
Abstract
Purpose
To determine the frequency of co-occurring genes in non-small cell lung cancer (NSCLC) patients with epidermal growth factor receptor (EGFR) mutation and the predictive effect of co-mutations on the efficacy of EGFR tyrosine kinase inhibitors (EGFR-TKIs).
Methods
54 patients with advanced NSCLC were tested for 422 clinically relevant genes by next-generation sequencing (NGS) before treatment. Among them, patients with EGFR mutation received first-line treatment of EGFR-TKIs. Progression-free survival (PFS) and objective response rate (ORR) were evaluated using Kaplan–Meier methods and compared between two groups using log-rank test.
Results
Among 24 EGFR mutant and 30 EGFR wild-type patients, co-mutation rate was lower in patients with EGFR mutation (62.5% [15/24] vs 93.3% [28/30], p = 0.005). There was lower frequency for co-alterations in BRAF (0% [0/24] vs 20% [7/30], p = 0.033), NF1 (4.2% [1/24] vs 30% [9/30], p = 0.038) and RAS–RAF–MAPK pathway genes (16.6% [4/24] vs 56.7% [17/30], p = 0.003) in EGFR mutation group. 24 patients with EGFR mutation received first-line treatment of gefitinib or erlotinib, with an ORR of 83.3% and a median PFS of 12.3 months (95% CI 10.00–14.60). Co-mutation was associated with shorter median PFS (10.2 months [95% CI 5.20–15.20] vs 15.3 months [95% CI 12.09–15.81]; HR 0.29 [95% CI 0.10–0.82]; p = 0.014) in EGFR mutation cohort. Among patients with EGFR mutation and distant metastasis, median PFS was decreased in those with co-mutations (6.3 months [95% CI 3.25–9.35] vs 22.0 months[95% CI 12.10–31.90]; HR 0.12 [95% CI 0.00–5.87]; p = 0.007) and frequency of PIK3CA (0% [0/12] vs 41.7% [5/12], p = 0.037) and PI3K/AKT/mTOR pathway genes (0% [0/12] vs 50% [6/12], p = 0.014) was lower.
Conclusion
The presence of co-mutations was lower in the EGFR mutation patients and reduces the efficacy of EGFR-TKI, especially in patients with distant metastases. Lower frequency of co-mutation in PIK3CA and PI3K/AKT/mTOR pathway genes may be responsible for promoting metastasis and limiting the efficacy of EGFR-TKIs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The emergence of the targeted therapeutic drug epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) has significantly improved the objective response rate (ORR) and progression-free survival (PFS) of advanced non-small cell lung cancer (NSCLC) patients with epidermal growth factor receptor (EGFR) mutant, becoming a milestone event in the history of lung cancer treatment. Multiple phase III studies have confirmed that NSCLC patients with EGFR mutant received TKIs treatment can obtain a median PFS about 10 months (Mok et al. 2009; Sequist et al. 2013; Zhou et al. 2011). However, approximately 30% of NSCLC patients with EGFR mutation develop drug resistance in the early stage of treatment with EGFR-TKIs (Janne et al. 2015; Morgillo et al. 2016; Xu et al. 2017), which is called primary drug resistance. At this time, the disease often progresses rapidly, thus limiting the efficacy of targeted drugs.
The mechanism of primary drug resistance of EGFR-TKIs has not been fully elucidated. Past studies have suggested that the driver genes are mutually exclusive, and current NSCLC-targeted therapies are mainly targeted at single oncogene driver (Li et al. 2013). Despite some sporadic reports says that TP53, KRAS, PTEN, PIK3CA and BRAF mutation may be used as driver mutations co-existing with EGFR to jointly promote tumor progression and affect the efficacy of EGFR-TKIs (Canale et al. 2017; VanderLaan et al. 2017; Wu et al. 2016). However, multiple genetic changes and signaling pathways co-existing with EGFR that affect the efficacy of EGFR-TKIs are far from elucidated.
As a high-throughput sequencing technique, next-generation sequencing (NGS) can perform multiple typology analysis on thousands of genes. Even in patients with EGFR negative lung cancer, NGS can be used to detect unknown genetic mutations (Jin et al. 2016; Kamps et al. 2017). The main purpose of clinical implementation of NGS is to find the main driver gene of advanced patients and carry out targeted therapy, as well as to try to find the molecular mutation target of drug resistance and treatment countermeasures. In this study, we used NGS technology to detect multi-gene changes before TKIs treatment in advanced NSCLC patients with EGFR mutation, analyzed their clinical and pathological characteristics, and tried to verify that multiple gene mutations co-existing with EGFR would affect the clinical efficacy of EGFR-TKIs.
Materials and methods
Patients and samples
We retrospectively screened consecutive patients from June 2016 to August 2017, a total of 54 patients with advanced lung adenocarcinoma in Second Affiliated Hospital of Harbin Medical University, China, were undergoing tumor biopsies for gene analysis before any therapy. Formalin-fixed paraffin-embedded (FFPE) tumor samples were obtained from the Second Affiliated Hospital of Harbin Medical University and all participants had signed informed consent. Use of samples was approved by the Ethical Review Committee of Second Affiliated Hospital of Harbin Medical University. All tissues were reviewed by pathologists for confirmation of tumor histology and tumor content. All patients were tested for 422 cancer-related genes by next-generation sequencing using KAPA LTP Library Prep Kit before treatment to confirm the presence of EGFR-sensitive mutations (determined in tumor tissue). 422 cancer-related genes are listed in supplementary Table 1. Among them, patients with EGFR-sensitive mutation received first-line treatment of EGFR-TKIs. The tests were performed in a centralized clinical testing center (Nanjing Geneseeq Technology Inc., Nanjing, China). From each paraffin block of representative tumor areas, serial sections with a thickness of 10 μm were prepared. The specimen contained a minimum of 20% tumor cells, and patients with insufficient or poor-quality tissue for molecular analyses were excluded from this study. The TNM classification was determined according to the Seventh Edition of the TNM Classification for Lung Cancer (Goldstraw et al. 2007).
DNA extraction
Five to eight of 10-μm FFPE tissue sections were used to scrap into microcentrifuge tubes. The tissues were deparaffinized with 1 mL xylene at 56 °C for 10 min, washed with 1 mL 100% ethanol for 5 min at RT, and then dried at 37 °C for 10 min. Genomic DNA was extracted using QIAamp DNA FFPE Tissue Kit (Qiagen, Valencia, CA, USA). DNA concentration was determined by Qubit dsDNA HS assay kit on the Qubit Fluorometer according to the manufacturing protocol (Life Technologies, Carlsbad, CA, USA). The DNA quality was measured by Nanodrop2000 (Thermo Fisher Scientific) and the quantity was measured by dsDNA HS Assay Kit (Life Technologies) on Qubit 2.0.
Library preparation and sequencing
Sequencing library was prepared by Illumina TruSeq DNA PCR-Free Sample Preparation Kit (Illumina, San Diego, CA, USA) with optimized protocols. Extracted tumor genomic DNA was fragmented into 300–350 bp using Covaris M220 instrument (Covaris, Woburn, MA, USA). Sheared tissue DNA were experienced with end-repairing, A-tailing, adapter ligation and size selection using Agencourt AMPure XP beads (Beckman Coulter). Libraries were then subjected to PCR amplification and purification before targeted enrichment.
Different DNA libraries marked with unique indices and up to 2 μg of libraries input were pooled together for targeted enrichment. Human cot-1 DNA (Life Technologies) and xGen Universal blocking oligos (p5 or p7; Integrated DNA Technologies, Coralville, IA, USA) were added to block nonspecific binding of library DNA to targeted probes. Customized xGen lockdown probes panel (IDT) and TruSight Cancer Panel Probes (Illumina) were used for targeted enrichment of 422 cancer-related genes. The hybridization reaction was performed by using NimbleGen SeqCap EZ Hybridization and Wash Kit (Roche). Dynabeads M-270 (Life Technologies) was used to capture probe-bind fragments, followed by postcapture amplification with Illumina p5 (5′ AAT GAT ACG GCG ACC ACCGA 3′) and p7 primers (5′ CAA GCA GAA GAC GGC ATA CGA GAT 3′) in KAPA HiFi HotStart ReadyMix (KAPA Biosystems). Postcapture amplified library was purified by Agencourt AMPure XP beads. Library quantification was analyzed by KAPA Library Quantification kit (KAPA Biosystems, Boston, MA, USA). Library fragment size was measured by Agilent Technologies 2100 Bioanalyzer (Agilent Technologies). The enriched libraries were sequenced on Hiseq4000 NGS platforms (Illumina) according to its instruction.
Sequence data processing
Trimmomatic (Bolger et al. 2014) was used for FASTQ file sequencing data quality control. The reads with a low quality (below the threshold of 15), as well as N bases were removed before mapping to reference sequence hg19 (Human Genome version 19) using Burrows–Wheeler Aligner (BWA) (Li and Durbin 2009) with modified parameters. SNPs/indels were identified using VarScan2 (MAF < 10%) (http://dkoboldt.github.io/varscan/) and HaplotypeCaller/UnifiedGenotyper in Genome Analysis Toolkit (GATK) (MAF > 10%) (DePristo et al. 2011). A mutation was called when at least 3 mutated reads were found in the sample on different strands with good quality scores and manually inspected in Integrative Genomics Viewer (IGV, Broad Institute). Genomic fusions were identified by FACTERA (Newman et al. 2014) with default parameters. Copy number variations (CNVs) were detected using ADTEx (http://adtex.sourceforge.net) with default parameters. Proposed discrete wavelet transform (DWT) was used to reduce intrinsic noise. The copy number gains/losses of each targeted region are performed by a Hidden Markov Model (HMM).
Statistical analysis
Activating EGFR mutations are defined as mutations in the first four exons (18–21) of tyrosine kinase. Mutations other than exon 20 insertion or T790M mutation were defined as sensitizing EGFR mutation. The association between response and concomitant mutation was determined by logistic regression analysis. Data were analyzed from June 1, 2016, to August 31, 2018. Kaplan–Meier survival curves and Cox proportional-hazards regression analysis were performed, and hazard ratios (HRs) and 95% CIs were calculated to determine the survival difference. Statistical significance was defined as a 2-sided p < 0.05. Survival curves were calculated using the Kaplan–Meier method from the start of diagnosis of advanced NSCLC until death or last follow-up. PFS of EGFR-TKIs was defined as the time from EGFR-TKIs therapy to documented progression or death from any cause or until the time of the last follow-up. Lung function results of the two groups were tested by t test using SPSS 19.0 software (Chicago, IL, US). p < 0.05 was considered statistically significant. The median follow-up period was 14.3 months (0.6–26) and the last follow-up was on August 31, 2018.
Results
Baseline characteristics
From June 1, 2016, to August 31, 2017, a total of 54 patients were screened for genetic alterations in tumor tissue by NGS. 24 (44.4%) patients had EGFR activating mutations with a median age of 68 years (range 35–84 years), 16 (66.7%) were female, 16 (66.7%) were non-smokers, and 23 (95.8%) had adenocarcinoma. In EGFR mutation-negative cohort, the median age was 65.5 years (range 35–84 years), including 10 (33.3%) females, 14 (46.7%) non-smokers and 22 (73.3%) adenocarcinoma. EGFR mutation are more common in women (66.7% vs 33.3%, p = 0.015)and patients with adenocarcinoma (95.8% vs 73.3%, p = 0.028). EGFR mutation status was independent of family history of malignancy and distant metastasis at initial diagnosis. At the time of data cutoff (August 31, 2018), 11 (11/54) patients had progressive disease or died, median follow-up was 14.3 months. Overall survival (OS) data were still immature until the end of the follow-up. Detailed clinicopathological characteristics between two groups are listed in Table 1.
Co-occurring genetic analysis between EGFR mutation-positive patients and EGFR mutation-negative patients
To determine the prevalence of co-occurring genetic alterations in patients with advanced lung cancers, multiple gene assays were performed (the spectrum of somatic genetic alterations) in 24 EGFR mutation-positive and 30 EGFR mutation-negative patients with advanced stage (stage IIIB or IV). Copy number variants (CNV), inframe_indel, fusions, frameshift, missense, splicing, stop_gained across 422 clinically relevant cancer genes were tested by NGS.
Analysis of 24 EGFR mutation-positive cohort and 30 EGFR mutation-negative cohort showed the widespread presence of co-occurring genetic alterations beyond EGFR driver mutation (Fig. 1a, b). A total of 15 patients (15/24, 62.5%) were found to have co-occurring genetic alterations in EGFR mutation-positive patients, compared with 93.3% (28/30) in the EGFR mutation-negative group (p = 0.005). The most common co-mutated genes in EGFR mutation-positive cohort were TP53 (37.5%, 9/24), PIK3CA (20.8%, 5/24), KRAS (12.5%, 3/24), PKHD1 (12.5%, 3/24) and RB1 (8.3%, 2/24), while in EGFR mutation-negative group were TP53 (36.7%, 11/30), NF1 (30%, 9/30), BRAF (23.3%, 7/30), RB1 (20%, 6/30), and KRAS (16.7%, 5/30), respectively (Fig. 1c). The average genetic alterations (beyond EGFR) per patient in EGFR mutation-positive cases were 3.04 ± 1.63 (mean ± s.e.m), the range of detectable alterations was 0–17, compared with 3.97 ± 1.95 (mean ± s.e.m) in EGFR mutant-negative group, range 0–16 (p = 0.821). The proportion of patients with at least one co-mutation gene was associated with a family history of malignancy in the EGFR mutation-positive group compared with the EGFR mutation-negative group (80% [12/15] vs 37.5% [10/28], p = 0.014) (Table 2). No differences were found in age, gender, smoking status, histology subgroups and distant metastasis between two groups (Table 2).

Co-occurring genomic alterations detectable in patients with advanced-stage EGFR mutation-positive (n = 24) compared with EGFR mutation-negative (n = 30) NSCLC detected by next-generation sequencing. a, b Frequency of genetic mutations: copy number variants (CNV), inframe_indel, fusions, frameshift, missense, splicing, stop_gained across 422 cancer-related genes detected by next-generation sequencing from 24 patients with advanced-stage EGFR mutation-positive NSCLC (a) and 30 patients with advanced-stage EGFR mutation-negative NSCLC (b). c Top 5 concomitant genes in EGFR mutation-positive cohort (beyond EGFR) and EGFR mutation-negative cohort. d Concomitant gene alterations in EGFR mutant-positive compared with EGFR mutant-negative samples (two-tailed Fisher’s exact test, p values). e Differences in pathway-level alterations between EGFR mutation-positive and EGFR mutation-negative cases (two-tailed Fisher’s exact test, p values)
Next, we queried the function of all detected concomitant genes and the involved signaling pathways using an online method (http://www.genecards.org). Frequency of patients had at least 1 variant of known functional mutations other than EGFR was statistically lower in EGFR mutation-positive cohort (62.5% [15/24] vs 93.3% [28/30], p = 0.005). Most of the concomitant genes in EGFR mutation-positive cohort are known functional genes (88.9% [80/90] vs 77.1% [91/118], p = 0.028), and only 11.1% were determined as likely passenger events (11.1% [10/90] vs 22.9% [27/118], p = 0.028) (Table 3).
Further comparison of the frequency of co-occurring genetic alterations in the EGFR mutation-positive samples (n = 24) with those present in the EGFR mutation-negative samples (n = 30) showed significant differences for certain genetic events. There was lower frequency for co-alterations in BRAF (frequency of alteration in EGFR mutation-positive cases, 0% [0/24] vs EGFR mutation-negative cases, 20% [7/30], p = 0.033), NF1 (frequency of alteration in EGFR mutation-positive cases, 4.2% [1/24] vs EGFR mutation-negative cases, 30% [9/30], p = 0.038) in the EGFR mutation-positive samples compared with EGFR mutation-negative cohort (Fig. 1d).
BRAF and NF1 genes all belong to RAS–RAF–MAPK pathway at the signal pathway level, further signaling pathways analysis showed co-alterations in RAS–RAF–MAPK pathway genes (16.6% [4/24] vs 56.7% [17/30], p = 0.003) was significantly lower in EGFR mutation-positive cohort than in EGFR mutation-negative cohort. While alterations in RTK-pathway genes (26.7% [8/30] vs 8.3% [2/24], p = 0.170), TP53-pathway genes (37.5% [9/24] vs 40% [12/30], p = 0.854) and PI3K/AKT/MTOR pathway genes (25% [6/24] vs 26.7% [8/30], p = 0.832) had no difference between two groups. This data indicated a potential role for abnormal expression of RAS–RAF–MAPK signaling pathway genes in the pathogenesis of advanced EGFR mutation-positive NSCLC (Fig. 1e).
EGFR gene alterations and efficacy analysis
The incidence of EGFR mutation among detected NSCLC patients were 44.4% (24/54). Among them, 8 (33.3%) patients were confirmed as exon 19 deletion, 16 (66.7%) patients hold L858R point mutation in exon 21. Only 1 (4.2%) had multiple EGFR mutations (L858R point mutation in exon 21, G719C in exon 18 and R776L point mutation in exon 20). Additionally, 3 (12.5%) patients had EGFR mutation accompanied by EGFR gene amplification. No de novo co-occurring T790M mutations were detected.
24 patients with EGFR mutation received first-line treatment with gefitinib 250 mg/day or erlotinib 150 mg/day and the efficacy was assessed. Among them, 17 (70.8%) patients had partial responses (PR), 3 (12.5%) patients had complete response (CR), 2 (8.3%) patients had stable disease (SD) and 2 (8.3%) patient had progressive disease (PD). The ORR in the overall population was 83.3%, disease control rate (DCR) was 91.7% (Supplementary Table 3). First-line treatment of EGFR-TKIs received a median PFS of 12.3 months (Fig. 2a; 95% CI 10.00–14.60). One patient with multiple EGFR mutations had lower PFS than full analysis set (9.3 months vs 12.3 months).

Kaplan–Meier curves of progression-free survival (PFS) (N = 24). a Progression-free survival in the EGFR mutation-positive cohort. b Progression-free survival according to EGFR mutation subtypes. c Progression-free survival according to concomitant mutations status in EGFR mutation-positive patients. Patients who had neither disease relapse or metastasis nor death were censored on their last tumor evaluable date. p values were calculated using a two-sided log-rank test. Hazard ratios were calculated with the use of a Cox proportional-hazards model. EGFR denotes epidermal growth factor receptor. CI confidence interval, HR hazard ratio
Analyses of clinicopathologic data by subtypes of EGFR mutation status at baseline (exon 19 deletion vs exon 21 Leu858Arg) are summarized in Supplementary Table 2. The mutant subtype of EGFR was independent of gender, age, smoking status and distant metastasis. The proportion had not achieved an increased ORR (75% vs 87.5%, p = 0.846) and DCR (87.5% vs 83.3%, p = 1) in patients with EGFR exon 19 deletion compared with those with exon 21 Leu858Arg (Supplementary Table 2). Besides, although median PFS was extended, the difference between subgroups was not significant (12.4 months [95% CI 4.33–20.47] vs 11.8 months [95% CI 9.15–14.45]; HR 1.10, 95% CI 0.68–1.77; p = 0.701; Fig. 2b).
Analysis of concomitant gene mutations in EGFR mutation-positive patients treated with EGFR-TKI
Of 24 EGFR mutation patients with baseline NGS data, 15 (66.7%) patients had concomitant gene mutations. The 24 patients were separated into two subgroups according to the presence of co-occurring genetic alterations. The first subgroup (n = 9) had only EGFR-sensitive mutations; the second subgroup (n = 15) had EGFR-sensitive mutations with concomitant mutation.
Concomitant mutation was significantly associated with shorter duration of PFS (Fig. 2c); median PFS, 10.2 months [95% CI 5.20–15.20] vs 15.3 months [95% CI 12.09–15.81]; HR, 0.29 [95% CI 0.10–0.82]; p = 0.014). Due to the small sample size, there was no statistical difference in ORR (88.9% vs 80%, p = 0.572) and DCR (100% vs 86.7%, p = 0.511) between the two subgroups, but ORR in the concomitant mutation group tended to decrease (Supplementary Table 2).
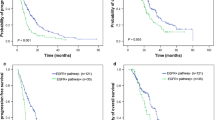
We then investigated the relationship between co-mutation and distant metastasis at initial diagnosis in EGFR mutation-positive patients treated with EGFR-TKIs. Subgroup analysis of PFS was performed based on the presence or absence of distant metastasis. Among the patients without distant metastasis, PFS was close in concomitant not detected group and concomitant detected group (Fig. 3a; median PFS, 12.3 months [95% CI 11.23–13.37] vs 10.8 months [95% CI 8.16–13.44]; HR, 0.72 [95% CI 0.22–2.83]; p = 0.718). However, it is worth noting that among patients with distant metastasis, PFS decreased obviously in those with co-occurring genetic alternations (Fig. 3b; median PFS, 6.3 months [95% CI 3.25–9.35] vs 22.0 months [95% CI 12.10–31.90]; HR 0.12 [95% CI 0.00–5.87]; p = 0.007).

a Kaplan–Meier curves of progression-free survival according to concomitant mutations status in EGFR mutation-positive patients without distant metastasis. b Progression-free survival according to concomitant mutations status in EGFR mutation-positive patients with distant metastasis. Patients who had neither disease relapse or metastasis nor death were censored on their last tumor evaluable date. p values were calculated using a two-sided log-rank test. Hazard ratios were calculated with the use of a Cox proportional-hazards model. EGFR denotes epidermal growth factor receptor. CI confidence interval, HR hazard ratio. c Gene alterations with higher frequency according to distant metastasis sites in EGFR mutant-positive cases. d Differences in pathway-level alterations according to distant metastasis sites in EGFR mutant-positive cases. p values were calculated using two-tailed Fisher’s exact test
Co-occurring genetic alterations frequency comparison between EGFR mutation-positive samples with distant metastasis cohort (n = 12) and those present in the EGFR mutation-positive samples without metastasis (n = 12) showed significant differences. There was lower frequency for co-alterations in PIK3CA in EGFR mutation-positive patients with distant metastasis cohort (0% [0/12] vs 41.7% [5/12], p = 0.037). While alterations in TP53 (58.3% [7/12] vs 25% [3/12], p = 0.214), KRAS (0% [0/12] vs 25% [3/12], p = 0.217), NF1 (8.3% [1/12] vs 0% [0/12], p = 1), AKT3 (0% [0/12] vs 8.3% [1/12], p = 1) and other genes had no difference between two groups (Fig. 3c).
Signaling pathways analysis showed PI3K/AKT/mTOR pathway genes in EGFR mutation-positive patients with distant metastasis cohort were significantly lower than that in those without distant metastasis (0% [0/12] vs 50% [6/12], p = 0.014). While co-alterations in TP53-pathway genes (58.3% [7/12] vs 25% [3/12], p = 0.214), MAPK-pathway genes (8.3% [1/12] vs 25% [3/12], p = 0.590), DNA repair co-alterations (8.3% [1/12] vs 8.3% [1/12], p = 1) and Cell Cycle co-alterations (16.7% [2/12] vs 8.3% [1/12], p = 1) had no differences between EGFR mutation-positive patients with or without distant metastasis cohort (Fig. 3d).
Discussion
Currently, the main principle of lung cancer targeted therapy is to discover and target mutations of a driver gene, such as EGFR-TKIs yield significant benefits in patients with EGFR mutations (Mok et al. 2009; Sequist et al. 2013; Zhou et al. 2011). However, with the development of NGS, we found co-mutations of other genes often exist combined with EGFR mutation, which will significantly alter the biological characteristics of tumors and affect the prognosis of patients. Consistent with previous studies (Blakely et al. 2017; Hong et al. 2018), our study also reveals the widespread existence of co-mutations in EGFR mutation and wild-type patients. Besides, the presence of co-mutations may promote tumor metastasis and is negatively associated with response and survival rates in patients receiving first-line treatment with EGFR-TKIs.
Although driver genes like EGFR in NSCLC were reported to be mutually exclusive (Li et al. 2013), several studies have shown that multiple genes occur concurrently with EGFR mutations in almost all the advanced NSCLC (Blakely et al. 2017; Hong et al. 2018; Chiadini et al. 2018). In our study, in order to determine the prevalence of co-mutations in patients with advanced lung cancers, we tested 422 clinically relevant cancer genes by NGS among 24 EGFR mutation-positive and 30 EGFR mutation-negative patients with advanced-stage NSCLC. Similar to a recent study (Blakely et al. 2017), our study also found frequency of patients who had co-occurring genetic alterations was statistically lower in EGFR mutation-positive patients compared with EGFR wild-type patients. In addition, patients with EGFR mutant were more likely to be associated with functional co-mutant genes. Few previous studies have discussed the correlation between co-mutation and clinicopathologic information. Hong et al. (2018) insisted that patients with EGFR mutation-positive and smoking history were significantly associated with a higher incidence of concomitant mutation. However, this study only retrospectively analyzed the clinicopathological features of patients with EGFR mutation-positive without comparing those with EGFR wild-type. In our study, we found that among all the patients with co-mutations, those with EGFR mutations are associated with a family history of malignancy compared with EGFR mutation-negative patients. No differences were found in age, gender, smoking status, histology subgroups and distant metastasis.
The occurrence of tumors is closely related to the mutation of some key genes that mediate cell proliferation, differentiation and apoptosis. As EGFR mutant and wild-type NSCLC patients have different biological properties, their concomitant genes are also different. The most common co-mutated genes in EGFR mutation-positive cohort were TP53, PIK3CA, KRAS, PKHD1 and RB1, while in EGFR mutation-negative group were TP53, NF1, BRAF, RB1 and KRAS, respectively. TP53 is highly mutated in both EGFR mutant and wild-type patients, which is a potential target for lung adenocarcinoma. Although such mutations would seem to confer resistance to TKIs, there are still no drugs capable of inhibiting the growth of TP53-mutated cells (Canale et al. 2017). It is worth noting that our study found the proportion of NF1 and BRAF genes in the EGFR mutant is significantly lower than in the EGFR wild-type patients. Although the RB1 gene was not statistically different between the two groups, there was a tendency of low mutation rate in patients with EGFR mutant. BRAF gene activation mutation can occur in a variety of tumors and cancer cell lines. Recent studies suggest that BRAF gene activation mutation may be closely related to the occurrence, development and treatment prognosis of lung cancer. BRAF mutation rate is about 3% in NSCLC (Paik et al. 2011) and represent possible targets for therapy using anti-BRAF agents (vemurafenib or dabrafenib) (Gautschi et al. 2015; Hyman et al. 2015). A slightly higher frequency of BRAF mutations was observed in EGFR mutation-negative patients in our study, possibly attributable to the fact that the number of patients enrolled is small and patients with EGFR mutation-positive were excluded. No co-mutation of EGFR and BRAF genes were found. NF1 is a genetic disorder that can negatively regulate the RAS–RAF–MAPK signaling pathway (Chen et al. 2018). Recently, a report showed that co-occurrence of RASA1 and NF1 mutations shows mutual exclusivity with other oncogenic drivers such as KRAS and EGFR, revealing RASA1/NF1 co-mutation as new potential target of NSCLC (Hayashi et al. 2018). Another study indicated that lower expression of NF1 was significantly correlated with primary and acquired resistance of EGFR-TKIs (Chen et al. 2018; de Bruin et al. 2014). BRAF and NF1 genes all belong to RAS–RAF–MAPK pathway at the signal pathway level. Previous studies have shown that approximately two-thirds of NSCLC patients harbored RAS–RAF–MAPK-mediated genetic changes in downstream signals (Kitajima and Barbie 2018). Our study showed that co-alterations in RAS–RAF–MAPK pathway genes were significantly lower in EGFR mutation-positive cohort than in EGFR mutation-negative cohort, indicating a potential role for abnormal expression of RAS–RAF–MAPK signaling pathway genes in the pathogenesis of advanced EGFR mutation-positive NSCLC and the possible connections agents of anti-RAS–RAF–MAPK signaling pathway targeted therapies in EGFR mutation-negative patients. Targeting the MAPK pathway downstream oncogenic directly like BRAF mutation in lung adenocarcinoma has been effective clinically. Besides, while NF1 gene mutation can theoretically activate the upstream of RAS pathway, whether it can be used as a therapeutic driving target for patients with EGFR wild-type still needs to be verified by more clinical studies since there is still no suitable target for those patients and platinum-based chemotherapy remains to be the first-line treatment. In addition, how EGFR gene expression and MAPK pathway genes interact remains to be further studied.
Clinically, the mutation rate of EGFR in the east Asian population is as high as 40–50%, and the treatment with EGFR-TKIs has achieved significant clinical efficacy, with the median PFS of about 10 months and ORR of about 80% (Mok et al. 2009; Sequist et al. 2013; Zhou et al. 2011). In our study, the incidence of EGFR mutation among detected NSCLC patients was 44.4% all of whom received first-line treatment with gefitinib or erlotinib. Similar to previous studies, ORR in our study was 83.3%, DCR was 91.7%. First-line treatment of EGFR-TKIs received a median PFS of 12.3 months. Several clinical trials have reported on multiple mutations in EGFR, mutation rate is about 2.1%(4/437)in IPASS trail (Mok et al. 2009), 1.5% (3/204) in BR.21 trail (Shepherd et al. 2005). In addition, the ORR to EGFR-TKI was lower in patients with multiple EGFR mutation than in those with single EGFR mutation (Lowder et al. 2015). In our study, only 1 (4.2%) patient had multiple EGFR mutations (L858R point mutation in exon 21, G719C in exon 18 and R776L point mutation in exon 20) and received a PFS of 9.3 months which was significantly lower than full analysis set. Whether activating EGFR mutation type will affect EGFR-TKIs clinical efficacy remains controversial, some researches holds the point that patients with EGFR exon 19 deletion were found to have longer PFS than those with exon 21 mutation (Hong et al. 2018; Lee et al. 2015). However, IPASS indicated no significant difference in PFS with gefitinib between exon 19 deletions and exon 21 L858R mutation subgroup (Mok et al. 2009). Our study also found the proportion had not achieved an increased ORR and PFS in patients with EGFR exon 19 deletion compared to those with exon 21 L858R. Analyses of clinicopathologic data showed activating EGFR mutation type was independent of gender, age, smoking status and distant metastasis.
Although EGFR-TKIs brings significant survival benefits to patients with EGFR mutation, approximately 30% of patients were found to be initially resistant to EGFR-TKIs and the disease progressed rapidly (Janne et al. 2015; Morgillo et al. 2016; Xu et al. 2017). The mechanism of this primary resistance has not yet been elucidated. A few anecdotal reports point out that the prevalence of concomitant mutations may affect clinical outcomes in advanced-stage lung cancers with EGFR mutation. It has been reported that EGFR mutation-positive patients treated with first-line EGFR-TKIs showed a significantly lower ORR and shorter PFS when accompanied by TP53 co-mutation, especially EGFR exon 19 deletion with TP53 exon 8 co-mutation (Canale et al. 2017). In the current commentary of EBioMedicine, Rafael Rosell, Niki Karachaliou pointed out that shorter PFS was related to co-mutations in EGFR-driven NSCLC, most studies show that co-mutation of TP53, RB1, PTEN or MET are poor prognostic factors (Rosell and Karachaliou 2019). A recent study (Blakely et al. 2017) found that changes in the Wnt/β-catenin pathway and mutations in CDK4 and CDK6 cell cycle related genes may affect EGFR inhibitor responses. Besides, the authors found that co-mutation of EGFR with CTNNB1 or PIK3CA resulted in synergistic promotion of tumor metastasis or EGFR inhibitor resistance. In addition to advanced-stage NSCLC, co-mutation in resected EGFR mutation-positive NSCLC may also lead to poor treatment effect of EGFR-TKIs. In 139 resected stage I–IIIA EGFR-mutant NSCLC, 34% patients had EGFR downstream or bypass gene co-mutation, such as PIK3CA, BRCA1 and NOTCH1, which affected the EGFR-TKIs efficacy (Zhao et al. 2019). Consistent with most of the studies, our study found that concomitant mutation was significantly associated with shorter duration of PFS, however, there was no statistical difference in ORR, but ORR in the concomitant mutation group tended to decrease. Our study was limited by small sample size, of which may limited further exploration of the co-mutation gene and signal pathway changes that affect the efficacy of EGFR-TKI. Although there is a consensus that co-mutations reduce the efficacy of EGFR-TKIs, researchers differ on which of the co-mutated genes might truly affect the effect. It may be due to the experimental results bias caused by the difference of sample size, or it may be due to genetic heterogeneity. In a word, these results could have an instructive significance on the selection of EGFR-mutant NSCLC patients to be treated with first-line TKIs.
Distant metastasis is the main factor affecting the course and prognosis of lung cancer, and the molecular mechanism of distant metastasis in lung cancer-related signal pathways has not been elucidated in current studies. Some studies have found that EGFR mutation can promote the activation of STAT3 signaling pathway and lead to brain metastasis in lung cancer cells by inhibiting the expression of miR-2 (Singh et al. 2015). In addition, mutations of EGFR gene combined with the downstream MET gene are more likely to have distant metastasis (Breindel et al. 2013). To study the molecular mechanism of distant metastasis in patients with positive EGFR mutation, we investigated the relationship between co-mutation and distant metastasis at initial diagnosis in EGFR mutation-positive patients treated with EGFR-TKI. The study found that among patients with distant metastasis, PFS decreased obviously in those with co-occurring genetic alternations. A higher median PFS (median PFS, 22.0 months) than usual was observed in EGFR mutation-positive patients with distant metastasis in our study, possibly attributable to the small sample size. Further analysis of co-occurring alterations revealed that lower frequency of PIK3CA and PI3K/AKT/mTOR pathway genes were seen in EGFR mutation-positive patients with distant metastasis cohort. PIK3CA is a universal cancer driver that connects growth factor signals with many downstream signaling pathways, such as cell proliferation, metabolism and survival. Recently, a new study by scientists from Wister institute found that use of PI3K inhibitors alone for cancer treatment may induces the transcription and signaling pathways of cancer cells to be reprogrammed, promote the invasiveness of tumor cells and spread to other organs, which fully demonstrated the key role of PI3K signaling pathway in the metastasis of cancer cells (Caino et al. 2015). In summary, our study is the first to show that inhibition of the PI3K signaling pathway in patients with positive EGFR mutation may be the mechanism leading to distant metastasis. However, whether the PI3K signaling pathway can be a target for the inhibition of distant metastasis in patients with positive EGFR mutation still needs to be verified by more clinical trials.
The main shortcoming of our study is the sample size, therefore, genetic analysis may be biased and further analysis of co-occurring gene changes and signaling pathway alteration in patients with initial EGFR resistance may be limited. Second, our study is only a retrospective analysis and needs to be validated by prospective studies. In addition, because of the heterogeneity, gene expression in metastatic lesions and primary lesions may be inconsistent. Due to the difficulty in obtaining tissue samples from metastatic lesions, our study only analyzed the genetic changes in the primary lesions of patients with distant metastasis at initially diagnosed, so the results may be biased.
In conclusion, our study highlights the widespread existence of concomitant genes in the vast majority of EGFR mutation and wild-type patients. Besides, the presence of co-occurring genetic alterations may lead to initial resistance to first-line treatment of EGFR-TKIs. Of note, our study is the first to show that lower expression of PIK3CA and PI3K/AKT/mTOR pathway genes in patients with positive EGFR mutation may be the mechanism leading to distant metastasis. Analysis of EGFR mutations and their co-occurring gene changes have a decisive impact on the selection of EGFR-mutated NSCLC patients to be treated with first-line TKIs.
References
Blakely CM, Watkins TBK, Wu W, Gini B, Chabon JJ, McCoach CE et al (2017) Evolution and clinical impact of co-occurring genetic alterations in advanced-stage EGFR-mutant lung cancers. Nat Genet 49(12):1693–1704. https://doi.org/10.1038/ng.3990
Bolger AM, Lohse M, Usadel B (2014) Trimmomatic: a flexible trimmer for Illumina sequence data. Bioinformatics 30(15):2114–2120. https://doi.org/10.1093/bioinformatics/btu170
Breindel JL, Haskins JW, Cowell EP, Zhao M, Nguyen DX, Stern DF (2013) EGF receptor activates MET through MAPK to enhance non-small cell lung carcinoma invasion and brain metastasis. Can Res 73(16):5053–5065. https://doi.org/10.1158/0008-5472.Can-12-3775
Caino MC, Ghosh JC, Chae YC, Vaira V, Rivadeneira DB, Faversani A et al (2015) PI3K therapy reprograms mitochondrial trafficking to fuel tumor cell invasion. Proc Natl Acad Sci USA. 112(28):8638–8643. https://doi.org/10.1073/pnas.1500722112
Canale M, Petracci E, Delmonte A, Chiadini E, Dazzi C, Papi M et al (2017) Impact of TP53 mutations on outcome in EGFR-mutated patients treated with first-line tyrosine kinase inhibitors. Clin Cancer Res 23(9):2195–2202. https://doi.org/10.1158/1078-0432.CCR-16-0966
Chen J, Cui JD, Guo XT, Cao X, Li Q (2018) Increased expression of miR-641 contributes to erlotinib resistance in non-small-cell lung cancer cells by targeting NF1. Cancer Med 7(4):1394–1403. https://doi.org/10.1002/cam4.1326
Chiadini E, Canale M, Delmonte A, Dazzi C, Casanova C, Capelli L et al (2018) Frequency of actionable alterations in epidermal growth factor receptor (EGFR) wild type non-small cell lung cancer: experience of the Wide Catchment Area of Romagna (AVR). J Thorac Dis. 10(8):4858–4864. https://doi.org/10.21037/jtd.2018.07.22
de Bruin EC, Cowell C, Warne PH, Jiang M, Saunders RE, Melnick MA et al (2014) Reduced NF1 expression confers resistance to EGFR inhibition in lung cancer. Cancer Discov 4(5):606–619. https://doi.org/10.1158/2159-8290.CD-13-0741
DePristo MA, Banks E, Poplin R, Garimella KV, Maguire JR, Hartl C et al (2011) A framework for variation discovery and genotyping using next-generation DNA sequencing data. Nat Genet 43(5):491–498. https://doi.org/10.1038/ng.806
Gautschi O, Milia J, Cabarrou B, Bluthgen MV, Besse B, Smit EF et al (2015) Targeted therapy for patients with BRAF-mutant lung cancer: results from the European EURAF Cohort. J Thorac Oncol 10(10):1451–1457. https://doi.org/10.1097/JTO.0000000000000625
Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R et al (2007) The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. J Thorac Oncol 2(8):706–714. https://doi.org/10.1097/JTO.0b013e31812f3c1a
Hayashi T, Desmeules P, Smith RS, Drilon A, Somwar R, Ladanyi M (2018) RASA1 and NF1 are preferentially co-mutated and define a distinct genetic subset of smoking-associated non-small cell lung carcinomas sensitive to MEK inhibition. Clin Cancer Res 24(6):1436–1447. https://doi.org/10.1158/1078-0432.CCR-17-2343
Hong S, Gao F, Fu S, Wang Y, Fang W, Huang Y et al (2018) Concomitant genetic alterations with response to treatment and epidermal growth factor receptor tyrosine kinase inhibitors in patients with EGFR-mutant advanced non-small cell lung cancer. JAMA Oncol 4(5):739–742. https://doi.org/10.1001/jamaoncol.2018.0049
Hyman DM, Puzanov I, Subbiah V, Faris JE, Chau I, Blay JY et al (2015) Vemurafenib in multiple nonmelanoma cancers with BRAF V600 mutations. N Engl J Med 373(8):726–736. https://doi.org/10.1056/NEJMoa1502309
Janne PA, Yang JC, Kim DW, Planchard D, Ohe Y, Ramalingam SS et al (2015) AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N Engl J Med 372(18):1689–1699. https://doi.org/10.1056/NEJMoa1411817
Jin Y, Shao Y, Shi X, Lou G, Zhang Y, Wu X et al (2016) Mutational profiling of non-small-cell lung cancer patients resistant to first-generation EGFR tyrosine kinase inhibitors using next generation sequencing. Oncotarget 7(38):61755–61763. https://doi.org/10.18632/oncotarget.11237
Kamps R, Brandão RD, Bosch BJVD, Paulussen ADC, Xanthoulea S, Blok MJ et al (2017) Next-generation sequencing in oncology: genetic diagnosis, risk prediction and cancer classification. Int J Mol Sci 18(2):308. https://doi.org/10.3390/ijms18020308
Kitajima S, Barbie DA (2018) RASA1/NF1-mutant lung cancer: racing to the clinic? Clin Cancer Res 24(6):1243–1245. https://doi.org/10.1158/1078-0432.CCR-17-3597
Lee CK, Wu YL, Ding PN, Lord SJ, Inoue A, Zhou C et al (2015) Impact of specific epidermal growth factor receptor (EGFR) mutations and clinical characteristics on outcomes after treatment with EGFR tyrosine kinase inhibitors versus chemotherapy in EGFR-mutant lung cancer: a meta-analysis. J Clin Oncol 33(17):1958–1965. https://doi.org/10.1200/JCO.2014.58.1736
Li H, Durbin R (2009) Fast and accurate short read alignment with Burrows–Wheeler transform. Bioinformatics 25(14):1754–1760. https://doi.org/10.1093/bioinformatics/btp324
Li H, Pan Y, Li Y, Li C, Wang R, Hu H et al (2013) Frequency of well-identified oncogenic driver mutations in lung adenocarcinoma of smokers varies with histological subtypes and graduated smoking dose. Lung Cancer 79(1):8–13. https://doi.org/10.1016/j.lungcan.2012.09.018
Lowder MA, Doerner AE, Schepartz A (2015) Structural differences between wild-type and double mutant EGFR modulated by third-generation kinase inhibitors. J Am Chem Soc 137(20):6456–6459. https://doi.org/10.1021/jacs.5b02326
Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N et al (2009) Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med 361(10):947–957. https://doi.org/10.1056/NEJMoa0810699
Morgillo F, Della Corte CM, Fasano M, Ciardiello F (2016) Mechanisms of resistance to EGFR-targeted drugs: lung cancer. ESMO Open 1(3):e000060. https://doi.org/10.1136/esmoopen-2016-000060
Newman AM, Bratman SV, Stehr H, Lee LJ, Liu CL, Diehn M et al (2014) FACTERA: a practical method for the discovery of genomic rearrangements at breakpoint resolution. Bioinformatics (Oxford, England) 30(23):3390–3393. https://doi.org/10.1093/bioinformatics/btu549
Paik PK, Arcila ME, Fara M, Sima CS, Miller VA, Kris MG et al (2011) Clinical characteristics of patients with lung adenocarcinomas harboring BRAF mutations. J Clin Oncol 29(15):2046–2051. https://doi.org/10.1200/JCO.2010.33.1280
Rosell R, Karachaliou N (2019) Co-mutations in EGFR driven non-small cell lung cancer. EBioMedicine 42:18–19. https://doi.org/10.1016/j.ebiom.2019.03.037
Sequist LV, Yang JC, Yamamoto N, O’Byrne K, Hirsh V, Mok T et al (2013) Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations. J Clin Oncol 31(27):3327–3334. https://doi.org/10.1200/JCO.2012.44.2806
Shepherd FA, Rodrigues Pereira J, Ciuleanu T, Tan EH, Hirsh V, Thongprasert S et al (2005) Erlotinib in previously treated non-small-cell lung cancer. N Engl J Med 353(2):123–132. https://doi.org/10.1056/NEJMoa050753
Singh M, Garg N, Venugopal C, Hallett R, Tokar T, McFarlane N et al (2015) STAT3 pathway regulates lung-derived brain metastasis initiating cell capacity through miR-21 activation. Oncotarget 6(29):27461–27477. https://doi.org/10.18632/oncotarget.4742
VanderLaan PA, Rangachari D, Mockus SM, Spotlow V, Reddi HV, Malcolm J et al (2017) Mutations in TP53, PIK3CA, PTEN and other genes in EGFR mutated lung cancers: correlation with clinical outcomes. Lung Cancer 106:17–21. https://doi.org/10.1016/j.lungcan.2017.01.011
Wu S-G, Chang Y-L, Yu C-J, Yang P-C, Shih J-Y (2016) The role of PIK3CA mutations among lung adenocarcinoma patients with primary and acquired resistance to EGFR tyrosine kinase inhibition. Sci Rep 6:35249. https://doi.org/10.1038/srep35249
Xu J, Wang J, Zhang S (2017) Mechanisms of resistance to irreversible epidermal growth factor receptor tyrosine kinase inhibitors and therapeutic strategies in non-small cell lung cancer. Oncotarget 8(52):90557–90578. https://doi.org/10.18632/oncotarget.21164
Zhao ZR, Lin YB, Ng CSH, Zhang R, Wu X, Ou Q et al (2019) Mutation profile of resected EGFR-mutated lung adenocarcinoma by next-generation sequencing. Oncologist 1:1. https://doi.org/10.1634/theoncologist.2018-0567
Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C et al (2011) Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol 12(8):735–742. https://doi.org/10.1016/S1470-2045(11)70184-X
Acknowledgements
This study was funded by a research Grant from the Postdoctoral Scientific Research Developmental Fund (Grant no. LBH-Q16143) provided by the Administration Office of Heilongjiang Postdoctoral Program, China, and a Special fund for clinical research from Wu Jieping medical foundation (Grant no. 320.6750.18050). Our thanks to all participants who consented to take part in this trial.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declared that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the Ethical Review Committee of Second Affiliated Hospital of Harbin Medical University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this retrospective of study formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Deng, LL., Gao, G., Deng, HB. et al. Co-occurring genetic alterations predict distant metastasis and poor efficacy of first-line EGFR-TKIs in EGFR-mutant NSCLC. J Cancer Res Clin Oncol 145, 2613–2624 (2019). https://doi.org/10.1007/s00432-019-03001-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-019-03001-2