
Abstract
Background
The most important long-term complications after inguinal hernia repair are chronic pain and recurrence. Previous follow-up studies showed that physical examination is the only reliable method of follow-up to detect recurrences. However, physical examination is laborious and time consuming. We designed a telephone questionnaire as a method of follow-up after laparoscopic inguinal hernia surgery; the PINQ-PHONE (Post-INguinal-repair-Questionnaire by telePHONE). The aim of this study is to validate the PINQ-PHONE for detecting both asymptomatic and symptomatic recurrences.
Methods
This prospective study contained 300 randomly selected patients after laparoscopic inguinal hernia repair. All patients were contacted by telephone and the PINQ-PHONE was carried out. The PINQ-PHONE contains four elements; three questions and a do-it-yourself Valsalva maneuvre. Subsequently, all patients were seen in clinic and physical examination (gold standard) was done.
Results
The majority (96 %) was male and the mean age was 66 (range 26–93) years old. The mean interval between surgery and study inclusion was 58 (range 6–141) months. In five (1.7 %) patients, a recurrence was found. All of them replied positively to one or more elements of the PINQ-PHONE. Two-hundred-fifty-two (84 %) patients replied negatively to all elements and none of them had a recurrence. The overall sensitivity was 1.00 and the overall specificity was 0.86.
Conclusion
This study validated the PINQ-PHONE. It is a reliable, practical, and simple method of follow-up after laparoscopic inguinal hernia repair to detect both symptomatic and asymptomatic recurrences.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Inguinal hernia repair is one of the most common performed operation by a general surgeon. Annually over 20 million groin hernias are repaired worldwide accounting for 10–15 % of all general surgical procedures [1, 2]. The main long-term complications after inguinal hernia repair are recurrences and chronic pain. Recurrence rates have diminished significantly since the introduction of the tension free mesh, popularized by Lichtenstein, and vary from 0 to 4 % now [3–7]. With the decrease of the recurrence rate, focus shifted to what was previously perceived as a “secondary” outcome; chronic pain. Incidences of chronic pain reported are high and a systematic review shows that 11 % of the patients deal with chronic pain after mesh repair [8].
The outcomes of conventional anterior mesh repair are now compared to the outcomes of newer techniques with a posterior approach to the abdominal wall, such as laparoscopic repairs. Numerous new hernia meshes and mesh fixation products are continuously introduced by the medical industry and they all suggest to be beneficial to reduce recurrences and chronic pain. Providing best medical care to their patients, for surgeons it is of great importance, to critically appraise and receive feedback on outcomes of new techniques or materials. Adequate, reliable follow-up is, therefore, essential.
Pain is a subjective outcome and can be assessed by questioning, while a recurrence is an objective outcome. Until now, the gold standard for follow-up and monitoring recurrences after inguinal hernia repair is physical examination. Patients are routinely scheduled for clinical visits, even when patients lack of symptoms or signs of a recurrence. Clinical follow-up is time consuming and a laborious job to the physician and patient. Moreover, it is unlikely for patients to visit clinic when symptoms are absent. It is commonly expected in daily practice that patients will return to clinic when symptoms emerge and are, therefore, not routinely scheduled for follow-up. In such daily practice, the surgeon relates the outcomes of a specific surgery to the number of patients that visit clinic with symptoms. All patients that have presented with their symptoms to another physician’s office, patients with an asymptomatic recurrence, or patients who have not presented yet, remain unnoticed. An underestimation of the real outcomes of a specific inguinal hernia repair remains.
Surgeons have dealt with this problem by designing new methods of less time-consuming and reliable follow-up. Some have reported written questionnaire as a method of follow-up. However, none have showed any reliability, with low sensitivity and specificity, resulting in high false-positive rates and asymptomatic recurrences remaining undetected [9–11]. Subsequently, the written questionnaire was declined as a valid method of follow-up after open inguinal hernia repair.
In search of a simple, practical, reliable, and contemporary method of follow-up after laparoscopic inguinal hernia repair to monitor recurrences, less time consuming than physical examination, we designed a telephone questionnaire to detect both asymptomatic and symptomatic recurrences. The telephone is an ideal medium for follow-up since direct feedback can be given by the patient and physician, and everybody is reachable with the wide implementation and use of mobile phones. We conducted a prospective study to validate our Post-INguinal-repair-Questionnaire by telePHONE, the PINQ-PHONE.
Methods
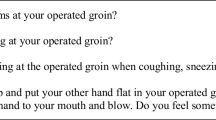
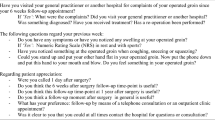
This prospective study included 300 patients who were randomly selected from the database of all patients that were operated for an inguinal hernia between 2001 and 2012. This database includes more than 2500 patients who underwent laparoscopic inguinal hernia repair at the Slotervaart Hospital since its introduction in 1993. We chose a recent timeslot to limit loss of follow-up. Every patient in the database is numbered. Every alternating year even or odd patient numbers were selected. Altogether, 324 patients were reached by telephone before 300 patients consented to participate. All patients were operated or supervised by two expert surgeons and underwent either TEP or TAPP repair. Both surgeons have repaired over 2000 inguinal hernias laparoscopicly. Inclusion criteria were age more than 18 and a laparoscopic inguinal hernia repair at the Slotervaart Hospital between 2001 and 2012. All operations were done in a routine manner, with a preperitoneal positioned polypropylene mesh. Exclusion criteria were reported insufficient understanding of the Dutch language, reported mental disorder or inability to do a physical examination by oneself. A telephone questionnaire was developed to assess the presence of a recurrence after inguinal hernia repair. This Post-INguinal hernia repair-Questionnaire by PHONE (PINQ-PHONE) contains four elements; three questions about the patient’s operated groin, and one element includes the instructions of a physical examination done by the patients themselves. Patients are instructed to do a Valsalva maneuvre at their operated groin (Table 1).
After registration and approval by the local ethics committee patients were contacted by phone. Trial information and informed consent forms were sent by mail to patients’ home addresses. After obtaining returned written informed consent forms, patients were phoned again. The PINQ-PHONE was carried out. Outcomes of the telephone questionnaire were registered and saved in a database. Subsequently patients were scheduled for a clinical visit. The interval between the PINQ-PHONE and the clinical visit was no more than 2 weeks. The same questions were asked in clinic and a physical examination was done by one of two researchers. Both researchers were independent, not involved by the initial treatment, nor responsible for the health care-related consequences of the outcomes. A recurrence was defined as a clinical detectable bulge in the operated groin, protruding during straining observed by the researcher and confirmed by an expert clinician. In case of doubt an ultrasound was made in addition. An asymptomatic recurrence was defined as a recurrence in a patient who responded negatively to the first question. Outcomes were registered and saved in the same database.
The primary outcome was detection of a recurrence. Details of the operation technique, type and side of the hernia were obtained from the patients’ files.
Statistical analyses
The sample size was calculated based on recurrence percentages reported in the literature and our own experience, and estimated to be 3.5 %. We aimed to calculate the specificity, but especially the sensitivity with a certain reliability, and we, therefore, needed a minimum of 10 patients with a recurrence. The sample size accordingly is 10/3.5 * 100 = 286 participants. Considering the risk of some loss, we invited 300 patients. The sensitivity and specificity of the PINQ-PHONE as a diagnostic tool were calculated by comparing its outcomes with the outcomes of the gold standard; clinical examination with addition to an ultrasound in case of doubt. The 95 % confidence intervals were calculated. For all statistical procedures, a probability value (p value) <0.05 was considered to be statistically significant. The test–retest reliability of the PINQ-PHONE is tested using the Kappa-value, comparing the answers of the PINQ-PHONE to the answers of the questionnaire at clinic. Analysis of data was performed in SPSS version 20 and the program Confidence Interval Analysis.
Results
Three hundred patients were randomly selected and included between October 2011 and April 2013. The majority of the patients had a unilateral repair done, and in case of a bilateral repair, one side was randomly selected to be included for analysis. The mean time for executing the PINQ-PHONE was 3–4 min. The majority (96 %) was male and the mean age was 66 (range 26–93) years old. The mean interval between surgery and study inclusion was 58 (range 6–141) months. Ninety-two percent of the patients underwent TAPP repair and 8 % TEP repair. The affected side was in 52 % of the patients the right side and in 48 % of the patients the left side. Fifty-six percent of the patients had an indirect hernia, 37 % a direct hernia, 5 % a pantaloon hernia, and 1 % had a femoral hernia. Clinically, in none of the patients an ultrasound was indicated. Altogether, in five (1.7 %) patients, a recurrence was found at physical examination during clinical visit. None of these patients had consulted a physician yet.
The first question concerned the presence of symptoms in the operated groin. Thirty-nine patients had some kind of symptoms in their operated groin, such as pain, discomfort or the sensation of “something in the way,” of which three patients had indeed a recurrence. Two-hundred-sixty-one patients did not have any symptoms, of which two patients had a recurrence. The sensitivity of question 1 was 0.60 and the specificity was 0.88 (Table 2).
The second question referred to whether the patient had noticed anything in the operated groin. Seven patients had noticed something, of which four patients had a recurrence during clinical physical examination. Two-hundred-ninety-three patients had not noticed anything at the operated groin, of which one patient had a recurrence. The sensitivity of question two was 0.80 and the specificity was 0.99 (Table 3).
The third question related to whether the patient had noticed anything in the operated groin during moments of increased abdominal pressure, such as sneezing, coughing, or squeezing. Eleven patients noticed something in the operated groin during increased abdominal pressure, of which four had a recurrence at clinical physical examination. Two-hundred-eighty-nine patients noticed nothing during increased abdominal pressure, of which one patient had a recurrence. The sensitivity of question three was 0.80 and the specificity was 0.98 (Table 4).
The fourth element of the PINQ-PHONE contained the instructions of the do-it-yourself Valsalva maneuvre. Patients were asked whether they noticed anything at the groin during the Valsalva maneuvre. Four patients felt something in the operated groin, of which three patients had a recurrence during clinical physical examination. Two-hundred-ninety-six patients did not notice anything during the do-it-yourself Valsalva maneuvre, of which two patients did have a clinical recurrence. The sensitivity of element four was 0.60 and the specificity was 1.00 (Table 5).
Altogether, in five (1.7 %) patients, a recurrence was found at clinical examination. Table 6 shows the results of all five patients with a recurrence and accordingly the outcomes of the PINQ-PHONE. Three out of five patients were symptomatic and had symptoms such as pain, swelling, or the sensation of “something.” Two patients were asymptomatic and responded negatively to the first question. None of the patients had consulted a physician.
Only patient number three had symptoms of feeling “something,” but he had not noticed anything physically. This 74-year-old patient was re-contacted and had forgotten that he had participated. His wife revealed that her husband appeared to suffer from progressive dementia. In retrospect, this patient should have not been included in the first place, but at the time of inclusion dementia was not diagnosed yet.
Overall, 252 (84 %) patients answered “NO” to all questions. None of these patients were diagnosed with a recurrence (Table 7). Forty-eight patients answered “YES” to some or more questions, of which five patients were diagnosed with a recurrence. The overall sensitivity was 1.00 (CI 0.57–1.00) and specificity was 0.85 (CI 0.81–0.89). The positive predictive value was 0.10 (CI 0.05–0.22) and the negative predictive value was 1.00 (0.99–1.00).
The test–retest reliability of our PINQ-PHONE is tested using the Kappa-value, comparing the answers of the PINQ-PHONE with the answers of the questionnaire in clinic. The Kappa-value was 1.000 (CI 1.00–1.00).
Discussion
In our hernia practice, containing more than 2,500 patients, we were searching for a reliable, simple, and practical method of follow-up after laparoscopic inguinal hernia repair to detect both symptomatic and asymptomatic recurrences. We developed a telephone questionnaire, the PINQ-PHONE, including four elements; three questions and the instructions of a physical examination by means of a do-it-yourself Valsalva maneuvre. The purpose of this study was to validate the PINQ-PHONE for detecting symptomatic and asymptomatic recurrences.
The overall sensitivity of the PINQ-PHONE was 1.00, meaning that all recurrences, either symptomatic or asymptomatic, were detected by the PINQ-PHONE. None of the patients that replied negatively to all elements of the PINQ-PHONE had a recurrence. This is an excellent outcome, validating our PINQ-PHONE and showing 100 % reliability in excluding a recurrence when replied negatively to all elements of the PINQ-PHONE.
The Kappa-value of PINQ-PHONE was 1.00. Patients showed absolute consistency giving the exact same answers on the phone as they do in clinic, resulting in a 100 % agreement. This implies that the questions of the PINQ-PHONE are simple, and the answers are likely to be reliable. We introduced a do-it-yourself Valsalva maneuvre. Patients appeared to be capable of following instructions and recognizing a bulge in their groin during Valsalva as the majority of the patients with a recurrence scored positive for this element. Altogether, it took the physician approximately 3–4 min to carry out the PINQ-PHONE, demonstrating that PINQ-PHONE is a time-saving and practical method of follow-up after inguinal hernia repair.
Not all recurrences were symptomatic. Three (60 %) patients had a swelling, pain or the sensation of “something,” and two (40 %) patients were asymptomatic. None of the patients with a recurrence had consulted a physician yet. When patients are not followed in a routine manner after inguinal hernia surgery, and patients are expected to report themselves when symptoms are present, our study shows that 40 % of the recurrences will be missed, because they are asymptomatic. For physicians to gain reliable feedback of the outcomes of their inguinal hernia surgery, it is of the great importance to detect asymptomatic recurrences as well. Until now, this could only have been obtained by examining all patients in clinic.
The outcomes of the PINQ-PHONE imply that when a patient responds negatively to all elements of the PINQ-PHONE, the physician can be almost 100 % sure that the patient has no recurrence, either symptomatic or asymptomatic. If the patient responds positively to one of the elements of the PINQ-PHONE a recurrence cannot be excluded. These patients should be invited for a clinical assessment. In our series, 48 patients responded positively to one of the elements, of which 5 patients had a recurrence and 43 patients had not. This implies that 14 % of the patients will be invited to clinic to exclude a recurrence and 2 % will be invited to confirm a recurrence
This outcome has a tremendous impact on the daily practice of a laparoscopic hernia surgeon. Follow-up after laparoscopic inguinal hernia repair can now firstly be carried out by the PINQ-PHONE and if scored positively to one of the elements, subsequently at clinic. By implementing this method, 84 % of the patients can refrain from visiting clinic, saving large amounts of time to the physician and also to the patient. None of the recurrences will be missed, all of them will be detected.
We have the impression, since the questions are simple and the kappa-value is 1.00, this method can be easily taught to others. In our practice, we will train a dedicated nurse or physician assistant to carry out the PINQ-PHONE at all our patients annually after inguinal hernia surgery as method of follow-up.
Incidence of chronic pain is not detected by this questionnaire. There are several diagnostic methods and classification systems to evaluate chronic pain. We hope to implement the evaluation of chronic pain in the PINQ-PHONE in the future as soon as a universal accepted method and classification system is clarified. It should also be emphasized that this study included laparoscopic inguinal hernia repairs only. Future research needs the reveal whether the PINQ-PHONE shows the same results in follow-up after open inguinal hernia repair. Due to scar tissue in the groin, results from the laparoscopic group cannot be blindly extrapolated to the open group. Also, this questionnaire was executed in Dutch, and therefore, validated only in Dutch language. Future validation of the PINQ-PHONE in other languages needs to be undertaken.
Patients that have to be excluded from this method of follow-up are patients with physical disability that is not able to carry out a physical examination by themselves, patients who are deaf, patients with a language barrier, or patients with a mental or cognitive disorder such as dementia. During the first clinical visit, the physician should evaluate and document whether the patients are capable of doing self-examination.
In our series of 300 patients, we found a recurrence rate of 1.7 %. We estimated the recurrence rate to be 3.5 % and used this number in our sample size calculations. Since the actual recurrence rate appeared to be lower than expected, the confidence intervals of the sensitivity are broader.
Conclusion
The PINQ-PHONE is a validated method of follow-up after laparoscopic inguinal hernia repair. It is reliable, simple, and practical. This method is less time consuming compared to physical examination and widely applicable, since everybody is reachable with the wide use of mobile phones. All recurrences, either symptomatic or asymptomatic can now be reliably detected. If a patients replies negatively for all elements of the PINQ-PHONE, a recurrence can be excluded with certainty. This simple method provides surgeons all over the world with a tool to reliably appraise outcomes of laparoscopic inguinal hernia repair. Future employment of the PINQ-PHONE will establish its role in evaluating outcomes after open inguinal hernia repair and its role in the evaluation of chronic pain.
References
Kingsnorth A, LeBlanc K (2003) Hernias: inguinal and incisional. Lancet 362:1561–1571
Rutkow IM (2003) Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin North Am 83:1045–1051
Lichtenstein IL (1987) Herniorrhaphy. A personal experience with 6,321 cases. Am J Surg 153:553–559
Leibl BJ, Jäger C, Kraft B et al (2005) Laparoscopic hernia repair–TAPP or/and TEP? Langenbecks Arch Surg 390:77–82
Langeveld HR, van’t Riet M, Weidema WF et al (2010) Total extraperitoneal inguinal hernia repair compared with Lichtenstein (the LEVEL-Trial): a randomized controlled trial. Ann Surg 251:819–824
Tamme C, Scheidbach H, Hampe C et al (2003) Totally extraperitoneal endoscopic inguinal hernia repair (TEP). Surg Endosc 17:190–195
Felix E, Scott S, Crafton B et al (1998) Causes of recurrence after laparoscopic hernioplasty. A multicenter study. Surg Endosc 12:226–231
Nienhuijs S, Staal E, Strobbe L et al (2007) Chronic pain after mesh repair of inguinal hernia: a systematic review. Am J Surg 194:394–400
López-Cano M, Vilallonga R, Sánchez JL et al (2007) Short postal questionnaire and selective clinical examination combined with repeat mailing and telephone reminders as a method of follow-up in hernia surgery. Hernia 11:397–402
Vos PM, Simons MP, Luitse JS et al (1998) Follow-up after inguinal hernia repair. Questionnaire compared with physical examination: a prospective study in 299 patients. Eur J Surg 164:533–536
Haapaniemi S, Nilsson E (2002) Recurrence and pain three years after groin hernia repair. Validation of postal questionnaire and selective physical examination as a method of follow-up. Eur J Surg 168:22–28
Disclosures
Baukje van den Heuvel, J.A. van Jarwaarde, P. Wichers, E.S.M. de Lange de Klerk, H.J. Bonjer, and B.J. Dwars, have no conflicts of interest or financial ties to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
van den Heuvel, B., van Jarwaarde, J.A., Wichers, P. et al. Follow-up after laparoscopic inguinal hernia repair, can it be done by phone? A prospective study in 300 patients, the PINQ-PHONE. Surg Endosc 29, 3292–3297 (2015). https://doi.org/10.1007/s00464-015-4080-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-015-4080-6