of the dysphagia and regurgitation scores, while the chest pain score was considered separately [14].
All patients had the following preoperative tests: (Table 1)
-
barium swallow X-rays to assess esophageal diameter and shape;
-
endoscopy to rule out esophageal or cardia malignancies;
-
esophageal manometry using the high-resolution technique; and
-
in selected cases, CT scan to exclude malignant disease.
High-resolution manometry (HRM)
Before and after surgery, HRM was performed using a catheter with 36 solid-state circumferential sensors spaced at 1-cm intervals and spanning the whole esophagus (Medtronic, Minneapolis, MN, USA). The catheter was inserted transnasally, and the study was conducted with the patient in a supine position. The study protocol required 10 swallows of 5 ml of saline water solution, using a standardized electrolyte concentration to ensure proper catheter function, separated by at least 20-second intervals [15, 16].
The manometric data were analyzed with the ManoView™ software (Medtronic, USA) [17]. The IRP was ascertained by adjusting the pressure on the isobaric contour tool to the lowest value at which a cumulative period of 4 s was excluded on the axial plane of the EGJ within the relaxation window. This procedure was applied for each swallow [18].
The pre- and postoperative manometric patterns were classified according to the Chicago criteria: pattern I = 100% failed contractions and no esophageal pressurization (Fig. 1); pattern II = panesophageal pressurization occurring with at least 20% of the swallows (Fig. 2); and pattern III = traces of preserved distal peristalsis or premature contractions for at least 20% of the swallows (Fig. 3) [19].

Achalasia pattern I. High-resolution manometric picture showing no distal esophageal pressurization. Impaired LES relaxation is also evident as a continuous high-pressure band across the lower portion of the image

Achalasia pattern II. High-resolution manometric picture of panesophageal pressurization, showing simultaneous isobaric esophageal pressurization ≥30 mmHg

Achalasia pattern III. High-resolution manometric picture of rapidly propagating pressurization with spastic contractions. The high-amplitude contractions of the distal esophageal body are evident from the red high-pressure area of the esophageal body contraction
Laparoscopic Heller–Dor myotomy technique
The surgical technique has been described in detail elsewhere [20]. Briefly, only the anterior part of the esophagus was dissected and a myotomy 6–8 cm long was performed, extending it 1.5–2 cm on the gastric side. During the myotomy, a 30-mm Rigiflex balloon was placed inside the esophageal lumen at cardia level using an endoscopically positioned guide wire; the balloon was gently inflated and deflated with 40–60 cc of air using a syringe. This maneuver afforded a better exposure of the circular muscle fibers. The procedure was completed with a Dor anterior partial fundoplication [6].
Follow-up
Clinical outcome was assessed 1, 6 and 12 months after LHM and every 2 years thereafter, by means of the same questionnaire as was administered preoperatively. Treatment failure was defined as a postoperative symptom score higher than the 10th percentile of the preoperative score for the group of patients as a whole (i.e., >8) [6, 21]. Barium swallow X-rays were obtained 1 month after the myotomy and in the event of recurrent dysphagia. Endoscopy was repeated 12 months after surgery and then every 2 years thereafter, to identify and control any complications (i.e., esophagitis) and rule out any neoplastic degeneration. HRM was performed 6 months after LHM, together with 24-hour pH monitoring to assess any abnormal acid exposure of the distal esophagus. Tracings from patients with abnormal reflux on computer analysis were carefully reviewed to distinguish true gastroesophageal reflux episodes from false reflux due to stasis [22].
Statistical analysis
Continuous data were expressed as median and interquartile range, categorical data as number and percentage. Continuous data and categorical data were compared between the three pattern groups using Kruskal–Wallis test and Fisher test, respectively. Preoperative to postoperative variations of symptom scores, LES basal pressure and IRP were evaluated using Wilcoxon test. The association between failure and patients’ preoperative demographic and clinical findings was assessed using Mann–Whitney test and Fisher test. A p value less than 0.05 was considered significant. Statistical analysis was performed using SAS 9.1 software (SAS Institute Inc., Cary, NC, USA).
Results
Preoperative assessment
The study population consisted of 206 consecutive achalasia patients (111 men, 95 women; median age 48 years, IQR 37–58). Based on their HRM findings, 88 patients (42.7%) were classified as having pattern I, 100 (48.6%) had pattern II, and 18 (8.7%) had pattern III. The study population’s demographic and clinical data are summarized in Table 1. Patients with pattern I achalasia had a higher mean symptom score than the other two groups.
The three patterns were associated with a statistically different median esophageal diameter, which was: 45 mm (IQR 38–60) for pattern I; 35 mm (IQR 30–40) for pattern II; and 25 mm (IQR 25–30) for pattern III (p < 0.001). All patients with a sigmoid-shaped mega-esophagus (radiological grade IV) had pattern 1 achalasia preoperatively. Patients with pattern III tended to have a shorter history of symptoms before their achalasia was diagnosed, though this difference fell short of statistical significance (p = 0.06); they also had a longer overall LES length than the other two groups (p = 0.04).
Surgical outcome
The surgical procedure was completed laparoscopically in all cases. One patient died on postoperative day 1 due to an acute myocardial infarction. The esophageal mucosa was perforated during the procedure of two patients and repaired intraoperatively in both cases. One other mucosal leak was identified on water-soluble contrast swallows on the first postoperative day. None of these complications were associated with persistent or recurrent symptoms after surgery. The patients involved had pattern I in two cases and pattern II in one.
After LHM, there was a significant decrease in patients’ symptom scores (median 16 [IQR 9–20] preoperatively vs median 0 [IQR 0–3] postoperatively; p < 0.001), LES basal pressure (median 41 [IQR 31–52.2] preoperatively versus median 16 [IQR 11–22] postoperatively; p < 0.001) and IRP (median 29.1 [IQR 20.8–38.1] preoperatively versus median 7.7 [IQR: 5.2–11] postoperatively; p < 0.001).
After a median follow-up of 15 months (IQR 12–24), the outcome after LHM was still favorable in 195 patients (95.1%), while 10 patients had a recurrence of their achalasia symptoms. Patients with pattern III achalasia had the highest incidence of failures (22.2%, 4/18) (p < 0.01), while the failure rate was similar for patterns I and II (3 and 3.4%, respectively).
All patients whose surgical treatment failed had one or more complementary endoscopic pneumatic dilations using Rigiflex balloons (30 or 35 mm), after which none of them reported persistent dysphagia.
During the follow-up, 117 patients agreed to undergo 24-hour pH monitoring and 11 of them (9.4%) revealed a pathological distal esophageal acid exposure. Two of these patients had pattern I achalasia, seven had pattern II, and two had pattern III.
On univariate analysis, only the preoperative achalasia pattern correlated with the final outcome, while postoperative pattern and changes from one pattern to another did not (Table 2).
Postoperative pattern
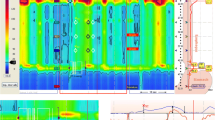
HRM after surgery was available for 133 patients: 91 had pattern I postoperatively, 32 had pattern II, and eight had pattern III. Two patients showed signs of a partial recovery of peristalsis (before surgery, they had both had pattern II achalasia; Fig. 4).

Recovery of peristalsis. Pre- and postoperative HRM of a patient whose peristalsis recovered after surgery
All the patients with pattern I preoperatively had the same pattern I after LHM, whereas the pattern changed in 28/63 (44.4%) patients with pattern II and 8/16 (50%) with pattern III: All of the 28 patients with a preoperative pattern II changed to pattern I after surgery; of the eight patients with a preoperative pattern III, four changed to pattern I and four to pattern II.
The pre- to postoperative changes in achalasia pattern are shown in Table 3.
Discussion
The main aim of this study was to ascertain the effect of surgical myotomy on the manometric pattern in achalasia patients. LHM significantly improves LES outflow, reducing the LES basal pressure and IRP (Fig. 4) . Our surgical failure rate was less than 5%, but this low figure may naturally be due partly to the short follow-up in this study.
None of the patients with preoperative patterns I or II developed a pattern III achalasia after surgery, while half of the patients with pattern III preoperatively changed to patterns I or II (Tables 2, 3).
This study confirms the findings of a previous publication of ours (using conventional manometry), i.e., that the outcome of LHM correlates with the preoperative manometric pattern: Pattern III has a negative prognostic impact. Judging from the data obtained in the present study, we can also say that a patient’s postoperative manometric pattern or a change of pattern after myotomy is not a predictor of treatment outcome.
Apart from the preoperative manometric pattern, the reasons for treatment failure in some patients are hard to identify in the medical literature. Offering various explanations, several articles have suggested that radiological stage IV, high chest pain scores, low LES resting pressures and previous endoscopic treatments (according to some authors, at least) are negative prognostic factors in patients undergoing surgery for achalasia [6, 23,24,25,26,27]. The most important cause of surgical failure, however, is probably a faulty surgical technique, especially if symptoms persist or recur soon after the procedure [8]. The risk of some of the muscle fibers being left uncut or of an excessively short myotomy on the gastric side of the LES (where the submucosal plane is more difficult to manage) should certainly be borne in mind.
The radiological and manometric results emerging from the present study, and the clinical characteristics of the patients involved, prompt us to advance the hypothesis that achalasia could be staged by pattern, where pattern III coincides with an earlier stage of the disease and pattern I with more advanced achalasia. Should further studies support this hypothesis, we might call it the “Padova theory.” In our sample, none of the patients with pattern I or II preoperatively developed a postoperative pattern III, whereas the opposite was true of one in two patients initially presenting with pattern III. In addition, all our pattern III patients had a clinical history typical of achalasia and a barium swallow showing grade I–II disease. By cutting the LES muscle fibers, the myotomy naturally reduced the outflow obstruction.
It may be that the gullet develops a spastic-like motor activity in an unsuccessful effort to overcome the LES barrier, which is reduced or destroyed by myotomy. Once such a spastic-like activity is no longer needed, the esophageal body may reveal the behavior typical of achalasia, i.e., aperistalsis, with or without esophageal pressurization. This is pure speculation, of course, since we have no experience of patients with a manometric diagnosis of achalasia being followed up without any form of therapy. In our knowledge, this was never reported in the literature. The possibility of a manometric diagnosis changing from diffuse esophageal spasm to achalasia was reported by Kramer [28] nearly 50 years ago and confirmed by Vantrappen [29]. In those days, achalasia was considered a single entity (the only variant being “vigorous achalasia”), and this modification/evolution may be true also for the different forms of achalasia.
That pattern I is the most advanced of the three patterns of achalasia is confirmed by the radiological findings in our study. The esophageal diameter became gradually larger from pattern III to patterns II and I, and all patients with a sigmoid-shaped mega-esophagus (radiological grade IV) had pattern I preoperatively.
The main weakness in our theory lies in that our patients had surgical treatment, which modifies the outflow obstruction, and would therefore influence any change in their postoperative achalasia pattern, though it is worth emphasizing that all of our patients had exactly the same standardized treatment (LHM).
Postoperative manometry 6 months after LHM revealed a partial recovery of peristalsis in two of our patients. This issue has always been controversial, however. Some older studies suggested that peristalsis may return after the treatment in some cases [30,31,32,33]. Parrilla and colleagues described some degree of peristalsis in the distal esophagus of 9% of patients and in the mid-esophagus of as many as 24% of patients after surgery, especially among cases with a more acute onset of dysphagia, a less dilated esophagus preoperatively and a greater contractility of the esophageal body [30]. In a recent study, Roman and co-authors also described some degree of peristaltic contraction after myotomy that had not been manometrically evident beforehand. The frequency of observation of this condition may reflect particular pathogenetic features (especially in patients with pattern III achalasia) or the extent to which the neurodegenerative process has progressed [33]. We believe that such findings need to be tested by means of further postoperative manometric investigations because such a partial recovery of peristalsis might be only temporary.
In conclusion, this was the first study to examine postoperative achalasia patterns, how they may change after LHM and their correlation with final outcome. Neither postoperative pattern nor changes of pattern emerged as predictors of final outcome in our sample of patients. The different manometric patterns of achalasia could represent different stages of evolution of the disease—where pattern III would be the earlier stage, pattern II an intermediate stage and pattern I the end stage—rather than different phenotypes of the same disease or manifestations of different diseases.
References
Pandolfino JE, Kwiatek MA, Nealis T, Bulsiewicz W, Post J, Kahrilas PJ (2008) Achalasia: a new clinically relevant classification by high-resolution manometry. Gastroenterology 135(5):1526–1533
Williams VA, Peters JH (2009) Achalasia of the esophagus: a surgical disease. J Am Coll Surg 208(1):151–162
Gennaro N, Portale G, Gallo C, Riocchietto S, Caruso V et al (2011) Esophageal achalasia in the Veneto region: epidemiology and treatment. Epidemiology and treatment of achalasia. J Gastrointest Surg 15:423–428
Richter JE (2001) Oesophageal motility disorders. Lancet 358(9284):823–828
Boeckxstaens GE (2007) Achalasia. Best Pract Res Clin Gastroenterol 21(4):595–608
Zaninotto G, Costantini M, Rizzetto C, Zanatta L, Guirroli E, Portale G, Nicoletti L, Cavallin F, Battaglia G, Ruol A, Ancona E (2008) Four hundred laparoscopic myotomies for esophageal achalasia: a single centre experience. Ann Surg 248(6):986–993
Patti MG, Pellegrini CA, Horgan S, Arcerito M, Omelanczuk P, Tamburini A, Diener U, Eubanks TR, Way LW (1999) Minimally invasive surgery for achalasia: an 8-year experience with 168 patients. Ann Surg 230(4):587–593
Oelschlager BK, Chang L, Pellegrini CA (2003) Improved outcome after extended gastric myotomy for achalasia. Arch Surg 138(5):490–495
Khajanchee YS, Kanneganti S, Leatherwood AE, Hansen PD, Swanström LL (2005) Laparoscopic Heller myotomy with Toupet fundoplication: outcome predictors in 121 consecutive patients. Arch Surg 140(9):827–833
Liu JF, Zhang J, Tian ZQ, Wang QZ, Li BQ, Wang FS, Cao FM, Zhang YF, Li Y, Fan Z, Han JJ, Liu H (2004) Long-term outcome of esophageal myotomy for achalasia. World J Gastroenterol 10(2):287–291
Kilic A, Schuchert MJ, Pennathur A, Gilbert S, Landreneau RJ, Luketich JD (2009) Long-term outcomes of laparoscopic Heller myotomy for achalasia. Surgery 146(4):826–831
Salvador R, Costantini M, Zaninotto G, Morbin T, Rizzetto C, Zanatta L, Ceolin M, Finotti E, Guirroli E, Nicoletti L, Da Dalt GF, Cavallin F, Ancona E (2010) The preoperative manometric pattern predicts the outcome of surgical treatment for esophageal achalasia. J Gastrointest Surg 211(6):754–761
Rohof WO, Salvador R, Annese V, Bruley des Varannes S, Chaussade S, Costantini M, Elizalde JI, Gaudric M, Smout AJ, Tack J, Busch OR, Zaninotto G, Boeckxstaens GE (2013) Treatment outcome of achalasia depends on the manometric subtype. Gastroenterology 144(4):718–725
Salvador R, Costantini M, Cavallin F, Zanatta L, Finotti E, Pozza G, Longo C, Nicoletti L, Capovilla G, Bardini R, Ancona E, Zaninotto G (2014) Laparoscopic Heller myotomy can be used as primary therapy for esophageal achalasia regardless of age. Journal Gastrointest Surg 18(1):106–112
Pandolfino JE, Ghosh SK, Zhang Q, Jarosz A, Shah N, Kahrilas PJ (2006) Quantifying EGJ morphology and relaxation with high-resolution manometry: a study of 75 asymptomatic volunteers. Am J Physiol Gastrointest Liver Physiol 290(5):G1033–G1040
Tolone S, de Cassan C, de Bortoli N, Roman S, Galeazzi F, Salvador R, Marabotto E, Furnari M, Zentilin P, Marchi S, Bardini R, Sturniolo GC, Savarino V, Savarino E (2015) Esophagogastric junction morphology is associated with a positive impedance-pH monitoring in patients with GERD. Neurogastroenterol Motil 27(8):1175–1182
Salvador R, Dubecz A, Polomsky M, Gellerson O, Jones CE, Raymond DP, Watson TJ, Peters JH (2009) A new era in esophageal diagnostics: the image-based paradigm of high-resolution manometry. J Am Coll Surg 208(6):1035–1044
Salvador R, Savarino E, Pesenti E, Spadotto L, Capovilla G, Cavallin F, Galeazzi F, Nicoletti L, Merigliano S, Costantini M (2016) The impact of Heller myotomy on integrated relaxation pressure in esophageal achalasia. J Gastrointest Surg 20(1):125–131
Kahrilas PJ, Bredenoord AJ, Fox M, Gyawali CP, Roman S, Smout AJ, Pandolfino JE, International High-Resolution Manometry Working Group (2015) The Chicago classification of esophageal motility disorders, v3.0. Neurogastroenterol Motil 27(2):160–174
Ancona E, Peracchia A, Zaninotto G, Rossi M, Bonavina L, Segalin A (1993) Heller laparoscopic cardiomyotomy with antireflux anterior fundoplication (Dor) in the treatment of esophageal achalasia. Surg Endosc 7(5):459–461
Salvador R, Caruso V, Costantini M, Parise P, Nicoletti L, Cavallin F, Zanatta L, Bardini R, Ancona E, Zaninotto G (2015) Extending myotomy on the gastric side does not influence the final outcome of laparoscopic Heller-Dor for esophageal achalasia. Dis Esophagus 28(5):412–417
Crookes PF, Corkill S, DeMeester TR (1997) Gastroesophageal reflux in achalasia. When is reflux really reflux? Dig Dis Sci 42(7):1354–1361
Patti MG, Feo CV, Diener U, Tamburini A, Arcerito M, Safadi B, Way LW (1999) Laparoscopic Heller myotomy relieves dysphagia in achalasia when the esophagus is dilated. Surg Endosc 13(9):843–847
Omura N, Kashiwagi H, Ishibashi Y, Yano F, Tsuboi K, Kawasaki N, Suzuki Y, Yanaga K (2006) Laparoscopic Heller myotomy and Dor fundoplication for the treatment of achalasia. Assessment in relation to morphologic type. Surg Endosc 20(2):210–213
Portale G, Costantini M, Rizzetto C, Guirroli E, Ceolin M, Salvador R, Ancona E, Zaninotto G (2005) Long-term outcome of laparoscopic Heller-Dor surgery for esophageal achalasia: possible detrimental role of previous endoscopic treatment. J Gastrointest Surg 9(9):1332–1339
Arain MA, Peters JH, Tamhankar AP, Portale G, Almogy G, DeMeester SR, Crookes PF, Hagen JA, Bremner CG, DeMeester TR (2004) Preoperative lower esophageal sphincter pressure affects outcome of laparoscopic esophageal myotomy for achalasia. J Gastrointest Surg 8(3):328–334
Torquati A, Richards WO, Holzman MD, Sharp KW (2006) Laparoscopic myotomy for achalasia: predictors of successful outcome after 200 cases. Ann Surg 243(5):587–591
Kramer P, Harris L, Donaldson R (1967) Transition from symptomatic diffuse spasm to cardiospasm. Gut 8(2):115–119
Vantrappen G, Janssens J, Hellemans J, Coremans G (1979) Achalasia, diffuse esophageal spasm, and related motility disorders. Gastroenterology 76:450–457
Parrilla P, Martinez de Haro LF, Ortiz A, Morales G, Garay V, Aguilar J (1995) Factors involved in the return of peristalsis in patients with achalasia of the cardia after Heller’s myotomy. Am J Gastroenterol 90(5):713–717
Patti MG, Galvani C, Gorodner MV, Tedesco P (2005) Timing of surgical intervention does not influence return of esophageal peristalsis or outcome for patients with achalasia. Surg Endosc 19(9):1188–1192
Zaninotto G, Costantini M, Anselmino M, Boccù C, Ancona E (1995) Onset of oesophageal peristalsis after surgery for idiopathic achalasia. Br J Surg 82(11):1532–1534
Roman S, Kahrilas PJ, Mion F, Nealis TB, Soper NJ, Poncet G, Nicodème F, Hungness E, Pandolfino JE (2013) Partial recovery of peristalsis after myotomy for achalasia: more the rule than the exception. JAMA Surg 148(2):157–164
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Renato Salvador, Edoardo Savarino, Elisa Pesenti, Lorenzo Spadotto, Guerrino Voltarel, Giovanni Capovilla, Francesco Cavallin, Loredana Nicoletti, Michele Valmasoni, Alberto Ruol, Stefano Merigliano and Mario Costantini have no conflicts of interest or financial ties to disclose.
Rights and permissions
About this article

Cite this article
Salvador, R., Savarino, E., Pesenti, E. et al. Effects of laparoscopic myotomy on the esophageal motility pattern of esophageal achalasia as measured by high-resolution manometry. Surg Endosc 31, 3510–3518 (2017). https://doi.org/10.1007/s00464-016-5377-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-5377-9