
Abstract
Fluid overload (FO) has been associated with an increased risk for adverse outcomes in critically ill patients. Information on the impact of FO on mortality in a general population of pediatric intensive care unit (PICU) is limited. We aimed to determine the association of early FO with the development of acute kidney injury (AKI) and mortality during PICU stay and evaluate whether early FO predicts mortality, even after adjustment for illness severity assessed by pediatric risk of mortality (PRISM) III. This prospective study enrolled 370 critically ill children. The early FO was calculated based on the first 24-h total of fluid intake and output after admission and defined as cumulative fluid accumulation ≥5 % of admission body weight. Of the patients, 64 (17.3 %) developed early FO during the first 24 h after admission. The PICU mortality rate of the whole cohort was 18 of 370 (4.9 %). The independent factors significantly associated with early FO were PRISM III, age, AKI, and blood bicarbonate level. The early FO was associated with AKI (odds ratio [OR] = 1.34, p < 0.001) and mortality (OR = 1.36, p < 0.001). The association of early FO with mortality remained significant after adjustment for potential confounders including AKI and illness severity. The area under the receiver operating characteristic curve (AUC) of early FO for predicting mortality was 0.78 (p < 0.001). This result, however, was not better than PRISM III (AUC = 0.85, p < 0.001).
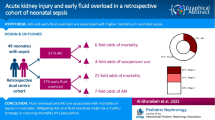
Conclusion: Early FO was associated with increased risk for AKI and mortality in critically ill children.
What is Known: • Fluid overload is associated with an increased risk for adverse outcomes in specific clinical settings of pediatric population. |
What is New: • Early fluid overload during the first 24 h after PICU admission is independently associated with increased risk for acute kidney injury and mortality in critically ill children. |
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Fluid administration is fundamental in critically ill patients; however, it often leads to the development of significant fluid overload (FO), which may promote tissue edema and contribute to organ dysfunction [4, 24]. There is growing evidence supporting the relationship between FO and adverse outcomes in critically ill adult patients admitted to the intensive care unit (ICU) [5, 29, 32, 35].
In pediatric population, the positive correlation between FO and adverse outcomes has been demonstrated in specific clinical settings [2, 12, 13, 16, 18, 21, 25, 26, 28, 30, 31], such as in children requiring continuous renal replacement therapy (CRRT) [26, 30] and in children undergoing cardiac surgery [18, 25]. Information on the impact of FO on mortality in a general pediatric ICU (PICU) population is limited. One study of 266 critically ill children admitted to the PICU found that FO ≥10 % was associated with increased morbidity and mortality [28].
Furthermore, in children undergoing cardiac surgery, children with early FO were more likely to develop acute kidney injury (AKI) and required prolonged mechanical ventilation (MV) than those without early FO, suggesting that early FO often precedes AKI and is associated with worse outcomes [18]. The predictive significance of early FO for mortality in general PICU patients remains unknown. In addition, very few studies have adjusted for illness severity in the analysis on FO and mortality [17, 28, 30].
AKI, which is well recognized as an independent risk factor for mortality, is commonly encountered in critically ill patients [1, 10, 11, 27]. AKI patients are more likely to develop FO. AKI contributes to impaired free water and sodium excretion, resulting in fluid accumulation. In turn, FO results in tissue edema, contributing to progressive organ dysfunction. These effects are pronounced in the kidneys. Tissue edema may directly participate in the progression of AKI [8, 9, 15, 19, 24]. The previous studies conducted in children and infants suggest that both AKI and FO were associated with increased mortality [3, 28]. However, whether or not the association of FO with mortality is due to direct effects of FO itself or due to indirect associations between FO and other disease states, such as AKI, is unknown [9]. It remains unclear whether the effect of FO on mortality is independent of AKI.
The aims of the study were to evaluate the impact of early FO developed during the first 24 h after PICU admission on the development of AKI and PICU mortality, and to determine whether early FO predicts mortality, even after adjustment for potential risk factors associated with mortality, including AKI and illness severity assessed by the pediatric risk of mortality III (PRISM III) score, in the general population of PICU. In addition, given the potential importance of FO on clinical outcomes, it is worthwhile understanding risk factors associated with early FO.
Patients and methods
All patients admitted to the PICU from January to June 2011 and from May to August 2012 were eligible for the study. The criteria for PICU admission in the university-affiliated tertiary children hospital were as described previously [6]. The inclusion criteria were admission to the PICU, including both medical and surgical patients, for 24 h or more and age between 1 month and 16 years. The exclusion criteria were length of stay in the PICU less than 24 h, including patients who did not survive the first 24 h after admission and patients who did not require at least 24 h of PICU hospitalization judged by the chief physicians; transfer to another hospital; and unexpected discharge from the PICU due to economic reason. This study was approved by the Ethics Committees of the Children’s Hospital of Soochow University and performed in accordance with the Declaration of Helsinki. Informed consent was obtained from the parents of the critically ill children enrolled in the study.
Clinical and laboratory data collection
Demographic, clinical, and laboratory data collected on the first 24 h of PICU admission, including age, body weight, sex, admission diagnosis, arterial blood gas analysis, and routine biochemical profile, were analyzed to determine the independent contributors to the risk of early FO. The first available laboratory results during the first 24 h after PICU admission were used for analysis.
Clinical status, medication, and therapies were recorded daily until PICU discharge or death. Multiple organ dysfunction syndrome (MODS) was diagnosed when three or more organ dysfunctions were detected during PICU stay, according to the criteria described previously [14, 33] .
Assessment of fluid overload
In order to quantify FO, 24-h total of fluid intakes and outputs were measured. Fluid intake included all enterally and parenterally administered fluids (maintenance fluids, medications, blood products, and all forms of nutritional support). Fluid output included urine, stool, blood loss, drain output, and nasogastric tube output. Fluid management was determined by the practicing physicians and not influenced by the study researchers. Urine output was calculated by weighing disposable diapers or measuring the volume of urine collected using an indwelling urethral catheter.
Fluid accumulation was calculated according to the following formula: [(total amount of fluid intake (L) − total amount of fluid output (L))/body weight at PICU admission (kg)] × 100 [17, 28]. FO was defined as ≥5 % of fluid accumulation [18]. The threshold of 5 % FO, which is equivalent to a positive fluid balance of 50 mL/kg, was recommended as a cutoff point for higher AKI risk in very high-risk patients who require mechanical ventilation and one or more vasoactive agents [7, 18]. Early FO was considered when FO occurred during the first 24 h after PICU admission.
Assessment of illness severity
The severity of illness was assessed by the PRISM III score, which was previously described in detail in the original studies [23]. Sixteen age-related physiological parameters required for calculation of the PRISM III score were collected during the first 24 h after PICU admission.
Definition of AKI and clinical outcomes
AKI was defined according to the AKI network (AKIN) criteria: a ≥50 % increase in the serum creatinine level from baseline and/or urine output <0.5 mL/kg per hour for 6 h [20]. The serum creatinine at the time of PICU admission was defined as baseline creatinine. For patients who presented to the PICU with an elevated serum creatinine (>106.1 μmol/L), the lowest creatinine value within 2 weeks in the PICU was considered as baseline creatinine adapted from a previous study [22]. Clinical outcomes measured included length of MV, length of PICU stay, and PICU mortality that was defined as a death occurring during PICU stay after admission.
Statistical analysis
Statistical analyses were conducted using SPSS 13.0. For continuous variables with normal or skewed distribution, descriptive results were expressed as mean ± standard deviation (SD) or median and interquartile range (IQR), respectively. The student’s t test for unpaired samples and the Mann-Whitney U test were used to determine the differences between two groups, depending on the distribution of the data. The chi-square test or Fisher’s exact test were used to compare the differences of categorical variables between groups. Stepwise multivariate linear regression analysis was performed to investigate factors potentially associated with FO. To assess whether there was significant multicollinearity among variables, collinearity diagnostics were performed using variance inflation factor (VIF) and tolerance values. Continuous variables with skewed distribution were log-transformed for linear regression analysis. Univariate and multivariate binary logistic regression models were conducted to calculate odds ratio (OR) with 95 % confidence interval (CI) for PICU mortality. The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was calculated to assess the predictive ability. The nonparametric method of Delong was performed to compare difference between AUCs, and sensitivity and specificity were calculated at the optimal cut-off values using the software of SigmaPlot 10.0. All probability values were two-sided. Differences with p values <0.05 indicated statistical significance.
Results
Patient characteristics
The study enrolled 370 critically ill children. During the study period, 407 children were admitted to PICU. Thirty-seven children were excluded: 4 died and 5 were discharged from PICU in the first 24 h after admission, 4 were transferred to another hospital or unexpectedly discharged due to economic reasons, and 24 had incomplete data on fluid balance. There were no significant differences between the included and excluded patients in age (median [IQR]: 11 [3–33] vs. 14 [7–26] months; p = 0.300), gender (male/female 238:132 vs. 23/14; p = 0.849), and PRISM III score (3 [0–6] vs. 2.5 [0–11.5]; p = 0.621).
The PICU mortality rate of the whole cohort with or without early FO was 18 of 370 (4.9 %). Of the 370 patients, 64 (17.3 %) developed early FO defined as ≥5 % of fluid accumulation during the first 24 h after admission. Admission diagnoses in patients with and without early FO are listed in Table 1. Early FO was associated with more severe illness as assessed by PRISM III score (6 [2–12.5] vs. 2 [0–6]; p < 0.001), a larger proportion of AKI (18.8 vs. 4.2 %; p < 0.001), and a higher mortality rate (15.6 vs. 2.6 %; p < 0.001) when compared with patients without early FO. The comparison of demographic and clinical characteristics between patients with and without early FO is displayed in Table 2.
Determination of clinical and laboratory factors potentially associated with early fluid overload
Variables including age; gender; PRISM III scores; the first available laboratory results of PaO2, PaCO2, arterial pH, serum albumin, serum creatinine, blood urea nitrogen, blood glucose, serum sodium, serum potassium, and blood bicarbonate; and AKI and mechanical ventilation developed during PICU stay, were entered into a stepwise multivariate linear regression analysis. As displayed in Table 3, PRISM III score (p < 0.001), age (p < 0.001), AKI (p = 0.003), and blood bicarbonate level at admission (p = 0.016) were identified as independent factors significantly associated with early FO (total R 2 = 0.20). VIF and tolerance values of <2 and >0.5, respectively, indicate the absence of significant multicollinearity between variables in the final model of multivariate regression analysis.
Association of early fluid overload with AKI
AKI was diagnosed in 25 (6.8 %) patients, including 17 (68.0 %) classified as AKIN stage 1: 14 on the first, 2 on the third, and 1 on the fifth day after admission; 2 (8.0 %) classified as stage 2: 1 on the second and 1 on the third day; and 6 (24 %) classified as stage 3: 4 on the first, 1 on the fourth, and 1 on the seventh day after PICU admission. Diagnosis of AKI was based on serum creatinine change, except for four patients with AKIN stage 1 on the first day after admission, who were diagnosed based on urine output <0.5 mL/kg per hour for 6 h.
The early FO was associated with AKI developed during PICU stay (OR = 1.31; 95 % CI, 1.17–1.46; p < 0.001). The association, however, did not remain significant after adjustment for PRISM III score (OR = 1.09; 95 % CI, 0.95–1.25; p = 0.231). Fluid balance between patients with and without AKI is compared in Fig. 1a. The fluid balance during the first 24 h after admission was significantly higher in patients who developed AKI during PICU stay compared to those who did not (6.32 ± 1.17 vs. 1.94 ± 0.17 %; p < 0.001).

Comparison of the fluid balance calculated during the first 24 h after admission between critically ill children who did or did not develop acute kidney injury (AKI) during PICU stay (a) and between survivors and non-survivors (b). Boxes represent medians and interquartile ranges and whiskers represent minimums and maximums. Probability values: Student’s t test
Association of both early fluid overload and AKI with mortality
Both early FO (OR = 1.36; 95 % CI, 1.20–1.55; p < 0.001) and the presence of AKI (OR = 15.77; 95 % CI, 5.52–45.03; p < 0.001) were significantly associated with PICU mortality and independent of each other (FO: OR = 1.28; 95 % CI, 1.11–1.48; p = 0.001. AKI: OR = 6.41; 95 % CI, 1.89–21.81; p = 0.003).
In addition, the association of early FO with PICU mortality remained significant after adjustment for potential confounders including illness severity assessed by the PRISM III score and other risk factors for mortality such as the presence of AKI and the use of MV, as displayed in Table 4. However, the association between AKI and mortality did not remain significant after adjustment. The comparison of fluid balance between survival and non-survival critically ill children is shown in Fig. 1b. Non-survival children had significantly higher fluid balance during the first 24 h after admission compared to survivors (7.40 ± 1.52 vs. 1.97 ± 0.17 %; p < 0.001).
Ability of early fluid overload to predict PICU mortality
The predictive ability of early FO calculated during the first 24 h after PICU admission for PICU mortality was assessed in Table 5. The level of early fluid accumulation achieved AUC of 0.78 (95 % CI, 0.65–0.91; p < 0.001), which was better than AKI (AUC = 0.70; 95 % CI, 0.55–0.85; p = 0.005), but not than PRISM III (AUC = 0.85; 95 % CI, 0.74–0.96; p < 0.001) for predicting mortality. The p value for comparison between the two AUCs of early FO and PRISM III was 0.422. In addition, when combining early FO and AKI, the predictive performance improved (AUC = 0.83; 95 % CI, 0.72–0.95; p < 0.001) over that of early FO alone, but not reaching statistical significance (p = 0.520). The ROC curves of early FO and PRISM III for predicting the PICU mortality of critically ill children are displayed in Fig. 2.

Receiver operating characteristic (ROC) curves for the ability of early fluid overload and the score of pediatric risk of mortality III (PRISM III) to predict PICU mortality in critically ill children (n = 370). The area under the ROC curve (AUC) for early fluid overload and PRISM III were 0.78 and 0.85, respectively. p value of comparison of the difference between AUCs = 0.422
The sensitivity and specificity of early FO and PRISM III score at the optimal cut-off value to predict PICU mortality are shown in Table 5. Early FO displayed a sensitivity of 78 % and a specificity of 74 % at the cut-off value of 3.8 %. At the optimal cut-off score of 5.5, the sensitivity and specificity were 83 and 72 %, respectively, for PRISM III score to predict PICU mortality.
Discussion
This study provides data on FO developed during the first 24 h after PICU admission in critically ill children and demonstrates that early FO is significantly associated with the development of AKI and mortality during PICU stay.
FO had been previously found to be associated with increased risk of mortality in pediatric patients [12, 13, 25, 26, 28, 30, 31]. To our knowledge, only one study verified the use of early FO as a predictive marker in the pediatric population. Early postoperative FO was independently associated with worse outcomes, including prolonged MV and extended length of hospital stay, in a subgroup of PICU patients after cardiopulmonary bypass [18]. We evaluated the impact of early FO on predicting mortality in a general PICU population, independent of the severity of illness.
It is reasonable to question the association of FO with clinical outcomes, because it may be a surrogate for illness severity. Indeed, the degree of FO was significantly affected by the severity of illness assessed by the PRISM III score in our study, and more severely ill patients had greater degrees of early FO. A limited number of pediatric studies have adjusted for illness severity in their analysis of FO and outcomes [17, 28, 30]. In critically ill children receiving CRRT, the effect of FO on the prediction of PICU mortality persisted after adjustment for disease severity measured by the PRISM II score [30]. In children admitted to the PICU, FO developed in the first 14 days of admission to the PICU was associated with increased mortality even when adjusted for age and PRISM II score [28]. These results are similar to our study. We further examined the confounding effects of illness severity and other clinical factors associated with mortality to account for differences between patients who are fluid overloaded and those who are not. Our data imply that early FO is not merely a marker of disease severity, but an independent factor associated with mortality.
The other major finding in this study was the association between FO in the first 24 h and AKI occurring within the first week of PICU admission, suggesting that early FO relates to AKI as it is diagnosed by serum creatinine change and/or urine output. Previous studies suggest that significant FO may occur prior to the development of AKI, as defined by SCr rise [18, 25]. However, whether the fluid accumulation is a contributor to AKI is yet to be determined, because that AKI may have occurred before it was detected with current clinical diagnostics. Our study confirmed that both early FO and AKI were associated with adverse outcomes. The bidirectional interaction between FO and AKI raises the question of whether it is possible that the association of FO with mortality could be at least partially attributed to the occurrence of AKI. Although the contiguity and possible overlapping of FO and AKI make it difficult to establish the exact border between these two clinical events in a study, we demonstrated that early FO was significantly associated with mortality, even accounting for its interaction with AKI. This implies that mortality might be impacted negatively by early FO regardless of the presence of AKI.
There are no specific criteria for defining fluid accumulation in critically ill children. This 5 % FO threshold was observed in the previous study performed in the subgroup of PICU patients with cardiopulmonary bypass [18]. The percentage threshold of FO may depend on what patient population is being studied [25]. One previous study demonstrated a dose-response relationship between FO and mortality, independent of the severity of illness [30]. In our data, for every 1 % increase in early fluid accumulation, the odds for PICU mortality increased by 36 %. Moreover, early FO achieved AUC of 0.78 for predicting mortality. However, the ROC curve analysis in the present study showed that PRISM III score (AUC = 0.85) seemed to play a greater role than early FO in predicting the PICU mortality, although there was no significant difference between the two AUCs. This might be explained by the fact that the PRISM III score, which has been well validated as a measure of illness severity and predictor of mortality in children admitted to the PICU, is calculated using age-related physiological parameters measured precisely [23, 36]. However, documentation of the exact fluid intake and output may not be always accurate in critically ill children, especially in infants. These results suggested that accurate and precise measurements should be used to predict clinical outcomes in critically ill children. Moreover, the possibility of the low performance of AKI in predicting mortality might be due to the fact that 68 % of the patients with AKI in the study had AKIN stage 1. One previous study suggests a nearly linear increase in hospital mortality with increasing the severity of AKI [27, 34]. Less severity of AKI may have resulted in underestimation of the impact of AKI on mortality.
This study has some limitations. First, we were not able to ascertain the fluid balance before PICU admission. The information concerning initial fluid resuscitation, pressor administration, and diuretic therapy prior to PICU admission, which contributes significantly to the fluid balance, was not available [8, 20, 21]. Therefore, whether the general PICU patients with early 5 % FO truly had pathologic fluid accumulation has to be considered. Second, because of the observational nature of the study, we cannot determine if early FO has a precise pathogenesis in increasing mortality or is merely a valuable biomarker of critical illness [5]. Third, although definition and staging of AKI are based on serum creatinine and urine output [20], the use of urine output criteria for diagnosis has not been well validated. Four patients were diagnosed with AKI based on urine output in our study, which might increase the likelihood of observing an association between FO and AKI. Fourth, the PICU mortality found in this study was lower compared to our previous report [6], which might be explained by the fact that we excluded patients who died within 24 h after PICU admission. Nevertheless, we also excluded patients who did not require at least 24 h of PICU hospitalization. There was no significant difference between excluded and included patients in the illness severity assessed by the PRISM III score. Fifth, AKI occurred in the first week of PICU admission, with 72 % in the first day, implying that patients might be admitted later to the PICU in our unit. In addition, only 25 % of survivors are mechanically ventilated during PICU stay, suggesting that patients received less aggressive treatment. These may limit the generalizability of our findings to critically ill children admitted earlier in their critical illness courses and receiving aggressive management in the PICU. The exclusion of children who were unexpectedly discharged from the PICU due to economic reasons may also make it difficult to generalize the results of this study. Further multicenter studies are necessary to improve the generalizability of our findings.
In conclusion, our study indicates that early FO was significantly associated with increased risk for AKI and mortality in critically ill children. These findings support increased attention to monitoring the fluid balance. Further randomized and controlled clinical trials are needed to explore whether early FO would be a treatment target to lower mortality in PICU patients.
Abbreviations
- AKI:
-
Acute kidney injury
- AUC:
-
Area under the receiver operating characteristic curve
- CI:
-
Confidence interval
- CRRT:
-
Continuous renal replacement therapy
- FO:
-
Fluid overload
- MODS:
-
Multi-organ dysfunction syndrome
- MV:
-
Mechanical ventilation
- ROC:
-
Receiver operating characteristic
- IQR:
-
Interquartile range
- OR:
-
Odds ratio
- PICU:
-
Pediatric intensive care unit
- PRISM III:
-
Pediatric Risk of Mortality III
- VIF:
-
Variance inflation factor
References
Alkandari O, Eddington KA, Hyder A, Gauvin F, Ducruet T, Gottesman R, Phan V, Zappitelli M (2012) Acute kidney injury is an independent risk factor for pediatric intensive care unit mortality, longer length of stay and prolonged mechanical ventilation in critically ill children: a two-center retrospective cohort study. Crit Care 15:R146
Arikan AA, Zappitelli M, Goldstein SL, Naipaul A, Jefferson LS, Loftis LL (2012) Fluid overload is associated with impaired oxygenation and morbidity in critically ill children. Pediatr Crit Care Med 13:253–258
Askenazi DJ, Koralkar R, Hundley HE, Montesanti A, Patil N, Ambalavanan N (2013) Fluid overload and mortality are associated with acute kidney injury in sick near-term/term neonate. Pediatr Nephrol 28:661–666
Bagshaw SM, Bellomo R, Kellum JA (2008) Oliguria, volume overload, and loop diuretics. Crit Care Med 36:S172–S178
Bagshaw SM, Brophy PD, Cruz D, Ronco C (2008) Fluid balance as a biomarker: impact of fluid overload on outcome in critically ill patients with acute kidney injury. Crit Care 12:169
Bai Z, Zhu X, Li M, Hua J, Li Y, Pan J, Wang J, Li Y (2014) Effectiveness of predicting in-hospital mortality in critically ill children by assessing blood lactate levels at admission. BMC Pediatr 14:83
Basu RK, Chawla LS, Wheeler DS, Goldstein SL (2012) Renal angina: an emerging paradigm to identify children at risk for acute kidney injury. Pediatr Nephrol 27:1067–1078
Bouchard J, Soroko SB, Chertow GM, Himmelfarb J, Ikizler TA, Paganini EP, Mehta RL (2009) Fluid accumulation, survival and recovery of kidney function in critically ill patients with acute kidney injury. Kidney Int 76:422–427
Butcher BW, Liu KD (2012) Fluid overload in AKI: epiphenomenon or putative effect on mortality? Curr Opin Crit Care 18:593–598
Chertow GM, Soroko SH, Paganini EP, Cho KC, Himmelfarb J, Ikizler TA, Mehta RL (2006) Mortality after acute renal failure: models for prognostic stratification and risk adjustment. Kidney Int 70:1120–1126
Clec'h C, Gonzalez F, Lautrette A, Nguile-Makao M, Garrouste-Orgeas M, Jamali S, Golgran-Toledano D, Descorps-Declere A, Chemouni F, Hamidfar-Roy R, Azoulay E, Timsit JF (2011) Multiple-center evaluation of mortality associated with acute kidney injury in critically ill patients: a competing risks analysis. Crit Care 15:R128
Foland JA, Fortenberry JD, Warshaw BL, Pettignano R, Merritt RK, Heard ML, Rogers K, Reid C, Tanner AJ, Easley KA (2004) Fluid overload before continuous hemofiltration and survival in critically ill children: a retrospective analysis. Crit Care Med 32:1771–1776
Gillespie RS, Seidel K, Symons JM (2004) Effect of fluid overload and dose of replacement fluid on survival in hemofiltration. Pediatr Nephrol 19:1394–1399
Goldstein B, Giroir B, Randolph A (2005) International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 6:2–8
Goldstein SL (2012) Fluid management in acute kidney injury. J Intensive Care Med 29:183–189
Goldstein SL, Somers MJ, Baum MA, Symons JM, Brophy PD, Blowey D, Bunchman TE, Baker C, Mottes T, McAfee N, Barnett J, Morrison G, Rogers K, Fortenberry JD (2005) Pediatric patients with multi-organ dysfunction syndrome receiving continuous renal replacement therapy. Kidney Int 67:653–658
Goldstein SL, Currier H, Graf C, Cosio CC, Brewer ED, Sachdeva R (2001) Outcome in children receiving continuous venovenous hemofiltration. Pediatrics 107:1309–1312
Hassinger AB, Wald EL, Goodman DM (2014) Early postoperative fluid overload precedes acute kidney injury and is associated with higher morbidity in pediatric cardiac surgery patients. Pediatr Crit Care Med 15:131–138
Heung M, Wolfgram DF, Kommareddi M, Hu Y, Song PX, Ojo AO (2011) Fluid overload at initiation of renal replacement therapy is associated with lack of renal recovery in patients with acute kidney injury. Nephrol Dial Transplant 27:956–961
Mehta RL, Kellum JA, Shah SV, Molitoris BA, Ronco C, Warnock DG, Levin A (2007) Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care 11:R31
Michael M, Kuehnle I, Goldstein SL (2004) Fluid overload and acute renal failure in pediatric stem cell transplant patients. Pediatr Nephrol 19:91–95
Pickering JW, Endre ZH (2010) Back-calculating baseline creatinine with MDRD misclassifies acute kidney injury in the intensive care unit. Clin J Am Soc Nephrol 5:1165–1173
Pollack MM, Patel KM, Ruttimann UE (1996) PRISM III: an updated pediatric risk of mortality score. Crit Care Med 24:743–752
Prowle JR, Echeverri JE, Ligabo EV, Ronco C, Bellomo R (2010) Fluid balance and acute kidney injury. Nat Rev Nephrol 6:107–115
Seguin J, Albright B, Vertullo L, Lai P, Dancea A, Bernier PL, Tchervenkov CI, Calaritis C, Drullinsky D, Gottesman R, Zappitelli M (2014) Extent, risk factors, and outcome of fluid overload after pediatric heart surgery. Crit Care Med
Selewski DT, Cornell TT, Lombel RM, Blatt NB, Han YY, Mottes T, Kommareddi M, Kershaw DB, Shanley TP, Heung M (2011) Weight-based determination of fluid overload status and mortality in pediatric intensive care unit patients requiring continuous renal replacement therapy. Intensive Care Med 37:1166–1173
Singbartl K, Kellum JA (2012) AKI in the ICU: definition, epidemiology, risk stratification, and outcomes. Kidney Int 81:819–825
Soler YA, Nieves-Plaza M, Prieto M, Garcia-De Jesus R, Suarez-Rivera M (2013) Pediatric risk, injury, failure, loss, end-stage renal disease score identifies acute kidney injury and predicts mortality in critically ill children: a prospective study. Pediatr Crit Care Med 14:e189–e195
Stein A, de Souza LV, Belettini CR, Menegazzo WR, Viegas JR, Costa Pereira EM, Eick R, Araujo L, Consolim-Colombo F, Irigoyen MC (2012) Fluid overload and changes in serum creatinine after cardiac surgery: predictors of mortality and longer intensive care stay. A prospective cohort study. Crit Care 16:R99
Sutherland SM, Zappitelli M, Alexander SR, Chua AN, Brophy PD, Bunchman TE, Hackbarth R, Somers MJ, Baum M, Symons JM, Flores FX, Benfield M, Askenazi D, Chand D, Fortenberry JD, Mahan JD, McBryde K, Blowey D, Goldstein SL (2010) Fluid overload and mortality in children receiving continuous renal replacement therapy: the prospective pediatric continuous renal replacement therapy registry. Am J Kidney Dis 55:316–325
Symons JM, Chua AN, Somers MJ, Baum MA, Bunchman TE, Benfield MR, Brophy PD, Blowey D, Fortenberry JD, Chand D, Flores FX, Hackbarth R, Alexander SR, Mahan J, McBryde KD, Goldstein SL (2007) Demographic characteristics of pediatric continuous renal replacement therapy: a report of the prospective pediatric continuous renal replacement therapy registry. Clin J Am Soc Nephrol 2:732–738
Teixeira C, Garzotto F, Piccinni P, Brienza N, Iannuzzi M, Gramaticopolo S, Forfori F, Pelaia P, Rocco M, Ronco C, Anello CB, Bove T, Carlini M, Michetti V, Cruz DN (2013) Fluid balance and urine volume are independent predictors of mortality in acute kidney injury. Crit Care 17:R14
Typpo KV, Petersen NJ, Hallman DM, Markovitz BP, Mariscalco MM (2009) Day 1 multiple organ dysfunction syndrome is associated with poor functional outcome and mortality in the pediatric intensive care unit. Pediatr Crit Care Med 10:562–570
Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C (2005) Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA 294:813–818
Vaara ST, Korhonen AM, Kaukonen KM, Nisula S, Inkinen O, Hoppu S, Laurila JJ, Mildh L, Reinikainen M, Lund V, Parviainen I, Pettila V (2012) Fluid overload is associated with an increased risk for 90-day mortality in critically ill patients with renal replacement therapy: data from the prospective FINNAKI study. Crit Care 16:R197
Wang JN, Wu JM, Chen YJ (2001) Validity of the updated pediatric risk of mortality score (PRISM III) in predicting the probability of mortality in a pediatric intensive care unit. Acta Paediatr Taiwan 42:333–337
Compliance with ethical standards
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from the parents of all individual children included in the study.
Funding
This study was funded by the Natural Science Foundation for Research Projects in the Colleges and Universities of Jiangsu Province (12KJB320006), the Natural Science Foundation of Jiangsu Province (BK2012604), and the National Natural Science Foundation of China (81370773).
Conflict of interest
The authors declare that they have no competing interests.
Authors’ contributions
Dr. Yanhong Li had primary responsibility for study design, data analysis, interpretation of data, and writing of the manuscript. Dr. Jian Wang and Dr. Zhenjiang Bai participated in study design. Jiao Chen, Xueqin Wang, and Dr. Jian Pan were responsible for clinical data collection and participated in data analysis. Dr. Xiaozhong Li and Dr. Xing Feng participated in the design of the study and coordination. All authors read and approved the final manuscript.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Communicated by Patrick Van Reempts
Xiaozhong Li and Xing Feng contributed equally to this work.
Rights and permissions
About this article

Cite this article
Li, Y., Wang, J., Bai, Z. et al. Early fluid overload is associated with acute kidney injury and PICU mortality in critically ill children. Eur J Pediatr 175, 39–48 (2016). https://doi.org/10.1007/s00431-015-2592-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00431-015-2592-7