
Abstract
The SARS-CoV-2 virus has infected more than 235 million people since it was accepted as a pandemic in March 2020. Although a milder disease is seen in the pediatric age group, the extent of lung damage and its long-term effects are still unknown. In this study, persistent respiratory symptoms and pulmonary function tests were investigated in children with COVID-19. Fifty children with a confirmed diagnosis of COVID-19 were included in the study. Patients were evaluated for ongoing respiratory symptoms and pulmonary function tests 3 months after infection. Patients with and without persistent symptoms were compared in terms of demographic, clinical, laboratory, and radiological characteristics and also disease severity. Three months after infection, persistent respiratory symptoms were found to be present in 28% of patients; cough, chest pain and tightness, dyspnea, and exertional dyspnea were the most common symptoms. Three patients had an obstructive deficit, and one had a restrictive deficit. Four patients had impaired diffusing capacity of the lungs for carbon monoxide (DLCO). A significant decrease in FEV1/FVC and an increase in lung clearance index were found in the patients with persistent respiratory symptoms. Persistent respiratory symptoms were present in 50% of patients who had severe disease and 12.5% with non-severe disease. DLCO was also significantly lower in the severe disease group.
Conclusions: Our study suggests that the persistence of respiratory symptoms is not related to the severity of acute COVID-19 in children. The inflammatory process due to COVID-19 may continue regardless of its severity, and consequently, peripheral airways may be affected.
What is Known: • As compared with adults, children with COVID-19 exhibit a milder disease course and lower mortality rates. However, due to the lack of follow-up studies on children, the long-term effects of their contracting the disease are unknown. | |
What is New: • Although COVID-19 has been thought to have a milder course in children, respiratory system symptoms persist in approximately 30% of patients 3 months after infection. The persistent respiratory symptoms suggest that the inflammatory process due to COVID-19 may continue in some children, even if the clinical findings at admission are not severe, and that the peripheral airways may be affected accordingly. |
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection arose in Wuhan, China, in December 2019; spread rapidly across the world; and was declared a global pandemic in March 2020 [1]. Over 235 million confirmed cases and 4.7 million COVID-19-related deaths have been reported by the World Health Organization (WHO). The course of the disease, its effects on chronic diseases and mortality, and its long-term complications have become a global concern.
As compared with adults, children exhibit a milder disease course and lower mortality rates [2, 3]. However, due to the lack of follow-up studies on children, the long-term effects of them contracting the disease are unknown. Over time, coronavirus pneumonia (severe acute respiratory syndrome [SARS] and the Middle East respiratory syndrome coronavirus [MERS-CoV]) can cause lung damage and a decrease in pulmonary function tests (PFTs). Adult follow-up studies investigating the respiratory system and pulmonary function effects of SARS-CoV-2 have found restrictive ventilation defects; diffusion capacity impairment; decrease in total lung capacity; and various other symptoms, such as ongoing cough and shortness of breath [4,5,6]. Whether and how COVID-19 affects the developing lungs of children remains unknown.
In our clinic, respiratory symptoms were observed in the outpatient follow-up of some COVID-19 infection patients who had non-severe disease. This study aimed to evaluate persistent respiratory symptoms and PFTs of children diagnosed with COVID-19 and to investigate the factors associated with persistent respiratory symptoms.
Materials and methods
This is a retrospective study evaluating COVID-19 patients who followed up in our outpatient clinic and underwent PFT 3 months after discharge. The study was approved by the local ethics committee, and informed consent was obtained from all subjects and their parents (No: 2020.12.213).
Study group
Patients aged 5–18 years who were hospitalized with a confirmed SARS-CoV-2 infection between May 15 and August 1, 2020, and followed up at our clinic were included in the study. Patients were evaluated for ongoing respiratory symptoms and PFTs 3 months after discharge.
There were no patients with acute respiratory distress syndrome, sepsis, septic shock, or other conditions that would normally require the provision of life-sustaining therapies such as mechanical ventilation (invasive or non-invasive) or vasopressor therapy in the study group. So, the patients were classified into two severity groups based on WHO classification [7]:
-
1.
Non-severe disease: fever, myalgia, and upper respiratory tract infection symptoms such as cough, sneezing, sore throat, and rhinorrhea and pneumonia findings on the chest x-ray/CT with normal oxygen saturation on room air and normal respiratory rate.
-
2.
Severe disease: oxygen saturation < 90% on room air or respiratory rate ≥ 60 breaths/min in children < 2 months old; ≥ 50 in children 2–11 months old; ≥ 40 in children 1–5 years old; and > 30 breaths/min in children > 5 years old or signs of severe respiratory distress (accessory muscle use, grunting, central cyanosis, feeding difficulties).
Further comparisons in terms of demographic, clinical, and laboratory characteristics were performed between non-severe and severe groups. Patients with acute upper respiratory tract infection in the 2 weeks before the study and known comorbid diseases (chronic respiratory diseases, neurodevelopmental diseases, etc.) were excluded.
PFTs
Pulmonary function tests were performed using the Quark PFT (COSMED, Rome, Italy) at the 3-month follow-up. Forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and forced expiratory flow during the middle half of FVC (FEF25–75) were measured by spirometry and the FEV1/FVC ratio calculated. Results were expressed as a percentage of predicted values [8, 9]. Lung clearance index (LCI) was measured using the multiple breath nitrogen washout (N2MBW) technique. Three tests were performed with the mean result of at least two acceptable tests recorded. The standard procedure in our laboratory is to perform LCI before spirometry [10]. Diffusion capacity of the lung for carbon monoxide (DLCO) and total lung capacity (TLC) were measured using the single-breath test. The hemoglobin value was also taken to correct the DLCO. DLCO and TLC were expressed as percentages of predicted normal values [11]. All measurements were performed according to the American Thoracic Society and European Respiratory Society (ERS/ATS) consensus criteria [9,10,11]. An obstructive ventilatory defect is defined by a reduced FEV1/FVC ratio below the 5th percentile of the predicted value. A restrictive ventilatory defect is characterized by a reduction in TLC below the 5th percentile of the predicted value and a normal FEV1/FVC [12].
Chest CT
The chest CTs were performed on admission and evaluated by an experienced (15 years of experience in chest imaging and 5 years of experience in pediatric chest imaging) pediatric radiologist blinded to the clinical data. The distribution of lung opacities was reported as central (predominantly the inner 2/3 of the lungs) and peripheral (predominantly 1/3 outer region of the lung), or peribronchial. The CT findings were evaluated in terms of the presence of ground-glass opacities (GGOs), accompanying consolidation, pure consolidation, nodule, bronchial wall thickening, curvilinear opacities, lymphadenopathy, and pleural effusions. A semi-quantitative lung severity score was used to assess lung involvement, with each of the five lung lobes scored visually on a scale from 0 to 5, as follows: (0) no involvement, (1) minimal (1–25%), (2) mild (26–50%), (3) moderate (51–75%), and (4) severe (76–100%). The total CT score was the sum of the lobar scores and was rated between 0 and 20 [13].
Statistical analysis
The IBM SPSS Statistics 21.0 program was used for statistical analysis. The Kolmogorov–Smirnov/Shapiro–Wilk test was applied to test the normal distribution of the numerical variables, which were presented as mean (± standard deviation) and median (minimum–maximum). Pearson χ2 and Fisher’s exact χ2 tests were used for categorical data. The two independent samples t-test and Mann–Whitney U test were used for group comparisons. Univariate and multivariate logistic regression were used to determine predictors of persistent respiratory symptoms. The significance level was accepted as 0.05 for all hypotheses.
Results
Patient characteristics
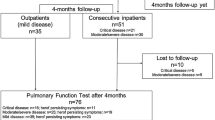
A total of 70 COVID-19 pediatric patients were evaluated in the third month after infection; 20 were excluded (14 with comorbid diseases and six due to inability to perform all PFTs). A flowchart showing how the patients were selected and grouped for the study is presented in Fig. 1. The median age of 50 patients included in the study was 15 (8–18) years, and 56% were male. The demographic and clinical characteristics of COVID-19 patients at 3 months after infection are presented in Table 1.

Patient selection and grouping for the study
The respiratory symptoms were present in 14 (28%) patients; common symptoms were dyspnea (35.7%), exertional dyspnea (35.7%), dry cough (21.4%), and chest pain and tightness (21.4%), The physical examinations and chest x-rays of all patients were normal. Four patients who did not have respiratory symptoms at active infection stated respiratory symptoms at follow-up. One of these patients was asymptomatic; two had a fever; and one had myalgia, headache, and weakness on admission.
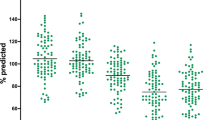
Spirometry and LCI measurement were performed in 50; DLCO was performed in 40 patients. Three patients had obstructive deficit (FEV1/FVC < 80%) and one patient had restrictive deficit (FVC < 80% and TLC < 80%). Four patients had impaired DLCO.
Comparison of clinical characteristics and PFTs in patients with and without persistent respiratory symptoms
When the age, gender, and BMI for the groups with and without persistent respiratory symptoms at 3 months were compared, no statistically significant difference was found (p > 0.05). Also, in both these groups, no significant difference was observed between the rates of respiratory symptoms (p = 0.24) and severe disease (p = 0.09) on admission. From the laboratory data, the only significant difference concerned the lymphocyte count in the group with respiratory symptoms, which was lower than among those patients without these symptoms (p < 0.05). There was no significant difference between the two groups in terms of the frequency of lobe involvement score (p > 0.05), total lung severity score (p = 0.28), or the rate of bilateral lung disease (p = 0.60) by CT. When the PFTs were compared, there was a significantly lower FEV1/FVC and higher LCI among the patients with respiratory symptoms (p < 0.05). DLCO measurements were performed in a total of 40 patients, 12 with respiratory symptoms and 24 without, with similar results (p = 0.88) (Table 2). The association of factors (age, gender, BMI, severe disease, laboratory data, bilateral lung disease) with persistent respiratory symptoms was examined by univariable and multivariable logistic regression. In univariable analysis, the lymphocyte count and elevation of d-dimer were associated with respiratory symptoms. In multiple univariable analysis, no risk factors associated with persistent respiratory symptoms were detected.
Comparison of clinical characteristics and PFTs in patients with severe and non-severe disease
There was a history of severe disease in 10 (20%) of the 50 patients. Seven (14%) patients required supplemental oxygen. The demographic, laboratory (except platelet count), and radiological data of the severe disease and non-severe disease patients were similar (p > 0.05). The platelet counts were significantly lower in the patients with severe disease.
Persistent respiratory symptoms were reported in 50% of patients with severe disease and 12.5% of patients with non-severe disease, and there was not a statistically significant difference between these two groups (p = 0.09). The LCI was similar in both the severe and non-severe disease groups (p = 0.89), while DLCO was significantly lower in the severe disease group (p < 0.05). DLCO was impaired in 30% of the patients in patients with severe disease (Table 3.)
Discussion
According to the results of this study, approximately 30% of children with COVID-19 infection have respiratory symptoms at 3-month follow-up; moreover, these patients have a higher LCI than asymptomatic patients. Abnormal PFTs were found in 14% and impaired diffusing capacity in 30% of patients. In addition, diffusion capacity was significantly lower in children who had severe disease.
Most of the studies in children with COVID-19 have focused on epidemiological features, clinical characteristics, treatment strategies, and the role of children in disease transmission [14,15,16,17,18]. These studies showed that, notwithstanding comorbid conditions and underlying diseases, children had a milder disease compared to adults. However, a potentially life-threatening hyperinflammatory condition associated with the SARS-CoV-2, named “multisystem inflammatory syndrome in children” (MIS-C), has been increasingly reported [19, 20]. Since the pathogenesis and facilitating factors of MIS-C have not been understood yet, the follow-up of children with COVID-19 is of great importance.
In a study evaluating 34 children with COVID-19 1 month after acute infection, clinic follow-up in 14 patients, and phone call follow-up in 20 patients, no symptoms were reported in phone call follow-up. However, pulmonary sequelae were detected in seven (50%) of the 14 patients (N = 3, spots or patches of opacities; N = 4, fibrosis). The fibrous stripes were detected in areas other than the original lesion by CT in some patients, which suggested the likelihood of continued effects of the disease on the lungs [21]. In our study, we found that 28% of the patients had respiratory symptoms 3 months after infection. Moreover, four patients who did not have respiratory symptoms at infection stated respiratory symptoms at follow-up. No significant difference was found between patients with and without respiratory symptoms at 3 months in terms of frequency of lobe involvement or total lung severity or the rates of bilateral lung disease on admission. We also identified higher FEV1/FVC and lower LCI in patients with respiratory symptoms. Our results support the hypothesis that the effects of COVID-19 on the lung may continue.
After viral pneumonia, long-term complications may be observed, such as prolonged cough, chronic bronchitis, asthma, and bronchiectasis, and result in respiratory dysfunction by causing obstructive and restrictive lung diseases [22]. The SARS-CoV-2 binds to the angiotensin-converting enzyme 2 receptor on the alveolar cell surface, damaging the integrity of the epithelium and disturbs microcirculation. In severe forms of the disease, alveolar gas diffusion is impaired due to diffuse alveolar damage. Moreover, increased airway inflammation and mucus plugs in the peripheral airways can cause impaired ventilation [23,24,25]. Evaluated with MBW, the LCI is a measurement that can be used to determine ventilation inhomogeneity in the peripheral airways. The increased LCI in patients with respiratory symptoms in our study suggests that the inflammatory process due to COVID-19 may continue in some children and that the peripheral airways may be affected accordingly, even in cases where the clinical findings on admission are not severe.
Lung function abnormalities, especially impaired diffusing capacity, can occur after severe infections. In a long-term follow-up study after the SARS infection, children were evaluated at 6 months with high-resolution CT and PFTs. Although none of the patients had respiratory symptoms, 34% had mild abnormalities on CT and 10.5% had PFT abnormalities. No difference was found in the PFTs of the patients with and without pulmonary sequelae on CT [26]. In a multicenter study of 103 adults with COVID-19, dyspnea with exertion was reported in approximately half of the subjects in the third month after discharge. Persistent GGO was detected in 25% of the subjects and parenchymal band in approximately 20% on CT. Despite the majority of subjects having values within the normal limits of PFTs, approximately 10% had FVC or FEV1 below lower limits of normal, while 24% had significantly decreased DLCO. Similar dyspnea scores and PFT measurements were found between the group with and without intensive care unit admission [27].
There are few studies evaluating pulmonary functions in children after COVID-19 infection. Bottino et al. followed 16 asymptomatic and mildly symptomatic pediatric patients prospectively for at least 30 days after COVID-19 infection, and none of the patients was found any abnormality in lung ultrasonography, airway resistance test, spirometry, and DLCO [28]. Vezir et al. reported 75 pediatric patients with COVID-19 who were classified according to clinical severity and evaluated with PFTs 1 to 3 months after the infection. Fifty-seven patients were evaluated with spirometry, and three patients with comorbid disease had impaired PFT (obstructive type deficit in 2 patients and restrictive type deficit in one patient). When the patients were grouped as asymptomatic/mild and moderate/severe/critical, spirometry measurements were found to be similar in both groups [29]. In our study, three patients had an obstructive deficit, three had impaired diffusion capacity, and one had restrictive type deficit and impaired diffusion capacity 3 months after infection whose no underlying disease. In addition, a significant decrease in diffusion capacity was found among patients with severe disease compared to non-severe disease. It is necessary to investigate the underlying pathophysiology of these results, which are different from other studies, and to plan studies for their long-term effects.
There were several limitations in this study. The first was its retrospective design and therefore limited number of patients. Second, no radiological evaluation with CT was performed 3 months after infection due to the risk from radiation exposure. Therefore, the radiological sequelae of the patients are not known, and no comparison has been made with PFTs. In addition, since the radiological examinations on admission may reflect the early stages of the disease, there may not be a significant difference among these data. Although we did not detect any difference in terms of d-dimer levels in patients with and without persistent respiratory symptoms, small pulmonary microthrombi could be present. Despite being a tertiary referral hospital, due to the inability to contact the patients who had been followed in our intensive care unit, these critically ill patients were not included in the study. This was another limitation of our study. If these patients were included, we might see the impact of disease severity on pulmonary function. In addition, the absence of a control group did not allow the comparison of lung functions with healthy children.
In conclusion, our study is of great importance in terms of showing persistent respiratory symptoms and impairment in lung functions in children with COVID-19. Although COVID-19 has been thought to have a milder course in children, the persistence of respiratory symptoms 3 months after acute infection suggests an ongoing inflammatory process. Additionally, the peripheral airways may be affected even if the clinical findings of disease on admission are not severe. The information gained here can guide future studies examining the effects of COVID-19 on a child’s lung and planning diagnostic investigations and preventive strategies.
Abbreviations
- BMI:
-
Body mass index
- CT:
-
Computed tomography
- DIC:
-
Disseminated intravascular coagulation
- DLCO:
-
Diffusion capacity of the lung for carbon monoxide
- FEF25–75 :
-
Forced expiratory flow during the middle half of FVC
- FEV1:
-
Forced expiratory volume in 1 s
- FRC:
-
Functional residual capacity
- FVC:
-
Forced vital capacity
- GGOs:
-
Ground-glass opacities
- LCI:
-
Lung clearance index
- MBW:
-
Multiple breath washout
- MERS-CoV:
-
The Middle East respiratory syndrome coronavirus
- MIS-C:
-
Multisystem inflammatory syndrome in children
- PFT:
-
Pulmonary function test
- SARS:
-
The severe acute respiratory syndrome
- SARS-CoV-2:
-
The severe acute respiratory syndrome coronavirus 2
- TLC:
-
Total lung capacity
- WHO:
-
World Health Organization
References
Zhu N et al (2020) A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med 382(8):727–733
Lu X et al (2020) SARS-CoV-2 infection in children. N Engl J Med 382(17):1663–1665
Dong Y et al (2020) Epidemiology of COVID-19 among children in China. Pediatrics 145(6)
Mo X et al (2020) Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J 55(6)
Huang Y et al (2020) Impact of coronavirus disease 2019 on pulmonary function in early convalescence phase. Respir Res 21(1):163
Daher A et al (2020) Follow up of patients with severe coronavirus disease 2019 (COVID-19): pulmonary and extrapulmonary disease sequelae. Respir Med 174:106197
World Health Organization (2020) COVID-19 clinical management: living guidance. 25 January 2021, World Health Organization
Quanjer PH et al (2012) Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J 40(6):1324–1343
Graham BL et al (2019) Standardization of spirometry 2019 update. An official american thoracic society and european respiratory society technical statement. Am J Respir Crit Care Med 200(8):p e70–e88
Robinson PD et al (2013) Consensus statement for inert gas washout measurement using multiple- and single- breath tests. Eur Respir J 41(3):507–522
Graham BL et al (2017) ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur Respir J 49(1)
Pellegrino R et al (2005) Interpretative strategies for lung function tests. Eur Respir J 26(5):948–968
Chung M et al (2020) CT Imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 295(1):202–207
Hoang A et al (2020) COVID-19 in 7780 pediatric patients: a systematic review. EClinicalMedicine 24:100433
Tsabouri S et al (2021) Risk factors for severity in children with coronavirus disease 2019: a comprehensive literature review. Pediatr Clin North Am 68(1):321–338
Sinaei R et al (2021) Why COVID-19 is less frequent and severe in children: a narrative review. World J Pediatr 17(1):10–20
Shen KL et al (2020) Updated diagnosis, treatment and prevention of COVID-19 in children: experts’ consensus statement (condensed version of the second edition). World J Pediatr 16(3):p 232–239
Cui X et al (2020) Children with coronavirus disease 2019: a review of demographic, clinical, laboratory, and imaging features in pediatric patients. J Med Virol 92(9):1501–1510
European Centre for Disease Prevention and Control (2020) Rapid risk assessment: paediatric inflammatory multisystem syndrome and SARS-CoV-2 infection in children. May 15, 2020. https://www.ecdc.europa.eu/en/publications-data/paediatric-inflammatory-multisystem-syndrome-and-sars-cov-2-rapid-risk-assessment
World Health Organization (2020) Multisystem inflammatory syndrome in children and adolescents with COVID-19. Published May 15, 2020. https://www.who.int/publicationsdetail/multisystem-inflammatory-syndrome-in-children-and-adolescents-withcovid-19. (accessed 5 Aug 2020)
Zhang C et al (2021) Pulmonary sequelae of pediatric patients after discharge for COVID-19: an observational study. Pediatr Pulmonol 56(5):1266–1269
Edmond K et al (2012) Long term sequelae from childhood pneumonia; systematic review and meta-analysis. PLoS ONE 7(2):e31239
Teo JTR, Abidin NH, Cheah FC (2020) Severe acute respiratory syndrome-coronavirus-2 infection: a review of the clinical-pathological correlations of Coronavirus disease-19 in children. Malays J Pathol 42(3):349–361
Bourgonje AR et al (2020) Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J Pathol 251(3):228–248
Wang F, Kream RM, Stefano GB (2020) Long-term respiratory and neurological sequelae of COVID-19. Med Sci Monit 26:e928996
Li AM et al (2004) Radiological and pulmonary function outcomes of children with SARS. Pediatr Pulmonol 38(6):427–433
Lerum TV et al (2021) Dyspnoea, lung function and CT findings 3 months after hospital admission for COVID-19. Eur Respir J 57(4)
Bottino I et al (2021) Can asymptomatic or non-severe SARS-CoV-2 infection cause medium-term pulmonary sequelae in children? Front Pediatr 9:621019
Vezir E et al (2021) Does aeroallergen sensitivity and allergic rhinitis in children cause milder COVID-19 infection?. Allergy Asthma Proc 42(6):522–529
Acknowledgements
The authors thank Sultan Camlı for the secretarial work and the nurse Namık Çakar for PFTs.
Author information
Authors and Affiliations
Contributions
GKÖ is the guarantor of this study and contributed to the writing of the manuscript, patient recruitment, data collection, analysis, and interpretation, and manuscript review. BB designed the study and contributed to the writing of the manuscript, patient recruitment, data collection, analysis, interpretation, and manuscript review. SD contributed to data collection, analysis, and interpretation and manuscript review. HHA contributed to patient recruitment, data analysis and interpretation, and manuscript review.
Corresponding author
Ethics declarations
Ethics approval
This retrospective study was approved by the local ethics committee (No: 2020.12.213).
Consent to participate
Informed consent was obtained from all subjects and their parents.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Communicated by Peter de Winter
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This manuscript is original and has not been published and is not under consideration for publication elsewhere.
Rights and permissions
About this article

Cite this article
Öztürk, G.K., Beken, B., Doğan, S. et al. Pulmonary function tests in the follow-up of children with COVID-19. Eur J Pediatr 181, 2839–2847 (2022). https://doi.org/10.1007/s00431-022-04493-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-022-04493-w