
Abstract
The aim of this study was to determine if bolus and dry swallow showed similar pressure changes in the oropharynx using our newly developed device. A unique character of it includes that baropressure can be measured with the sensor being placed in the balloon and can assess the swallowing mechanics in terms of pressure changes in the oropharynx with less influences of direct contacts of boluses and oropharyngeal structures during swallow indirectly. Fifteen healthy subjects swallowed saliva (dry), 15 ml of water, 45 ml of water, and 15 ml of two different types of food in terms of viscosity (potage soup-type and mayonnaise-type foods). Suprahyoid muscle activity was recorded simultaneously. Three parameters, area under the curve (AUC), peak amplitude, and duration of pressure, were analyzed from each swallow. Almost all of the bolus swallowing events had biphasic baropressure responses consisting of an early phase and late phase (99%), whereas 90% of the saliva swallowing events had a single phase. AUC, peak, and duration displayed greater effects during the late phase than during the early phase. Baropressure of the early phase, but not of the late phase, significantly increased with increasing volume; however, small but significant viscosity effects on pressure were seen during both phases. Peak pressure of the late phase was preceded by maximum muscle activity, whereas that of the early phase was seen when muscle activity displayed a peak response. These findings indicated that our device with the ability to measure baropressure has the potential to provide additional parameter to assess the swallow physiology, and biphasic baropressure responses in the early and late phases could reflect functional aspects of the swallowing reflexes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
During the past three decades, there has been an abundance of studies investigating the physiology and biomechanics of swallowing [1, 2]. There is no doubt that advancements in technology to assess the motor function of the pharynx have provided significant information underlying the basis for swallowing [3]. Several methodologies, such as electromyography [4], intrapharyngeal impedance [5], pressure in the oropharyngeal and esophageal regions [6], and imaging of the oropharyngeal movement using videofluoroscopy [7, 8] and manofluorography [9], have been used to assess the function of swallowing. Although pharyngeal motor function during swallowing has been extensively investigated using these methods, widely obtained data vary among studies. It is commonly known that pharyngeal pressure reflects the pharyngeal contraction indirectly linked to swallowing [6, 8] and that measurement of its pressure is critical for determining the extent to which the highly coordinated and complex action of the pharyngeal stage of swallowing is reflexive. Several methods have been developed to examine pharyngeal pressure, such as conventional manometry [4, 10,11,12] and high-resolution manometry [3, 8, 13]. These technologies, especially high-resolution manometry, have provided substantial information demonstrating the transient process of swallowing in relation to the temporal and spatial aspects of pressure change [3, 8, 13]. Measurements of pharyngeal pressure with traditional manometric devices include several factors that might confound data interpretation, such as changes in pressure due to the influences of direct contact pressure of boluses and surrounding tissues with the transducer [14]. Furthermore, inconsistent results in terms of the effects of viscosity and/or volume of boluses on pressure changes in the pharynx could be attributed, in part, to the effects of direct contact with sensors in the manometer [6, 10, 15, 16]. These findings might raise interesting questions regarding results obtained using traditional manopressure and other factors (aside from baropressure) that affect pressure measurements in the pharynx.
Recently, we developed a new device to gain a better understanding of the change in pressure during swallowing by using transducers placed in a silicon balloon to eliminate the influences of bolus contact. This system allows another evaluation of the changes indicated by baropressure, and suggests that our analysis of oropharyngeal pressure should provide additional information regarding swallow mechanisms compared to other sensors. Besides, assessment of pressure changes during swallow in the presence and absence of boluses provide us possible mechanisms regarding the swallow physiology. In this study, we evaluated the pressure changes in the pharynx during several different types of swallowing tasks in healthy human subjects and clarified their validity for assessing swallowing.
Materials and Methods
Volunteers
Studies were performed using 15 healthy volunteers aged 21–50 years who were asymptomatic for oropharyngeal diseases (13 males and 2 females). The experimental protocol was approved by the Ethics Committee of Niigata University Faculty of Dentistry. All participants provided written informed consent prior to enrollment.
Intrapharyngeal Pressure
Research participants were seated comfortably in a chair and were unable to observe barometric tracing on the monitor. A pressure sensor (Miniature SPI Digital barometer; Freescale Semiconductor, Inc., Austin, TX, USA) placed at the tip of a guide catheter was placed in the cavity of the oropharynx via the left nasal cavity. In this study we focus on changes in baropressure in the oropharynx, since assessment of pressure changes reflects the swallow mechanics coordinated by several structures such as tongue, soft palate, and pharyngeal wall between oral and pharyngeal stages [3]. The location of the tip of the sensor was visually confirmed through the oral cavity. The transducer (1.5 × 3 × 5 mm) was placed in a balloon made of thin silicon (diameter <4 mm) to minimize the influences of direct contact with various boluses that subjects swallowed, the tongue base, and the pharyngeal wall; the outer surface of the balloon acted as the pressure-sensing portion that transmitted pressure to the transducer. No air leakage from the balloon was confirmed by the surgical microscope just before data acquisition. The characteristic of this sensor is described in our recent report [17].
The catheter was taped to the nose to eliminate unexpected movement of the transducer; the average distance between the nose and sensors in the pharynx was 13.5 ± 0.2 cm. To evaluate the accuracy of measurements using the pressure transducer in the balloon, baropressure calculated from transducer output was compared with the pressure measured using a transducer without a balloon prior to each test. Signals were amplified with a custom-made amplifier, connected to an A/D converter, and fed into a computer equipped with a CED Power 1401 board and analysis software (Spike 2; Cambridge Electronics Design Ltd., Cambridge, UK). Data were obtained with a resolution of 0.15 kPa and sampling frequency of 3 ms. Preliminary experiments revealed that movements of this device did not induce any baropressure changes (Data not shown).
Suprahyoid Muscle Activity
Bipolar surface EMG electrodes were placed on the skin bilaterally over the digastric muscles to record activity of the suprahyoid muscle simultaneously during swallowing [18] (Fig. 1A). Signals were sampled at 1 kHz, amplified (×1000), displayed by the custom-made amplifier, connected to an A/D converter, and fed into a computer equipped with a CED Power 1401 board and analysis software (Spike 2; Cambridge Electronics Design Ltd.).

Experimental set-up (A) and design (B). A baropressure sensor (barometer, a) in a balloon was placed in the oropharynx via the nasal cavity (b) and activity of the suprahyoid muscle was recorded during swallowing tasks (c). Overview of experimental set-up is shown in (d)
Experimental Design
The experimental design is shown in Fig. 1B. After 5 min of accommodation, subjects participated in a series involving dry swallowing (i.e., swallowing saliva) under resting conditions and bolus swallowing of 15 ml of water, 45 ml of water, 15 ml of potage soup-type (pota) food, and 15 ml of mayonnaise-type (mayo) food (commercially available; Tsururinko, Morinaga, Japan). For the dry swallow task, subjects were asked to swallow their own saliva. Subjects were instructed to hold each bolus on the dorsum of the tongue for 2 s before swallowing each bolus, and were directed to swallow each bolus at once. When each bolus was divided into more than twice to swallow, multiple waveforms for baropressure responses and EMG activity at the suprahyoid muscles were detected. In such a case, results were not included for analysis. This protocol that seems to be less typical range of normal ingestive behavior was employed to control the experimental condition with less variability. The interval between each swallow was set at 3 min. Pota and mayo were diluted with water, and the characteristics of both testing solutions appeared to be liquid-like; however, the consistency of mayo was much thicker than that of pota. Pota and mayo can be categorized as moderately thick and liquidized and extremely thick, respectively. The series was repeated three times for each subject. The average of results based on three trials was represented as the data of each individual. Before and after testing, the position of the sensor was verified by a laryngoscope. As far as we checked the location of it before and after each experiment through oral cavity, the sensor appeared to be placed in the same area in the oropharynx.
Data Analyses
The peak value of the wave (kilopascal [kPa]), duration (s), and area under curve (AUC; kPa s) were analyzed using the pressure waveform of each recording (Fig. 2). Peak pressure was defined as the highest pressure reading of the sensors during swallowing. Measurements of the duration of barometric waveforms were determined by calculating the time between the onset and the offset of pressure generation with values more than the average ± 2SD from the baseline. The baseline refers to the average baropressure calculated by the value during resting conditions for 3 min prior to swallowing tasks. As shown in Fig. 2, two wave phases were observed during bolus swallowing, and results were analyzed separately between T0 (the starting point of the early phase) and T1 (the end of the early phase) and between T1 (the starting point of the late phase) and T2 (the end of the late phase). P1 and P2 refer to the points when the maximum amplitude of the pressure was shown (Fig. 2). In addition, we analyzed small but significant negative pressure that was induced consistently by dry and bolus swallows (T2 and T3). T2 and T3 refer to the end of the late phase and the negative phase, respectively. EMG activity of the suprahyoid muscle was rectified and stored for offline analyses and was quantified as the AUC (µV s). The onset and offset of EMG activity evoked by swallowing were defined as the first and last time points that exceeded the average baseline amplitude of EMG + 2SD, respectively. The duration of muscle activity was determined by calculating the time between the onset and the offset of muscle activity with values more than the average + 2SD from the baseline. The point when the largest EMG amplitude response occurred during swallowing was referred to as the peak response (M0). We analyzed the interval between the two points that corresponded to the muscle activity and pressure of the early and late phases that reached the peak level to assess the temporal relationships between muscle activity and intrapharyngeal pressure. The intervals between the onset of muscle and pressure changes were also analyzed for dry swallow and 15 ml of water swallow. The effects of each test solution on pressure and EMG were analyzed statistically with the paired t test, repeated-measures ANOVA, and post hoc comparisons (Bonferroni test, SPSS version 22; IBM, Armonk, NY, USA) as necessary. Data were expressed as average ± SEM. Statistical significance was set at P < 0.05.

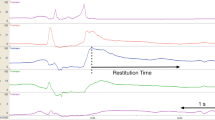
Simultaneous recordings of suprahyoid muscle activity (upper panel) and pharyngeal pressure waveform (lower panel) induced by swallowing saliva (dry swallow) and 15 ml of water. Three parameters, area under curve (AUC), peak pressure (peak value), and duration, were analyzed on the raw waveform. P1 and P2 display the peak response points of baropressure. T0, T1, and T2 indicate the onset of the baropressure responses during the early, late, and negative phases, respectively. T3 is the return of the pressure wave to baseline. The durations between T0 and T1 and between T1 and T2 represent the early phase and late phase, respectively.
Results
Early and Late Phases
Positive pressure generation was observed during all instances of swallowing (Fig. 2a, lower panel). Two sequential waveforms of positive pressure were called the early phase and late phase. The former showed shorter durations and smaller amplitudes compared to the late phase, and both phases were connected at the point of inflection (T1; Fig. 2b). Bolus swallowing displayed a greater occurrence of the early phase (4/45; 8.9%) compared to dry swallowing (179/180; 99.4%; Chi square = 7.9; P < 0.01). Negative pressure with a small amplitude and short duration was observed at the termination of positive pressure, just before the pressure returned to the pre-swallowing levels (Fig. 2b); 33/45 (73.3%) and 159/225 (85.3%) trials displayed negative pressure with dry swallowing and bolus swallowing. Swallowing tasks showed substantial increases in activity of the suprahyoid muscles (Fig. 2a, upper panel).
Pharyngeal Pressure
First, we tested the reproducibility of baropressure generation during three trials for each individual. The AUC, peak pressure, and response duration showed similar values between trials during the early phase (P > 0.05) and late phase (P > 0.05) for dry swallow and water swallow (Data not shown). Consequently, the average of the data obtained from three trials represented the result of each subject. Second, we determined the volume effects on pressure changes while swallowing water (Fig. 3). Swallowing 15 and 45 ml of water displayed biphasic positive pressure responses consisting of the early phase and late phase. The pressure responses during the late phase had significantly greater AUC (P < 0.001), peak value (P < 0.001), and duration (P < 0.001) values compared to those during the early phase (Fig. 3). Figure 3 demonstrates that 45 ml of water increased the AUC, peak pressure, and duration compared to 15 ml of water during the early phase (P < 0.01), with less effect found during the late phase (P < 0.15). Muscle activity indicated by the AUC was greater with 45 ml of water than with 15 ml water (P < 0.001), with no effect on duration (data not shown). Third, we determined the effects of different types of boluses in terms of viscosity on baropressure with water, pota, and mayo swallows (Fig. 4). During the early phase, mayo resulted in significant increases in peak value (P < 0.05) compared to 15 ml of water (Fig. 4, left column), with no effects on response duration (P > 0.82; Fig. 4). Although viscosity had no effect on the AUC during the late phase (P > 0.52; Fig. 4), right column), mayo resulted in greater and shorter responses in the peak value (P < 0.05) and duration (P < 0.001), respectively, compared to 15 ml of water. Different types of boluses had fewer effects on suprahyoid muscle activity indicated by the AUC (P > 0.49; data not shown). Finally, we determined the AUC of negative pressure induced at the end of the baropressure changes with dry and bolus swallows. The AUC appeared to be similar for the five tasks (dry, −0.56 ± 0.15; 15 ml of water, −0.77 ± 0.19; 45 ml of water, −0.93 ± 0.02; pota, −0.77 ± 0.16; mayo, −0.75 ± 0.16 kPa s; P > 0.05). Negative pressure duration showed similar values for the five tasks (0.06–0.08 s; P > 0.05).

Effect of water volume on three parameters, AUC, peak value, and response duration, for baropressure in the oropharynx indicated during the early and late phases. **P < 0.01. † P < 0.001 versus early phase

Effect of the viscosity on three parameters, AUC, peak value, and response duration, for baropressure in the pharynx indicated in the early and late phases. *P < 0.05 versus 15 ml of water. †P < 0.001 versus early phase
Baropressure and Muscle Activity
We compared the temporal relationships between suprahyoid muscle activity (Fig. 5a, upper panel) and peak pressure (Fig. 5a, lower panel) when both reached maximum responses during bolus swallowing. Peak pressure during the early phase (P1) was seen when muscle activity reached the peak level, except with 45 ml of water (Fig. 5b). However, peak pressure during the late phase (P2) was preceded by muscle activity that reached the peak level (Fig. 5c). We also analyzed the temporal relationship of the timing of the onset of muscle activity and baropressure for 15 ml of water and saliva swallowing. Consequently, the onset of the early phase with 15 ml of water and dry swallow appeared to be delayed by 0.51 ± 0.05 and 0.24 ± 0.02 s, respectively, compared to that of muscle activity, indicating that the onset of baropressure increases after the onset of suprahyoid muscle activity during swallowing.

The temporal relationship between time points of baropressure for each phase and the suprahyoid muscle activity that displayed maximum levels. The time course effect of the muscle activity and baropressure were recorded simultaneously in the oropharynx during swallowing of 15 ml of water. Peak response for muscle activity (M0) was set to 0 s, whereas P1 and P2 indicated the intrapharyngeal pressure responses with the maximum amplitude in the waveform. The average time lag was calculated between the peak muscle activity (M0) and peak pressure values (P1, P2) during the early phase (B) and late phase (C). *P < 0.05 versus 15 ml of water. N.S., no significant difference
Dry and Bolus Swallowing
As shown in Fig. 2a, we observed significant increases in baropressure with the dry swallow; the waveform seemed to be similar to that of the late phase induced by a bolus swallow (Fig. 2a). We compared the characteristics of baropressure induced by the dry swallow compared to that induced by 15 ml of water. Results revealed that the AUC for the late phase for 15 ml of water (3.7 ± 0.4 kPa s) was similar to that for saliva (3.4 ± 0.3 kPa s) (P > 0.15). The interval relative to the time point of maximum suprahyoid muscle activity was 0.26 ± 0.02 s for dry swallow, which was significantly greater than that seen during the late phase for 15 ml of water (0.19 ± 0.01 s; P < 0.003). The AUC for negative pressure seen at the end of positive baropressure was −0.56 ± 0.15 kPa s for dry swallow and −0.77 ± 0.19 kPa s for 15 ml of water (P > 0.05).
Discussion
It is well documented that changes in pressure in the pharynx evoked by the approximation of the base of the tongue to the posterior pharyngeal wall appear to be the principal mechanism for propulsion of the bolus through the pharynx during swallowing [19, 20]. In this study, we used a small (2 × 3 × 5 mm) factory-calibrated absolute pressure sensor with high resolution for time (3 ms) and pressure (0.15 kPa) that was equipped with a thermometer for temperature compensation [17]. With the sensor uniquely placed in the silicon balloon, we were able to measure the baropressure changes; therefore, this tool provided information to better understanding of swallowing physiology.
Technical Considerations
The oropharynx was able to be strongly compressed by the surrounding soft tissues during swallowing. Baropressure provided mechanical stress to the sensing elements, and the mechanical distortion was able to be converted to an electrical signal. These baropressure measurements were performed in the pharynx during swallowing. However, one might consider that baropressure changes are contaminated by the effects of direct contact of foreign substances, such as saliva, soft tissues, and/or food, with the sensor. For example, when the sensing element is mechanically stimulated by soft materials, such as cotton or a feather, through the small hole (1 mm in diameter) of the sensor, the system creates loud, sharp, noisy electrical signals (data not shown). The output signal, however, shows features distinct from those of baropressure changes, as indicated by waveforms that are much smaller and much gentler in shape after swallowing. Consistent with these results, Ryu [14] showed that epiglottis tilt evoked a transient increase in pressure, followed by significant increases in pressure that should be relevant for “real” pressure changes during swallowing. These findings indicate that possible contamination of pressure during the recording due to direct contact with a foreign substance should be excluded for our device. However, when a sticky substance enters the hole of the sensor, the sensing elements might show irreversible changes on the sensor reading. We placed the sensor in a balloon to exclude this possibility. This allowed us to measure the baropressure in the oropharynx. These findings indicate that changes in baropressure during swallowing should be due to pressure changes generated after narrowing of the pharyngeal space by contraction of the pharyngeal wall, soft palate, and tongue base during swallowing. In this respect, Pascal’s law may allow some freedom regarding placing of the sensor (i.e., position and/or direction of the sensing hole).
We compared our results of the duration and peak amplitude for pharyngeal pressure reported by previous studies that used traditional manometric devices. Evidence revealed that the durations in those studies (410–450 ms) [21,22,23] appeared to be shorter than those in our study (580 ms). However, peak pressure in our study (~13 kPa) appeared to be less than that in several previous reports using traditional manometric devices (18–26 kPa) [15, 16, 21, 23, 24]. Comparisons of these parameters for pharyngeal pressure might be difficult due to the disparity of methodologies. Furthermore, consistent results produced by three trials for each individual indicated that our sensor has sufficient ability to collect data with high reproducibility.
Biphasic Feature of Baropressure
Interestingly, more than 99% of trials of bolus swallowing, but less than 9% of trials of dry swallowing, displayed a biphasic waveform. The waveform can be distinguished at the point of inflection, and both phases were called early phase and late phase, thus reflecting the pressure changes in the pharynx. These results indicated that the physiological basis underlying bolus swallowing could be different from that of dry swallowing. In accordance with our findings, previous studies demonstrated a biphasic waveform by conventional and high-resolution manometric procedures during bolus swallowing measured [6, 9, 10, 21, 25, 26]. Perlman [10] explained that the onset of the early phase and late phase refer to the driving pressure of the tongue and pharyngeal pressure, respectively. However, Raut [26] referred to two distinct phases as bolus and pharyngeal waves. Interestingly, Omari [5] demonstrated a biphasic response pattern using intraluminal impedance changes in the pharynx that seemed to be well-matched with the response pattern of pressure changes in the pharynx. These works clearly support the biphasic pressure changes in the oropharynx found in our study; however, they do not explain the functional roles of two phases of intrapharyngeal pressure during swallowing.
It is well documented that oral closure and naso-pharyngeal closure are required for swallow; the space should be isolated from the area outside the oropharynx to apply positive pressure to the sensor in the pharyngeal space. Thus, our results revealed that onset of the early phase induced by 15 ml water, which was induced approximately 0.5 s after the onset of suprahyoid muscle activity, might be induced soon after the onset of the oral phase of the swallowing process. In fact, using videofluorography, we previously reported that naso-pharyngeal closure was induced during the time between the onset of the oral phase and the pharyngeal phase [27], whereas the late phase reflected strong compression of the pharyngeal space for propelling food into the lower pharynx, as reported by Perlman [10]. Taniguchi [28] revealed the temporal relationships between suprahyoid muscle activity and tongue pressure against the hard palate during bolus swallow; consequently, they showed that the time points when muscle activity and tongue pressure displayed the maximum level appeared to be induced simultaneously. Our results showed that the peak of pressure during the early phase (P1) and muscle burst were seen at the nearly same time in all situations except with 45 ml of water (Fig. 5b). These findings lead to the possibility that the early phase could be induced, at least in part, by the driving force of the tongue to the palate at the maximum level. The time point of the peak pressure during the early phase with 45 ml of water (compared to other type’s boluses at a volume of 15 ml) relative to the time of the peak suprahyoid muscle activity level was significantly delayed. The volume of the bolus did not affect the intervals between peak pressure during the late phase and muscle activity. Previously, McConnel [25] indicated that dysphagia patients do not display two functional components of waveforms that might reflect the transmitted driving force and pharyngeal clearing force. This finding suggests that mechanisms underlying bolus propulsion in the pharynx indicated by induction of the biphasic feature of baropressure could be altered under pathological conditions. The determination of negative baropressure is another novelty of this study. Although Perlman [10] demonstrated similar findings with no interpretation, it is reasonable that negative pressure induced after positive baropressure could reflect the relaxation of the oral and pharyngeal muscles during swallowing.
Bolus volume and viscosity appeared to be critical factors for biomechanical events during swallowing. Ample evidence using traditional manometric devices quantified the contribution of the bolus volume to pharyngeal pressure [10, 16, 24, 29]; however, those results seemed to be different due to a variety of experimental conditions. Our results showed significant volume effects on intrapharyngeal pressure during the early, but not the late, phase. Perlman [10] demonstrated that the duration of the pressure, possibly related to the pharyngeal contraction stage, which could correspond with the late phase in our study was independent of bolus volume. A minor role of volume effects on baropressure during the late phase and negative phase supports the idea that pharyngeal contraction seems to be a highly stereotyped event during swallowing.
Interestingly, despite similar AUC values for 15 ml of water and 15 ml of mayo, the peak amplitude of pressure and duration for mayo were greater and shorter, respectively, than those for water during the late phase (Fig. 4). These findings indicate that swallowing a very viscous bolus uses quicker and more contractions of the pharyngeal muscle in comparison to swallowing water. Although the results showed a small but significant effect of peak amplitude and duration between treatments in terms of viscosity, minor effects of viscosity on muscle activity that could reflect the workload of the oropharyngeal structure had less influence on the baropressure in the oropharynx. Collectively, these findings with similar AUC values for mayo and water swallow suggest that swallowing can be coordinated by the functional balance between the duration and level of peak contraction to propel various types of boluses.
Conclusions
Our newly developed and uniquely designed device with the capability to measure baropressure allowed us to provide another physiological mechanism underlying swallowing reflexes with mono and biphasic response patterns of baropressure in the pharynx during swallowing.
References
Salassa JR, DeVault KR, McConnel FM. Proposed catheter standards for pharyngeal manofluorography (videomanometry). Dysphagia. 1998;13:105–10.
Pitts T. Airway protective mechanisms. Lung. 2014;192:27–31.
Kuo P, Holloway RH, Nguyen NQ. Current and future techniques in the evaluation of dysphagia. J Gastroenterol Hepatol. 2012;27:873–81.
Huckabee ML, Butler SG, Barclay M, Jit S. Submental surface electromyographic measurement and pharyngeal pressures during normal and effortful swallowing. Arch Phys Med Rehabil. 2005;86:2144–9.
Omari TI, Rommel N, Szczesniak MM, Fuentealba S, Dinning PG, Davidson GP, Cook IJ. Assessment of intraluminal impedance for the detection of pharyngeal bolus flow during swallowing in healthy adults. Am J Physiol Gastrointest Liver Physiol. 2006;290:G183–8.
Al-Toubi AK, Doeltgen SH, Daniels SK, Corey DM, Huckabee ML. Pharyngeal pressure differences between four types of swallowing in healthy participants. Physiol Behav. 2015;140:132–8.
Kendall KA, McKenzie S, Leonard RJ, Goncalves MI, Walker A. Timing of events in normal swallowing: a videofluoroscopic study. Dysphagia. 2000;15:74–83.
Yoon KJ, Park JH, Park JH, Jung IS. Videofluoroscopic and manometric evaluation of pharyngeal and upper esophageal sphincter function during swallowing. J Neurogastroenterol Motil. 2014;20:352–61.
Yano J, Aoyagi Y, Ono T, Hori K, Yamaguchi W, Fujiwara S, Kumakura I, Minagi S, Tsubahara A. Sequential coordination between lingual and pharyngeal pressures produced during dry swallowing. Biomed Res Int. 2014;2014:691352.
Perlman AL, Schultz JG, VanDaele DJ. Effects of age, gender, bolus volume, and bolus viscosity on oropharyngeal pressure during swallowing. J Appl Physiol. 1985;75(33–37):1993.
Gumbley F, Huckabee ML, Doeltgen SH, Witte U, Moran C. Effects of bolus volume on pharyngeal contact pressure during normal swallowing. Dysphagia. 2008;23:280–5.
Fox MR, Bredenoord AJ. Oesophageal high-resolution manometry: moving from research into clinical practice. Gut. 2008;57:405–23.
Kahrilas PJ, Sifrim D. High-resolution manometry and impedance-pH/manometry: valuable tools in clinical and investigational esophagology. Gastroenterology. 2008;135:756–69.
Ryu JS, Park DH, Kang JY. Application and interpretation of high-resolution manometry for pharyngeal dysphagia. J Neurogastroenterol Motil. 2015;21:283–7.
Castell JA, Dalton CB, Castell DO. Pharyngeal and upper esophageal sphincter manometry in humans. Am J Physiol. 1990;258:G173–8.
Butler SG, Stuart A, Castell D, Russell GB, Koch K, Kemp S. Effects of age, gender, bolus condition, viscosity, and volume on pharyngeal and upper esophageal sphincter pressure and temporal measurements during swallowing. J Speech Lang Hear Res. 2009;52:240–53.
Hiraki K, Yamada Y, Kurose M, Ofusa W, Sugiyama T, Ishida R. Application of a barometer for assessment of oral functions: donders space. J Oral Rehabil. 2017;44:65–72.
Otake M, Kurose M, Uchida Y, Hasegawa M, Yamada Y, Saito I, Yamamura K. The interactions between different tastes on initiation of reflex swallow elicited by electrical stimulation in humans. Odontology the Society of the Nippon Dental University, 2015.
Donner MW, Bosma JF, Robertson DL. Anatomy and physiology of the pharynx. Gastrointest Radiol. 1985;10:196–212.
Kahrilas PJ, Lin S, Logemann JA, Ergun GA, Facchini F. Deglutitive tongue action: volume accommodation and bolus propulsion. Gastroenterology. 1993;104:152–62.
Dodds WJ, Hogan WJ, Lydon SB, Stewart ET, Stef JJ, Arndorfer RC. Quantitation of pharyngeal motor function in normal human subjects. J Appl Physiol. 1975;39:692–6.
Cerenko D, McConnel FM, Jackson RT. Quantitative assessment of pharyngeal bolus driving forces. Otolaryngol Head Neck Surg. 1989;100:57–63.
Lin T, Xu G, Dou Z, Lan Y, Yu F, Jiang L. Effect of bolus volume on pharyngeal swallowing assessed by high-resolution manometry. Physiol Behav. 2014;128:46–51.
Omari TI, Dejaeger E, Tack J, Van Beckevoort D, Rommel N. Effect of bolus volume and viscosity on pharyngeal automated impedance manometry variables derived for broad dysphagia patients. Dysphagia. 2013;28:146–52.
McConnel FM. Analysis of pressure generation and bolus transit during pharyngeal swallowing. Laryngoscope. 1988;98:71–8.
Raut VV, McKee GJ, Johnston BT. Effect of bolus consistency on swallowing–does altering consistency help? Eur Arch Otorhinolaryngol. 2001;258:49–53.
Okada A, Honma M, Nomura S, Yamada Y. Oral behavior from food intake until terminal swallow. Physiol Behav. 2007;90:172–9.
Taniguchi H, Tsukada T, Ootaki S, Yamada Y, Inoue M. Correspondence between food consistency and suprahyoid muscle activity, tongue pressure, and bolus transit times during the oropharyngeal phase of swallowing. J Appl Physiol. 1985;105(791–799):2008.
Hiiemae KM, Palmer JB. Food transport and bolus formation during complete feeding sequences on foods of different initial consistency. Dysphagia. 1999;14:31–42.
Acknowledgements
This work was supported by JSPS KAKENHI [Grant Number JP15K11055]. We would like to thank Editage (www.editage.jp) for English language editing. We are grateful to Prof. Takahiro Ono (Niigata University) for their discussion and helpful comments.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Rights and permissions
About this article

Cite this article
Hasegawa, M., Kurose, M., Okamoto, K. et al. Differential Response Pattern of Oropharyngeal Pressure by Bolus and Dry Swallows. Dysphagia 33, 83–90 (2018). https://doi.org/10.1007/s00455-017-9836-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-017-9836-9