
Abstract
Purpose
Colon cancer survivors can experience several post-treatment consequences that include fatigue and often report severe psychological illnesses such as depression or anxiety. There is little published quantitative data on the quality of life and psychological well-being associated with the health of Tunisian colon cancer survivors.
Methods
A total of 60 recovering colon cancer patients underwent a structured interview, which included the Hospital Anxiety and Depression (HADS) scale, the Piper fatigue scale and the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30).
Results
Patients were 59.26 years old on average. The median length of remission was 33.3 months. Surgery was performed on all patients, followed by 96.7% adjuvant chemotherapy. 15.1% of study participants were in the severe category for the depression score and 10% were in this category for the anxiety score. Ninety-one percent reported pathological fatigue scores on the Piper scale. However, only 8.33% were experiencing severe fatigue. According to the QLQ-C30 assessment, the overall quality of life was slightly impaired with an overall average score of 79.54 ± 16.98. Anxiety, depression and fatigue negatively affect global health outcomes and all their dimensions.
Conclusion
Even in the recovery phase, colon cancer patients can see their quality of life deteriorate. It comes out of their psychological experience and their physical life. It is, therefore, crucial to provide greater attention to these patients for holistic and multi-disciplinary care.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colon cancer (CC) has become a major public health problem because of its high incidence. Over 1.9 million new cases were diagnosed in 2020 (Sung et al. 2021). In Tunisia, the incidence rates are predicted to continue increasing year on year. Fortunately, more innovative screening techniques have allowed for earlier disease detection and the development of better treatment options increased CC survival.
Therefore, the management of survivorship issues is of paramount importance, especially the specific psychological concerns of CC.
Depression and anxiety are the most common psychiatric disorders largely diagnosed. In addition, patients often report fatigue as a common long-term consequence of cancer (Berger et al. 2015). These symptoms affect the quality of life (QoL) adversely.
To the best of our knowledge, there is little published quantitative data on the quality of life and psychological well-being associated with the health of Tunisian CC survivors. The current study aims to address this problem and provides a baseline estimate of depression, anxiety and fatigue prevalence in CC patients, to identify the best predictors and their impact on QoL.
Materials and methods
The project was a cross-sectional study carried out at the Medical Oncology Department of Farhat Hached Hospital in Sousse, Tunisia, between January 2020 and January 2022. Sixty patients were enrolled.
Inclusion criteria were being a non-metastatic CC patient, hisologically confirmed, in recovery for at least 3 months prior to the interview. An informed consent was obtained from each participant. Exclusion criteria were having a history of another cancer, a disabling somatic or intellectual pathology hampering the data collection.
Eligible participants were interviewed alone by the same research assistant and the data were collected through a face-to-face interview or indirectly via a telephone call and file review forms which covered sociodemographic variables, histopathological findings, anatomoclinical features and therapeutic management of CC.
All patients were given the Hospital Anxiety and Depression Scale (HADS) which is a self-administered questionnaire that can detect minor psychiatric impairment validated in Arab populations (Malasi et al. 1991). A score of 0–7 is categorized as normal, a score of 8 to 10 suggests possible anxiety or depressive disorder and a score of 11 or above indicates probable anxiety or depressive disorder (Zigmond et al.1983).
The Arabic version of the Piper scale was used to assess cancer-related fatigue. It is a 22-item scale that measures 4 subscales: behaviour (6 items), affect (5 items), sensory (5 items) and cognition/mood (6 items). Each item has 11 response categories on a 0–10 metric with verbal descriptor sanchoring the endpoints. Each subscale is scored individually and then aggregated together for an overall score, with higher scores reflecting more fatigue (Gledhill et al. 2002). Translation to Arabic dialect and cross-cultural adaptation followed the recommendations of international guidelines (Koller et al. 2005).
The 30-item European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core30 (EORTC QLQ-C30) was used to assess the QoL. The scale was specifically developed and validated for use in Arabic version with cancer patients (Ben Dahhou 2011). Two items ask about overall QoL and overall health, and the remainder covers five functioning scales (physical, role, social, emotional, and cognitive functioning) and nine symptoms scales (fatigue, nausea and vomiting, pain, dyspnea, sleep disturbance, appetite loss, constipation, diarrhea, and financial impact). For the global score and functional scales, higher scores indicate a better response, while for the symptoms scales, higher scores mean a worse response (Aaronson et al.1993).
Analysis was conducted using SPSS software version 25.0. Chi-square test and Fisher’s exact probability test were used for the comparison of frequencies. Student’s t test, Mann–Whitney and Kruskal-Wallis tests were used to compare the mean scores taking the value of 5% as the significance level. The Spearman bivariate correlation was used to investigate the interconnection between the QoL and the psychological characteristics of the patients.
Results
Patients were 59.26 years old on average [27–85 years]; 61.7% were males. Ninety per cent were married. Regarding the medical history of the participants, 40% reported common chronic conditions. The average time to treatment was 3.88 months [1–12 months]. Surgery was performed on all patients, followed by 96.7% adjuvant chemotherapy (CT). The median length of remission was 33.3 months [3–167 months].
Analysis of the HADS questionnaire showed that the mean scores for depression and anxiety were 4.83 ± 4.61 Standard Deviation (SD) and 5.23 ± 3.8 SD, respectively.
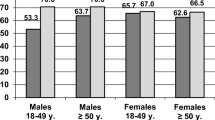
Figure 1 shows that 83.2% of participants were in the regular category for the depression score, while 15.1% were in a severe category. Regarding the anxiety score, 83.3% of participants were in the regular category, while 10% of them were in the severe one.

Distribution of patients according to HAD-S score levels
Eighty percent of patients had both normal anxiety and depression subscores (≤ 7). Only 6.6% had both anxiety and depression pathological scores.
The average fatigue score was around 3, indicating mild fatigue. It also involved the 4 sub-scales (behavioural, affective, sensory and cognitive) equally (Table 1). Ninety-one point six percent had an overall fatigue score > 1. However, only 8.33% had severe fatigue.
The mean global health score for the QLQ-C30 was79.4 ± 16.98 SD. Among functional scales, emotional functioning scored the highest 89.31 ± 16.04 SD, whereas physical functioning scored the lowest 76.39 ± 17.51 SD.
The highest scores for the QLQ-C30 symptom scales were financial difficulties and constipation with means of 30.52 ± 23.98 SD and 23.85 ± 20.39 SD, respectively, as shown in Table 2.
For the anxiety score, the statistically significant predictors were the existence of comorbidities (p = 0.05) and the administration of CT (p = 0.05). Besides, Patients with pathological anxiety score had significantly higher average scores on all subscales of the Piperscale. The affective dimension was the most influenced (p = 0.03). Depression scores were predicted by the following factors: marital status « married» (p = 0.028), associated somatic diseases (p = 0.05) and high fatigue scores. The fatigue-related factors were the lack of regular physical activity (p = 0.00) and the altered functional status during the treatment period (p = 0.009).
Analysis of QLQ-C30 by psychological indicators revealed that participants who reported suffering from anxiety and depression had worse scores in global health and all functional scales. The results of the items relating to the various physical symptoms showed that the scores for fatigue, nausea/vomiting, pain, insomnia, constipation and financial difficulties were significantly higher in the anxious patients. Depression was strongly related to the following physical symptoms: fatigue, nausea/vomiting, pain, insomnia and constipation (Tables 3 and 4).
All components of the fatigue scale were significantly related to global health (p = 0.00) and all functional scales (Table 5). Among the symptom scales, only the items "sleep disturbance" and "loss of appetite" were not related to the different domains of fatigue (Table 6).
Discussion
The proportion of participants with only an abnormal depression score and an abnormal anxiety score was 6.6% and 3.3%, respectively, and 6.6% had mixed emotional disorders.
A large systematic review performed in 2019 showed the prevalence increase and variability of these disorders in the CC remission phase with an estimate of 1.6–57% for depressive decompensations and 1–47% for anxiety disorders (Yu-Ning Peng et al. 2019). These wide variations are explained by the heterogeneity of the studied populations. Besides, it was evident that fatigue persisted years after treatment completion and even very long-term survivors experienced significantly more fatigue than the general population similar to our study (Maass et al. 2021).
Prevalence rates of anxiety and depression were higher in patients with comorbidities which is consistent with those reported by Abu-Helalah et al. (2014). Mental disorders and fatigue were positively correlated, findings suggested by Dos Santos et al. (2009) in their series identifying the comorbidities between fatigue and depression in colorectal cancer patients through specific biological mechanisms. In fact, pro-inflammatory cytokines (PICs) released during tissue destruction can have a substantial impact on neuroendocrine function and behaviour and induce a syndrome called "behavioural illness" which has many features of major depression and includes, in addition to anhedonia, anxiety and cognitive disorders, manifestations of fatigue such as slowing psychomotor, asthenia, anorexia, sleep disturbances and increased sensitivity to pain (Dunn et al. 1999).
Marital status was associated with a high HADS-D score and CT induced more anxiety. For Ell et al. (2005), it is the fear of CT side effects that significantly increases the risk of anxiety in cancer patients (p = 0.008). The lack of regular physical activity and altered performance status during treatment were associated with high scores on all dimensions of the Piper scale and these are consistent with results from other countries (Van Vulpen et al. 2016; Mota et al. 2012).
The overall mean QLQ-C30 score was 79.54 ± 16.98, which was fairly degraded and similar to that reported in a Jordanian series (Abu-Helalah et al. 2014) but higher than that mentioned in the Egyptian one conducted by Hokkam et al. (2013) which was 64.5 ± 11.9.
The worst reported symptom within the QLQ-C30 questionnaire was sleep disturbance (mean score = 25 ± 18.95). Still, this score is better than that reported for German patients (32.1) (Arndt et al. 2004).
The mean score of the financial difficulties scale (30.52 ± 23.98) is lesser than that reported in Egypt where the mean score was 47.6 (Hokkam et al. 2013) but worse than the Germanian one (20.9). Variations in the cost of cancer treatment and differences in the social security system between countries might alter the issues of this scale. In Germany, cancer patients benefit from free health insurance for cancer management.
Likewise, diarrhea and constipation with mean scores of 23.29 ± 22.34 and 23.85 ± 20.39, respectively, represent the most common physical effects induced by CC treatments that can become chronic or even unrecoverable with a negative impact on QoL (Abu-Helalah et al. 2014).
In our study, HADS-A score was an important predictor of the QoL scores especially in its physical, cognitive and social components (p < 0.05): After cancer treatment, numerous survivors report feeling alone or even abandoned following the intensive support provided during their treatment. They frequently are fearful of recurrence, generating anxiety disorder and having a negative impact on several areas of QoL (Yi and Syrjala 2017).
We demonstrated also a positive correlation between pathological HADS-A scores and symptoms of nausea, vomiting, pain and insomnia which are part of the usual autonomic symptoms of anxiety it self. Therefore, the QLQ-C30 physical symptoms may be due to anxiety rather than directly to cancer or its treatments and this is verified by Forester et al. (1993) who showed a symptoms reduction after psychotherapy. On the other hand, patients with higher scores of HADS-D had worse QoL compared to those lower scores. Results analogous to those of Weitzner et al. (1997). A pathological score on the HADS-D scale is associated with higher levels of symptoms of fatigue, pain and insomnia which are even criteria for the diagnosis of depression in the DSM IV.
As our series, there were several reports on the impact of fatigue on the deterioration of QoL in patients with CC (Mrabti et al. 2016; Tung et al. 2016; Sánchez-Jiménez et al. 2015). Fatigue is the most common symptom which significantly predicts QoL deterioration (Färkkilä et al. 2014) well a head of clinical or demographic factors.
The main limitation of the current study is the small sample size due to the reduction of patients number consulting for surveillance because of the COVID-19 epidemic situation.
However, the present study has several strengths: it offers a clear picture of prevalence rates of emotional distress and it identifies distinct associated factors. It focuses on a specific population, that is in recovery from CC because few studies carried out on such population. Furthermore, the interview led by the same health professional induces a share of homogeneity in the collection of data and finally, the use of validated measurement instruments for emotional disorders assessment and a good response rate in the patients.
Conclusion
Even in the recovery phase, CC patients can see their QoL deteriorate. It comes out of their psychological experience and their physical life. It is therefore crucial to provide greater attention to these patients for holistic and multi-disciplinary care.
References
Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ et al (1993) The European Organization for Research and Treatment of Cancer QLQ-C30:quality-of-life instrument for use in international clinical trials in oncology. J Nat Cancer Inst 85:365–376
Abu-Helalah MA, Alshraideh HA, Al-Hanaqta MM, Arqoub KH (2014) Quality of life and psychological well-being of colorectal cancer survivors in Jordan. Asian Pac J Cancer Prev 15(18):7653–7664
Arndt V, Merx H, Stegmaier C, Ziegler H, Brenner H (2004) Quality of life in patients with colorectal cancer 1 year after diagnosis compared with the general population : a population-based study. J Clin Oncol 22:4829–4836
Ben Dahhou K (2011) Adaptation transculturelle et validation des outils de mesure de qualité de vie des patients atteints de cancer au Maroc. Thèse de Doctorat en Médecine Maroc
Berger AM, Mooney K, Alvarez-Perez A et al (2015) National comprehensive cancer network. Cancer-related fatigue, version 2.2015. J Nat Compr Canc Netw. 13:1012–1039
Dos Santos J, Mota DD, Pimenta CA (2009) Co-morbida de fadiga e depressão em pacientes com câncer colo-retal [Comorbidities between fatigue and depression in patients with colorectal cancer]. Rev Esc Enferm USP 43:909–914
Dunn AJ, Wang J, Ando T (1999) Effects of cytokines on cerebral neurotransmission. Comparison with the effects of stress. Adv Exp Med Biol 461:117–127
Ell K, Sanchez K, Vourlekis B, Lee PJ, Dwight-Johnson M, Lagomasino I et al (2005) Depression, correlates of depression, and receipt of depression care among low-income women with breast or gynecologic cancer. J Clin Oncol 23:3052–3060
Färkkilä N, Torvinen S, Roine RP, Sintonen H, Hänninen J, Taari K et al (2014) Health-related quality of life among breast, prostate, and colorectal cancer patients with end-stage disease. Qual Life Res 23:1387–1394
Forester B, Kornfeld DS, Fleiss JL, Thompson S (1993) Group psychotherapy during radiotherapy: effects on emotional and physical distress. Am J Psychiatry 150:1700–1706
Gledhill J, Laizet C, Mahe C, Rodary C (2002) Validation française de l’échelle de fatigue révisée de Piper. Rech Soins Infirm 68:50–65
Hokkam E, Farrag S, El Kammash S, Faisal M (2013) Assessment of quality of life of colorectal carcinoma patients after surgery. World J Colorectal Surg 3:4
Koller M, West K (2005) Linguistic validation manual for patient-reported outcomes (PRO) instruments, By C Acquadro, K Conway, C Girourdet and I Mear, MAPI Research Trust, Lyon, France, 2004,184 pp. Qual Life Res 14:1791–1792
Maass SWMC, Brandenbarg D, Boerman LM, Verhaak PFM, de Bock GH, Berendsen AJ (2021) Fatigue among long-term breast cancer survivors: a controlled cross-sectional study. Cancers (Basel) 13(6):1301
Malasi TH, Mirza IA, El-Islam MF (1991) Validation of the hospital anxiety and depression scale in Arab patients. Acta Psychiatr Scand 84:323–326
Mota DD, Pimenta CA, Caponero R (2012) Fatigue in colorectal cancer patients: prevalence and associated factors. Rev Lat Am Enfermagem 20:495–503
Mrabti H, Amziren M, El Ghissassi I, Bensouda Y, Berrada N, Abahssain H et al (2016) Quality of life of early stage colorectal cancer patients in Morocco. BMC Gastroenterol 16:131
Sánchez-Jiménez A, Cantarero-Villanueva I, Delgado-García G, Molina-Barea R, Fernández-Lao C, Galiano-Castillo N et al (2015) Physical impairments and quality of life of colorectal cancer survivors:a case-control study. Eur J Cancer Care 24:642–649
Sung H, Ferlay J, Siegel L, R, Laversanne M, Soerjomataram I, Jemal A, et al (2021) Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209–249
Tung HY, Chao TB, Lin YH, Wu SF, Lee HY, Ching CY et al (2016) Depression, fatigue, and QoL in colorectal cancer patients during and after treatment. West J Nurs Res 38:893–908
Van Vulpen JK, Velthuis MJ, SteinsBisschop CN, Travier N, Van Den Buijs BJ, Backx FJ et al (2016) Effects of an exercise program in colon cancer patients undergoing chemotherapy. Med Sci Sports Exerc 48:767–775
Weitzner MA, Meyers CA, Stuebing KK, Saleeba AK (1997) Relationship between quality of life and mood in long-term survivors of breast cancer treated with mastectomy. Support Care Cancer 5:241–248
Yi JC, Syrjala KL (2017) Anxiety and depression in cancer survivors. Med Clin N Am 101(6):1099–1113
Yu-Ning P, Mei-Li H, Chia-Hung K (2019) Prevalence of depression and anxiety in colorectal cancer patients: a literature review. Int J Environ Res Public Health 16:411
Zigmond AS, Snaith RP (1983) The Hospital anxiety and Depression scale. Acta Psychiatr Scand 67:361–370
Funding
No funding declaration.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. AC material preparation, data collection and analysis and manuscript writing. FE commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
No conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chamsi, A., Ezzaairi, F., Sahli, J. et al. Assessment of depression, anxiety and fatigue in Tunisian patients in recovery from colon cancer and their impact on quality of life. J Cancer Res Clin Oncol 149, 4269–4274 (2023). https://doi.org/10.1007/s00432-022-04334-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-022-04334-1