
Abstract
Since the publication of the 2020 World Health Organization classification of soft tissue and bone tumors, the classification of “fibroblastic” tumors has expanded to include a novel subset of tumors characterized by PRRX1::NCOA1/2 gene fusions. These tumors defy conventional classification and are morphologically distinct, characterized by a multi-nodular growth of bland spindle cells suspended in a myxo-collagenous stroma with mild cytologic atypia, “staghorn-like” vessels, and variable perivascular hyalinization. Mitotic activity is rare, and necrosis is not identified. Herein, we present six additional cases of PRRX1-rearranged mesenchymal tumors, including five cases with PRRX1::NCOA1 fusion and one case with PRRX1::KMT2D fusion. Three cases (3/6, 50%) demonstrated focal co-expression of S100 protein and SOX10, thereby expanding the immunohistochemical profile of this emerging entity. Like prior reported cases, there was no evidence of malignant behavior on short-term follow-up. The novel fusion, PRRX1::KMT2D, further expands the molecular spectrum of this entity and leads to a proposed revision of the provisional nomenclature to “PRRX1-rearranged mesenchymal tumor” to both accommodate non-NCOA1/2 fusion partners and allow for the possibility of partial neural or neuroectodermal differentiation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Since the publication of the 2020 World Health Organization classification of soft tissue and bone tumors [1], the classification of so-called fibroblastic tumors has expanded to include a novel subset of tumors characterized by PRRX1::NCOA1/2 gene fusions [2]. These morphologically unique tumors were first formally described in 2019 in a series of four cases by Lacambra et al. [3], who proposed the name “PRRX1-NCOAx-rearranged fibroblastic tumor.” These distinct tumors are characteristically multinodular, well-circumscribed, predominantly hypocellular, and composed of bland spindle cells growing in a myxo-collagenous stroma with minimal to mild cytologic atypia. Mitotic activity is rare, and necrosis is not identified. The tumors are most often centered in the subcutis and follow a benign clinical course following marginal excision. Since their initial description, additional studies have further characterized and expanded the morphologic spectrum of this newly recognized mesenchymal tumor [4,5,6].
Herein, we present six additional cases of PRRX1-rearranged mesenchymal tumors, a subset of which demonstrated variable degrees of expression of S100 protein and SOX10, thereby broadening the immunohistochemical profile of this emerging entity. Moreover, one of our cases harbored a novel PRRX1::KMT2D fusion, which expands the molecular spectrum of this tumor. Based on these observations, we propose a revision to the provisional nomenclature from “PRRX1-NCOAx-rearranged fibroblastic tumor” to “PRRX1-rearranged mesenchymal tumor” to both accommodate non-NCOA1/2 fusion partners and allow for the possibility of partial neural or neuroectodermal differentiation.
Materials and methods
Case selection
This study was approved by the Institutional Review Boards of the participating institutions. All cases were identified either through routine clinical practice or through expert subspecialty consultation by the authors. Clinicopathologic features of all six cases were assessed.
Immunohistochemistry
Immunohistochemical stains were performed on available 4-µm formalin-fixed paraffin-embedded (FFPE) tissue sections for each case using standard techniques. Due to the consultative nature of the cases, immunohistochemistry techniques and panels varied among contributing institutions. The details of the staining protocols and antibody sources are available upon request.
Next-generation sequencing (NGS)
Cases were sent for testing with the Sarcoma Targeted Gene Fusion/Rearrangement (SARCP) panel, performed at Mayo Clinic Laboratories. The SARCP panel is a custom-designed, PCR-based panel developed in collaboration with Qiagen. The panel is designed to detect 138 gene fusions (> 280 gene variants) in 39 sarcoma types. Next-generation sequencing (NGS) is performed on an Illumina MiSeq instrument, and the NGS data is analyzed using an in-house developed bioinformatic pipeline called SeekFusion. Case 3 underwent additional testing at Cleveland Clinic using an anchored multiplex polymerase chain reaction and at the University of Washington using FusionPlex analysis, neither of which identified any gene fusion. Finally, at Bioptical Laboratory, Ltd. (Plzen, Czech Republic), RNA libraries were prepared using the TruSight Oncology 500 Kit (Illumina) according to the manufacturer’s protocol. The original set of probes for fusion detection was replaced with TruSight RNA Pan-Cancer Panel (Illumina) targeting 1385 genes. Data analysis for fusion detection was performed using Dragen RNA app version 4.0.4 (Illumina). Case 4 was analyzed using TruSight RNA Fusion panel (Illumina, Inc., San Diego, CA, USA) at the Institute of Pathology, Friedrich‐Alexander University Erlangen‐Nürnberg in Germany as previously described in detail [7]. Cases 5 and 6 were analyzed using the TruSeq RNA Access Library Prep Kit (Illumina, San Diego, CA, USA) as previously described [8].
Results
Clinically, the tumors frequently presented as slow-growing nodules centered in the subcutaneous tissue of middle-aged patients (median, 41 years; range, 29–65 years) with a female predominance (4 female, 2 male). The duration of the clinical history varied from weeks to years with one patient reporting a 4–5-year history of a slow-growing mass prior to presenting for excision. While most of the tumors were centered in the superficial subcutaneous tissue, two were intramuscular and involved deeper soft tissue. Half of the cases involved the head and neck region (neck, n = 2; forehead, n = 1), and half involved the trunk (chest wall, n = 1; flank, n = 1; back, n = 1). Most tumors were relatively small in size (median, 3.2 cm; range, 2.2–9.5 cm) with only one case being larger than 4.0 cm.
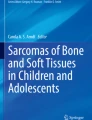
Each patient underwent a marginal to complete excision, which grossly showed a circumscribed, multi-nodular, solid and firm, white-tan mass (Fig. 1) involving the subcutaneous tissue. Microscopically, the characteristic multi-nodularity was further appreciated from low-power (Fig. 2 A, B). The tumors were composed of bland, predominantly hypocellular spindle cells (Fig. 2C) with focal areas with increased cellularity (Fig. 2D). The tumors had, at most, mild cytologic atypia and were embedded in a myxo-collagenous stroma with ropey collagen bundles (Fig. 2E) and rare mast cells. No melanin pigment was identified. One case had a focal area with entrapped benign adipose tissue (Fig. 2F). Along the periphery of the lesion, scattered “staghorn-like” vessels with prominent perivascular hyalinization were variably present (Fig. 2 G–I). Mitotic figures were inconspicuous, and no areas of necrosis were identified.

Resection specimens typically showed a circumscribed, multi-nodular, solid and firm, white-tan mass

PRRX1-rearranged mesenchymal tumors are usually treated with conservative excision, which often shows a circumscribed and multinodular bland spindle cell neoplasm (A, B). These spindle cell neoplasms are predominantly hypocellular (C) with focal areas with increased cellularity (D). The spindle cells grow in a myxo-collagenous stroma with ropey collagen bundles (E). One case also had a focal area with entrapped benign adipose tissue (F). Along the periphery of the lesion, scattered “staghorn-like” vessels with prominent perivascular hyalinization are present (G–I)
Immunohistochemical stains showed that scattered cells were positive for S100 protein (Fig. 3) in four cases (4/6, 67%) and SOX10 (Fig. 3) in three cases (3/6, 50%), while all tested cases were negative for CK cocktail, EMA, SMA, desmin, CD34, STAT6, MUC4, CD117, MDM2, and CDK4. One case (Case 6) was also diffusely positive for pan-TRK, raising the possibility of a TRK-rearranged neoplasm. All control slides are stained appropriately.

Immunohistochemical stains showed that while several cases were negative for both S100 protein and SOX10 (A, Case 5), a subset of cases (4/6, 67%) demonstrated focal expression of S100 protein (B, Case 6). Three cases showed focal positivity for both S100 protein (C, Case 1) and SOX10 (D, Case 1)
In five of the cases, next-generation sequencing (NGS) revealed a gene rearrangement between PRRX1 exon 1 at genomic position Chr1:g.170633600 and NCOA1 exon 13 at genomic position Chr2:g.24949458. Case 3 underwent additional testing with several sarcoma-targeted gene panels, including the SARCP panel at Mayo Clinic Laboratories, the Sarcoma Fusion NGS panel at Cleveland Clinic, and FusionPlex analysis at the University of Washington. All three targeted panels screened for alterations in the NCOA1 gene; however, they did not specifically search for gene rearrangements involving either PRRX1 or KMT2D and failed to identify any gene fusions. Further molecular testing using a TruSight RNA Pan-Cancer Panel (Illumina) eventually revealed a reciprocal fusion of KMT2D and PRRX1. The sample showed 3 co-existing breakpoint-defined subclones affecting adjacent exons 25, 26, and 27 of KMT2D. The morphologic features and immunohistochemical profile of the mesenchymal tumor with PRRX1::KMT2D fusion were the same as the mesenchymal tumors with PRRX1::NCOA1 fusion (Fig. 4).

Mesenchymal tumor with PRRX1::KMT2D fusion (Case 3). A 65-year-old female presented with a soft tissue mass involving her left posterior chest wall. Axial CT scan (A) showed that the mass (arrowheads) arose within the skeletal musculature near the uninvolved rib. Excision of the mass showed a multinodular bland spindle cell neoplasm growing in a myxo-collagenous stroma (B, C). Scattered vessels with prominent perivascular hyalinization were present (D). Immunohistochemical stains showed that the tumor cells were focally positive for both S100 protein (E) and SOX10 (F)
All patients with clinical follow-up (range, 4–16 months; median 9 months) were alive with no evidence of disease at last follow-up.
Discussion
Since the first description of PRRX1-rearranged mesenchymal tumors in 2019 by Lacambra et al. [3], 20 cases, including the six cases presented in this series, have been reported in the literature (Table 1). The most common fusion partner for PRRX1 is NCOA1 (n = 17), followed by KMT2D (n = 2) and NCOA2 (n = 1). Clinically, the tumors most often present as slow-growing nodules centered in the subcutaneous tissue of middle-aged patients (median, 40 years; range, 20–76 years) with an equal gender distribution (10 male, 10 female). The most common anatomic locations are the neck (n = 4), abdominal wall (n = 3), shoulder (n = 2), and groin (n = 2). The lesions are well-circumscribed, multi-nodular, and composed of bland spindle cells growing in a myxo-collagenous stroma with rope-like collagen bundles and inconspicuous mitotic activity. Cellularity is generally low but often focally increased; cytologic atypia is, at most, mild; and necrosis has not been reported. Furthermore, “staghorn-like” vessels, often present at the periphery of the tumor, have also been a frequent finding. A subset of cases demonstrates focal immunohistochemical expression of S100 protein (6/20, 30%) and SOX10 (at least 3/11, 27%). Since S100 and SOX10 co-expression is present in a significant subset of cases, it may be utilized as a useful diagnostic hint, while at the same time representing a potential diagnostic pitfall. Co-expression of these two markers also raises the possibility of partial neural or neuroectodermal differentiation, which may be explored further in subsequent studies. Of the fourteen cases with clinical follow-up, all patients treated with simple, conservative excision are alive with no evidence of disease, suggesting benign behavior; however, long-term follow-up is still warranted to fully understand the full biologic potential of this emerging entity.
PRRX1 (paired related homeobox 1) is a gene that encodes a DNA-binding protein that acts as a transcription co-activator that is important in development. Fusions involving PRRX1 have previously been reported in acute myelogenous leukemia [9]. In PRRX1-rearranged mesenchymal tumors, the most common fusion partner is nuclear receptor coactivator 1 (NCOA1), also known as steroid receptor coactivator-1 (SRC-1), which is a transcriptional coregulatory protein that contains nuclear receptor-interacting domains [10]. NCOA1 mediates transcriptional up-regulation by acetylating histones [11]. When PRRX1 is fused to NCOA1, the nuclear receptor binding protein of NCOA1 is lost, being replaced by exon 1 of PRRX1, whereas the transcriptional activation domains of NCOA1 remain intact. While less common than NCOA1, one tumor with PRRX1::NCOA2 has been reported [3]. NCOA2 fusions have also been described in other soft tissue tumors including mesenchymal chondrosarcoma [12], spindle cell rhabdomyosarcoma [13], uterine adenosarcoma [14], and biphenotypic sinonasal sarcoma [15], among others.
PRRX1-rearranged mesenchymal tumors can mimic both benign and malignant lesions. The bland spindle cells with rope-like collagen bundles and rare mast cells can resemble the RB1-deficient family of tumors, including spindle cell lipomas when rare areas with entrapped benign adipose tissue are present. The finding of CD34 positivity and loss of Rb1 expression, however, contrasts with the immunohistochemical profile of PRRX1-rearranged mesenchymal tumor. The focal staining for both S100 protein and SOX10 in a subset of PRRX1-rearranged mesenchymal tumors, along with the prominent perivascular hyalinization, could be mistaken for a schwannoma on limited sampling with core needle biopsy. However, the lack of Verocay bodies, lack of distinct Antoni A and B areas, and lack of strong, diffuse staining for both S100 protein and SOX10, could help to exclude schwannoma. The focal staining for S100 protein could further raise consideration for an unusual, non-ossifying variant of ossifying fibromyxoid tumor (OFMT); however, the lack of expression of desmin as well as the absence of PHF1 gene rearrangements eliminates this possibility. Nevertheless, the expression of SOX10 is not a feature of OFMT and helped exclude OFMT as a diagnostic consideration. The focal staining for S100 protein, along with diffuse expression of pan-TRK in one case, also raises the possibility of kinase-fused tumors, which can also have hyalinized blood vessels and myxoid stroma. In contrast to PRRX1-rearranged mesenchymal tumors, kinase-fused tumors often have an infiltrative growth pattern, rarely have ropey collagen bundles, often express CD34, and are not known to express SOX10. The presence of “staghorn-like” vessels at the periphery of the lesion can further mimic solitary fibrous tumor (and, interestingly, unsupervised hierarchical clustering of RNA-Seq data has shown that PRRX1-rearranged mesenchymal tumors cluster closely with solitary fibrous tumor [3]). Fortunately, the lack of nuclear staining with STAT6 excludes this possibility. The rare presence of fusions involving the NCOA2 gene raises the possibility of soft tissue angiofibroma, which has been described to have fusions involving AHRR::NCOA2 [16] and GTF2I::NCOA2 [17]. The lack of staining with EMA, which is frequently positive in soft tissue angiofibroma, and careful attention to morphologic features, particularly the different pattern of tumor vasculature, can help to distinguish these two entities. PRRX1-rearranged mesenchymal tumors can also resemble sarcomas, including low-grade fibromyxoid sarcoma (LGFMS), sclerosing epithelioid fibrosarcoma (SEF), and the recently described KMT2A-rearranged sarcomas. The lack of immunohistochemical expression of MUC4 could exclude both LGFMS and SEF, while the lack of usually more high-grade morphological features combined with NGS studies could help exclude a rare KMT2A-rearranged sarcoma.
Similar to PRRX1-rearranged mesenchymal tumors, NGS has identified another new subset of clinically significant fibroblastic tumors characterized by gene rearrangements involving KMT2A. In 2019, Yoshida et al. first described two sarcomas with KMT2A (MLL) fusions, one each having YAP1 and VIM partners [18]. Prior to being described in soft tissue tumors, lysine methyltransferase 2A (KMT2A) was known as a frequent fusion partner in ~ 10% of acute leukemias [19, 20], while fusions have also been reported in type B2 and B3 thymomas [21]. Within soft tissue pathology, KMT2A-rearranged sarcomas usually have infiltrative growth, distinct morphologic features resembling SEF when fused to YAP1, and aggressive behavior. In a subsequent study, Puls et al. described seven additional tumors with YAP1::KMT2A fusions, as well as one case with PRRX1::KMT2D fusion, which was notably distinct from the other tumors with KMT2A alterations [22]. Their case with PRRX1::KMT2D fusion morphologically resembled our Case 3, was multi-nodular, well-circumscribed without infiltrative borders, relatively hypocellular, had no areas resembling SEF, and lacked both mitotic activity and necrosis. Puls et al. conceded that the tumor was morphologically similar to those described by Lacambra et al. and noted prominent perivascular hyalinization as described in our cases. Furthermore, the patient with the previously described case of PRRX1::KMT2D-rearranged tumor was confirmed to be well and without disease at last clinical follow-up over 2 years after the publication of their article (personal communication with Drs. Puls and Flucke). Based on the morphologic similarities and seemingly benign clinical behavior, we think that these lesions with PRRX1::KMT2D fusions are best classified with the PRRX1-rearranged mesenchymal tumors as opposed to the aggressive KMT2A-rearranged sarcoma family.
KMT2D (also known as MLL2) encodes histone-lysine methyltransferase 2D belonging to the same family as KMT2A [23]. KMT2D predominantly monomethylates H3K4 whereas KMT2A shows mono and dimethyltransferase activity [24]. Somatic KMT2D loss-of-function mutations are frequently found in a variety of human cancers, including prostatic adenocarcinoma and lung squamous cell carcinoma [25, 26]. In sarcomas, a KMT2D::BCOR gene fusion has been identified in a large pelvic undifferentiated round cell sarcoma in a 10-year-old girl [27], and point mutations in KMT2D have been identified in approximately 25% of adamantinoma tumors [28]. While the characterization of soft tissue tumors with KMT2D rearrangements continues to evolve, it is important to note that both KMT2A and KMT2D are frequently not included in solid tumor or sarcoma-targeted gene panels due to the low prevalence of structured alterations in these tumors [29]. Fortunately, sarcoma-targeted gene panels continue to expand as new entities are described, and both KMT2A and KMT2D alterations can often be identified within sequencing panels for hematolymphoid neoplasms.
In summary, we present six additional cases of PRRX1-rearranged mesenchymal tumors, expanding the immunohistochemical profile with co-expression of S100 protein and SOX10. We also expand the molecular spectrum with a relatively novel PRRX1::KMT2D fusion, which appears to fit best within the family of PRRX1-rearranged mesenchymal tumors, and propose a revision of the provisional nomenclature from “PRRX1-NCOAx-rearranged fibroblastic tumor” to “PRRX1-rearranged mesenchymal tumor” to both accommodate non-NCOA1/2 fusion partners and allow for the possibility of partial neural or neuroectodermal differentiation. Due to the tumor’s ability to mimic other benign and malignant lesions, molecular support, including coverage of KMT2A and KMT2D, is essential to avoid misclassification and advance our understanding of this emerging entity.
References
WHO Classification of Tumours Editorial Board (2020) Soft tissue and bone tumours, 5th edn. IARC Press, Lyon
Folpe AL (2022) ‘I can’t keep up!’: an update on advances in soft tissue pathology occurring after the publication of the 2020 World Health Organization classification of soft tissue and bone tumours. Histopathology 80:54–75
Lacambra MD, Weinreb I, Demicco EG et al (2019) PRRX-NCOA1/2 rearrangement characterizes a distinctive fibroblastic neoplasm. Genes Chromosom Cancer 58(10):705–712
Dermawan JK, Azzato EM, Thangaiah JJ et al (2021) PRRX1-NCOA1-rearranged fibroblastic tumor: a clinicopathological, immunohistochemical and molecular genetic study of six cases of a potentially under-recognised, distinctive mesenchymal tumour. Histopathology 79:997–1003
Chen CH, Chang KC, Chuang CH et al (2022) The emerging PRRX1-NCOA fibroblastic neoplasm: a combined reappraisal of published tumors and two new cases. Virchows Arch 481:111–116
Cloutier JM, Maloney NS, Wang WL et al (2022) Pigmented PRRX1::NCOA1-rearranged fibroblastic tumor: A rare morphologic variant of an emerging mesenchymal tumor. J Cutan Pathol 49(9):802–807
Agaimy A, Stoehr R, Tögel L et al (2021) YAP1-MAML2-rearranged poroid squamous cell carcinoma (squamoid porocarcinoma) presenting as a primary parotid gland tumor. Head Neck Pathol 15(1):361–367
Nihous H, Baud J, Azmani R et al (2022) Clinicopathologic and molecular study of hybrid nerve sheath tumors reveals their common association with fusions involving VGLL3. Am J Surg Pathol 46(5):591–602
Nakamura T, Yamazaki Y, Hatano Y et al (1999) NUP98 is fused to PMX1 homeobox gene in human acute myelogenous leukemia with chromosome alteration t(1;11)(q23;p15). Blood 94:741–747
Ornate SA, Tsai SY, Tsai MJ et al (1995) Sequence and characterization of a coactivator for the steroid hormone receptor superfamily. Science 270:1354–1357
Ornate SA, Boonyaratanakornkit V, Spencer TE et al (1998) The steroid receptor coactivator-1 contains multiple receptor interacting and activation domains that cooperatively enhance the activation function 1 (AF1) and AF2 domains of steroid receptors. J Biol Chem 273:12101–12108
Wang L, Motoi T, Khanin R et al (2012) Identification of a novel, recurrent HEY1-NCOA2 fusion in mesenchymal chondrosarcoma based on a genome-wide screen of exon-level expression data. Genes Chromosom Cancer 51:127–139
Mosquera HM, Sboner A, Zhang L et al (2013) Recurrent NCOA2 gene rearrangements in congenital/infantile spindle cell rhabdomyosarcoma. Genes Chromosom Cancer 52:538–550
Piscuoglio S, Burke KA, Ng CK et al (2016) Uterine adenosarcomas are mesenchymal neoplasms. J Pathol 238:381–388
Le Loarer F, Laffont S, Lesluyes T et al (2019) Clinicopathologic and molecular features of a series of 41 biphenotypic sinonasal sarcomas expanding their molecular spectrum. Am J Surg Pathol 43(6):747–754
Bekers EM, Groenen P, Verdijk MAH et al (2017) Soft tissue angiofibroma: Clinicopathologic, immunohistochemical and molecular analysis of 14 cases. Genes Chromosom Cancer 56:750–757
Arbajian E, Magnusson L, Mertens F et al (2013) A novel GTF2I/NCOA2 fusion gene emphasizes the role of NCOA2 in soft tissue angiofibroma development. Genes Chromosom Cancer 52:330–331
Yoshida A, Arai Y, Tanzawa Y et al (2019) KMT2A (MLL) fusions in aggressive sarcomas in young adults. Histopathology 75:508–519
Winters AC, Bernt KM (2017) MLL-rearranged leukemias— an update on science and clinical approaches. Front Pediatr 5:11–13
Meyer C, Burmeister T, Groger D et al (2018) The MLL recombinome of acute leukemias in 2017. Leukemia 32:273–284
Massoth LR, Hung YP, Dias-santagata D et al (2020) Pan-cancer landscape analysis reveals recurrent KMT2A-MAML2 gene fusion in aggressive histologic subtypes of thymoma. JCO Precis Oncol 4:109–115
Puls F, Agaimy A, Flucke U et al (2020) Recurrent fusions between YAP1 and KMT2A in morphologically distinct neoplasms within the spectrum of low-grade fibromyxoid sarcoma and sclerosing epithelioid fibrosarcoma. Am J Surg Pathol 44:594–606
Froimchuk E, Jang Y, Ge K (2017) Histone H3 lysine 4 methyltransferase KMT2D. Gene 627:337–342
Rao RC, Dou Y (2015) Hijacked in cancer: the KMT2 (MLL) family of methyltransferases. Nat Rev Cancer 15:334–346
Lv S, Wen H, Shan X et al (2019) Loss of KMT2D induces prostate cancer ROS-mediated DNA damage by suppressing the enhancer activity and DNA binding of antioxidant transcription factor FOX03. Epigenetics 14(12):1194–1208
Pan Y, Han H, Hu H et al (2023) KMT2D deficiency drives lung squamous cell carcinoma and hypersensitivity to RTK-RAS inhibition. Cancer Cell 41(1):88–105
Kao YC, Owosho AA, Sung YS et al (2018) BCOR-CCNB3 fusion positive sarcomas: a clinicopathologic and molecular analysis of 36 cases with comparison to morphologic spectrum and clinical behavior of other round cell sarcomas. Am J Surg Pathol 42:604–615
Ali NM, Niada S, Morris MR et al (2019) Comprehensive molecular characterization of adamantinoma and OFD-like adamantinoma bone tumors. Am J Surg Pathol 43:965–974
Massoth LR, Hung YP, Nardi V et al (2020) Pan-sarcoma genomic analysis of KMT2A rearrangements reveals distinct subtypes defined by YAP1-KMT2A-YAP1 and VIM-KMT2A fusion. Mod Pathol 33:2307–2317
Acknowledgements
The authors wish to thank Dr. Francisco Llamas-Gutierrez (CHU de Rennes, France), who kindly provided clinical follow-up information for Case 6, Dr. Corinne Bouvier (APHM Marseille) for providing one case, Dr. Florian Puls and Dr. Uta Flucke for kindly providing clinical follow-up information on the previously published case of PRRX1::KMT2D-rearranged tumor, and Frederik Hans Skarstedt for his expertise in graphical design.
Funding
FLL is supported by grants from the charity Fondation Bergonié and Au Fil d’Oriane.
Author information
Authors and Affiliations
Contributions
Laura Warmke contributed a case, interpreted the results, collected data, and prepared the manuscript draft. Michael Michal and Petr Martinek analyzed and interpreted the results and performed molecular analysis. Nasir Ud Din contributed a case and collected imaging findings. Abbas Agaimy helped with study conception and design and data collection. Raul Perret, François Le Loarer, and Isabelle Hostein contributed a case and helped with the analysis and interpretation of results. Lysandra Voltaggio contributed a case and helped with data collection. John Gross contributed a case, helped with study conception and design, and performed analysis and interpretation of results. All authors reviewed the results and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study was performed in accordance with the ethical standards of the participating institutions. No animals were involved in this research.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Warmke, L.M., Michal, M., Martínek, P. et al. “PRRX1-rearranged mesenchymal tumors”: expanding the immunohistochemical profile and molecular spectrum of a recently described entity with the proposed revision of nomenclature. Virchows Arch 483, 207–214 (2023). https://doi.org/10.1007/s00428-023-03575-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-023-03575-w