
Abstract
It is well-known that children and adolescents with obesity have increased over recent decades which in turn carries greater risk of co-morbidities and poses a preventive as well as a therapeutic challenge. Currently, there are limited recommendations available on proven methods for recording physical fitness in children and adolescents presenting with extreme obesity. In this study, twenty participants, aged 12–17 years, with a body mass index (BMI) above the 99.5th percentile, were comparatively assessed, using a correlation between their physical fitness on a bicycle (BC) and treadmill (TM) cardiopulmonary exercise testing (CPET) with a lactate diagnostic. The results of the BC and the TM were as follows: maximum heart rate (HRmax) 186.4 ± 8.6 beats per minute (bpm) vs. 190.8 ± 8.8 bpm, peak oxygen consumption (VO2peak/kg) 23.5 ± 2.9 ml/min/kg vs. 25.4 ± 3.1 ml/min/kg, and maximum lactate (Lamax) 6.4 ± 1.6 mmol/l vs. 5.6 ± 1.4 mmol/l. The values of HRmax and VO2peak/kg were significantly higher for adolescents tested on the TM. However, no significant difference was observed in either Lamax values or between the genders.
Conclusions: The higher values of HRmax and VO2peak/kg could be attributed to the activation of a higher percentage of muscle mass on the TM. Lower Lamax values on the TM suggest maximum physical exertion was not achieved. This could be due to the extreme body weight carried by the participants. Both the BC and the TM CPET could be used for assessing physical fitness in children and adolescents with extreme obesity but should not be used interchangeably.
What is Known: • Currently, there are only limited recommendations available on proven methods for recording physical fitness in children and adolescents with extreme obesity available. | |
What is New: • Cardiopulmonary exercise testing with maximum physical exertion has been shown to be feasible in children and adolescents with extreme obesity. The results obtained from this study demonstrated that both a bicycle and a treadmill can be effectively used for assessing the physical fitness levels in children and adolescents with extreme obesity. |
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Obesity in childhood and adolescence is a growing and worldwide issue [1]. The KiGGS study, a representative population-based survey [2], showed that, in Germany, 15.4% of the adolescents are overweight and 5.9% are obese [3]. Extreme obesity is defined by a body mass index (BMI) above the 99.5th percentile. This corresponds to a standard deviation score (SDS) of more than + 2.5. Extreme obesity in childhood and adolescence is associated with an increased metabolic and cardiovascular morbidity (e.g., type 2 diabetes or coronary heart disease) in adulthood [4].
Physical fitness encompasses both physical and psychological components, although sports science only takes the physical components into consideration. According to Weineck [5], physical fitness defines the degree of expression of a certain sports motor performance. Physical fitness can be determined and assessed during maximal exercise testing. Using standardized examination conditions, performance diagnostics can be conducted on an ergometer. Evaluation of the results enables athletes, as well as recreational athletes and study participants, to receive specific training recommendations, based on findings. Additionally, results can provide supplementary therapy planning for people who are suffering from different diseases [6].
Physical activity plays an important role in prevention and treatment of overweight and obesity in childhood and adolescence [7]. Indeed, several recent publications have put forward different types of physical activities that have been shown to be effective in fighting obesity [8,9,10]. Dias et al. [10] have demonstrated how high-intensity interval training can be effective for people with obesity, especially by decreasing BMI-SDS and increasing cardiorespiratory fitness. For correct execution and highest levels of effectiveness, high-intensity interval training needs to be performed at a high-level heart rate. However, there is currently very little data on adolescents with extreme obesity exercising at such high-level heart rates. Hansen et al. [11] found in their systematic review and meta-analysis that there are differences between obese and lean adolescents in VO2peak measurements. Klijn et al. [12] found relevant and significant improvements on aerobic performance in adolescents with extreme obesity following an aerobic training program. When treating children and adolescents with extreme obesity, it is essential to consider individual performance limits and to make recommendations based on the data.
The aim of the present study was therefore to compare two methods of cardiopulmonary exercise testing (CPET) in terms of their feasibility and efficiency for maximum physical exertion in children and adolescents with extreme obesity. Additionally, possible gender-specific differences in physical fitness were also considered. Analysis of each individual’s physical fitness could, potentially, in addition substantiate personalized therapy recommendations already in place.
Methods
Written informed consent was obtained from each participant prior to testing. All examinations were carried out at the outpatient clinic of the Department of Sports Medicine at Charité – Universitätsmedizin Berlin/Humboldt, University of Berlin. Participants were recruited from the Center for Social-Paediatric Care of the Charité Berlin.
Participants
All participants were free of any medical condition that could have affected their performance of medical measurements. Exclusion criteria were individuals under 10 or over 17 years of age and body weight < 97. Percentile or BMI is < 25. The participants (n = 20; f: n = 11; m: n = 9) were 12 to 17 years of age (15.2 ± 1.6) at the time of examination. Table 1 shows anthropometric data of the study population with mean values and standard deviation for age, BMI, BMI-SDS, body fat percentage, and achieved power of each CPET.
Only subjects who participated in both examinations (BC and TM) were included in this study. There is, therefore, no missing data in this record.
Study design
Participants were tested in an incremental bicycle ergometry and running test in a laboratory setting (see protocols below) on two different days within a time frame of 2 weeks. In the first week, the bicycle exercise test was performed with the treadmill exercise test being carried out 1 week later. The tests were not carried out under fasting conditions, as this is not recommended for maximal exercise testing. Data collection started in July 2018 and finished in January 2019. Due to the pilot trial, a sample size calculation was not necessary.
Anthropometric data
The following anthropometric data were measured on two different days: body height, body weight, waist-to-hip ratio (WHR), BMI, caliperometry, and body composition with bioelectrical impedance analysis. The average of each data was subsequently calculated.
With the participant in an upright position, the body height and body weight of each were measured using a calibrated scale (Seca 285 DP, Seca GmbH & Co. KG, Hamburg, Germany). To calculate the BMI of each subject, the formula BMI = kg/m2 was used. Subsequently, waist and hip circumference was measured in cm with a standardized tape measure (Seca GmbH) in cm to determine the WHR. The WHR is the dimensionless ratio of the circumference of the waist to that of the hips and is calculated as waist measurement divided by hip measurement.
The anthropometry of fatty and fat-free mass was based on caliperometry of 7 and 10 skin folds. First, the thickness of designated skin folds was obtained using a caliper (Harpenden Skinfold Caliper, UK). A total of eleven different points of the body were included in the measurement, allowing the percentage body fat to be calculated using formulas from Jackson and Pollock and Johnson and Scholz [13,14,15]. Additionally, a bioelectrical impedance analysis was repeated at each appointment to measure body composition before exercise testing, to allow changes to be recorded. A body analysis scale (InBody770, JP Global Markets GmbH, Eschborn, Germany) was used to determine muscle, fat, and water proportions by measuring resistance [16, 17].
Exercise testing
Prior to the test, participants were informed of the importance of maximal physical effort. They were, however, instructed to immediately report any occurrence of thoracic pain, limiting dyspnea, or dizziness experience during testing. Prior to the beginning of each exercise, a clinical examination and an inconspicuous 12-lead rest electrocardiogram (ECG) (Custo Cardio 200 Saug-EKG, Custo med GmbH, Ottobrunn, Germany) were mandatory. During the test, a 12-lead ECG (Custo Cardio 300) was continuously running and monitoring (Software Custo diagnostics, Version 4.6.4).
After completion of the BC test, the running examination on the TM was planned after a 1-week break. This sequence was chosen deliberately, as experience has shown that the ECG quality during BC testing is improved, and any abnormalities can be detected at an earlier stage. Both examination methods were conducted under standardized laboratory conditions. The ambient temperature was between 18 and 24 °C with a humidity of 30–60%.
All participants were encouraged by the medical staff to exercise at their maximal effort level. During the test, the subjective state and the rating of perceived exertion (RPE) were recorded by the BORG 20 scale (Borg RPE) [18, 19]. The end of the test was generally determined by the participants’ maximum exhaustion.
Bicycle ergometer (BC)
Adjustments were made to the height of the BC saddle (Ergoselect 100 k. Ergoline GmbH, Bitz, Germany) and handlebars prior to testing. After a rest period of 3 min, the participants started at 25 W with a 25 W increase every 3 min. The ideal pedaling cadence was a consistent speed of 60–70 RPM, and no less than 60 RPM. At the point of exertion, the test was concluded, and participants remained on the BC at a low frequency with light resistance so that there was no abrupt load termination.
Throughout testing, ECG recordings continued to monitor recovery, ensuring 5-min rest. During the test, the blood pressure was measured every 3 min, with a standard suitable arm cuff, and a blood sample from the earlobe was taken every 3 min for lactate diagnostic purposes.
Treadmill ergometer (TM)
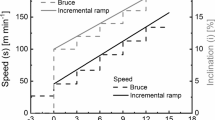
A constant speed on the TM (h/p cosmos sports & medical GmbH, Nussdorf-Traunstein, Germany) was set at 4 km/h with an initial elevation of 2.5%. This was increased by 2.5% every 3 min until the participant was seen to be exhausted. The protocol was selected [20] and needed to be adjusted for each participant, because high-speed running is not recommended for people with extreme obesity. The intensity of the exercise was therefore increased by raising the elevation rather than the speed of the TM.
Between the 3-min training intervals, a 30-s rest was given to measure lactate accumulation (LA) from capillary blood samples taken from the earlobe. Blood pressure was measured at the beginning of the test, at the point of exertion (until the end of the test), and after a minimum of 5 min in a resting position. The ECG was recorded continuously as in the first test on BC. The participants were able to stop the examination at any time.
Lactate accumulation (LA)
In order to be able to determine the blood lactate concentration, capillary blood was taken from the earlobe [21]. The earlobe had already been prepared with a blood flow-enhancing warming ointment (Finalgon) and then disinfected. LA was taken once at rest, during the test in the last 10 s of each stage and 3 times during the recovery phase. Immediately after the recovery phase, the blood samples were placed in a sample tray of the lactate device EKF Diagnostics Biosen C-line Clinic (Barleben, Germany) and analyzed within a few seconds by enzymatic-amperometric chip-sensor technology. Incremental exercise tests eliciting an increase in lactate values were then used to produce lactate curves. The lactate curve could be used to determine the aerobic and anaerobic threshold and may serve as a basis for individually assessing endurance capacity and training zones. In addition, a maximum lactate concentration provided proof of maximum exertion [22].
Cardiopulmonary exercise testing (CPET)
After a spirometry, a bodyplethysmography was conducted for each participant. Both resting pulmonary function tests were performed using COSMED Q-Box with COSMED Quark PFT (Pavona di Albano, Italy). This procedure made it possible to diagnose respiratory impairment prior to CPET [20].
Noninvasive metabolic testing equipment (K5 Wearable Metabolic System, COSMED, Pavona di Albano, Italy) supplied comprehensive measurements and therefore invaluable information about physical fitness and individual exercise limits, from which the training status could be generated [23].
Self-reported questionnaire
In order to gain further insights in the subjects’ well-being during both CPET, all subjects received a short questionnaire at the end of the second examination. Each of the subjects filled out the questionnaire themselves, providing subjective feelings of perceived exertion as a supplement to the BORG RPE scale. The combination of both tools was used so that the subjects did not have any difficulty in assessing their subjective perception of effort during exercise. Six age-appropriate questions were asked on parameters such as effort, joy, comfort, discomfort, motivation, and ambition, and the subjects could each choose a preferred CPET.
Data evaluation/statistics
The collected anthropometry data were recorded using a clinic software [I/med] (Version 6.34, DORNER GmbH & Co. KG). Resting ECG and stress ECG were recorded using Custo diagnostics (Custo med GmbH Version 4.6.4). The results of both pulmonary function tests and CPET were obtained using Omnia software from COSMED 2013/06). The data of performance diagnostics and in particular the LA values were visualized and recorded in Ergonizer (Version 5.0.1 Build 134; Röcker, 2013), and all data were transferred into an Excel spreadsheet (Microsoft Office Excel, 2019). Data were processed with the statistical program SPSS (IBM, SPSS Statistics, Version 25). For descriptive statistics, i.e., anthropometric data, respective mean values and standard deviations (SD) were calculated using SPSS.
A significance level of p < 0.05 was selected in the following evaluation to determine statistical significance [24]. Using SPSS, an analysis of variance (ANOVA) with repeated measures is applied as part of the inferential statistics. First, the residuals were tested for assumption of normality. The homogeneity of variance was subsequently proved, so that an ANOVA could be given [25]. ANOVA was performed on three parameters (HRmax, Lamax, and VO2peak/kg) and calculated for the effects of ergometry (within-subject factor, i.e., intraindividual) and sample and supplemented with the variable gender as a between-subject factor, i.e., inter-individual [24]. For the scatterplots, the software R (version 4.0.4) with the R-package ggplot2 (version 3.3.3) was used.
Results
Power
The participants achieved a mean power of 160.4 ± 6 W on BC. The girls reached an average of 155.6 ± 37 W and the boys 166.3 ± 23.6 W. As shown in Table 1, the boys reached a relative power of 1.2 ± 0.2 W/kg on the BC and the girls 1.2 ± 0.3 W/kg. In relation to fat-free mass, the subjects had a relative power of 2.7 ± 0.4 W/kg FFM. The boys reached a relative power of 2.5 ± 0.3 W/kg FFM, and the girls reached a relative power of 2.8 ± 0.4 W/kg FFM. On average, the participants achieved a 17.1 ± 3.4% slope at a constant speed of 4 km/h on the TM. The average load for the girls occurred at a mean slope of 16.6 ± 2.6%, and the boys achieved a 17.6 ± 2.3% slope.
Maximum heart rate (HRmax)
The achieved HRmax was on average 186.4 ± 8.6 bpm during BC testing and hence slightly lower than for TM testing which was 190.8 ± 8.8 bpm. For the female participants, the HRmax was 186.7 ± 8.1 bpm on BC and 190.9 ± 6.8 bpm on the TM. For the male participants, the HRmax on the BC was 186 ± 9.7 bpm and 190.6 ± 11.2 bpm on the TM.
Maximum lactate (Lamax)
The Lamax average was 6.4 ± 1.6 mmol/l on the BC and 5.6 ± 1.4 mmol/l on the TM. Female participants obtained a Lamax of 6.3 ± 1.7 mmol/l on the BC and 5.5 ± 1.2 mmol/l on the TM. Male participants achieved a Lamax of 6.5 ± 1.5 mmol/l on the BC and 6.0 ± 1.8 mmol/l on the TM.
Absolute and relative VO2peak
The absolute VO2peak for all subjects was, on average, 2.5 ± 0.4 l/min on the BC and 2.7 ± 0.5 l/min on the TM. The female subjects reached 2.4 ± 0.4 l/min on BC and 2.6 ± 0.5 l/min on the TM. Male subjects achieved 2.6 ± 0.4 l/min on the BC and 2.9 ± 0.5 l/min on the TM.
The achieved relative VO2peak/kg was on average 23.5 ± 2.9 ml/min/kg on the BC CPET and 25.4 ± 3.1 ml/min/kg on the TM. The female participants reached 23.3 ± 2.7 ml/min/kg on BC and 24.9 ± 3.4 ml/min/kg on the TM. Male participants obtained 23.7 ± 3.2 ml/min/kg on the BC and 26.0 ± 2.8 ml/min/kg on the TM.
Self-reported questionnaire
The two methods of CPET were compared on subjective parameters taken from the questionnaire. Fifteen subjects wrote that the cycling was more enjoyable than walking (five). In this context, seventeen subjects also felt more comfortable and safe on the BC, whereas only three subjects preferred the TM. Thirteen subjects reported being more ambitious and motivated when cycling than walking (seven). In terms of effort, the TM got more votes (twelve) than the BC (eight).
Discussion
Children and adolescents with extreme obesity are able to achieve maximum physical exertion on CPET. We demonstrated that both the BC and the TM are suitable for CPET for this specific age and weight group. The advantages of using a BC are a more accurate evaluation of the exercise ECG and a more comfortable measurement of blood pressure [26]. A sitting position is considered safer and more comfortable, especially for obese patients. A conscious decision was made to use this device because a higher muscular and therefore cardiovascular exertion could be achieved on a standard bicycle ergometer than on a recumbent ergometer. A self-reported questionnaire revealed that the BC was more comfortable and probably more familiar than the TM. This also led to the assumption that the examination carried out on the TM was perceived as more strenuous for the subjects. It is important to mention that the questionnaire is not a valid instrument but was used in addition to the BORG RPE scale. On the other hand, the TM examination led to significantly higher levels of HR and VO2peak/kg. This could be considered as a better achievement of a maximum physical exertion [27, 28]. Another explanation could be that due to the high body weight, exhaustion and an anaerobic metabolic state were reached more quickly, and thus, the maximum load is reached sooner. This could result in a higher percentage of activated muscle mass. The subjects may have been unable to reach maximum muscular exertion due to reaching the cardiopulmonary maximum on the BC [23, 29].
Criteria for maximum physical load (and their most common definitions) are as follows: (I) plateau of VO2 (with an increase of less than 150 ml/min), (II) HRmax (+ / − 10 bpm of age-dependent HRmax), (III) respiratory quotient RQ (VCO2/VO2 > 1.10), (IV) Lamax (> 8 mmol/l), and (V) Borg RPE scale (> 18/20) [30]. These criteria are used in a standardized way for athletes and helped as a reliable orientation in this study [31]. The participants achieved maximum physical load by obtaining a Borg RPE scale value of at least 18 or more. The mean RQ of our participants was, on the BC 1.08 + / − 0.1 and 1.09 + / − 0.1 on the TM. Due to the lack of regular physical training and low exercise level of our participants, these two criteria were fulfilled. The previous study has found a lowered RERpeak in obese adolescents in contrast to lean adolescents [32]. Therefore, the present study has proved that both CPETs can determine of maximum physical load in children and adolescents with extreme obesity. Recent studies have shown that a supramaximal validation test to confirm VO2max is unaffected by sex, cardiorespiratory fitness level, and especially body mass [33]. Regarding the maximum effort evaluation, these supramaximal validation tests could be suitable for children and adolescents with extreme obesity.
The main limitation of the present study was the modest number of participants due to the study being explorative in nature. Based on the inclusion criteria, only a few subjects were eligible. The main issue with participant acquisition was the necessity for a two-staged examination over a 1- to 2-week period. Forty-five families were informed and received information sheets. Twenty-five of these families did not take up the opportunity. Additionally, both the BC and the TM represented a very unusual activity situation for the participants, so that the subjective rating of maximum exertion (Borg RPE scale) was probably reached before maximum cardiopulmonary load. One implication of the study was that the examinations on the TM led to a higher level of motivation at the second appointment, because the participants were eager to improve their previous achievements [34]. Regarding the significantly higher levels of HRmax and VO2peak/kg in TM, this CPET should be considered as the more valid one for cardiopulmonary performance assessment. This is in line with findings in several other studies [27, 28, 35]. In this study, participants showed lower levels of Lamax on the TM. These values (p = 0.076), however, did not reach a significance level of p < 0.05. A lower Lamax in the TM compared to the BC could be due to a higher demand for lactate as a source of energy by both cardiac muscle fibers and the active muscles that have no heavy involvement in propulsion, f.e. arms and shoulder muscles [36,37,38]. Further studies comparing both methods need to be performed to analyze whether this is due to a lower level of fitness in children and adolescents with extreme obesity or whether other TM protocols need to be applied.
Interestingly, there were no significant differences between male and female participants, which comparable results for HRmax, Lamax, and VO2peak/kg in both male and female participants. There are usually differences in gender-specific athletic performances [39]. These results can be explained by the homogeneity of the participants. Both, females and males, were most likely unfamiliar with this kind of physical activity and reached a considerably lower maximum power on BC performed by normal weight boys (3–4 W/kg) and girls (2.8–3.5 W/kg) [40].
Given the fact that the BC and the TM are easily accessible instruments for measuring the maximum physical load in children and adolescents with extreme obesity, both methods could potentially be used as longitudinal parameters in intervention studies. Further studies must be performed to optimize the exercise protocols, especially the TM protocol (Figs. 1, 2 and 3).

Differences in maximum heart rate between the treadmill and the bicycle compared to average measurements of each subject. The black line refers to a mean to the mean difference of 4.4 beats per minute. Consequently, using an ANOVA, a statistically significant effect was calculated for the within-subject factor method (cardiopulmonary exercise testing: bicycle and treadmill), F = 4.848, p = 0.041; i.e., p < 0.05. There was no significant effect for the interaction method × sex (F = 0.005, p = 0.945; i.e., p > 0.05)

Differences in maximum lactate between the treadmill and the bicycle compared to average measurements of each subject. The black line refers to a mean difference of − 0.79 mmol/l. Using an ANOVA, which did not show significant differences for the within-subject factor method (cardiopulmonary exercise testing: bicycle and treadmill), F = 3.558, p = 0.076; i.e., p > 0.05. There was also no significant effect with the interaction method × sex (F = 0.000, p = 0.983; i.e., p > 0.05)

Differences in relative VO2peak between the treadmill and the bicycle compared to average measurements of each subject. The black line refers to a mean difference of 1.92 ml/min/kg. Using an ANOVA, a statistically significant effect was calculated for the within-subject factor method (cardiopulmonary exercise testing: bicycle and treadmill), F = 19.049, p = 0.000; i.e., p < 0.01. There was no significant effect with the interaction method × sex (F = 0.630, p = 0.438; i.e., p > 0.05)
Data availability
All data and materials support our published claims and comply with field standards.
Abbreviations
- ANOVA :
-
Analysis of variance
- BC:
-
Bicycle ergometer
- BMI:
-
Body mass index
- CPET:
-
Cardiopulmonary exercise testing
- ECG:
-
Electrocardiogram
- HR:
-
Heart rate
- LA:
-
Lactate accumulation
- RPE:
-
Rating of perceived exertion
- SDS:
-
Standard deviation score
- TM :
-
Treadmill ergometer
- VO2peak:
-
Peak oxygen consumption
- WHR:
-
Waist-to-hip ratio
References
Guthold R et al (2020) Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health 4(1):23–35
Schienkiewitz A, Brettschneider AK, Damerow S et al (2018) Overweight and obesity among children and adolescents in Germany. Results of the cross-sectional KiGGS Wave 2 study and trends. J Health Monit 3(1):15–22. https://edoc.rki.de/handle/176904/5627
Schienkiewitz A, Damerow S, Schaffrath Rosario A, Kurth BM (2019) body-mass-index von kindern und jugendlichen: prävalenzen und verteilung unter berücksichtigung von untergewicht und extremer adipositas : ergebnisse aus kiggs welle 2 und trends [Body mass index among children and adolescents: prevalences and distribution considering underweight and extreme obesity : results of KiGGS Wave 2 and trends]. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 62(10):1225–1234. https://doi.org/10.1007/s00103-019-03015-8
Llewellyn A, Simmonds M, Owen CG, Woolacott N (2016) Childhood obesity as a predictor of morbidity in adulthood: a systematic review and meta-analysis. Obes Rev 17(1):56–67. https://doi.org/10.1111/obr.12316 (Epub 2015 Oct 6 PMID: 26440472)
Weineck J (2010) Optimales Training: leistungsphysiologische Trainingslehre unter besonderer Berücksichtigung des Kinder- und Jugendtrainings 16, durchges. Spitta-Verlag, Balingen
Löllgen H, Leyk D (2018) Ergometrische Belastungsuntersuchungen in der Sportmedizin. Dtsch Arztebl Int 115(24):409–416
Hills AP, Andersen LB, Byrne NM (2011) Physical activity and obesity in children. Br J Sports Med 45(11):866–870. https://doi.org/10.1136/bjsports-2011-090199
Alberga AS, Prud’homme D, Sigal RJ et al (2016) Effects of aerobic training, resistance training, or both on cardiorespiratory and musculoskeletal fitness in adolescents with obesity: the HEARTY trial. Appl Physiol Nutr Metab 41(3):255–265. https://doi.org/10.1139/apnm-2015-0413
Niemiro GM, Rewane A, Algotar AM (2021). Exercise and fitness effect on obesity. In StatPearls. StatPearls Publishing, Copyright©, StatPearls Publishing LLC
Dias KA, Coombes JS, Green DJ et al (2016) Effects of exercise intensity and nutrition advice on myocardial function in obese children and adolescents: a multicentre randomised controlled trial study protocol. BMJ Open 6(4):e010929. https://doi.org/10.1136/bmjopen-2015-010929
Hansen D, Marinus N, Remans M, Courtois I, Cools F, Calsius J, Massa G, Takken T (2014) Exercise tolerance in obese vs. lean adolescents: a systematic review and meta-analysis. Obes Rev 15(11):894–904. https://doi.org/10.1111/obr.12202 (Epub 2014 Aug 6. PMID: 25132188)
Klijn PH, van der Baan-Slootweg OH, van Stel HF (2007) Aerobic exercise in adolescents with obesity: preliminary evaluation of a modular training program and the modified shuttle test. BMC Pediatr 19(7):19. https://doi.org/10.1186/1471-2431-7-19.PMID:17445257;PMCID:PMC1866229
Jackson AS, Pollock ML (1978) Generalized equations for predicting body density of men. Br J Nutr 40(3):497–504. https://doi.org/10.1079/bjn19780152 (PMID: 718832)
Jackson AS, Pollock ML, Ward A (1980) Generalized equations for predicting body density of women. Med Sci Sports Exerc 12(3):175–181 (PMID: 7402053)
Johnson D, Scholz C (1989) Anthropometrische Methoden zur Ermittlung und Beurteilung des Ernährungszustandes des Menschen. In Wissenschaftliche Zeitschrift der Humboldt-Universität zu Berlin, Reihe Medizin, Angewandte Anthropometrie 38(2):218–226
Brewer GJ, Blue MNM, Hirsch KR, Saylor HE, Gould LM, Nelson AG, Smith-Ryan AE (2021) Validation of InBody 770 bioelectrical impedance analysis compared to a four-compartment model criterion in young adults. Clin Physiol Funct Imaging 41(4):317–325. https://doi.org/10.1111/cpf.12700
Antonio J, Kenyon M, Ellerbroek A, Carson C, Tyler-Palmer D, Burgess V, Angeli G, Silver T, Jiannine L, Peacock C (2019) Body composition assessment: a comparison of the bod Pod, InBody 770, and DXA. J Exerc Nutr Biochem 2(2)
Borg G (1998) Borg’s Perceived Exertion and Pain Scales. Human Kinetics, Champaign, IL
Scherr J, Wolfarth B, Christle JW, Pressler A, Wagenpfeil S, Halle M (2013) Associations between Borg’s rating of perceived exertion and physiological measures of exercise intensity. Eur J Appl Physiol 113(1):147–155. https://doi.org/10.1007/s00421-012-2421-x
American Thoracic Society; American College of Chest Physicians (2003) ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med 167(2):211–277. https://doi.org/10.1164/rccm.167.2.211.Erratum.In:AmJRespirCritCareMed.2003May15;1451-2 (PMID: 12524257)
Goodwin ML, Harris JE, Hernández A, Gladden LB (2007) Blood lactate measurements and analysis during exercise: a guide for clinicians. J Diabetes Sci Technol 1(4):558–569. https://doi.org/10.1177/193229680700100414
Faude O, Kindermann W, Meyer T (2009) Lactate threshold concepts: how valid are they? Sports Med 39(6):469–490. https://doi.org/10.2165/00007256-200939060-00003 (PMID: 19453206)
Kroidl R, Schwarz S, Lehnigk B, Fritsch J (2015) Kursbuch spiroergometrie. technik und befundung verständlich gemacht (3. vollst. überarb. Aufl.). Stuttgart: Georg Thieme Verlag KG
Montgomery DC (2013) Design and Analysis of Experiments. John Wiley, New York
Shapiro SS, Wilk MB (1965) An analysis of variance test for normality (complete samples)†. Biometrika 52(3–4):591–611. https://doi.org/10.1093/biomet/52.3-4.591
Gilgen-Ammann R, Schweizer T, Wyss T (2019) RR interval signal quality of a heart rate monitor and an ECG Holter at rest and during exercise. Eur J Appl Physiol 119(7):1525–1532. https://doi.org/10.1007/s00421-019-04142-5 (Epub 2019 Apr 19 PMID: 31004219)
Basset FA, Boulay MR (2000) Specificity of treadmill and cycle ergometer tests in triathletes, runners and cyclists. Eur J Appl Physiol 81(3):214–221. https://doi.org/10.1007/s004210050033 (PMID: 10638380)
Abiodun OO, Balogun MO, Akintomide AO, Adebayo RA, Ajayi OE, Ogunyemi SA, Amadi VN, Adeyeye VO (2015) Comparison between treadmill and bicycle ergometer exercise tests in mild-to-moderate hypertensive Nigerians. Integr Blood Press Control 8:51–55. https://doi.org/10.2147/IBPC.S75888
Van Brussel M, Bongers BC, Hulzebos EHJ, Burghard M, Takken T (2019) A systematic approach to interpreting the cardiopulmonary exercise test in pediatrics. Pediatr Exerc Sci 31(2):194–203. https://doi.org/10.1123/pes.2018-0235
Scharhag-Rosenberger F, Schommer K (2013) Die Spiroergometrie in der Sportmedizin. Dtsch Z Sportmed 64:362–366
Meyer T, Lucía A, Earnest CP, Kindermann W (2005) A conceptual framework for performance diagnosis and training prescription from submaximal gas exchange parameters–theory and application. Int J Sports Med 26(Suppl 1):S38-48. https://doi.org/10.1055/s-2004-830514 (PMID: 15702455)
Marinus N, Bervoets L, Massa G, Verboven K, Stevens A, Takken T, Hansen D (2017) Altered gas-exchange at peak exercise in obese adolescents: implications for verification of effort during cardiopulmonary exercise testing. J Sports Med Phys Fitness 57(12):1687–1694. https://doi.org/10.23736/s0022-4707.16.06607-x
Sansum KM, Weston ME, Bond B et al (2019) Validity of the supramaximal test to verify maximal oxygen uptake in children and adolescents. Pediatr Exerc Sci 31(2):213–222. https://doi.org/10.1123/pes.2018-0129
Burgess E, Hassmén P, Pumpa KL (2017) Determinants of adherence to lifestyle intervention in adults with obesity: a systematic review. Clin Obes 7(3):123–135. https://doi.org/10.1111/cob.12183 (Epub 2017 Mar 15 PMID: 28296261)
Balogun MO, Sulyman BO, Akinwusi PO (1997) A comparison of the cardiovascular responses to treadmill and bicycle ergometer exercise in healthy male Nigerians. Afr J Med Med Sci 26(1–2):27–30 (PMID: 10895224)
Gladden LB (2008) A lactatic perspective on metabolism. Medicine and science in sports and exercise 40(3):477–85. https://doi.org/10.1249/MSS.0b013e31815fa580
Brooks GA (2021) Role of the heart in lactate shuttling. Front Nutr 22(8):663560. https://doi.org/10.3389/fnut.2021.663560.PMID:33968972;PMCID:PMC8101701
Brooks GA (2018) The science and translation of lactate shuttle theory. Cell Metab 27(4):757–785. https://doi.org/10.1016/j.cmet.2018.03.008 (PMID: 29617642)
Dominelli PB, Molgat-Seon Y, Sheel AW (2019) Sex differences in the pulmonary system influence the integrative response to exercise. Exerc Sport Sci Rev 47(3):142–150. https://doi.org/10.1249/JES.0000000000000188 (PMID: 30817330)
Washington RL, van Gundy JC, Cohen C, Sondheimer HM, Wolfe RR (1988) Normal aerobic and anaerobic exercise data for North American school-age children. J Pediatr 112:223–233
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
LK collected the anthropometric data and performed the medical examinations. The manuscript was written and edited by LK and MW and conceptualized and edited by SW and BW. The authors worked together to improve the manuscript and have all approved the submitted and published versions.
Corresponding author
Ethics declarations
Ethics approval
Ethical approval was not sought for this study, as all participants received usual care diagnostics.
Consent to participate
Informed consent was obtained from all participants and parents before the study.
Consent for publication
Informed consent for publication was obtained from all participants and parents before the study.
Conflict of interest
The authors declare no competing interests.
Additional information
Communicated by Gregorio Paolo Milani
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kalski, L., Wannack, M., Wiegand, S. et al. Comparison of two methods of cardiopulmonary exercise testing for assessing physical fitness in children and adolescents with extreme obesity. Eur J Pediatr 181, 2389–2397 (2022). https://doi.org/10.1007/s00431-022-04434-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-022-04434-7