
Abstract
Purpose
Epigenetic silencing of tumor suppressor genes is involved in early transforming events and has a high impact on colorectal carcinogenesis. Likewise, colon cancers that derive from chronically inflamed bowel diseases frequently exhibit epigenetic changes. But there is little data about epigenetic aberrations causing colorectal cancer in chronically inflamed tissue. The aim of the present study was to evaluate the aberrant gain of methylation in the gene promoters of VIM, TFPI2 and ITGA4 as putative early markers in the development from inflamed tissue via precancerous lesions toward colorectal cancer.
Methods
Initial screening of different cancer cell lines by using methylation-specific PCR revealed a putative colon cancer-specific methylation pattern. Additionally, a demethylation assay was performed to investigate the methylation-dependent gene silencing of ITGA4. The candidate markers were analyzed in colonic tissue specimens from patients with colorectal cancer (n = 15), adenomas (n = 76), serrated lesions (n = 13), chronic inflammation (n = 10) and normal mucosal samples (n = 9).
Results
A high methylation frequency of VIM (55.6 %) was observed in normal colon tissue, whereas ITGA4 and TFPI2 were completely unmethylated in controls. A significant gain of methylation frequency with progression of disease as well as an age-dependent effect was detectable for TFPI2. ITGA4 methylation frequency was high in precancerous and cancerous tissues as well as in inflammatory bowel diseases (IBD).
Conclusion
The already established methylation marker VIM does not permit a specific and sensitive discrimination of healthy and neoplastic tissue. The methylation markers ITGA4 and TFPI2 seem to be suitable risk markers for inflammation-associated colon cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colon cancer is one of the most frequent occurring cancers in the Western civilization. Furthermore, it is one of the leading causes of cancer-related deaths (Ferlay et al. 2010). One of the prevalent risk factors for developing colorectal cancer is inflammatory bowel diseases (IBD). Thus, patients with long-standing Crohn’s disease have a significantly elevated lifetime risk of developing colorectal cancer. As shown in a screening and surveillance study during a 17-year period, patients with long-standing Crohn’s disease developed cancer with increased risk depending on younger age at diagnosis, longer disease course and extent of the inflammation (Basseri et al. 2012). Similarly, the incidence rates of colorectal cancer are increased in patients with ulcerative colitis (Eaden et al. 2001). Particularly for risk groups like IBD patients, there is a need for defining risk markers for assessment of developing cancer. The mortality of colitis-associated and sporadic colorectal cancer (CRC) can be reduced significantly by frequent and regularly colorectal examination, which allows the early detection of premalignant adenomas and early-staged cancers (Center et al. 2009). The most effective screening method for colorectal cancer and the precancerous lesions is colonoscopy (Schoen et al. 2012). Yet the low compliance of patients has prompted the development of noninvasive screening tests. However, the vast majority of existing noninvasive screening tests, like the fecal occult blood test (FOBT), presents only low sensitivity and specificity, especially for precancerous lesions like adenoma (Hol et al. 2010).
In the past few years, it has become clear that abnormal hypermethylation of gene promoters and the associated loss of gene function is one of the early driving events of colonic carcinogenesis (Jones and Baylin 2007). Methylation of DNA occurs predominantly at the 5′-position of cytosines in the context of CG dinucleotides. In mammals, most of these dinucleotides are accumulated in so-called CpG Islands located in over 40 % of mammalian gene promoters. Methylation of the CpGs in gene promoters results in silencing of the respective gene. The finding of abnormal methylation of distinct genes like tumor suppressors due to carcinogenesis provides a new marker for early colon cancer detection (Lao and Grady 2011). Several abnormally methylated genes in colon cancer have been described recently. The aim of the present study was to identify and evaluate the benefit of a methylation marker panel for the early detection of colorectal cancer and its precancerous lesions considering that a large portion of colon cancers arise from chronic inflammation.
As putative risk markers for colitis-associated carcinogenesis, the methylation status of tissue factor pathway inhibitor (TFPI2), integrin alpha-4 (ITGA4) and vimentin (VIM) gene promoters was examined. The TFPI2 gene encodes a Kunitz-type serine proteinase inhibitor that protects the extracellular matrix of cancer cells from degradation and inhibits in vitro colony formation and proliferation. It is thought that loss of TFPI2 function could predispose cells toward a pro-invasive program, consistent with an important role for this protein in later stages of carcinogenesis (Glockner et al. 2009; Hahn et al. 2008).
The ITGA4 gene encodes the alpha-4 subunit of an integrin family member. Integrins are heterodimeric membranous receptor proteins consisting of two subunits, namely alpha and beta. They are receptors for VCAM1, whereas integrin alpha-4/beta-7 is a receptor for MADCAM1. Integrins have important functions in extracellular control of cell survival and differentiation via cell–cell interactions and cell–matrix communication. ITGA4 is a putative tumor suppressor because of its ability to control cell adhesion (Ausch et al. 2009).
The VIM gene encodes a protein constituent of intermediate filaments. Its expression is considered a classic marker of mesenchymal cells, such as fibroblasts; hence, VIM should not be expressed by normal colonic epithelium. Anyhow apparently it is being hypermethylated during colon carcinogenesis and already being used as a promising methylation marker (Chen et al. 2005). In the present study, VIM was analyzed for comparison purposes of the evaluated marker panel.
This work emphasizes the significance of methylation changes during carcinogenesis and evaluates the potential of different methylation markers for the early detection of CRC.
Materials and methods
Cell lines
Initial screening of ITGA4, TFPI2 and VIM promoter methylation was performed in cell lines LS174T, CaCo-2, Colo678, SW480, HT-29, HCT116, LS1034, HCEC, Colo357, HEK293, HeLa, HepG2, IGR-1, Jurkat, LNCaP, MCF7, MDA-MB231, Raji and SH-SY5Y. Cells were purchased from American Type Culture Collection and from DSMZ-German Collection of Microorganisms and Cell Cultures. LS174T, CaCo-2 and HCEC were obtained as generous gifts from A. M. Otto (Technical University of Munich, Germany), R. Brigelius-Flohé (German Institute of Human Nutrition (DIfE, Nuthetal, Germany), and the Nestlé Ltd. Research Centre (Lausanne, Switzerland), respectively. Cells were cultured according to protocols of the suppliers. Every cell line was tested negative for mycoplasma infection within 6 month before use.
Tissue samples
Colon tissue samples including 15 carcinomas, 76 adenomas, 13 serrated lesions and 9 normal colon tissue specimens from diverticulosis patients were obtained during colonoscopy and fresh-frozen. Additionally, ten chronically inflamed FFPE colon tissues from IBD patients were analyzed. Histologic findings of tissues are given in Table 1. The mean age of patients was 71.7 years, and 50.5 % of the subjects were male. The tissues were provided by the Division of Gastroenterology at the Maria Heimsuchung Caritas-Klinik Pankow (Berlin, Germany) and the Department of Medicine II, Division of Gastroenterology, University of Würzburg (Germany). The study was carried out in compliance with the Declaration of Helsinki. Written informed consent was received from participants prior to inclusion in the study. Permission for the study was given by the Ethics Commission of the University of Potsdam, Germany (Decision 14/2011).
DNA extraction and bisulfite conversion
Genomic DNA was extracted from cell pellets and from human tissue samples by use of the QIAamp DNA Mini Kit (Qiagen) according to the manufacturer’s protocol. For FFPE tissues, the QIAamp DNA FFPE tissue kit (Qiagen) was used. The DNA obtained from 2 × 106 cells was eluted in 100 µl ddH2O. Two different methods were used to convert the genomic DNA by bisulfite treatment. As described previously (12), 250 ng–2 µg DNA was denatured by NaOH (final concentration 0.3 mol/L) for 15 min at 37 °C. After that, 12 µl of 0.1 mol/L hydroquinone and 208 µl of 3.6 mol/L NaHSO3 (both freshly prepared) were added and incubated for 16 h at 55 °C. The bisulfite-converted DNA was purified using the Wizard DNA Clean-Up System (Promega) and eluted in 50 µl H2O. Desulfonation was carried out by addition of 5 µl 3 mol/L NaOH and incubation for 15 min at 37 °C. The DNA was precipitated by ethanol and resuspended in 50 µl H2O. In addition to this method, the EZ DNA Methylation Kit (Zymo Research) was used to modify the genomic DNA according to the manufacturer`s protocol.
Nested methylation-specific PCR (MSP)
Initially, MSP was performed in a 25-µl reaction volume containing 5 µl of bisulfite DNA as template, 1 U Dream Taq DNA polymerase (Thermo Scientific), 400 nmol/L forward and reverse primers, 0.1 mmol/L dNTPs, 1× Dream Taq Buffer, 4 mmol/L MgCl2 and H2O. As a positive control, 10 ng of EpiTect Control DNA (Qiagen, Hilden) was used. In a second nested PCR, 2 µl of the first amplicon was added to 23 µl reaction mix as above but with 400 nmol/L nested forward and reverse primers. Subsequently, the nested MSP products were analyzed on an agarose gel. Primer sequences and PCR conditions are listed in Supplementary Table ESM 1.
Demethylation assay with 5-aza-2′-deoxycytidine
In order to determine the inhibition of DNA methylation of the ITGA4-promoter, we treated the colon cancer cell line HCT116 with 5-aza-2′-deoxycytidine (5-aza-dC; Sigma-Aldrich). The cells were treated with final concentrations from 5, 10 and 15 µM 5-aza-dC, whereas PBS was used as solution control. The untreated cells were the negative control. After 96 h, the cells were harvested and frozen for further protein analysis.
Protein extraction and Western blot analysis
Briefly, the cell pellets were lysed in 200 µl RIPA buffer (50 mM Tris/HCl, 150 mM NaCl, 1 % Nonidet P-40, 0.5 % sodium deoxycholate, 0.1 % SDS in PBS) and 30-min incubation at 4 °C. Subsequently, the lysed cells were centrifugated at 10,000 rpm for 30 min and the supernatant was used for protein analysis.
For the Western blot analysis, 100-µg protein was used for each lane. The protein aliquots were separated on SDS-PAGE and subsequently transferred to PVDF membrane filters, followed by blocking with 5 % milk powder in TBST buffer. The membranes were probed with the primary antibody anti-ITGA4 (Epitomics, Burlingame) and anti-β-actin (Abcam, Cambridgeshire), reacted with the corresponding horseradish peroxidase-conjugated secondary antibody (Cell Signaling, Boston) and detected using a chemiluminescence reaction. The membranes were exposed to X-ray film to visualize the detected proteins of interest.
Statistics
The levels of significance between the disease-dependent groups were calculated by the software Prism 6 (Graphpad Software, La Jolla, USA) using Fisher’s exact test. Differences between the groups were considered significantly in case of p < 0.05.
Results
Methylation pattern of candidate markers in cell lines
Initially, the organ specificity of the candidate methylation markers was studied by analyzing the promoter methylation status of ITGA4, TFPI2 and VIM by MSP in a total of 19 cell lines. These cells included seven colon cancer cell lines and one normal colon epithelial cell line as well as eleven cell lines from different organs. Whereas the target genes were unmethylated in the normal colon cell line HCEC, they were consistently methylated in the analyzed colon cancer cells except for SW480 where VIM was unmethylated (Table 2). However, cell lines originating from different tissues exhibited a vastly heterogenic methylation profile. Accordingly, all of the examined gene promoters were unmethylated in cell lines HEK293 derived from embryonic kidney, HeLa from cervical carcinoma and SH-SY5Y from neuroblastoma. The other non-colon cell lines exhibited inconsistently methylated gene promoters of ITGA4, TFPI2 and VIM (Table 2). A representative MSP analysis of the VIM promoter is exemplarily shown (Fig. 1).

Verification of VIM gene promoter methylation in cell lines by MSP. PCR products of unmethylated (U) and methylated (M) VIM from sodium bisulfite-treated genomic DNA from cell lines are visualized by ethidium bromide staining. 1–6—analyzed cell lines as indicated; 7—positive methylated and unmethylated control DNA; 8—negative control; L—base length standard
Demethylation assay and reexpression of ITGA4
The methylation-dependent inhibition of TFPI2 gene expression has been shown already (Heller et al. 2008). In contrast, VIM is not expressed in colon tissue independently from the methylation status (Chen et al. 2005), but gains hypermethylation during carcinogenesis. In order to determine the methylation-dependent inhibition of the gene expression of ITGA4, we performed a demethylation assay using 5-aza-2′-deoxycytidine, a common demethylating agent. The methylation status of the treated cells was analyzed by MSP, and ITGA4 reexpression was investigated by Western blotting.
The ITGA4 promoter was fully methylated in the colon cancer cell line HCT116. After cell treatment with 0, 5, 10 and 15 µM 5-aza-2′-deoxycytidine, genomic DNA was isolated and prepared by bisulfite treatment. Subsequently, the methylation status of the ITGA4 promoter was analyzed by MSP. As expected, the treatment with 5-aza-2′-deoxycytidine (5-aza-dC) revealed demethylation of the ITGA4 promoter, which was shown by a PCR signal in the unmethylated MSP reaction (Fig. 2).

DNA methylation changes in the ITGA4-promoter after 5-aza-dC treatment. The methylation status of ITGA4 in HCT116 cells treated with 5, 10 and 15 µM 5-aza-dC for 96 h was analyzed by MSP. The non-treated control (neg.) and the solvent control with PBS (0 µM) displayed no detectable unmethylated signal. In vitro methylated and unmethylated control DNA (pos.) was used as positive control
The Western blot analysis of the protein lysate of the treated cells revealed a transcriptional and translational reactivation of ITGA4. We observed that the protein level of ITGA4 was increased with the 5-aza-dC treatment. The non-treated and solvent controls did not show any detectable ITGA4 protein appearance (Fig. 3). These results indicate that the methylation of the ITGA4 promoter directly mediates the transcriptional and translational silencing of ITGA4 in colon cancer cells.

Upregulation of ITGA4-gene expression after 5-aza-dC treatment. HCT116 cells are treated with 5 µM (3), 10 µM (4) or 15 µM (5) 5-aza-dC for 96 h resulting in reexpression of the ITGA4 protein. The untreated negative control (1) and the solvent control PBS (2) showed no detectable signal. The positive control (Raji cell lysate—6) displayed a strong signal. The protein β-actin is used as loading control
Methylation status of ITGA4, TFPI2 and VIM in normal, precancerous and carcinoma tissue
Aware of the uniform methylation status of ITGA4, TFPI2 and VIM in colon cancer cell lines, we analyzed a total of 123 colon biopsies from patients with different disease states. In the subset of normal controls, neither ITGA4 nor TFPI2 promoters were methylated (Table 1). Surprisingly, a methylated VIM promoter was already found in five out of nine (55.6 %) normal colon mucosa specimens.
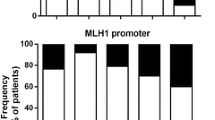
In inflamed tissue, methylation of the analyzed gene promoter regions was a common feature as well. The non-neoplastic mucosa samples of IBD patients showed relatively higher methylation levels in ITGA4 and TFPI2 than in normal colon mucosa samples (80 and 30 %, respectively) (Fig. 4a, b). ITGA4 methylation was significantly higher in inflamed than in normal tissue (p = 0.0007). The VIM promoter was methylated in 40 % of IBD-derived samples as well (Fig. 4c).

Fraction of samples with promoter methylation of the analyzed genes dependent of the histopathological features. The biomarkers have been analyzed in control and tumor samples by methylation-specific PCR (MSP). Bars represent the biopsies being methylated in a ITGA4; **p = 0.0017; ***p = 0.0007; ****p < 0.0001, b TFPI2; ***p = 0.0001; ****p < 0.0001 and VIMENTIN (c). IBD Inflammatory bowel disease, CRC colorectal carcinoma
Colon tissue samples from patients with serrated lesions and adenomas represented the precancerous subset. A significantly more frequent methylation of the ITGA4 promoter was observed in serrated lesions (69.2 %; p < 0.0001) as well as in adenomas (93.4 %; p < 0.0001) compared to the normal subset (Fig. 4a). Overall, a hypermethylated TFPI2 promoter has been detected less frequently than ITGA4 methylation in the precancerous subset (Table 1). A methylation of the TFPI2 promoter was found in 38.5 % of serrated biopsies and in 67.1 % of adenoma samples which was significantly more frequent compared to controls (p < 0.0001) (Fig. 4b). No significant increase in VIM methylation rates was found in the precancerous states as opposed to normal colon. The VIM gene exhibited promoter methylation in 30.8 and 75 % of serrated lesions and adenomas, respectively (Fig. 4c).
Additionally, a subset of colon carcinoma specimens consisting of UICC stages from I to IV revealed a highly frequent methylation of all observed gene promoters. Methylation rates of ITGA4 and TFPI2 were 93 and 93.3 %, respectively, in CRC biopsies (Fig. 4a, b). This represented a significant increase compared to the normal subset (p < 0.0001). Analysis of the VIM promoter revealed a methylation rate of 73.3 % (11/15) in CRC specimens.
An overview of the complete data set of tissue analysis is given in Table 1.
Influence of gender and age on candidate marker promoter methylation
A possible gender-specific change in methylation was analyzed in the three genes. The samples were equally distributed in male (49.5 %) and female (50.5 %). Regardless of the histopathological features, the gender-specific analysis of the MSP displayed a methylated ITGA4 promoter in 96.3 % of the male and in 90.9 % of female samples (Fig. 5a). The TFPI2 promoter was methylated in 75.9 % of male and 60 % of female specimens. Furthermore, the VIM promoter was methylated in 70.4 % of male and in 65.4 % of female samples. Overall, a less frequent methylation rate of all three genes was found in female samples. However, no significant difference was calculated.

Fraction of biopsies methylated in ITGA4, TFPI2 and VIM in dependence of gender (a) and age (b). Bars represent the biopsies being methylated in ITGA4, TFPI2 and VIM, respectively (****p < 0.0001)
Age is an important risk factor for the development of CRC, and aging colonic mucosa exhibits beside a genome-wide hypomethylation a locus-specific hypermethylation as well. In order to test a possible link between age- and site-specific gain of methylation, the obtained results from the different tissue samples were analyzed in an age-dependent manner. Therefore, the patients were divided into two populations. The group “<71 a” (n = 64) was defined as patients younger than the average age at sampling point. Accordingly, the group “>71 a” (n = 50) was defined as patients older than the average age at sampling point. The methylation level of ITGA4 was almost similar in the group “<71 a” with 89.1 % and in the older group “>71 a” with 86 % (Fig. 5b). The methylation level of VIM decreased slightly in the older subset where 62 % of the biopsies exhibited VIM promoter methylation compared with 71.9 % of the younger group. These differences were not statistically significant. Thus, changes in methylation frequency of the gene promoters of ITGA4 and VIM were not age-dependent. Interestingly, the methylation levels of TFPI2 varied significantly between the two populations (p < 0.0001). A methylated TFPI2 promoter was found in 72 % of the older subset versus 51.6 % in the younger group (Fig. 5b).
Combination of methylation markers ITGA4 and TFPI2 in tissue samples
In order to define the minimal yet best-informative methylation marker panel, we combined the results of the three genes ITGA4, TFPI2 and VIM. As expected, an increased hypermethylation of all three gene markers was observed in sporadic tumors, adenomas and serrated lesions, as well as in IBD samples. However, we decided to use only ITGA4 and TFPI2 for a putative methylation marker panel. Based on the findings of methylated VIM promoters in normal controls, the methylation analysis of this gene appeared to be more prone for false-positive results.
Accordingly, the analyzed MSP results revealed in none of the normal control samples neither a methylated ITGA4 nor a TFPI2 promoter (Fig. 6). In contrast, tissue samples derived from patients with IBD were in 9/10 cases methylated at least in one of the analyzed genes (90 %), whereas in eight out of the ten cases, one of the analyzed genes was unmethylated as well (Table 1). Both, ITGA4 and TFPI2, were methylated in only two IBD samples (p = 0.0455). Analysis of the serrated lesions revealed at least two genes methylated in three serrated lesions (23 %; p = 0.0275). In adenomas, the methylated proportion of at least one gene was 93.4 % of the adenomas (p < 0.0001). All of the two genes were methylated in 90.8 % of the adenoma samples. Most importantly, all of the CRC samples (100 %) were methylated in at least one gene (p < 0.0001). Even 86.7 % of CRC tissues revealed a methylated promoter in both analyzed genes (p < 0.0001).

Fraction of samples with promoter methylation of the analyzed genes ITGA4 and TFPI2 dependent of the histopathological features. The biomarker panel has been analyzed in control and tumor samples by methylation-specific PCR (MSP). Bars represent the biopsies being methylated in ITGA4, TFPI2 and VIM. IBD Inflammatory bowel disease (*p < 0.05; **p < 0.01); serrated lesions (*p < 0.05), adenoma (****p < 0.0001), CRC colorectal carcinoma (****p < 0.0001)
Discussion
Colon cancer is characterized by the accumulation of genetic and epigenetic alterations during carcinogenesis. By detecting these molecular changes in precancerous and early cancerous stages, the mortality rates of colon cancer can be reduced significantly (Bretthauer 2010; Jemal et al. 2010; Rabeneck et al. 2010; Zauber et al. 2012). In order to assess the suitability of frequently methylated putative tumor suppressors as markers for the early detection of colon cancer and its precursors, we evaluated the aberrantly methylated genes ITGA4, TFPI2 and VIM in colon tissues of different disease stages. Previously, several studies have demonstrated the high potential of the selected genes for the early detection of colon carcinogenesis (Ausch et al. 2009; Chen et al. 2005; Glockner et al. 2009).
In this study, the initial finding of colon cancer-specific hypermethylation of ITGA4, TFPI2 and VIM in cell lines was indicative for the suitability of all three genes as possible methylation markers in colon carcinogenesis. Correspondingly, the actively transcribed genes ITGA4 and TFPI2 were unmethylated in the normal colon cell line HCEC as expected. However, no VIM promoter methylation was detected in HCEC as well, although the VIM gene is transcriptionally silent in colonic epithelial cells.
In contrast, we were able to show a methylation-dependent silencing of the ITGA4 promoter in colon cancer cells. After treatment with the DNMT inhibitor 5-aza-2′-deoxycytidine, a demethylation of the ITGA4 promoter and a reexpression of the ITGA4 protein could be observed. This data prove DNA methylation to be the responsible mechanism for epigenetic gene silencing of ITGA4, which is frequently seen in colorectal carcinogenesis. These findings support our assumption that ITGA4 promoter hypermethylation appears to be a suitable marker for colon cancer detection.
Based on these findings, we analyzed human colon biopsies of different histological stages. All three candidate markers revealed high methylation rates in colon cancer and adenoma tissue. The already established methylation marker VIM appeared to be relatively common methylated in CRC and adenoma tissue. Several studies have been published reporting quite diverse sensitivities of CRC detection by VIM methylation analysis, ranging from 38 to 81 % (Ahlquist 2010; Ahlquist et al. 2008; Carmona et al. 2013). In the present work, VIM showed an intermediate value in relation to this range. Thereby, it represented the lowest sensitivity for CRC detection obtained among the three markers when evaluated individually (73.3 %). However, VIM appears to be minor suitable for colon cancer detection since we found high methylation rates throughout all histologic states including normal colon mucosa. The consequence is low specificity for the detection of neoplastic and pre-neoplastic lesions. Nevertheless, several studies have reported lower VIM methylation rates in normal controls ranging from 0 to 12 % (Baek et al. 2009; Itzkowitz et al. 2007). This discrepancy may be explained by the use of mucosal samples from diverticulosis patients as normal controls in our study. Although these tissue samples had a normal appearing histology, we cannot exclude possible inflamed regions within the biopsies causing a hypermethylated VIM promoter.
However, the additionally analyzed gene promoters of ITGA4 and TFPI2 did not show any methylation in the control samples. Levels of ITGA4 methylation in CRC samples were prominently high and could be used to significantly discriminate advanced adenoma and carcinoma from normal mucosa at the tissue level. Interestingly, serrated lesions and adenoma tissue samples showed methylation levels as high as carcinoma tissue, making ITGA4 methylation a robust biomarker. Unexpectedly, the non-neoplastic inflamed tissue samples exhibited a high ITGA4 methylation rate as well.
Additionally, the TFPI2 methylation levels were significantly elevated in CRC and adenoma tissue. Although the analysis of the methylation data revealed an age-dependent increase in the proportion of methylated biopsies in TFPI2, it became clear that the putative methylation markers ITGA4 and TFPI2 appeared to be methylated early during colorectal carcinogenesis and therefore are valuable markers for early detection of neoplastic lesions.
Importantly in inflamed tissue-derived biopsies, the hypermethylation of the analyzed gene promoter regions was a common feature as well. Consistent findings have been made in many other chronic inflammation conditions like Barrett’s esophagus or H. pylori infection of the stomach (Hahn et al. 2008; Nakajima et al. 2006). Patients with chronic gastrointestinal inflammations have an elevated risk of developing colorectal cancer (Bernstein et al. 2001). A possible explanation for the high methylation rates is provided by the high level of oxidative stress in inflamed regions leading to recruitment of DNA methyltransferase 1 (DNMT1) to the damaged chromatin regions and subsequent methylation of the DNA (Foran et al. 2010). Furthermore, it has been shown that proinflammatory factors like interferon gamma are able to induce the expression of DNMT3b leading to higher levels of 5-methylcytidine (Kominsky et al. 2011). Additionally, TNF-alpha induces cyclooxygenase-2 (COX-2) expression subsequently leading to higher prostaglandin E2 (PGE2) levels. The eicosanoid PGE2 is known to activate DNMT3b expression as well and induces hypermethylation of gene promoters (Xia et al. 2012). It has also been proposed that unrepaired inflammation-mediated halogenated DNA damage products can mimic 5‑methylcytosine due to their high affinity for methyl-binding proteins and ability to induce methylation of the daughter strand after DNA replication, leading to the establishment and propagation of aberrant methylation (Valinluck and Sowers 2007).
Generally, altered DNA methylation seems to be a result of chronic inflammation and not of acute inflammation (Niwa et al. 2010). For that reason, the duration of inflammation is an important risk factor for the development of CRC (Bernstein et al. 2001). In IBD tissue, it seems that hypermethylation of certain genes precedes dysplasia and neoplastic changes. Malignancy in IBD patients originates in precursor cells localized in or nearby the dysplastic mucosa (Grivennikov et al. 2010; Hartnett and Egan 2012; Itzkowitz and Yio 2004). However, the molecular events contributing to sporadic CRC, as mutations in WNT or EGFR signaling and methylation of CIMP genes, are considered to be different in inflammation-associated CRC (Samowitz et al. 2007). In detail, the timing and the frequency of epigenetic aberrations are altered by the underlying inflammatory process (Feagins et al. 2009). Thus, the methylation frequency of genes like O6-methylguanine DNA methyltransferase (MGMT), human mutL homolog 1 (hMLH1) and P16 was relatively low in IBD-associated cancers compared to sporadic neoplasia (Mikami et al. 2007). However, the methylation of other genes like estrogen receptor (ER), runt-related transcript factor-3 (RUNX3) and methylated-in-tumor-1 (MINT1) seems to occur more frequent in IBD patients with neoplasia (Fujii et al. 2005; Garrity-Park et al. 2010). These findings might explain the inconsistent methylation frequencies in IBD tissue and precancerous tissues like serrated lesions in our study.
A major drawback in this study is the lack of information about the duration of inflammation in the colitis patients. Therefore, it is difficult to correlate the disease duration and the methylation frequency of ITGA4, TFPI2 and VIM. However, we assume that ulcerative colitis as a chronic disease with heavy impairments existed for several years at the time of surgery. Further analysis regarding the correlation of methylation frequencies in IBD-associated carcinogenesis is needed.
Nonetheless, biomarkers like the three genes examined in this study may be helpful as risk markers for the prognosis of IBD patients to develop CRC; especially, the high sensitivity of ITGA4 for precancerous lesions makes it attractive as potential risk marker. Furthermore, the combination with TFPI2 methylation analysis, which showed elevated methylation rates with progression of disease, seemed to lead to an increase in specificity with minor decrease in sensitivity for detection of CRC and its precursors. Apparently, both methylation markers were methylated in a small subset of IBD samples, which was not depending on the severity and extent of the inflammation. Although this study was limited to a small group of IBD samples, we propose that TFPI2 and ITGA4 methylation could serve as possible risk markers for the development of IBD-related colorectal cancer. For this purpose, it will be necessary to test these biomarkers in studies extended to larger cohorts of IBD patients to confirm the robustness of the findings. Consequently, this could improve the early diagnosis of high-risk patients with IBD when assessed in non-neoplastic tissues obtained by screening colonoscopy. A noninvasive stool-based test might improve compliance with surveillance, which is currently poor, even among high-risk patients. Algorithms incorporating stool DNA as a complement to colonoscopy could potentially lengthen the interval between surveillance examinations in marker-negative patients, which could also reduce the high cost of surveillance endoscopy. Conversely, a patient with a positive stool DNA test may benefit from colonoscopy at shorter surveillance intervals. The tissue study based on well-matched cases and controls showed that methylation markers are highly discriminant for IBD.
Besides already established methylation markers like mSEPT9 (Payne 2010), there is a growing interest in new biomarkers for the early colon cancer detection (Nibbe and Chance 2009). Nevertheless, a sensitivity of 100 % will be practically impossible to reach by using methylation markers solely, because a subset of CRCs has low level or no detectable hypermethylated genes. Therefore, it will be necessary to combine methylation markers with alternative markers, like mutational DNA markers, as already proposed for other cancers (Cheon and Orsulic 2014). Additionally, RNA expression studies in colorectal cancer tissue revealed useful diagnostic markers like ARNTL2 and SERPINE1 (Mazzoccoli et al. 2012). Furthermore, it should be noticed that the detection of markers in precancerous lesions requires highly sensitive techniques. We recently introduced an ultrasensitive platform for the detection of known and unknown gene mutations in stool samples (Gerecke et al. 2013). An adaptation of this technique for detecting methylation could be used for sensitive methylation detection. For the purpose of a noninvasive screening in the future, the detection limits of methylation events should be evaluated equally in body fluids. A joint analysis of mutation and methylation markers for early detection of neoplastic diseases in body fluids like feces is desirable.
Conclusion
In conclusion, the gene methylation of ITGA4 and TFPI2 is an early and frequent event in precancerous and cancerous lesions of the colon and rectum. Furthermore, this methylation occurs in colon tissue from patients with chronic inflammation and was not detected in any normal colon samples. Finally, the methylation of ITGA4 and TFPI2 promoters is associated with a phenotypic down-regulation of these gene products. These factors make the ITGA4 and TFPI2 methylation a feasible epigenetic marker for early detection of CRC- and IBD-related cancer and may be useful for CRC screening in the future.
We have reported for the first time that VIM methylation was detected in normal colon tissue and therefore is not acceptable as specific early detection marker for colorectal neoplasia.
References
Ahlquist DA (2010) Molecular detection of colorectal neoplasia. Gastroenterology 138:2127–2139
Ahlquist T et al (2008) Gene methylation profiles of normal mucosa, and benign and malignant colorectal tumors identify early onset markers. Mol Cancer 7:94
Ausch C et al (2009) Comparative analysis of PCR-based biomarker assay methods for colorectal polyp detection from fecal DNA. Clin Chem 55:1559–1563
Baek YH, Chang E, Kim YJ, Kim BK, Sohn JH, Park DI (2009) Stool methylation-specific polymerase chain reaction assay for the detection of colorectal neoplasia in Korean patients. Dis Colon Rectum 52:1452–1459 (discussion 1459–1463)
Basseri RJ et al (2012) Colorectal cancer screening and surveillance in Crohn’s colitis. J Crohns Colitis 6:824–829
Bernstein CN, Blanchard JF, Kliewer E, Wajda A (2001) Cancer risk in patients with inflammatory bowel disease: a population-based study. Cancer 91:854–862
Bretthauer M (2010) Evidence for colorectal cancer screening. Best Pract Res Clin Gastroenterol 24:417–425
Carmona FJ et al (2013) DNA methylation biomarkers for noninvasive diagnosis of colorectal cancer. Cancer Prev Res (Phila) 6:656–665
Center MM, Jemal A, Ward E (2009) International trends in colorectal cancer incidence rates. Cancer Epidemiol Biomark Prev 18:1688–1694
Chen WD et al (2005) Detection in fecal DNA of colon cancer-specific methylation of the nonexpressed vimentin gene. J Natl Cancer Inst 97:1124–1132
Cheon DJ, Orsulic S (2014) Ten-gene biomarker panel: a new hope for ovarian cancer? Biomark Med 8:523–526
Eaden JA, Abrams KR, Mayberry JF (2001) The risk of colorectal cancer in ulcerative colitis: a meta-analysis. Gut 48:526–535
Feagins LA, Souza RF, Spechler SJ (2009) Carcinogenesis in IBD: potential targets for the prevention of colorectal cancer. Nat Rev Gastroenterol Hepatol 6:297–305
Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM (2010) Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 127:2893–2917
Foran E, Garrity-Park MM, Mureau C, Newell J, Smyrk TC, Limburg PJ, Egan LJ (2010) Upregulation of DNA methyltransferase-mediated gene silencing, anchorage-independent growth, and migration of colon cancer cells by interleukin-6. Mol Cancer Res 8:471–481
Fujii S et al (2005) Methylation of the oestrogen receptor gene in non-neoplastic epithelium as a marker of colorectal neoplasia risk in longstanding and extensive ulcerative colitis. Gut 54:1287–1292
Garrity-Park MM, Loftus EV Jr, Sandborn WJ, Bryant SC, Smyrk TC (2010) Methylation status of genes in non-neoplastic mucosa from patients with ulcerative colitis-associated colorectal cancer. Am J Gastroenterol 105:1610–1619
Gerecke C, Mascher C, Gottschalk U, Kleuser B, Scholtka B (2013) Ultrasensitive detection of unknown colon cancer-initiating mutations using the example of the Adenomatous polyposis coli gene. Cancer Prev Res (Phila) 6:898–907
Glockner SC et al (2009) Methylation of TFPI2 in stool DNA: a potential novel biomarker for the detection of colorectal cancer. Cancer Res 69:4691–4699
Grivennikov SI, Greten FR, Karin M (2010) Immunity, inflammation, and cancer. Cell 140:883–899
Hahn MA et al (2008) Methylation of polycomb target genes in intestinal cancer is mediated by inflammation. Cancer Res 68:10280–10289
Hartnett L, Egan LJ (2012) Inflammation, DNA methylation and colitis-associated cancer. Carcinogenesis 33:723–731
Heller G et al (2008) Genome-wide transcriptional response to 5-aza-2′-deoxycytidine and trichostatin a in multiple myeloma cells. Cancer Res 68:44–54
Hol L et al (2010) Screening for colorectal cancer: randomised trial comparing guaiac-based and immunochemical faecal occult blood testing and flexible sigmoidoscopy. Gut 59:62–68
Itzkowitz SH, Yio X (2004) Inflammation and cancer IV. Colorectal cancer in inflammatory bowel disease: the role of inflammation. Am J Physiol Gastrointest Liver Physiol 287:G7–17
Itzkowitz SH et al (2007) Improved fecal DNA test for colorectal cancer screening. Clin Gastroenterol Hepatol 5:111–117
Jemal A, Siegel R, Xu J, Ward E (2010) Cancer statistics, 2010. CA Cancer J Clin 60:277–300
Jones P, Baylin S (2007) The epigenomics of cancer. Cell 128:683–692
Kominsky DJ et al (2011) An endogenously anti-inflammatory role for methylation in mucosal inflammation identified through metabolite profiling. J Immunol 186:6505–6514
Lao VV, Grady WM (2011) Epigenetics and colorectal cancer. Nat Rev Gastroenterol Hepatol 8:686–700
Mazzoccoli G et al (2012) ARNTL2 and SERPINE1: potential biomarkers for tumor aggressiveness in colorectal cancer. J Cancer Res Clin Oncol 138:501–511
Mikami T et al (2007) Low frequency of promoter methylation of O6-methylguanine DNA methyltransferase and hMLH1 in ulcerative colitis-associated tumors: comparison with sporadic colonic tumors. Am J Clin Pathol 127:366–373
Nakajima T et al (2006) Higher methylation levels in gastric mucosae significantly correlate with higher risk of gastric cancers. Cancer Epidemiol Biomark Prev 15:2317–2321
Nibbe RK, Chance MR (2009) Approaches to biomarkers in human colorectal cancer: looking back, to go forward. Biomark Med 3:385–396
Niwa T et al (2010) Inflammatory processes triggered by Helicobacter pylori infection cause aberrant DNA methylation in gastric epithelial cells. Cancer Res 70:1430–1440
Payne SR (2010) From discovery to the clinic: the novel DNA methylation biomarker (m)SEPT9 for the detection of colorectal cancer in blood. Epigenomics 2:575–585
Rabeneck L, Paszat LF, Saskin R, Stukel TA (2010) Association between colonoscopy rates and colorectal cancer mortality. Am J Gastroenterol 105:1627–1632
Samowitz WS, Slattery ML, Sweeney C, Herrick J, Wolff RK, Albertsen H (2007) APC mutations and other genetic and epigenetic changes in colon cancer. Mol Cancer Res 5:165–170
Schoen RE et al (2012) Colorectal-cancer incidence and mortality with screening flexible sigmoidoscopy. N Engl J Med 366:2345–2357
Valinluck V, Sowers LC (2007) Inflammation-mediated cytosine damage: a mechanistic link between inflammation and the epigenetic alterations in human cancers. Cancer Res 67:5583–5586
Xia D, Wang D, Kim SH, Katoh H, DuBois RN (2012) Prostaglandin E2 promotes intestinal tumor growth via DNA methylation. Nat Med 18:224–226
Zauber AG et al (2012) Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med 366:687–696
Acknowledgments
This work was supported by the Foundation for Pathobiochemistry and Molecular Diagnostics, German Society for Clinical Chemistry and Laboratory Medicine e. V. (DGKL; Bonn, Germany) (grant to B.S.). Funding was restricted to personnel and non-personnel costs. M. Otto, R. Brigelius-Flohé and the Nestlé Ltd. Research Centre are acknowledged for providing cell lines LS174T, Caco-2 and HCEC, respectively. Thanks are given to Monika Haseloff for technical assistance.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Additional information
Christian Gerecke and Bettina Scholtka have contributed equally to this work.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Gerecke, C., Scholtka, B., Löwenstein, Y. et al. Hypermethylation of ITGA4, TFPI2 and VIMENTIN promoters is increased in inflamed colon tissue: putative risk markers for colitis-associated cancer. J Cancer Res Clin Oncol 141, 2097–2107 (2015). https://doi.org/10.1007/s00432-015-1972-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00432-015-1972-8