
Abstract
Background
In this study, the proposed technique is combining the invented method of extraperitoneal dissection utilizing gas insufflation through Veress needle introduced from the groin with the transabdominal approach. Such a combination minimizes operative demands, achieves major goals, and reduce operative time in an attempt to improve laparoscopic hernioplasty techniques.
Methods
The study recruited 211 patients having primary reducible inguinal hernia upon first diagnosis. Abdominal ultrasound examination achieved to exclude any additional pathology and confirming clinical diagnosis. The new technique is applied on all patients without any modification through the whole series.
Results
Patients’ epidemiology, operative characteristics, and follow-up are all tabulated. Results showed no complications nor conversion to open procedure.
Conclusions
The proposed procedure showed preliminary encouraging results regarding technique, clinical outcome, time-saving, and patients’ safety. Combination of extraperitoneal gas-derived dissection, transabdominal field review, and preperitoneal mesh application offers an innovative and promising laparoscopic hernioplasty technique. The study is introducing the technique and as well invites further trials on wider scale to verify the technique.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction and review of surgical technique concept
Laparoscopic hernioplasty is still not the standard for repair. Recent worldwide figures still favor open methods, and universally, only 15–20 % of hernias are being done laparoscopically. Laparoscopic hernioplasty has reduced the recurrence rates to <0.5 % in most series [1].
The main issues within any inguinal hernioplasty technique are dissecting hernia sac from the contents of the spermatic cord and positioning a mesh over the myopectineal orifice. It is well documented that laparoscopy is more sensitive than clinical examination in documenting hernia in patients with groin pain [2, 3].
The laparoscopic technique applied in hernia repair depends on the anatomic approach to the preperitoneal space. The two main approaches for laparoscopic repair of groin hernias are the totally extraperitoneal (TEP) and the transabdominal preperitoneal (TAPP) ones. TEP has been developed to address and potentially avoid complications of entering the peritoneal cavity. The major advantage of the posterior approach to groin hernias is that all three hernia defects, direct, indirect, and femoral, are well visualized and in close proximity to each other, allowing easy repair of any of them. The drawback of TAPP procedure is that it requires entry into the peritoneal cavity and peritoneal closure. On the other hand, TAPP is superior in discovering subclinical contralateral hernias and better control on dissection field and hernia sac [1, 2]. Combination of both TEP and TAPP and modifications in either technique has been tried but did not gain popularity due to complexity of techniques with no advantages [4, 5].
Hernia sac dissection has to be atraumatic to tissues resulting in a bloodless field and preserving the spermatic and inguinofemoral structures intact. In addition, preservation of testicular vascularity is another issue of importance [6]. Hernia recurrence is attributed mostly to overlooking spermatic adhesion or extraperitoneal fat attached to the internal ring [7]. This step has no definite technique but depends on the operative field situation and surgeon’s own experience. Another point of debate is excision or preservation of hernia sac. Excision of sac has less recurrence rate due to disconnection with any leading point to herniation namely extraperitoneal adhesions or fat [8].
In this study, adoption of a new technique offers automated, easy, safe, and fast hernia dissection in such a way; preperitoneal pocketing is made prior to peritoneal incision, and application of the mesh is facilitated and fastened. Another modification suggested in the hernioplasty technique is not to excise the hernia sac nor leaving untouched but transfixing the sac neck and suturing the sac itself within the peritoneal closure line. This method of hernia sac management is of great value in two ways: the first is to ensure the sac has no extraperitoneal leading point avoiding potential recurrence of hernia and the second is to overlap and cover any possible peritoneal tears or defects upon closing the peritoneal window. In this way, we confirm complete exclusion of the whole sac away from the myopectineum and insure complete closure of peritoneal sheet.
So in summary this study is proposing a new technique applying genuine concept, combining preperitoneal gas dissection and transabdominal preperitoneal approach with transfixing hernia sac to peritoneal closure line. The new technique is named “dual approach hernioplasty” (DAH).
Materials and methods
This is a case series pilot study introducing a new operative hernioplasty technique. More than 479 patients were included in the technique application until the moment of this study preparation. The author is presenting the first 211 cases in the series who completed a minimum of 2 years follow-up. Between January 2012 and February 2013, 211 patients suffering primary reducible inguinal hernia upon first diagnosis were included. Patients were diagnosed clinically regarding hernia type, size, degree of protrusion, reducibility, and either uni- or bilateral. Abdominal ultrasound examination is achieved to exclude any additional abdominal pathology and confirming clinical diagnosis.
Technique
Procedure name: dual approach hernioplasty (DAH)
The technique follows these steps:
-
1.
Patient is generally anesthetized, Trendelenburg positioned with adducted upper and lower limbs, and lower abdominal, groin and scrotal skin is prepared as usual.
-
2.
Single intravenous shot third-generation cephalosporin antibiotic is given.
-
3.
Peritoneal gas insufflation and three trocars are inserted at supraumbilical and both loins.
-
4.
Identification of the hernia sac and traction to inside the abdominal cavity is made on the sac fundus.
-
5.
Percutaneous Veress needle is introduced extraperitoneally through groin area. The needle is introduced lateral to the pubic tubercle, while the spermatic cord is pushed further laterally. The tip of needle is monitored transperitoneally anchoring the peritoneum above level of the hernia sac neck. Caution is paid not to injure peritoneum to preserve the sealant effect of the potential space and buildup gas pressure upon insufflation. Gas insufflation is then started on pressure 11–13 mm Hg for 3–5 min (Fig. 1).
Fig. 1 
Veress needle is introduced through the groin into the preperitoneal space, and needle tip is seen transabdominally
-
6.
This maneuver will blow the inguinal peritoneum inwards dissecting the sac and peritoneum around from the parietum and releases adhesions to the spermatic cord contents and the anterior abdominal wall. Gas insufflation will make the peritoneum far apart from the abdominal wall in case of direct inguinal hernias, and the sac will not be any more retractile into the inguinal canal in case of indirect inguinal hernia. The peritoneum will show glowing fascia with gas bubbles behind. Gas dissection is considered complete finding the hernia sac base or neck doming posteriorly apart from the abdominal wall without traction on the sac. In the same time, the peritoneum undersurface will appear glassy and full of air bubbles, Veress needle is then removed from the groin, and gas connection is transpositioned to the peritoneal port (Fig. 2).
Fig. 2 
Gas dissection of the preperitoneal space and hernia sac
-
7.
With inward traction of the hernia sac, the peritoneum is then incised transversely 6 cm wide 4 cm above the level of neck of the hernia sac. Wide pocketing for the mesh is found ready made by the previous gas dissection (Fig. 3).
Fig. 3 
Peritoneum is incised, and the preperitoneal fascia is observed as widely separated connective tissue
-
8.
The extraperitoneal space is experienced to be of loose tissue and easily dissected. Only mild refining touches needed to remove fine tissue fibers. The spermatic cord is isolated from whole hernia sac and surroundings (Fig. 4).
Fig. 4 
Spermatic cord is isolated, sac is completely free, and the preperitoneal space is ready for mesh translocation
-
9.
Mersilene mesh (6 × 9 cm) is introduced into the extraperitoneal space as a roll and positioned vertically in the medial side at the pubic tubercle (Fig. 5).
Fig. 5 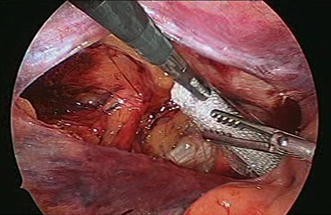
Mesh roll is introduced into the preperitoneal space
-
10.
The mesh sheet is spread laterally to overly the myopectineal rig. Mesh fixation is left to surgeon’s preference. For the author, mesh fixation was restricted to big and long-standing hernias or patients aged fifty or above. Fixation if needed is done to the anterior abdominal musculature using Vicryl tackers. No fixation is made to the pubic tubercle avoiding consequent periosteal-related pain (osteitis pubis) nor too laterally to avoid lateral cutaneous nerve of the thigh entrapment (Fig. 6).
Fig. 6 
Mesh is spread in the preperitoneal space, and sac is retracted intraperitoneally
-
11.
Peritoneum is closed with a pearce string suture using endosuture silk 2/0. The hernia sac is taken in the running suture with the lower edge of the peritoneal window from medial to lateral direction. Then the upper edge of the peritoneal window is taken in the running suture from lateral to medial direction. Finally the pearce string is tensed and closed with a single knot (Fig. 7).
Fig. 7 
Closure of the peritoneum started using sac transfixation with the lower edge of the incised peritoneum
-
12.
Peritoneal closure is completed utilizing the hernia sac been reflected transversely mediolaterally on the peritoneal incision and transfixed (Fig. 8).
Fig. 8 
Peritoneal closure completed with sac transfixed along the peritoneal incision line
-
13.
Abdomen is deflated, ports removed, skin incisions are infiltrated with lidocaine 2 % and closed with subcuticular suture using Vicrapid 4/0.
-
14.
Scrotum and groin are pressed to evacuate minimal to moderate surgical emphysema introduced.








Postoperative care
All patients were treated as day care cases. As patient gains full consciousness, he receives oral fluids and a light meal within 2 h. Patients were encouraged early ambulation and discharged the same procedure night.
Follow-up
First follow-up visit is scheduled within 4–6 days from the discharge date. Monthly follow-up phone call was maintained for at least 24 months. Instructions were given to patients for follow-up visit if any complication symptom is to be experienced by patient.
Results
All study results are tabulated in the following Tables 1, 2, and 3.
There was limited postoperative scrotal emphysema in nine patients out of 211 that resolved spontaneously within the first 4 h. There was no single complication that is known with traditional laparoscopic hernia repair through all approaches known, namely groin pain and numbness, testicular pain, injury to the vas deferens, seroma and hematoma formation, vascular injury, testicular atrophy, mesh infection or mesh migration.
Discussion
The proposed technique DAH proved gas dissection to the preperitoneal space is efficient in isolating hernia sac assisted by hernia sac traction to inside the peritoneal cavity. Such gas induced sac dissection is found to completely separate the sac from both spermatic cord contents and the myopectineal ring boundaries as confirmed by inspection after opening the peritoneal window. In addition, the clarity of the dissection field being bloodless adds another advantage to the DAH technique. Such complete isolation of the sac is considered a crucial point in hernioplasty. Overlooking a leading point of contact or adhesion between the hernia sac and the spermatic cord is the main reason for hernia recurrence. In every case, the neck of the hernia sac has been checked to be away from spermatic cord and the whole myopectineal ring in all cases of the study. There was no need for additional dissection or manipulation to hernia sac. Having a clean bloodless extraperitoneal space is an advantage of this technique. Such result gives a high potential to gas dissection maneuver and confirms the efficiency of such dissection method. Mesh laying down over the myopectineal ring is made easy and fast. Closure of the peritoneal window using endosuture is a little bit time-consuming than peritoneal clip application but serving the target of sac transfixation in the peritoneal suture line itself.
In addition, the technique instructed a new method for hernia sac management other than either excision followed by closure of defect or neck transfixation and excision of distal sac. This way of management is namely hernia sac transfixation and suturing the sac in the peritoneal window closure line. Such way serves two benefits: the first is transfixing the neck of the sac intraperitoneally and the second is the potential to use the sac in peritoneal closure in case there is deficient or macerated peritoneum not enough to interpret between the mesh and the abdominal cavity content.
The study has defined the procedure time (PT) as time interval between insertion of the first abdominal port and last abdominal port extraction. For unilateral case series, PT started with 50 min and reduced to 32 min with a median of 39 ± 2. For bilateral case series, PT started with 75 min and reduced to 55 min with a median of 60 ± 5. The learning curve for the proposed technique was steep within a short period proving technical simplicity.
The technique of DAH seems free of complications, accompanied with minimal scores of postoperative pain to patients and in addition being an easy and fast technique to surgeons.
The preliminary results of the proposed technique seem extremely encouraging. Verification of the new technique is needed on a large number of samples and controlled study design. Critic is invited.
References
Bittner R, Montgomery M, Arregui E, Bansal V, Bingener J, Bisgaard T, Buhck H, Dudai M, Ferzli G, Fitzgibbons RJ, Fortelny RH, Grimes KL, Klinge U, Koeckerling F, Kumar S, Kukleta J, Lomanto D, Misra M, Morales-Conde S, Reinpold W, Rosenberg J, Singh K, Timoney M, Weyhe D, Chowbey P (2015) Update of guidelines on laparoscopic (TAPP) and endoscopic (TEP) treatment of inguinal hernia (International Endohernia Society). Surg Endosc 2:289–321. doi:10.1007/s00464-014-3917-8
Bracale U, Mellilo P, Pignata G, Di Salvo E, Rovani M, Merola G, Pecchia L (2012) Which is the best laparoscopic approach for inguinal approach for inguinal hernia repair: TEP or TAPP? A systemic review of the literature with a network metanalysis. Surg Endosc 6(12):3355–3366
O’Rourke A, Zell J, Varkey-Zell T, Barone J, Bayona M (2002) Laparoscopic diagnosis and repair of asymptomatic bilateral inguinal hernias. Am J Surg 183(1):15
Carvalho G, Loureiro M, Bonin E, Claus C, Silva F, Cury A, Fernandes F (2012) Minilaproscopic technique for inguinal hernia combining transabdominal pre-peritoneal and totally extraperitoneal approaches. JSLS 16(4):569–575
Wenbin L, Yuzhou L (2010) The application of modified transabdominal preperitoneal and totally prosthetic laparoscopic hernioplasty. Surg Laparosc Endosc Percutan Tech 20(2):e57–e59
Dilek O (2014) Hernioplasty and testicular perfusion. Sprinerplus 21(3):107. doi:10.1186/2193-1801-3-107 (E Collection 2014)
Lau H (2007) Recurrence following endoscopic extraperitoneal inguinal hernioplasty. Hernia 11(5):415–418
Stylianidis G, Haapamaki M, Sund M, Nilsson E, Nordin P (2010) Management of the hernia sac in inguinal hernia repair. Br J Surg 97(3):415–419
Disclosures
The author Dr. Mohamed M. Nasr has no disclosures or conflicts of interest or financial ties to disclose related to this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nasr, M.M. Early results of dual approach hernioplasty (DAH): an innovative laparoscopic inguinal hernioplasty technique. Surg Endosc 30, 1113–1118 (2016). https://doi.org/10.1007/s00464-015-4308-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4308-5