
Abstract
This study aimed to investigate the trajectories of spinal pain frequency from 6 to 17 years of age and describe the prevalence and frequency of spinal pain and related diagnoses in children following different pain trajectories. First through fifth-grade students from 13 primary schools were followed for 5.5 years. Occurrences of spinal pain were reported weekly via text messages. Children reporting spinal pain were physically evaluated and classified using International Classification of Disease criteria. Trajectories of spinal pain frequency were modeled from age 6 to 17 years with latent class growth analysis. We included data from 1556 children (52.4% female, mean (SD) baseline age = 9.1 (1.9) years) and identified 10,554 weeks of spinal pain in 329,756 weeks of observation. Sixty-three percent of children reported one or more occurrences of spinal pain. We identified five trajectories of spinal pain frequency. Half the children (49.8%) were classified as members of a “no pain” trajectory. The remaining children followed “rare” (27.9%), “rare, increasing” (14.5%), “moderate, increasing” (6.5%), or “early-onset, decreasing” (1.3%) spinal pain trajectories. The most common diagnoses in all trajectory groups were non-specific (e.g., “back pain”). Tissue-specific diagnoses (e.g., muscle strain) were less common and pathologies (e.g., fracture) were rare.
Conclusion: From childhood through adolescence, spinal pain was common and followed heterogeneous courses comprising stable, increasing, and early-onset trajectories. These findings accord with recommendations from adult back pain guidelines that most children with spinal pain can be reassured that they do not have a serious disease and encouraged to stay active.
What is Known: • Spinal pain imposes a large burden on individuals and society. • Although many people first experience the condition in childhood, little is known about the developmental trajectories of spinal pain from childhood to adolescence. | |
What is New: • Data from 1556 children and 329,756 participant weeks showed five unique spinal pain trajectories from 6 to 17 years: most children rarely reported spinal pain, while one in five followed increasing or early-onset trajectories. • Most pain occurrences were non-specific; pathological diagnoses were rare. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Spinal pain imposes a large burden on individuals and society. For many, spinal pain develops in childhood; for example, the 12-month period prevalence of back pain in children ranges from 17.4 to 60.3% [1]. Back pain experienced in childhood tracks into adulthood [2], when it becomes the single largest source of years lived with disability [3].
Despite evidence of spinal pain’s burden, traditional clinical wisdom suggests that spinal pain in childhood is rare, and when present, stems from a pathological etiology (e.g., tumor, infection) [4]. However, current evidence shows spinal pain to be a common and usually benign condition in children, even when pain is persistent [5]. Thus, it may be the nature of symptoms and their developmental trajectories that distinguish different types of spinal pain rather than etiology. Life-course epidemiology emphasizes the importance of change in health-related features over time (i.e., health trajectories) [6]. Trajectory modeling has been used to understand the development of spinal pain, with models identifying discrete subgroups of adults who follow unique courses of pain over time [7]. Studies to date have focused on the trajectories of spinal pain in adult populations, leading researchers to highlight the development of spinal pain in youth as a priority [7, 8].
However, few studies to date have investigated the occurrence of spinal pain from adolescence to early adulthood. One study modeled the 3-year trajectories of low back pain in adolescents from ages 11 to 14 [9]. While 78% of participants had a very low probability of low back pain, the others followed trajectories showing an increasing (8%), decreasing (10%), early increase (2%), or persistently high (1%) probability of pain [9]. Another prospective study of individuals aged 14 to 22 found that most participants experienced impactful low back pain (i.e., pain resulting in care-seeking or interruption in activities) that followed an increasing (44%) or decreasing (10%) probability trajectory over the 8-year period [10].
There remains a lack of evidence regarding the developmental patterns of spinal pain in childhood as well as other fundamental aspects of pain, such as frequency and diagnostic characteristics. This knowledge is necessary to understand the development of spinal pain in the earlier life course. Therefore, the first aim of this study was to describe the trajectories of spinal pain frequency from 6 to 17 years of age. The second aim was to describe the prevalence and frequency of spinal pain and related diagnoses experienced by children following different pain trajectories.
Methods
Study design and participants
We analyzed prospective spinal pain data from the Childhood Health, Activity and Motor Performance School Study Denmark (CHAMPS Study-DK) collected between October 2008 and April 2014. The CHAMPS Study is a school-based health study; the study sample and procedures have been described in detail previously [11, 12]. In brief, CHAMPS Study-DK is a dynamic cohort in which some schools and participants entered the study at different times. In total, 19 public primary schools were invited, and 10 schools agreed to participate. A central feature of the original study design involved the comparison of outcomes between students attending schools implementing either usual or supplemented physical education. Because our study objectives were not concerned with the effects of physical education curriculum, we combined all data into a common cohort comprising students registered to attend grades one through five. We excluded children with serious chronic diseases and three children were excluded based on this criterion: one child with a congenital heart malformation, 1 child with cerebral palsy, and 1 child with dwarfism.
The study protocol was approved by the Regional Scientific Ethical Committee of Southern Denmark (ID S-20080047) and registered with the Danish Data Protection Agency (J.nr. 2008–41-2240). All participating children gave verbal assent and parents provided written informed consent prior to enrollment.
Spinal pain measurements
Weekly pain data were collected via short-message-service text messaging, except during the six-week summer and one-week Christmas holiday periods. Each week, the child’s parent or guardian was sent a text message inquiring about any occurrence of pain experienced by the child in different bodily regions over the preceding seven days: “Has (child’s name) had pain for the last week?”. Potential answers included “neck, back, or lumbar spine,” “shoulder, arm, or hand,” “hip, leg, or foot,” and “no, my child has not had any pain.” In this study, we limited our outcome to neck, back, or lumbar pain (i.e., spinal pain).
When spinal pain was reported by text message, a healthcare provider followed up with the parent by telephone within the week. If the pain continued to be present at the time of telephone interview, the child was scheduled for physical evaluation within 7 days. If the pain had resolved by the time of follow-up, the child continued to be monitored by text messaging as before. The evaluation comprised a standardized physical examination performed by study investigators who were registered physiotherapists or chiropractors. An orthopedic surgeon trained the examiners to ensure a standard examination approach, and the procedures were piloted by co-evaluating the first 20 children examined. The examiners maintained close contact with the orthopedic surgeon and each other throughout the study, discussing challenging cases and reinforcing examination procedures. When clinically indicated, children were referred for additional diagnostic investigation (e.g., blood tests, diagnostic imaging), orthopedic evaluation, or both. When children received medical evaluation or treatment outside of the study (e.g., emergency care), we obtained information through linked medical records.
All children who underwent physical examination with or without diagnostic testing were diagnosed using International Classification of Diseases (ICD-10) coding [13]. When more than one code was assigned for the same episode, we identified the primary diagnosis as the one most likely to be directly responsible for the child’s pain. Diagnostic codes were classified as either traumatic or non-traumatic. We considered four spinal pain outcomes: (i) self-reported spinal pain, (ii) diagnosed spinal pain, (iii) non-traumatic spinal pain, and (iv) traumatic spinal pain. Self-reported spinal pain included all pain reports. Diagnosed spinal pain was a subcategory of self-reported spinal pain comprising pain episodes for which the child underwent a physical evaluation and received a diagnosis. In this way, reports of diagnosed spinal pain indicated episodes lasting approximately 1 week or longer. Non-traumatic and traumatic spinal pain were subcategories of diagnosed pain and determined by ICD codes.
Anthropometric measurements and pubertal development
Height was measured to the nearest 0.5 cm with a portable stadiometer (SECA 214, Seca Corporation, Hanover, MD, USA) and weight to the nearest 0.1 kg using a calibrated Tanita BWB-800S digital scale (Tanita Corporation, Tokyo, Japan). Body mass index was calculated as weight(kg)/height(m)2. We classified BMI outcomes as normal, overweight, or obese according to age- and sex-specific criteria from the International Obesity Task Force [14].
Pubertal development was determined using Tanner stages [15]. During a structured interview that included explanatory text and visual diagrams of pubic hair development in boys and breast development in girls, participants self-assessed their Tanner stage on a 1 to 5 scale, with higher scores indicating later pubertal stages [16]. Tanner stage 1 represents prepubertal status, stages 2 to 4 denote increasing levels of adolescent development, and stage 5 indicates adult development. We collapsed Tanner stages 4 and 5 into a common category owing to their low prevalence in the sample population.
Data analysis
Missing spinal pain data were imputed with random hot deck multiple imputations [17] across five datasets. This approach involved the matching of missing data with observed records, generating probabilities for matched records, and sampling records based on the probability of each outcome. Covariates incorporated into the random hot deck imputations were sex and pain for the individuals with missing data in the surrounding weeks. Additional details have been reported previously [18]. To support the modeling procedure, the weekly pain data were collapsed into 11 six-month study periods. To contribute data to a study period, we required that participants were enrolled and responding to the text messages for at least 60% of that period.
All analyses were conducted with Stata 16.1 software (StataCorp, College Station, TX, USA). We described continuous variables as means and standard deviations (SD) and categorical variables as counts and percentages for the entire sample and stratified by trajectory subgroup. We modeled trajectories of self-reported spinal pain frequency (weeks with pain), as a function of age, with latent class growth analysis. This approach is a specialized application of finite mixture modeling used to identify meaningful trajectory subgroups (latent classes) within otherwise heterogeneous data [19; 20]. These models use maximum likelihood estimation to approximate trajectory distributions without assuming that trajectory classes comprise distinct populations; features that distinguish this approach from similar techniques such as growth mixture modeling [19]. We applied a zero-inflated Poisson distribution and applied equal weights across the five imputed datasets to generate a common model.
We first constructed a single-class model and then increased the number of latent classes, the complexity of the polynomial distributions (e.g., linear, quadratic, cubic) and zero-inflation patterns until an optimal model was identified. We used several criteria to define the optimal model as fit decisions should not hinge on a single metric [19]. Initial decisions were made using the Bayesian information criterion and judgment to identify clinically meaningful subgroups. We subsequently tested models with four a priori diagnostic criteria: (i) a minimum average posterior probability of group membership ≥ 0.7, (ii) minimum odds of correct classification > 5, (iii) precision of confidence intervals around estimates of group membership probabilities, and (iv) close correspondence between the estimated group membership probability and the proportion of participants assigned to each group based on the posterior probability [19, 20]. We explored for sex-specific differences in the spinal pain trajectories by analyzing data from boys and girls separately. The resulting models were very similar (data not shown), and we therefore elected to report one common model.
Results
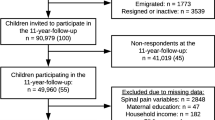
In total, 1670 children were enrolled in the study. We excluded 114 (6.8%) children as they only had spinal pain data for one study period. Therefore, data from 1556 children (baseline age = 9.1 (1.9) years, 52.4% female) comprising 329,756 weeks of observation were included in the trajectory model (Fig. 1). The average weekly response rate over the course of the study was greater than 96% [21, 22]; in total, valid responses were received for 94.8% of weeks prior to imputation. The mean number of 6-month study periods with valid spinal pain data was 8.0 (2.8). Therefore, participating children contributed approximately four years of weekly spinal pain data on average. Precise age data were unavailable for 19 children (1.2%) who provided spinal pain data via text messaging but did not participate in the measurement sessions; we estimated their ages using average values from children at the same grade level.

Participant flow diagram
Over the course of the study, 63.2% of children reported one or more occurrences of spinal pain and 27.5% of children experienced one or more pain occurrences of sufficient duration to allow for physical examination and diagnosis (diagnosed spinal pain). In total, spinal pain was reported in 10,554 participant weeks, among which 4,823 (45.7%) were weeks with diagnosed spinal pain. The large majority of diagnosed spinal pain weeks were categorized as non-traumatic (4342 weeks; 90.0%).
Spinal pain trajectories
The final trajectory model identified a five-class solution comprising zero-order, linear, and quadratic polynomials (Fig. 2). All predefined diagnostic criteria were met: posterior probabilities were 0.80 or greater, odds of correct classification exceeded 5.0, confidence intervals were relatively precise, and differences between the estimated group membership probability and the proportion of participants assigned to the group were small (Table 1).

Trajectories of self-reported spinal pain and their prevalence (N = 1556)1. 1Points represent weeks with spinal pain in each 6-month period. Dotted lines represent 95% confidence intervals
Latent trajectory subgroups were labeled according to the average frequency of weeks with spinal pain and the shapes of their distributions. Approximately half the children (49.8%) were classified as members of a trajectory defined by the absence or minimal occurrence of spinal pain (i.e., “no pain”). Although we received rare reports of pain from approximately one-third of children following the “no pain” trajectory (approximately 0.4 weeks per four years on average), the pain was nearly always transient and resolved prior to physical examination. Remaining children were assigned to a “rare” (27.9%), “rare, increasing” (14.5%), “moderate, increasing” (6.5%), or an “early-onset, decreasing” (1.3%) spinal pain trajectory. Baseline demographic, anthropometric, and pubertal development data for each trajectory subgroup are presented in Table 2.
Spinal pain prevalence, frequency, and diagnoses
Table 3 and Fig. 3 report descriptive statistics for spinal pain characteristics, stratified by trajectory subgroup. Primary diagnoses, stratified by spinal pain trajectory subgroup, are reported in Table 4. Back pain (non-specific) was the most common diagnosis received by participants in four of five trajectories groups, comprising 18 to 33% of all primary diagnostic codes. Tissue-specific spinal pain diagnoses (e.g., muscle strain, facet syndrome) were less common, and pathological diagnoses (e.g., fracture) were rare.

Average weeks with (A) self-reported spinal pain1 and (B) diagnosed spinal pain2, stratified by trajectory subgroup. 1Self-reported spinal pain includes all pain reports. 2Diagnosed spinal pain is a subcategory of self-reported spinal pain comprising pain episodes for which the child underwent a physical evaluation and received a diagnosis. Values are means and 95% confidence intervals (some intervals too narrow to visualize). NP, no pain; R, rare; RI, rare, increasing; MI, moderate, increasing; EOD, early-onset, decreasing
Discussion
In this study, children were classified as following one of five spinal pain trajectories from 6 to 17 years of age. Most children were classified as never or rarely experiencing spinal pain, while approximately 1 in 5 reported an increasing frequency of spinal pain into adolescence. The increasing trajectories are noteworthy as they may indicate children who suffer for prolonged periods and may also be at risk of developing more frequent or persistent spinal pain later in life. Moreover, a small subgroup of children experienced early-onset spinal pain. While children following the early-onset trajectory improved after about age 13, they reported the greatest number of weeks with pain overall. Most children (63%) reported at least one episode of spinal pain in approximately 4 years (including the few reports of usually transient pain from children in the “no pain” subgroup), and nearly 1 in 3 (28%) were diagnosed with at least one condition related to their pain, which were largely classified as non-traumatic. The most common diagnoses were descriptive and non-specific (e.g., “back pain”); tissue-specific and pathological diagnoses were less frequent. This means that spinal pain in children is common, often non-specific, and follows a heterogeneous course of pain frequency.
We are unaware of other studies that have modeled the developmental trajectories of spinal pain from childhood through adolescence. However, previous studies have estimated the probability of reporting low back pain during early adolescence [9] or from adolescence to early adulthood [10], with results that also suggest spinal pain to be common in those age groups. The primary differences between the current and previous studies involve the populations and methods of spinal pain measurement. We modeled the trajectories of spinal pain (back and neck pain) frequency over 5.5 years in children aged 6 to 11 years at baseline and covered a larger age span. We measured spinal pain frequency versus pain occurrences and applied shorter sampling windows (1 week versus 3 to 12 months). Despite these methodological differences, there were some similarities in the pain trajectories identified by the different studies.
One prospective study modeled the 3-year trajectories of low back pain experienced by 1336 11- to 14-year-old children from the USA and identified six unique trajectories [9]. Comparable to our study, in which 78% of participants had no pain or rare pain, approximately 3 in 4 participants in the other cohort had a very low probability of reporting pain. The remaining participants in that study followed trajectories whose probabilities of pain increased (8%), decreased (10%), peaked early (2%), or remained persistently high (1%) over time. We identified a greater proportion of participants who followed increasing spinal pain trajectories, which may reflect the larger age range of our population and the later stage of pubertal development for some participants, a potential risk factor for spinal pain [23, 24]. However, the early peak trajectory reported in that study included children whose probability of pain increased until around age 13 and sharply decreased thereafter, a pattern similar to the early-onset, decreasing frequency trajectory experienced by 1.3% of the participants in the current study. While most pain trajectories identified by the current and previous studies followed a course of consistent or increasing pain frequency or probability, this finding shows that some children with early-onset pain do experience a favorable prognosis.
The current study adds to the evidence that spinal pain in children rarely results from a pathological etiology. Of the 1556 participants enrolled in this study, we identified few cases of pathological spinal pain such as idiopathic scoliosis (12 cases; 0.8%), disc protrusion (6 cases; 0.4%), fractures (3 cases; 0.2%), inflammatory arthritis (1 case; 0.1%), and spondylolysis (1 case; 0.1%). In comparison, non-specific diagnoses such as back pain (211 cases; 13.6%), soft tissue pain (159 cases; 10.2%), and neck pain (86 cases; 5.5%) were more common. This finding accords with evidence from adult populations showing the vast majority (approximately 90%) of low back pain to be non-specific [25]. Given the implications of overdiagnosis, clinicians are encouraged to embrace non-specific labels when appropriate and avoid potentially harmful diagnostic labels during a formative period when one’s perceived vulnerability to spinal pain is poorly understood [26].
The number of children meeting our criteria for diagnosed spinal pain (27.5%) was less than half that of those with self-reported spinal pain (63.2%), indicating that many pain occurrences resolved within one week. However, previous findings have shown spinal pain to be episodic and recurrent for many [7, 27], and contemporary perspectives view spinal pain as a long-term condition with a variable course of symptoms and not a series of unrelated and self-limiting pain events [28, 29].
Clinical decision-making for children with spinal pain is a challenge. There have been few trials published on the treatment of spinal pain in the pediatric population and guideline recommendations are almost exclusively underpinned by evidence from adult studies of low back pain [30]. The current study results show concerning causes of spinal pain to be rare. This finding accords with guideline recommendations for clinicians to (1) reassure patients without clinical “red flags” that they do not have a serious disease, (2) encourage normal activities, and (3) avoid bed rest [31].
Study strengths and limitations
The strengths of this prospective study include the frequent and repeated measurements of spinal pain in a representative cohort of children from the general population. The 1-week sampling window likely reduced the potential for recall bias, and the integration of clinical examination and diagnostic information advances our understanding of spinal pain classification in the pediatric population.
Trajectory modeling is a person-centered approach, and our a priori statistical criteria suggested a high likelihood that participants were correctly classified. However, statistical models do not represent the individual experiences of all participants. For example, longitudinal evaluations show that some adults follow an episodic or “fluctuating” course of back pain in which intervals with minimal symptoms are separated by painful episodes that recur with time [7, 27]. These patterns are difficult to model, as the timing of the episodes can be unpredictable. Trajectory model outcomes “smooth” the course of symptoms and therefore represent the average experience of people assigned to a particular trajectory subgroup.
In the current study, participants contributed approximately 4 years of spinal pain data on average. Because we sought to understand the development of spinal pain as a function of age, we modeled pain trajectories from ages 6 to 17 years. This approach assumes that the participating children would follow similar trajectories at a given age, irrespective of their age at baseline and duration of participation. The validity of diagnostic criteria to identify specific pain-generating tissues such as joints, intervertebral discs, or muscles is unclear. Therefore, some diagnoses may be misclassified. Similarly, pain occurrences were reported by parents, and surrogate reporting is a potential source of bias, particularly with minor occurrences that may not be communicated from children to their parents [32]. The current study focused on the trajectories of spinal pain frequency, which is key to understanding the burden of this condition. However, investigating additional person-centered and societal outcomes (e.g., pain intensity, cost, school absenteeism, reduced physical activity participation) in future studies could provide important context to understanding the burden of spinal pain in children. Finally, while we attempted to recruit all 19 regional primary schools in Svendborg, nine schools elected not to participate in this study. Although our study sample represents approximately half of all primary school students in the region, there may be differences between the study and target populations.
Data science tasks in epidemiology can be classified as description, prediction, and causal inference [33], and future research is needed to investigate these aspects of spinal pain in children. For example, the trajectories described in this study can be extended to see if they predict persistent pain states in adulthood. Identifying baseline predictors of the different pain trajectories will help identify those children at risk of future spinal pain. Finally, the discovery of modifiable causes of spinal pain will be central to the development and testing of future interventions.
Conclusion
Spinal pain is common, often non-specific, and follows a heterogeneous course in children. Most children were classified as members of a no pain or rare spinal pain trajectory subgroup. About 1 in 5 children followed trajectories of increasing pain frequency, while a small subgroup of followed an early-onset, decreasing spinal pain trajectory. Children with early-onset pain reported the most weeks with spinal pain overall, while those following an increasing trajectory were tracking to experience the most pain in late adolescence. Pathological diagnoses were rare in all subgroups.
Availability of data and material
Data are available from the CHAMPS Study Steering Committee upon reasonable request. Legal and ethical restrictions apply. Interested parties may contact Dr. Niels Christian Møller (nmoller@health.sdu.dk), and the following information will be required at the time of application: a description of how the data will be used, securely managed, and permanently deleted.
Code availability
The code used in the analysis is available upon reasonable request.
Abbreviations
- CHAMPS study-DK:
-
Childhood health, activity, and motor performance school study Denmark
- ICD:
-
International Classification of Diseases
References
Calvo-Munoz I, Gomez-Conesa A, Sanchez-Meca J (2013) Prevalence of low back pain in children and adolescents: a meta-analysis. BMC Pediatr 13:14
Hestbaek L, Leboeuf-Yde C, Kyvik KO, Manniche C (2006) The course of low back pain from adolescence to adulthood: eight-year follow-up of 9600 twins. Spine 31:468–472
GBD 2019 Diseases and Injuries Collaborators (2020) Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396:1204–1222
Davis PJ, Williams HJ (2008) The investigation and management of back pain in children. Arch Dis Child Educ Pract Ed 93:73–83
Bhatia NN, Chow G, Timon SJ, Watts HG (2008) Diagnostic modalities for the evaluation of pediatric back pain: a prospective study. J Pediatr Orthop 28:230–233
Kuh D, Ben-Shlomo Y, Lynch J, Hallqvist J, Power C (2003) Life course epidemiology. J Epidemiol Community Health 57:778–783
Kongsted A, Kent P, Axen I, Downie AS, Dunn KM (2016) What have we learned from ten years of trajectory research in low back pain? BMC Musculoskelet Disord 17:220
Junge T, Wedderkopp N, Boyle E, Kjaer P (2019) The natural course of low back pain from childhood to young adulthood - a systematic review. Chiropr Man Ther 27
Dunn KM, Jordan KP, Mancl L, Drangsholt MT, Le Resche L (2011) Trajectories of pain in adolescents: a prospective cohort study. Pain 152:66–73
Beynon AM, Hébert JJ, Beales DJ, Jacques A, Walker BF (2021) Multi-trajectory analysis of C-reactive protein and low back pain from adolescence to early adulthood. Eur Spine J 30:1028–1034
Wedderkopp N, Jespersen E, Franz C, Klakk H, Heidemann M, Christiansen C, Moller NC, Leboeuf-Yde C (2012) Study protocol. The Childhood Health, Activity, and Motor Performance School Study Denmark (The CHAMPS-study DK). BMC Pediatr 12:128
Moller N, Tarp J, Kamelarczyk E, Brond J, Klakk H, Wedderkopp N (2014) Do extra compulsory physical education lessons mean more physically active children - findings from the childhood health, activity, and motor performance school study Denmark (The CHAMPS-study DK). Int J Behav Nutr Phys Act 11:121
World Health Organization (WHO) (1992) International statistical classification of diseases and related health problems. Geneva. ICD-10 1(10).
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH (2000) Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 320:1240–1243
Tanner JM (1962) Growth at adolescence, with a general consideration of the effects of hereditary and environmental factors upon growth and maturation from birth to maturity.2d edn. Blackwell Scientific Publications, Oxford
Duke PM, Litt IF, Gross RT (1980) Adolescents’ self-assessment of sexual maturation. Pediatrics 66:918–920
Andridge RR, Little RJ (2010) A review of hot deck imputation for survey non-response. Int Stat Rev 78:40–64
Wang C, Stokes T, Steele R, Wedderkopp N, Shrier I (2020) Implementing multiple imputation for missing data in longitudinal studies when models are not feasible: a tutorial on the random hot deck approach. p arXiv:2004.06630
Nagin DS, Odgers CL (2010) Group-based trajectory modeling in clinical research. Annu Rev Clin Psychol 6:109–138
Nagin D (2005) Group-based modeling of development. Harvard University Press, Cambridge, Mass
Fuglkjaer S, Hartvigsen J, Wedderkopp N, Boyle E, Jespersen E, Junge T, Larsen LR, Hestbaek L (2017) Musculoskeletal extremity pain in Danish school children - how often and for how long? The CHAMPS study-DK. BMC Musculoskelet Disord 18:492
Jespersen E, Holst R, Franz C, Rexen CT, Klakk H, Wedderkopp N (2014) Overuse and traumatic extremity injuries in schoolchildren surveyed with weekly text messages over 2.5 years. Scand J Med Sci Sports 24:807–813
Hébert JJ, Leboeuf-Yde C, Franz C, Lardon A, Hestbæk L, Manson N, Wedderkopp N (2019) Pubertal development and growth are prospectively associated with spinal pain in young people (CHAMPS study-DK). Eur Spine J 28:1565–1571
Janssens KA, Rosmalen JG, Ormel J, Verhulst FC, Hunfeld JA, Mancl LA, Oldehinkel AJ, LeResche L (2011) Pubertal status predicts back pain, overtiredness, and dizziness in American and Dutch adolescents. Pediatrics 128:553–559
Koes BW, van Tulder MW, Thomas S (2006) Diagnosis and treatment of low back pain. BMJ 332:1430–1434
Friedman DJ, Tulloh L, Khan KM (2021) Peeling off musculoskeletal labels: sticks and stones may break my bones, but diagnostic labels can hamstring me forever. Br J Sports Med
Axen I, Leboeuf-Yde C (2013) Trajectories of low back pain. Best Pract Res Clin Rheumatol 27:601–612
Dunn KM, Hestbaek L, Cassidy JD (2013) Low back pain across the life course. Best Pract Res Clin Rheumatol 27:591–600
Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J, Pransky G, Sieper J, Smeets RJ, Underwood M, Working LLBPS G (2018) What low back pain is and why we need to pay attention. Lancet 391:2356–2367
Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM, Koes BW, Peul W, Turner JA, Maher CG, Working LLBPS, G, (2018) Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet 391:2368–2383
UK National Institute for Health and Care Excellence (2016) Low back pain and sciatica in over 16s: assessment and management
Kamper SJ, Dissing KB, Hestbaek L (2016) Whose pain is it anyway? Comparability of pain reports from children and their parents. Chiropr Man Therap 24:24
Hernán MA, Hsu J, Healy B (2019) A second chance to get causal inference right: a classification of data science tasks. Chance 32:42–49
Funding
The CHAMPS Study-DK was originally supported by grants from The TRYG Foundation, University College Lillebaelt, University of Southern Denmark, The Nordea Foundation, The IMK foundation, e.g., The Egmont Foundation, The A.J. Andersen Foundation, The Danish Rheumatism Association, Østifternes Foundation, Brd. Hartmann’s Foundation, TEAM Denmark, The Danish Chiropractor Foundation, and The Nordic Institute of Chiropractic and Clinical Biomechanics. No funding was secured for the current study. The funders had no role in the design or conduct of the study.
Author information
Authors and Affiliations
Contributions
Prof Hébert analyzed and interpreted the data, drafted the initial manuscript, and critically reviewed the manuscript for important intellectual content. Dr Beynon, Ms Wang, Dr Shrier, and Dr Swain carried out initial analyses and interpreted the data, and critically reviewed the manuscript for important intellectual content. Dr Jones analyzed and interpreted the data and critically reviewed the manuscript for important intellectual content. Prof Leboeuf-Yde, Prof Hartvigsen, and Prof Hestbæk conceptualized and designed the study, and critically reviewed the manuscript for important intellectual content. Dr Junge and Dr Franz acquired data and critically reviewed the manuscript for important intellectual content. Prof Wedderkopp conceptualized and designed the study, coordinated and supervised data collection, interpreted the data, and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Ethics approval
The study protocol was approved by the Regional Scientific Ethical Committee of Southern Denmark (ID S-20080047) and registered with the Danish Data Protection Agency (J.nr. 2008–41-2240).
Consent to participate
All participating children gave verbal assent and parents provided written informed consent prior to enrollment.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests. Prof Hébert receives salary and research support from the Canadian Chiropractic Research Foundation and the New Brunswick Health Research Foundation.
Additional information
Communicated by Gregorio Paolo Milani
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hébert, J.J., Beynon, A.M., Jones, B.L. et al. Spinal pain in childhood: prevalence, trajectories, and diagnoses in children 6 to 17 years of age. Eur J Pediatr 181, 1727–1736 (2022). https://doi.org/10.1007/s00431-021-04369-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-021-04369-5