
Abstract
Background
Robot-assisted laparoscopic pancreaticoduodenectomy is a novel minimally invasive surgery technique, and its effectiveness and safety remain unknown in patients with borderline malignant or malignant diseases. This study aimed to prospectively evaluate the effectiveness and safety of RLPD versus open PD (OPD).
Methods
Between January 2010 and December 2013, 180 eligible patients were prospectively hospitalized for elective RLPD (n = 60) or OPD (n = 120). They were matched for tumor location, tumor type, tumor size, ASA classification, age, and sex. The main outcome measures included demographics, intraoperative variables, morbidity, postoperative recovery, and mid-term evaluation.
Results
Over the study period, the RLPD group had a significantly longer but decreasing operative time (median 410 vs. 323 min; P < 0.001), less blood loss (median 400 vs. 500 mL; P = 0.005), better nutritional status recovery, expedited off-bed return to activity (3.2 vs. 4.8 d; P < 0.001), faster resumption of bowel movement (3.6 vs. 5.2 d; P < 0.001), and shorter hospital stay (20 vs. 25 d; P = 0.002) compared to the OPD group. The two groups had similar surgical morbidities and mortality as well as R0 resection rate and number of lymph nodes resected. Among patients with pancreatic adenocarcinoma, the two groups had similar overall and disease-free survival (ACTRN12614000299606).
Conclusions
This first largest, prospective matched study demonstrated that for treating selected borderline and malignant pathologies, RLPD was associated with a significant learning curve effect and expedited postoperative recovery, but had a surgical and oncological safety profile similar to OPD.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Pancreaticoduodenectomy (PD) is a major surgical operation involving the pancreas, duodenum, and pylorus in most cases and was first described in 1938 for treating borderline or malignant pancreatic head, common bile duct, and duodenal pathologies [1]. PD has always been a huge challenging procedure for many surgeons because of its technical complexity and the difficulty associated with extensive visceral organ dissection and reconstruction of the digestive tract continuity. Therefore, PD is normally performed using an open approach through a long abdominal wall incision.
Laparoscopy is a minimally invasive surgery technique that has been widely accepted in surgical practice due to its good cosmetic outcome and expedited postoperative recovery [2]. However, the use of laparoscopy is relatively restricted in PD because of intrinsic technical limitations of PD and controversial surgical and oncological safety. No more than 300 cases of laparoscopic PD were retrieved from the current literature since the first case of laparoscopic PD was reported by Gagner et al. in 1994 [3]. Robot-assisted laparoscopy is the most advanced minimally invasive surgery technique and is characterized by magnified three-dimensional visualization and EndoWrist instruments with greater range of motion. Robotic assistance has been improving laparoscopic PD practice since Giulianotti et al. reported the first case of robot-assisted laparoscopic PD (RLPD) in 2003 [4].
Although more than 200 cases of RLPD have been documented in the current literature over recent years and the safety of RLPD has been recognized [5, 6], the effectiveness and safety of RLPD compared to open PD (OPD) have not yet been clearly described in comparative studies [7–10], especially with respect to radical resection associated with oncological prognosis. Given the high cost of robotic surgery, it is hard to conduct a randomized controlled study within the past 10 years, while a large-scale, non-randomized study comparing RLPD and OPD deserves equal attention. The primary objective of this study was to prospectively evaluate the effectiveness and safety (mainly including operative time, blood loss, and morbidity) of RLPD as compared to OPD. We also assessed the learning curves, nutritional status recovery, and mid-term oncologic outcomes.
Methods
Study design
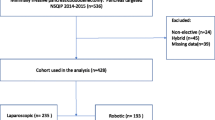
The study protocol was approved by the Medical Ethics Committee at Ruijin Hospital in accordance with the latest version of the Declaration of Helsinki and registered as http://www.anzctr.org.au (registration ID: ACTRN12614000299606). Between January 2010 and December 2013, 866 patients with confirmed or suspected borderline or malignant pathologies of the pancreatic head, distal common bile duct, and periampullary region were consecutively and prospectively enrolled for elective PD at our Department of General Surgery, a multidisciplinary, academic tertiary care unit with an annual volume of approximately 250 cases of PD. All included patients had to be eligible for both RLPD and OPD to minimize possible selection bias. The RLPD group was matched with the OPD group at a ratio of 1:2 using a matching patient’s algorithm according to age (within ±5 years), sex, body mass index (BMI <18.5 vs. 18.5–24.9 vs. 25.0–29.9 vs. ≥30 kg/m2), American Society of Anesthesiologists (ASA) physical status classification (I vs. II vs. III), malignancy (malignant vs. non-malignant), location (pancreas vs. distal common bile duct vs. periampullary region), and size of tumor. The matching process was verified every two enrollments in the RLPD group to allow targeted recruitment into the OPD group. All patients included were well informed of the advantages and disadvantages of RLPD and OPD by independent research nurses. All patients voluntarily gave written informed consent for participation in this study, and the use of the robotic approach or not was at the sole discretion of the patient.
The inclusion criteria were at least 18 years old; a resectable malignant or borderline malignant pathology of the pancreatic head (including stage I and II pancreatic cancer), distal common bile duct or periampullary region in accordance with the National Comprehensive Cancer Network (NCCN) guidelines. The exclusion criteria were an excessively large lesion (tumor size >10 cm) invading adjacent organs and major vessels; involvement of superior mesenteric vein or portal vein (PV) longer than 3 cm detected on preoperative thin-slice (3 mm) computed tomography (CT) scan and CT portal venography, if applicable, possibly requiring interposed graft reconstruction, for which OPD was determined to be more suitable than RLPD; scheduled for surgical treatment other than PD, such as palliative biliary and gastroenteric anastomoses; having received neoadjuvant chemoradiation therapy; presence of complicating serious cardiopulmonary or hepatorenal insufficiency; extensive intraperitoneal or extraperitoneal metastases; and refusal to participate in or withdrawing from this study. Patients who had undergone palliative biliary drainage and PV resection or reconstruction were included, whereas those who had undergone a non-PD procedure, such as enucleation and segmental duodenal resection, with arterial reconstruction were excluded.
Surgical procedures
All patients received routine hematological, biochemical, and oncological tests in accordance with the institutional practice guidelines. An abdominal thin-slice (3 mm) computed tomography scan was performed to delineate the size and location of the lesion. All surgical procedures were performed by an assigned surgical team, consisting of resident surgeons, anesthesiologists, clinical pathologists, radiologists, surgical nurses, and research nurses and led by two board-certified attending general surgeons (BS and CP) experienced in both open and robotic surgery. In the pilot study before the present work, this surgical team had performed more than 50 robotic surgeries, including 12 PDs.
All RLPDs were performed using the da Vinci Surgical System Model S (Model S; Intuitive Surgical, Inc, Sunnyvale, CA, USA). The first 40 cases of RLPDs were performed using the previously reported classical procedure (Fig. 1A, left panel), and a modified “bottom-up” approach was used in the last 20 cases (Fig. 1A, right panel) from January 2013 onwards [11]. In the modified approach (Fig. 2), the lesser omental sac was dissected to expose the pancreas, and the pancreas was dissected along the inferior margin to expose the superior mesenteric vessels (SMVs). The SMVs were meticulously dissected to create a retropancreatic tunnel, and an extended Kocher maneuver was performed to mobilize the transverse duodenum and dissect the duodenojejunal flexure starting from the right margin of the ligament of Treitz beneath the superior mesenteric vessels. The jejunal loop was retracted into the right upper quadrant below the mesenteric vessels and transected at the right margin of the superior mesenteric vessels above the transverse mesocolon. After the dissection of the hepatic hilum, the gastroduodenal artery was dissected and ligated to expose the PV. The pancreatic neck was dissected to locate the pancreatic duct. The root of the SMVs was dissected from cephalically toward caudally, and the stomach was transected after the nasogastric tube was withdrawn. Intraoperative frozen biopsy was performed to evaluate the pathology of the pancreatic disease and the cleanness of the resection margin. The jejunal limb was retracted toward the right side beneath the SMVs and positioned in the right upper quadrant for reconstruction (Fig. 1B). A two-layered end-to-side, duct-to-mucosa pancreaticojejunostomy was performed in all patients as routine practice. The stumps of the pancreatic ducts were sutured using 6-0 absorbable polydioxanone sutures (PDS II; Ethicon, Cincinnati, OH, USA), and a 5F or 8F pediatric Silastic feeding tube was placed to stent the pancreatic duct. The stump of the pancreatic parenchyma was anastomosed with the seromuscular layer of the jejunum using 3-0 nonabsorbable polypropylene sutures in a horizontal mattress manner. A single-layer hepaticojejunostomy was fashioned as an end-to-side anastomosis using 5-0 Vicryl (RB1; Ethicon) in a running technique for a duct >5 mm in diameter or in an interrupted technique for a duct ≤5 mm. An antecolic, two-layered gastrojejunostomy was performed to reconstruct the gastrointestinal tract continuity. The PV and SMV were reconstructed using non-interrupted 5-0 polypropylene sutures. Two peritoneal drains were positioned posterior to the biliary anastomosis and inferior to the pancreatic anastomosis.

Conventional and modified “bottom-up” procedures of RLPD (A) and reconstruction in RLPD (B) and OPD (C). The arrows indicate the ligament of Treitz

Representative photographs and laparoscopic views of RLPD: A dissection of the pancreas; B dissection of the hepatic hilum; C division of the pancreatic neck; D dissection of the uncinate process; E pancreaticojejunostomy; F hepaticojejunostomy; G gastrojejunostomy; and H reconstruction of PV-SMV. PV portal vein, SMV superior mesenteric vein, GDA gastroduodenal artery, PHA proper hepatic artery, CBD common bile duct, ASPDV anterior superior pancreaticoduodenal vein, MCV middle colic vein, GCT Henle’s gastrocolic trunk. White arrowhead shows grasping of the accessory right colic vein in panel 1
All OPDs were performed using the standard PD procedure with antrectomy or pylorus preservation as previously described [12]. Segmentectomy or wedge resection was performed in the case of PV or SMV involvement. Lymphadenectomy involved all lymph nodes located to the right of the PV and SMV. The end-to-end pancreaticojejunostomy and end-to-side hepaticojejunostomy were performed to reconstruct continuity of the gastrointestinal tract (Fig. 1C).
Postoperative care
The nasogastric tube was removed on the first or second postoperative days, and frequent oral intake of a small amount of low-fat soft, solid diet was resumed if well tolerated. Plasma glucose was closely monitored, and hyperglycemia was controlled using intravenous insulin. The amylase content in peritoneal drainage was followed up on postoperative day 5, and the drain was removed in the absence of evident pancreatic fistula. All patients with pancreatic adenocarcinoma underwent adjuvant chemotherapy with gemcitabine and 5-fluorouracil as recommended by the NCCN guideline [13].
Main outcome measures
Patient characteristics included age, gender, body mass index (BMI), ASA score, and the presence of concomitant medical conditions, such as diabetes mellitus, hypertension, cardiac, and pulmonary disease.
Operative variables mainly included conversion rate, operative time (OT), intraoperative blood loss, and transfusion rate. Postoperative variables mainly included morbidity and mortality. Pancreatic fistula was diagnosed in accordance with the International Study Group for Pancreatic Fistula (ISGPF) criteria [14]. Postoperative morbidities were evaluated according to the Clavien–Dindo classification system [15]. A major complication was defined as Clavien–Dindo classification ≥3.
The learning curve was plotted to evaluate main intra- and postoperative variables, including OT, blood loss, and morbidities. Within the RLPD group, the first 40 patients (early period) using conventional approach were compared with the last 20 patients (late period) using “bottom-up” approach included in 2013, both of whom were further compared with those undergoing OPD within the same period to access the improvement of effectiveness of RLPD.
Recovery variables included times to resume off-bed activities, bowel movement and oral intake, fasting plasma glucose, time length of hospital stay, and nutritional status (total protein, pre-albumin, and hemoglobin) change from the baseline.
Short-term pathological and oncological variables included histological classification, tumor size, number of lymph nodes resected and positive nodes, TNM stage, and resection margin (the common bile duct, SMVs, portal vein, pancreatic neck, and uncinate process) cleanness. Mid-term outcomes included overall and disease-free survival. All patients with borderline malignant or malignant tumors were followed up monthly in the first year and quarterly afterwards in the absence of tumor recurrence. Computed tomography scanning was performed 1 month after the operation, quarterly in the first year, and semiannually afterwards. Tumor recurrence was identified using a combined examination of computed tomography scanning, magnetic resonance imaging, and serum tumor biomarker. Patients were followed up until the time of death or the cutoff date of this study (June 30, 2014).
Cost analysis included any costs associated with operation and consumables, anesthesia, nursing, laboratory tests, and overall hospital stay. The cost of postdischarge care, follow-up, or home nursing was excluded from this analysis.
Statistical analysis
The statistical software SPSS 19.0 (SPSS Inc, Chicago, IL, USA) was used for the statistical analysis. Continuous data were expressed as mean (SD) or mean (SEM) or median (interquartile range, IQR), and the means were compared using the two independent samples Student’s t test. Categorical data were compared using the Chi-square test or Fisher’s exact probability test. The Mann–Whitney U test was used for non-normally distributed variables. The Spearman’s rank correlation coefficient (ρ) was used to determine whether OT and bleeding volume indicated a significant “learning curve.” Survival analysis was performed using the Kaplan–Meier method and validated using the log-rank test. A P value less than 0.05 was considered statistically significant.
Results
Patient characteristics
Overall, 180 eligible patients, aged 18–77 years and including 99 males and 81 females, were included in this study. Among these patients, 60 patients underwent RLPD (RLPD group, n = 60) and 120 patients underwent OPD (OPD group, n = 120). The patients’ demographic and clinical characteristics are listed in Table 1. The two groups were comparable in terms of tumor location, tumor malignancy, tumor size, age, sex, body mass index, ASA physical status classification, previous history of abdominal surgery, and concomitant medical conditions (all P values >0.05). The maximum tumor size was 9.8 cm in the RLPD group and 10 cm in the OPD group. Within the RLPD group, the first 40 patients were similar to the last 20 patients with respect to tumor location, tumor malignancy, age, sex, BMI, ASA class, tumor size, and history of previous abdominal surgery (all P > 0.05) (Table 2). Among patients included in 2010–2012 or 2013, the two groups were comparable in demographic and clinical variables (Table S1).
Intraoperative outcome
The operative outcomes are listed in Table 3. All patients underwent successful en bloc PD as scheduled, and only one patient (1.7 %) enrolled in 2010 required conversion of RLPD to laparotomy due to difficulty in dissecting the uncinate process and requirement of PV-SMV and PV-splenic vein reconstruction. The RLPD group had a significantly longer mean OT (410 [103] vs. 323 [80] min; P < 0.001) but less median blood loss (400 vs. 500 mL; P = 0.005) compared to the OPD group. Both OT (ρ = −0.611; P < 0.001; Fig. 3A) and blood loss (ρ = −0.607, P < 0.001; Fig. 3B) were associated with significant “learning curves” in the RLPD group. The last 20 RLPD patients had significantly shorter mean OT (340 [98] vs. 445 [88] min; P < 0.001; Fig. 3C) and less mean blood loss (275 [255] vs. 532 [262] mL; P < 0.001; Fig. 3D) than the first 40 counterparts. Among patients included in 2010–2012, RLPD patients had a significantly longer mean OT (445 [88] vs. 322 [73] min; P < 0.001) but similar median blood loss (500 vs. 500 mL; P = 0.201) compared to OPD counterparts; however, among patients included in 2013, RLPD patients had a similar mean OT (340 [98] vs. 324 [92] min; P = 0.981) but significantly less median blood loss (200 vs. 500 mL; P = 0.002) compared to OPD counterparts.

Learning curve effects of RLPD with respect to OT, blood loss, and morbidity rates. Error bars represent SEM
No uncontrollable massive bleeding or other clinically significant intraoperative incidents occurred. The two groups had similar percentages of patients requiring blood transfusion and similar reconstruction approach of gastrointestinal continuity. It is noted that the frequency of vessel end-to-end reconstruction (3[5 %] vs. 8[6.7 %], P = 0.912) and the mean length of segmental PV resection (3.8 [0.8] vs. 3.9 [1.0] cm, P = 0.950) were equivalent between the two groups.
Morbidities and mortality
Surgical morbidities and mortality are described in Table 4. The two groups had similar overall morbidities, Clavien–Dindo class 1/2 morbidities, and Clavien–Dindo class 3/4/5 morbidities. The morbidity rate showed a decline in the RLPD group, especially for the overall (20.0 %) and major (0.0 %) complication rates among the last 20 cases (Fig. 3E, F). Among patients in 2010–2012 or 2013, the two groups also had similar overall morbidities, Clavien–Dindo class 1/2 morbidities and Clavien–Dindo class 3/4/5 morbidities (Table S2).
Major postoperative complications included pancreatic fistula, delayed gastric emptying, bile leak, gastrointestinal anastomostic leak, postoperative intra-abdominal bleeding, intraperitoneal fluid collection, surgical site infection, and afferent loop obstruction. Among overall patients, the two groups experienced a similar frequency of overall and ISGPF grade A/B/C pancreatic fistula (all P values > 0.05), but no grade C pancreatic fistula occurred in the RLPD group. The two groups also exhibited similar frequencies of all other major complications (all P values > 0.05) except for surgical site infection (1[1.7 %] vs. 15[12.5 %]; P = 0.033). Most of postoperative complications required no surgical intervention and resolved after medical treatment. The two RLPD patients (3.3 %) who experienced afferent loop obstruction required second-look surgery, and one RLPD patient (1.7 %) died of refractory acute renal failure of unknown etiology. In contrast, four OPD patients (3.3 %) experienced grade C pancreatic fistula, developed complicating intra-abdominal bleeding, and required emergency second-look surgery; three of these patients (2.5 %) died of disseminated intravascular coagulation (1 patient), massive bleeding (1 patient), or sepsis (1 patient).
Postoperative recovery
The postoperative recovery data are listed in Table 5. The two groups had the similar preoperative nutritional at the baseline. And according to our center clinic path, the postoperative fluid replacement strategy between two groups was same. The RLPD group showed a significantly faster recovery of nutritional status compared to the OPD group (Fig. 4). Since the 7th postoperative day, the RLPD group had significantly better recovery in total protein, pre-albumin, and hemoglobin levels (all P values < 0.05) compared to the OPD group.

Changes in postoperative serum total protein (A), pre-albumin (B), and hemoglobin (C) relative to baseline levels. Error bars represent SEM. *P < 0.05
The RLPD group had significantly shorter mean times to resume off-bed activities (3.2 [0.6] vs. 4.8 [2.4] d; P < 0.001), bowel movement (3.6 [1.6] vs. 5.2 [2.3] d; P < 0.001), and oral intake (3.1 [1.7] vs. 4.7 [2.3] d; P < 0.001) compared to the OPD group. The RLPD group also had a significantly shorter mean length of hospital stay than the OPD group (20 [7.4] vs. 25 [11.2] d; P = 0.002). The RLPD group had a significantly lower mean fasting plasma glucose level than the OPD group (7.0 [1.8] vs. 7.5 [1.4] mmol/L; P = 0.042). Moreover, RLPD was associated with a significantly higher overall cost (19,755 [10,067] vs. 12,111 [6456] USD; P < 0.001) but a significantly lower postoperative cost (8529 [4253] vs. 10,559 [6291] USD; P = 0.025) compared to OPD.
Oncological outcome
Pathological outcomes are described in Table 6. The two groups were similar in pathology of the pancreatic head disease (P > 0.05), and the most frequent pathology was pancreatic adenocarcinoma in both groups. The two groups had similar mean tumor size (2.9 [1.4] vs. 3.0 [1.3] cm; P = 0.636), mean number of lymph nodes resected (13.6 [6.0] vs. 12.5 [8.0]; P = 0.350), and rate of R0 resection for non-benign diseases (45/46[97.8 %] vs. 88/92[95.7 %]; P = 0.872).
Among patients with pancreatic adenocarcinoma, the two groups also had similar mean tumor size (3.0 [0.9] vs. 3.1 [1.0] cm; P = 0.716), mean number of lymph nodes resected (18.1 [6.6] vs. 17.8 [7.1]; P = 0.890), R0 resection rate, number of lymph nodes resected and positive nodes, T stage, lymph node metastasis rate, and American Joint Committee on Cancer tumor stage [16]. No patient was lost to follow-up. Mean oncologic follow-up period was 22 ± 10 mo in the RLPD group and 21 ± 8 mo in the OPD group, respectively. The two groups had similar median overall survival (23.0 vs. 22.0 months; P = 0.748; Figure S1-A) and disease-free survival (14.0 vs. 13.0 months; P = 0.364; Figure S1-B).
Discussion
The recent technical developments have made it feasible to apply the use of laparoscopy to pancreatic surgery including PD, one of the most complex abdominal surgical procedures. However, laparoscopic PD is still considered as an “investigational” procedure in current practice due to its huge intrinsic technical challenges and, as such, is normally performed only in highly selected patients by a few expert laparoscopic surgeons [17]. The limitations of laparoscopic pancreatic surgery include reduced freedom of manipulative motion, narrowed two-dimensional view, and a long learning curve. Two previous comparative studies could not clearly justify the advantages of laparoscopic PD over OPD [18, 19].
Robotic surgery, the state-of-art minimally invasive surgery technology, has been developed to overcome the aforementioned limitations and improve the precision of surgical procedures. In the scenario of PD, RLPD is especially advantageous in dissecting lymph nodes of major vasculatures and the uncinated process and in the reconstruction of gastrointestinal continuity due to the superior dexterity of the robotic surgery system [11]. Four retrospective case series were reported in the current literature to retrospectively assess the safety and feasibility of RLPD compared with OPD [7–10]. Our results together with these previous reports confirm that RLPD has a similar feasibility and safety profile compared to open surgery. Furthermore, our study demonstrated that RLPD is associated with a significant learning curve effect with respect to OT, blood loss, and morbidity; faster recovery of nutritional status; and similar survival compared to OPD. To the best of our knowledge, the present work was the first prospective study comparing RLPD and OPD, especially with respect to the mid-term follow-up result, and involved the largest sample size ever in Chinese population.
A major limitation of RLPD shown by our results is the relatively long OT including the time for preparing the robotic system and instruments, consistent with previous reports [7–9]. However, the OT of RLPD became gradually shortened over the 4-year study period, especially in the last 20 cases (P < 0.001) comparing to the early period. This reduction might result from the use of our modified laparoscopic technique, in which an upward angle of view in the abdominal cavity could help to improve the flow of laparoscopic manipulation. When the robotic arms held the laparoscopic instruments in the lower abdominal cavity through the fixed trocar ports, a limited range of movement was available for the laparoscope and other manipulating instruments, resulting in a large number of “blind spots” in the early 40 cases. In contrast, the modified “bottom-up” approach maximized the use of robotic arms in the last 20 cases and significantly shortened the OT and robotic surgery learning curve. The OT of RLPD was significantly shortened close to that of OPD reported by our series and some other high-volume academic pancreatic surgery centers. The shortest case in the last 20 RLPD cases cost only 180 min in a patient with pseudopapillary tumor.
Better bleeding control is one of the primary advantages of the robotic approach, which facilitates dissection of major vessels by effectively preventing massive bleeding. Our study demonstrated that RLPD-associated blood loss was significantly decreased and also exhibited an encouraging “learning curve” effect compared to OPD, especially for the late period. Owing to a large degree of freedom offered by the EndoWrist technique and an improved three-dimensional visualization, robotic assistance allows the surgeon to more precisely locate and dissect the SMVs for vessel control, especially in the case of tumor invasion. Moreover, the increased degree of freedom also enables the surgeons to complete relatively complex vessel reconstruction, which used to be impossible if using conventional laparoscopy. Giulianotti et al. pioneered the use of the robotic system for vessel reconstruction and suggested that robotic assistance would be able to widen the indications of laparoscopic surgery to locally advanced pancreatic tumors [20]. Our finding that RLPD resulted in a vessel reconstruction profile similar to that for OPD reaffirmed the effectiveness and safety of robot-assisted vessel reconstruction in PD, which was also reported for the first time in Asia. Venous involvement may not be an absolute contraindication to robotic surgery. It is also likely that prosthetic graft reconstruction can be completed using the robotic surgery technique for segmental PV resection longer than 5 cm. Conversely, uncontrollable bleeding and vessel reconstruction are also major causes of conversion of laparoscopic PD to OPD. Our results together with previous reports showed that robotic assistance was beneficial in reducing conversion rate when compared to conventional laparoscopic approach [5, 6].
PD is subject to a high morbidity rate even in high-volume centers, approximating 41 % for the open approach [21]. In accordance with the Clavien–Dindo classification system, the two groups experienced similar frequencies of mild, moderate, severe, and overall complications shown by our results, similar with that reported by Chalikonda et al. in a case-matched comparison study [8]. It was encouraging that RLPD also exhibited a “learning curve” effect with respect to postoperative complications. This suggested that a lower morbidity rate associated with RLPD might result from the minimized invasiveness of robotic assistance and become evident in the hands of experienced laparoscopic surgeons.
Pancreatic fistula remains the most common and serious postoperative complication associated with PD. The incidence rate of pancreatic fistula after OPD was reported to be 10 − 20 % in accordance with the ISGPF criteria [22, 23]. Our results together with previous reports showed that robotic assistance could not decrease the occurrence or severity of pancreatic fistula associated with PD. It was noted that none of the patients who experienced severe (grade C) pancreatic fistula required surgical intervention in the RLPD group. However, grade C pancreatic fistula was the major cause of reoperation and mortality, although the mortality rate was similar between the two groups in agreement with the previous reports regarding RLPD and OPD [24, 25]. However, statistical insignificance might be due to the insufficient statistical power.
The robotic approach was associated with a statistically higher frequency of afferent loop obstruction although not clinically significant compared to the open approach. Afferent loop obstruction usually occurs in 0.3 % of patients undergoing gastroenterostomy [26], including Billroth II gastrectomy and PD, possibly due to intestinal adhesion/angulation, internal hernia, anastomostic stricture, and tumor recurrence [27, 28]. A major procedural difference between the two approaches was the position of the pancreaticobiliary jejunal limb. In the open approach, the jejunal limb is brought through the transverse mesocolon to the right upper quadrant and fixed to the transverse mesocolon (Fig. 1C), whereas in the robotic approach, the jejunal limb is directly brought through the opening left to the ligament of Treitz and posterior to the SMVs into the supramesocolic compartment for technical convenience (Fig. 1B) [11]. Therefore, RLPD patients were more prone to angulation when intestinal adhesions or internal hernia occurring in the jejunum limb. The second-look surgery in the two patients who experienced afferent loop obstruction identified intestinal angulation in proximity to the ligament of Treitz.
Expedited postoperative recovery is expected to be one of the main advantages of incorporating robotic assistance. Our results showed that RLPD patients were able to resume off-bed activities, bowel movement, oral intake, and after-discharge daily activities at an earlier time point than OPD patients. It is noted that the expedition of postoperative recovery associated with robotic assistance was not sufficiently addressed in previous reports. Our biochemical data demonstrated for the first time that RLPD patients exhibited a significantly faster nutritional status recovery with respect to serum total protein and pre-albumin as well as hemoglobin within the first two postoperative weeks. This clinical benefit might result from earlier resumption of oral intake, less incisional pain, and a more relaxed psychological status, especially after parenteral nutrition was switched to enteral nutrition at postoperative day 5–7 [29–31]. Expedited postoperative recovery might help to improve RLPD patients’ short-term postoperative quality of life and reduce postoperative cost. It was noteworthy that hemoglobin slightly decreased within the first three postoperative days, which might result from no routine use of hemostatic medication at our center. Hyperglycemia is a common surgical morbidity after PD, but blood glucose was well controlled in both groups within the normal limits [32].
Oncological outcome is the major concern arising from RLPD among patients suffering from malignant diseases. R0 resection and the number of lymph nodes resected, two key oncologic adequacy measures, are accepted as two reliable factors predicting the long-term survival after PD for malignant pancreatic or periampullary diseases [33, 34]. Our results showed that the two groups had similar R0 resection rates and numbers of lymph nodes resected; however, Chalikonda et al. and Zeh et al. reported a significantly higher frequency of R0 resection after RLPD [8, 35], and Buchs et al. reported a significantly greater number of lymph nodes resected in RLPD patients [10]. These differences might result from the investigator’s bias (relatively fewer selected patients in our study). The mid-term survival data are rarely reported for pancreatic cancer patients undergoing RLPD versus OPD. Our follow-up results demonstrated for the first time that the two approaches were associated with a similar overall survival among patients with pancreatic adenocarcinoma, consistent with the previous report [36]. Given our follow-up period might be relatively short considering the usual survival analysis, we also collected the data of disease-free survival which would be strongly correlated with 5-year overall survival [37]. Moreover, most recurrences of pancreatic cancer usually occur within 6–15 months and median disease-free survival was 6.9 months for patients received no postoperative chemotherapy according to a multicenter RCT [38]. Therefore, the length of follow-up in our study could be considered acceptable for comparison of oncological outcome between RLPD and OPD.
We acknowledged that our study was a non-randomized study with some inherent bias; however, a 1:2 matching comparison was used to control patient selection bias. In addition, all included patients were determined to be eligible for both RLPD and OPD on preoperative workup to minimize patient selection bias. Although a randomized, controlled study is ideal to validate the effectiveness and safety of RLPD, it poses some practical challenges as robotic surgery is at a high cost. We observed that hospital stay including preoperative period in our center was relatively longer compared to that in Western practices, mainly due to sociocultural variation in Chinese healthcare system rather than surgical care quality. It is noted that the average length of hospital stay was approximate 3–4 weeks in most area of mainland China. In addition, our center provided both early postoperative care and subsequent nursing care for each patient in a single hospitalization. Therefore, patients usually opted to discharge after full recovery.
Conclusions
RLPD is an effective, safe alternative treatment option compared to OPD. The primary advantages of RLPD over OPD include minimal invasiveness and expedited postoperative recovery possibly due to the improved visualization and precise manipulation. The relatively longer OT and similar morbidity associated with RLPD compared to OPD show a significant “learning curve” effect, and both are expected to improve in the hands of experienced laparoscopic surgeons. Our oncological results demonstrated that the two approaches are associated with a similar oncologic adequacy and overall survival. The long-term therapeutic benefit of RLPD remains to be investigated in further large-scale, multi-center, randomized controlled studies.
References
Whipple AO (1945) Pancreaticoduodenectomy for islet carcinoma: a five-year follow-up. Ann Surg 121:847–852
Gagner M, Lacroix A, Bolte E (1992) Laparoscopic adrenalectomy in Cushing’s syndrome and pheochromocytoma. N Engl J Med 327:1033
Gagner M, Pomp A (1994) Laparoscopic pylorus-preserving pancreatoduodenectomy. Surg Endosc 8:408–410
Giulianotti PC, Coratti A, Angelini M et al (2003) Robotics in general surgery: personal experience in a large community hospital. Arch Surg 138:777–784
Cirocchi R, Partelli S, Trastulli S et al (2013) A systematic review on robotic pancreaticoduodenectomy. Surg Oncol 22:238–246
Zureikat AH, Moser AJ, Boone BA et al (2013) 250 robotic pancreatic resections: safety and feasibility. Ann Surg 258:554–562
Lai EC, Yang GP, Tang CN (2012) Robot-assisted laparoscopic pancreaticoduodenectomy versus open pancreaticoduodenectomy—a comparative study. Int J Surg 10:475–479
Chalikonda S, Aguilar-Saavedra J, Walsh R (2012) Laparoscopic robotic-assisted pancreaticoduodenectomy: a case-matched comparison with open resection. Surg Endosc 26:2397–2402
Zhou NX, Chen JZ, Liu Q et al (2011) Outcomes of pancreatoduodenectomy with robotic surgery versus open surgery. Int J Med Robot Comp 7:131–137
Buchs NC, Addeo P, Bianco FM et al (2011) Robotic versus open pancreaticoduodenectomy: a comparative study at a single institution. World J Surg 35:2739–2746
Giulianotti PC, Sbrana F, Bianco FM et al (2010) Robot-assisted laparoscopic pancreatic surgery: single-surgeon experience. Surg Endosc 24:1646–1657
Warshaw AL, Thayer SP (2004) Pancreaticoduodenectomy. J Gastroint Surg 8:733–741
Tempero MA, Arnoletti JP, Behrman SW et al (2012) Pancreatic adenocarcinoma, Version 2.2012 featured updates to the NCCN Guidelines. J Natl Compr Cancer Netw 10:703–713
Bassi C, Dervenis C, Butturini G et al (2005) Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 138:8–13
Dindo D, Demartines N, Clavien P-A (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240:205–213
Greene FL (ed) (2002) AJCC cancer staging manual, vol 1. Springer, New York
Gumbs AA, Rivera AMR, Milone L et al (2011) Laparoscopic pancreatoduodenectomy: a review of 285 published cases. Ann Surg Oncol 18:1335–1341
Kuroki T, Adachi T, Okamoto T et al (2012) A non-randomized comparative study of laparoscopy-assisted pancreaticoduodenectomy and open pancreatico- duodenectomy. Hepatogastroenterol 59:570–573
Cho A, Yamamoto H, Nagata M et al (2009) Comparison of laparoscopy-assisted and open pylorus-preserving pancreaticoduodenectomy for periampullary disease. Am J Surg 198:445–449
Giulianotti PC, Addeo P, Buchs NC et al (2011) Robotic extended pancreatectomy with vascular resection for locally advanced pancreatic tumors. Pancreas 40:1264–1270
Cameron JL, Riall TS, Coleman J et al (2006) One thousand consecutive pancreaticoduodenectomies. Ann Surg 244:10–15
Gebauer F, Kloth K, Tachezy M et al (2012) Options and limitations in applying the fistula classification by the International Study Group for Pancreatic Fistula. Ann Surg 256:130–138
Dong X, Zhang B, Kang MX et al (2011) Analysis of pancreatic fistula according to the International Study Group on Pancreatic Fistula classification scheme for 294 patients who underwent pancreaticoduodenectomy in a single center. Pancreas 40:222–228
Venkat R, Puhan MA, Schulick RD et al (2011) Predicting the risk of perioperative mortality in patients undergoing pancreaticoduodenectomy: a novel scoring system. Arch Surg 146:1277–1284
Winter JM, Brennan MF, Tang LH et al (2012) Survival after resection of pancreatic adenocarcinoma: results from a single institution over three decades. Ann Surg Oncology 19:169–175
Jordan GL (1971) Surgical management of postgastrectomy problems. Arch Surg 102:251–259
Blachar A, Federle MP, Pealer KM et al (2002) Gastrointestinal complications of laparoscopic Roux-en-Y gastric bypass surgery: clinical and imaging findings I. Radiology 223:625–632
Higa KD, Ho T, Boone KB (2003) Internal hernias after laparoscopic Roux-en-Y gastric bypass: incidence, treatment and prevention. Obesity Surg 13:350–354
Fearon KCH, Ljungqvist O, Von Meyenfeldt M et al (2005) Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. Clin Nutr 24:466–477
Caro MMM, Laviano A, Pichard C (2007) Nutritional intervention and quality of life in adult oncology patients. Clin Nutr 26:289–301
Braga M, Ljungqvist O, Soeters P et al (2009) ESPEN guidelines on parenteral nutrition: surgery. Clin Nutr 28:378–386
Kansagara D, Fu R, Freeman M et al (2011) Intensive insulin therapy in hospitalized patients: a systematic review. Ann Intern Med 154:268–282
Shimada K, Sakamoto Y, Sano T et al (2006) Prognostic factors after distal pancreatectomy with extended lymphadenectomy for invasive pancreatic adenocarcinoma of the body and tail. Surgery 139:288–295
Slidell MB, Chang DC, Cameron JL et al (2008) Impact of total lymph node count and lymph node ratio on staging and survival after pancreatectomy for pancreatic adenocarcinoma: a large, population-based analysis. Ann Surg Oncol 15:165–174
Zeh HJ, Zureikat AH, Secrest A et al (2012) Outcomes after robot-assisted pancreaticoduodenectomy for periampullary lesions. Ann Surg Oncol 19:864–870
Sohn TA, Yeo CJ, Cameron JL et al (2000) Resected adenocarcinoma of the pancreas—616 patients: results, outcomes, and prognostic indicators. J Gastroint Surg 4:567–579
Sargent DJ, Wieand HS, Haller DG et al (2005) Disease-free survival versus overall survival as a primary end point for adjuvant colon cancer studies: individual patient data from 20,898 patients on 18 randomized trials. J Clin Oncol 23(34):8664–8670
Oettle H, Post S, Neuhaus P et al (2007) Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA 297(3):267–277
Acknowledgments
The authors thank all of the volunteer participants and their families. Shi Chen and Jiang-zhi Chen certify that each had a “first author” role equally. Qian Zhan and Cheng-hong Peng also contributed equally, and both should be considered as co-corresponding author. The authors thank Cheng-hui Ma and Zhi-hong Han for their surgery image.
Disclosure
Shi Chen, Jiang-zhi Chen, Qian Zhan, Xia-xing Deng, Bai-yong Shen, Cheng-hong Peng, and Hong-wei Li declares no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Drs Shi Chen and Jiang-zhi Chen contributed equally to this work, and both should be considered first author. Qian Zhan and Cheng-hong Peng also contributed equally, and both should be considered as co-corresponding author.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Chen, S., Chen, JZ., Zhan, Q. et al. Robot-assisted laparoscopic versus open pancreaticoduodenectomy: a prospective, matched, mid-term follow-up study. Surg Endosc 29, 3698–3711 (2015). https://doi.org/10.1007/s00464-015-4140-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4140-y