
Abstract
Different guidelines for colorectal cancer (CRC) pathology reporting have been published. We aimed to identify differences between publicly available CRC reporting guidelines and to survey pathologists from different countries to establish the degree of guideline implementation in local routine practice. We compared all core and non-core items of CRC reporting guidelines to identify discrepancies. We then created a survey, which was sent out to 782 pathologists practicing in 30 different countries. It included questions on the demographics of the reporting pathologist as well as resection specimen handling and microscopic evaluation, grading, staging, and additional techniques, such as immunohistochemistry or molecular pathology. First, core and non-core items of five national CRC reporting guidelines were compared and 12 items were found to differ. Different items are considered core or non-core by different guidelines and more than one TNM staging edition was applied across guidelines. The survey was completed by 143 pathologists from 30 countries. We identified differences between local practice and guidelines with potential clinical impact, e.g., tumor budding was never reported by 28.7% of responders, although it has prognostic value for survival in stage II CRC. This is the first international study comparing CRC pathology reporting guidelines with real-world local practices. There are differences in CRC pathology reporting guidelines and in guideline implementation into local practice, both with potential impact on patient care. Harmonization of datasets, use of templates, and audits of local pathology practice are needed to ensure best possible quality of CRC pathology reporting.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Colorectal cancer (CRC) is the third most common diagnosed cancer and the fourth most common cause of cancer death in the world, with 1.4 million new cases and 694,000 deaths in 2012 [1]. Standardized diagnostic pathology procedures are a key factor for appropriate treatment of CRC patients [2].
CRC pathology reporting guidelines have been published in several countries to ensure that all clinically relevant information is included in the pathology report. They usually include so-called “core” and “non-core” elements. Core items are required for cancer staging, patient management, and prognosis and are supported by strong evidence, e.g., resection margin status [3]. Non-core elements should ideally be included in the report to meet clinical or research needs at the local level, e.g., tumor budding (TB) [3]. Interestingly, the same item (for example perineural invasion (PNI)) is considered core in one national dataset and non-core in the dataset of another country [3, 4], which can lead to problems when comparing data especially in the setting of an international clinical trial or cancer registries.
A number of CRC pathology reporting audits have been conducted in the past. Most of them were performed at either local [5,6,7,8,9], regional [10,11,12,13,14,15,16,17], or national level [18, 19] and assessed the adherence to national pathology guidelines by reviewing pathology reports.
The aim of our study was to (a) compare CRC pathology reporting guidelines from different countries and to (b) assess how local pathologists implement existing guidelines.
Materials and methods
Comparing national CRC reporting guidelines
Prior to creating the survey, the authors reviewed CRC reporting guidelines from the Royal College of Pathologists, London (UK) (RCPath) (3rd edition, 2014) [3], the Royal College of Pathologists of Australasia (RCPA) (3rd edition, 2016) [20], the College of American Pathologists (CAP) (7th edition, 2016) [4], the Spanish Society of Pathology (SEAP) “Libro blanco 2017” (5th edition, 2017) [21], and the Italian group of Digestive Pathology and Italian Society of Pathology and Diagnostic Cytology—Italian division of International Academy of Pathology (GIPAD/SIAPEC-IAP) guidelines (2011) [22]. These guidelines were chosen because they represented major pathology organizations and because they were the most updated versions at the time when survey was sent out. By the time of the publication, RCPath dataset and CAP protocol have been updated in October 2017 and June 2017 respectively [23, 24].
We included core as well as non-core items. For each item, we recorded if it was core or non-core in the guideline we reviewed. Moreover, we recorded the differences in wording or values encountered in our search.
Designing the survey
The following items were included in the survey: demographic data of the reporting pathologist, CRC resection specimen handling, microscopic evaluation of the resection specimens, grading and staging system used, use of additional techniques such as immunohistochemistry or molecular pathology, and name of the guideline(s) used by the responder. The choice of these items was based on the identified differences between different national datasets. In total, the survey contained 35 questions concerning CRC pathology reporting, of which 23 questions focused on local practice, 8 questions on the characteristics of the survey participants and their institution, and 4 questions on the implementation of CRC pathology guidelines or templates for reporting. The full questionnaire can be found in the electronic supplementary material. The survey was designed by three pathologists with special interest in gastrointestinal (GI) pathology (M.U., H.G., and J-F.F.). A pilot version was tested by an independent team of three general pathologists. The revised and final questionnaire was emailed to 782 recipients from academic institutions, general hospitals, cancer centers, and private practice in 33 different countries in June 2017. Our network included pathologists involved in the European Organisation for Research and Treatment of Cancer (EORTC), European Society of Pathology (ESP) Gastrointestinal Working Group, and other organizations, such as the European Network of Gastrointestinal Pathology among others.
Descriptive statistical analysis was performed. We used proportions for qualitative variables. The analyses were conducted using SAS 9.4 (SAS, Cary, NC).
Results
Comparison of core and non-core items of five national CRC reporting guidelines
Currently, the CRC pathology reporting guidelines differ on a national [3, 4, 20,21,22] as well as local level (data from a survey responder) with respect to what is recognized as mandatory (core) or optional (non-core) item.
For example, regarding microscopic evaluation, RCPath [3] includes venous invasion as core data and lymphatic invasion as non-core data, which is similar to GIPAD/SIAPEC-IAP guidelines [22]. The latter, however, require only a statement about the presence or absence of extramural venous invasion. CAP considers distinction between venous and lymphovascular invasion (LVI) as optional, while RCPA and SEAP consider it as core item and require distinction between intra- or extramural. Interestingly, PNI is a core data item only in the CAP protocol, while SEAP does not cover this item at all. The other guidelines include it as a non-core item [3, 4, 20,21,22].
There are minor differences between the guidelines with respect to the assessment of tumor regression grade after chemo(radio)therapy. All of the reviewed datasets, except GIPAD/SIAPEC-IAP, present a four-tiered system based on a modified Ryan Scheme [25]. However, each guideline uses a slightly different wording. GIPAD/SIAPEC-IAP includes a three-tiered scheme based on the RCPath guidelines [3, 4, 20,21,22].
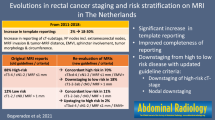
Other important differences between the datasets include recommendations on which TNM staging edition should be used. RCPA, CAP, SEAP, and GIPAD/SIAPEC-IAP protocols were based on the AJCC or AJCC/UICC 7th edition of TNM [26], while RCPath dataset was based on the UICC 5th edition of TNM [27]. The Dutch CRC reporting guideline also recommended use of TNM 5th [28]. The use of different TNM staging systems can potentially lead to over- or understaging of the same specimen which can impact treatment decisions or eligibility criteria for entry into a clinical trial. However, the updated versions of RCPath dataset and CAP protocols refer to the 8th TNM edition [23, 24].
Furthermore, there are items included in some but not all of the guidelines. One example is the maximum distance of tumor spread beyond the muscularis propria in millimeters, which is a core data item in RCPath dataset [3], while it is recommended in RCPA guidelines as an alternative to TNM [20] and not mentioned at all in the CAP protocol [4], SEAP guidelines [21], or in GIPAD/SIAPEC-IAP guidelines [22]. Details on items that differ between guidelines can be found in Table 1.
Characteristics of the responders
A total of 143 responses (response rate 18.3%) were received from 30 countries, 138 (96.5%) of which were from Europe and 5 (3.5%) from non-European countries (Fig. 1). The database was cleaned by deleting double data entries. There were 95 (66.4%) of responders who declared working in academic institutions, 35 (24.5%) in general hospitals, 19 (13.3%) in cancer centers, and 14 (9.8%) in private practice. Seventy-seven (53.8%) responders were pathologists with a special interest in GI pathology and 66 (46.2%) responders were general pathologists. The characteristics of the pathologists are presented in Table 2 and Fig. 2.

Countries participating in the CRC pathology reporting survey

Members of gastrointestinal pathology specialized organization
As the survey items were not obligatory, 28 of 35 questions were only answered by some of the responders amounting to missing responses from 2 to 9 responders per question (missing data 1.4–6.3%). One hundred thirty-five (94.4%) responders answered at least 30 questions. The percentages presented in the results are proportions of all respondents (n = 143 being 100%), unless stated otherwise. Although the majority of the responders were European (n = 138), we took into account also the responders from non-European countries, to get a broader overview of pathology reporting guidelines used worldwide.
CRC resection specimen handling
Fifty-eight (40.6%) departments receive colon and rectum resections fresh, 10 (7.0%) receive only rectum resections fresh and 71 (49.7%) of the responders receive colon and rectum resections fixed. For further details on specimen handling per responder, see Table 3.
Microscopic evaluation of CRC specimens
LVI was always reported by 131 responders (91.6%), while 10 (7.0%) responders reported it only when positive. The level of the deepest venous spread was reported by 82 (57.3%) and omitted by 52 (36.4%) responders. PNI was always reported by 103 (72%) responders, while 32 (22.4%) responders reported it only when positive, and 6 (4.2%) responders never reported it. TB was always reported by 52 (36.4%) responders, while 48 (33.6%) responders reported it only in selected cases and 41 (28.7%) responders never reported it. For details, see Table 3.
Grading and staging system used for CRC specimens
Regarding staging system, the most commonly applied was the 8th edition of TNM which was used by 55 responders (38.5%), followed by the 7th edition (n = 50, 35.0%), the 5th edition (n = 34, 23.8%), and the 6th edition (n = 1, 0.7%). The use of the 5th edition of TNM is related to responders from the UK (n = 28) and the Netherlands (n = 6), as RCPath guidelines (3rd edition) and Dutch guidelines were based on this edition at the time of the survey. Interestingly, 17.8% (n = 5) of the UK-based responders nevertheless used either TNM 7th or 8th edition. While the majority of the pathologists used only TNM for staging, 42 (29.4%) responders also used other systems, such as the Dukes or Astler Coller staging systems. For details, see Table 3.
Use of additional techniques (IHC, molecular pathology)
Forty-three (30.1%) responders performed microsatellite instability testing for every case, while 91 (63.6%) responders performed it in specific cases. For details, see Table 3.
Use of guidelines/proformas for CRC specimen reporting
Responders most commonly followed their national or local guidelines (n = 59; 41.3%, excluding those who followed RCPath), RCPath (n = 50; 35.0%), or CAP protocols (n = 42; 29.4%), respectively, while RCPA was used by 1 responder (0.7%), and 4 responders (2.8%) did not use any guidelines. Fifty (36.2%) out of 138 European pathologists (n = 138, 100%) used the RCPath guidelines, 60 (43.4%) national or local guidelines (excluding those who marked also RCPath), 37 (26.8%) the CAP protocols, while 4 (2.9%) did not use any guidelines. Twenty-eight (n = 28, 100%) UK pathologists followed the RCPath guidelines, while 22 (n = 115, 19.2%) non-UK pathologists also used these guidelines. For more details, see Table 3.
Discussion
Our study aimed to identify differences of existing CRC pathology reporting guidelines and to review local practice of pathologists in different countries, with the emphasis on whether and how local pathologists implement guidelines. To address these issues, a survey was sent out to pathologists practicing in different countries. Our survey shows that there is a wide variability among pathologists regarding which guideline they use and how strictly they follow individual recommendations in their daily practice. The differences we found are based on the fact that some data items were considered core or non-core, depending on the guidelines and that different TNM staging editions were recommended by different guidelines.
Interestingly, irrespective of the differences in the recommendations of the individual guideline, lymphovascular status was recorded by nearly all responders. This is reassuring, as LVI has been suggested as a prognostic factor for early-stage CRC and the presence of extramural vascular invasion is considered one of the high-risk factors in stage II CRC with impact on adjuvant treatment decisions [32]. PNI was reported by 72% of the responders. However, responders indicating not to report PNI deviate from all the guidelines we reviewed except the SEAP guideline, which does not include this item. TB is currently reported (either “always” or “only when positive”) by 70% of the responders and assessment methods applied by our responders differ. We believe, this is because the international standard on TB reporting has only been published recently [35]. TB is a non-core item, according to all the guidelines. It was found to be an independent predictor of lymph node metastasis in pT1 CRC and of survival in stage II CRC and can influence treatment decisions [32]. For the items, which are present in all or almost all of the analyzed guidelines (LVI, PNI, TB, or R margin status), we can identify non-compliers, as the percentage of responders, who never report certain item. For LVI, it is 0%, as all the responders report it. When it comes to PNI, it is 4.2% and R margin status is 3.5%. For TB, the percentage of those who do not report it is higher, mainly 28.7%; however, as mentioned above, the assessment was not standardized until recently. As these percentages are low, we could conclude that the compliance with guidelines is good. However, this criterium of evaluation can be somewhat controversial, as the total number of reported and omitted items should be analyzed for each responder.
Another difference between CRC guidelines is the recommended staging system. RCPA, CAP, SEAP, and GIPAD/SIAPEC-IAP protocols were based on the AJCC or AJCC/UICC 7th edition of TNM [26], while RCPath and the Dutch guidelines were based on the Union for International Cancer Control (UICC) 5th edition of TNM [27].Therefore, to avoid confusion, the information on which TNM edition was used should always be included in the pathology report. Current RCPath and CAP guidelines have been updated with the 8th edition of UICC and AJCC TNM staging respectively [39, 40]. Although the changes between the subsequent editions tend to be minor, Nagtegaal et al. highlighted how these modifications may affect the diagnosis and treatment decisions for CRC patients, using tumor deposits in pericolic fat as an example. There were different definitions throughout three editions (TNM5, TNM6, TNM7), which led to restaging of tumors, with a clear impact on the number of patients selected for chemotherapy [38]. This example shows how pathology reporting affects staging and therefore respective clinical decisions. Depending on the guidelines followed, patient could be staged with TNM 5th or 7th edition, which means potentially different treatment modalities.
Testing for microsatellite instability (MSI) is another issue where recommendations are currently not standardized across the guidelines. 63.6% of responders declared different criteria for mismatch repair deficiency assessment, while 30.1% of responders test all CRC. Universal testing is recommended by the newest guidelines of National Institute for Health and Care Excellence (NICE) [41] and the European Society for Medical Oncology (ESMO) guidelines [42]. The pathology datasets make reference to other guidelines, such as the revised Bethesda [43] or Amsterdam II criteria [44]; therefore, there is no unique approach. This item is important as it is prognostic for stage II CRC [32], potentially predictive for response to immune-checkpoint inhibitors in metastatic CRC [45] and is a screening tool for Lynch syndrome [41].
It is interesting to reflect on why there are differences between the national guidelines. We believe that these could be dictated by specific health care needs and standards of treatment in each country. They also depend on the standard procedures and protocols that define guidelines development, such as guidelines for authors of datasets of RCPA [46], and these can differ across countries. The differences depend also on who the stakeholders are and on their input in the guidelines, e.g., RCPath guidelines are consulted with five different organizations, among others, British Society of Gastroenterology or National Cancer Research Institute. Finally, different evidence-level scales serve as a reference for different guidelines. RCPath dataset is based on levels of evidence modified from Palmer K et al. [47]. RCPA and CAP use National Health and Medical Research Council (NHMRC) levels of evidence as a reference [46], while SEAP guidelines are based on other national guidelines, such as CAP protocols, RCPath, or RCPA datasets. GIPAD guidelines refer to other evidence scales; however, the source is not indicated in the text. Generally, core items are supported by strong evidence from scientific literature. When this is not the case, it is the expert consensus which decides on the relevance of including the item [46]. As the national experts are different in each country, it is only logical that their consensus may differ from that of their colleagues in other countries.
Although in our survey we focused on CRC surgical resection specimens only, it is worth mentioning that the pathology reporting guidelines also describe handling of local resections. There is a section dedicated to local excision in RCPath, CAP, SEAP, and GIPAD guidelines. The minimal data included in the report of local excision is similar to that of the resection specimen; however, there is a number of specific features that need to be addressed. These are prognostic factors used for risk assessment of potential lymph node metastasis, distant metastasis, and survival. They determine the necessity of a more radical surgical resection. These factors are tumor size, poor differentiation, the depth of invasion into the submucosa, submucosal lymphatic or venous invasion, positive resection margin, and TB [3, 4, 21, 22].
In conclusion, we compared different CRC pathology reporting guidelines used around the world and conducted an international survey. Our intention was to highlight differences among these guidelines and review how these were implemented in the local practice of pathologists.
To our knowledge, this is the first survey that focused on clinical practice of local pathologists and reached responders from different countries. Our survey shows that there is a gap between CRC pathology reporting guidelines and everyday pathology practice raising the question, how compliance with guidelines can be improved. We believe, it is not a matter of updating the guidelines that would reinforce the adherence to them. It is awareness of the clinical importance of individual items that could improve the compliance to the guidelines and the quality of the pathology report. This could be achieved by closer cooperation between specialists from different clinical areas, e.g., by joint scientific sessions or tumor boards. Regular audits of local pathology practice seem to be a potential way of reinforcing the adherence to the guidelines [48]. Whatever the differences are, the guidelines serve the same purpose: to set up the standards of pathology reporting in order to produce quality data for patient prognosis and management. Each of the guidelines we studied provides a template or a checklist to ensure the inclusion of important items. This approach is evidence-based, as use of proformas in pathology reporting have improved completeness of pathology reports [49, 50]. Ideally, such proformas would be agreed internationally. This universal approach is represented by International Collaboration on Cancer Reporting (ICCR), which consists of representatives from major pathology organizations and its goal is to create internationally standardized and evidence-based datasets for the pathology reporting of cancer [51]. The ICCR CRC dataset, however, is still in the process of development. Whether the publication of an international CRC dataset would eradicate the problem of guideline deviations remains to be seen. However, following a single international standard would have several advantages. One of the main beneficiaries would be patient management and clinical research. As clinical trials often take place in different countries and the data is collected from sites and centralized, the best solution to retrieve and analyze the data is to assure that they are in accordance with internationally approved guidelines. This is particularly important in pathology, where the diagnosis depends on the guidelines, as entity names and classification are constantly being updated. It would ensure use of consistent terminology and correct interpretation of data.
On the other hand, one can argue that a universal approach has also its shortcomings. The development of international guidelines can be disposed to limitations in terms of policies and available procedures in different countries. Also, the economic issues create a gap between developing countries and economically stable countries. The resources would not allow certain countries or institutions to perform certain procedures, like molecular testing. Therefore, the unified guidelines would have to consider these limitations. The solution could be a basic dataset, focused only on clinically relevant items, such as risk factors and items with a high level of evidence.
A limitation of our study was the missing data of a number of responders and the small size of subgroups (e.g., by nationality), which did not allow comparative analysis. Therefore, no statistically significant associations were found. However, we believe that the results are valid and should be made available to the public, as they address an important issue. We also found it impossible to directly link certain practice items to the guidelines, as in some cases the responders followed more than one type of guidelines. The generic term “national / local guidelines” did not allow us to know exactly which national or local guidelines the responders referred to in their answers. Moreover, the number of reviewed guidelines was limited. The study was also affected by the update in RCPath and CAP protocols, as the survey was performed before their release. However, in our opinion, this is a valid study, with the survey results compared to the recommendations available at that time.
In summary, we presented the variability of guidelines on CRC pathology reporting and the differences in adherence to these at a level of local practice. We believe that it is important to highlight these discrepancies among national guidelines and their local implementation because of their direct impact on patient management. This snapshot of real-life practice should challenge pathologists to perform critical review of their local practices, develop a strategy for harmonization, and raise the standards of quality in pathology.
References
Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F (2015) Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 136:E359–E386. https://doi.org/10.1002/ijc.29210
Nakhleh RE (2011) Quality in surgical pathology communication and reporting. Arch Pathol Lab Med 135:1394–1397
Dataset for colorectal cancer histopathology reports (3rd edition). https://www.rcpath.org/resourceLibrary/dataset-for-colorectal-cancer-histopathology-reports%2D%2D3rd-edition-.html. Accessed December 7, 2017
Tang LH, Branton P, Burgart LJ et al (2016) Protocol for the examination of specimens from patients with primary carcinoma of the colon and rectum. Accessed December 7, 2017
Obaseki D (2015) An audit of colorectal cancer histopathology reports in a tertiary health care center in Nigeria. Niger J Gastroenterol Hepatol 7:19–24
Nambiar A, Vivek N, Bindu MR, Sudheer OV, Bai L (2010) Completeness of low anterior resection pathology report: a hospital-based audit with recommendations on improving reporting. Indian J Cancer 47:156–159. https://doi.org/10.4103/0019-509X.63010
Messenger DE, McLeod RS, Kirsch R (2011) What impact has the introduction of a synoptic report for rectal cancer had on reporting outcomes for specialist gastrointestinal and nongastrointestinal pathologists? Arch Pathol Lab Med 135:1471–1475. https://doi.org/10.5858/arpa.2010-0558-OA
Chan NG, Duggal A, Weir MM, Driman DK (2008) Pathological reporting of colorectal cancer specimens: a retrospective survey in an academic Canadian pathology department. Can J Surg 51:284–288
Cross SS, Feeley KM, Angel CA (1998) The effect of four interventions on the informational content of histopathology reports of resected colorectal carcinomas. J Clin Pathol 51:481–482
Woods YL, Mukhtar S, McClements P, Lang J, Steele RJ, Carey FA (2014) A survey of reporting of colorectal cancer in Scotland: compliance with guidelines and effect of proforma reporting. J Clin Pathol 67:499–505. https://doi.org/10.1136/jclinpath-2013-202060
Olszyna-Serementa M, Kołodziejczyk M, Sprawka A, Nasierowska-Guttmejer A, Bujko K (2009) The quality of pathological reports of postoperative specimens in rectal cancer: an audit from the Mazovia region. Pol J Pathol 60:130–133
Eon Y, Le Douy J-Y, Lamer B, Battini J, Bretagne J-F (2006) Quality and completeness of histopathology reports of rectal cancer resections. Results of an audit in Brittany. Gastroenterol Clin Biol 30:235–240
Bull AD, Biffin AH, Mella J, Radcliffe AG, Stamatakis JD, Steele RJ, Williams GT (1997) Colorectal cancer pathology reporting: a regional audit. J Clin Pathol 50:138–142
Chapuis PH, Chan C, Lin BPC, Armstrong K, Armstrong B, Spigelman AD, O’Connell D, Leong D, Dent OF (2007) Pathology reporting of resected colorectal cancers in New South Wales. ANZ J Surg 77:963–969. https://doi.org/10.1111/j.1445-2197.2007.04291.x
Winn RD, Robinson DR, Farmer KC, Bell SW (2008) Deficiencies in pathological reporting of colorectal cancer in Victoria. ANZ J Surg 78:796–799. https://doi.org/10.1111/j.1445-2197.2008.04653.x
Idowu MO, Bekeris LG, Raab S, Ruby SG, Nakhleh RE (2010) Adequacy of surgical pathology reporting of cancer: a College of American Pathologists Q-Probes study of 86 institutions. Arch Pathol Lab Med 134:969–974. https://doi.org/10.1043/2009-0412-CP.1
Srigley J, Lankshear S, Brierley J, McGowan T, Divaris D, Yurcan M, Rossi R, Yardley T, King MJ, Ross J, Irish J, McLeod R, Sawka C (2013) Closing the quality loop: facilitating improvement in oncology practice through timely access to clinical performance indicators. J Oncol Pract 9:e255–e261. https://doi.org/10.1200/JOP.2012.000818
Haugland HK, Casati B, Dørum LM, Bjugn R (2011) Template reporting matters - a nationwide study on histopathology reporting on colorectal carcinoma resections. Hum Pathol 42:36–40. https://doi.org/10.1016/j.humpath.2010.06.009
Keating J, Lolohea S, Kenwright D (2003) Pathology reporting of rectal cancer: a national audit. N Z Med J 116:U514
Colorectal Cancer Structured Reporting Protocol (3rd Edition 2016) https://www.rcpa.edu.au/Library/Practising-Pathology/Structured-Pathology-Reporting-of-Cancer/Cancer-Protocols/Gastrointestinal/Protocol-colorectal-cancer. Accessed December 7, 2017
Libro Blanco de la Anatomía Patológica en España 2017 https://www.seap.es/documents/10157/1546214/LBAP_2017+-.pdf/c3fcb02b-3b08-4e6c-bbac-eda437485dc6. Accessed December 7, 2017
Lanza G, Messerini L, Gafà R, Risio M, Gruppo Italiano Patologi Apparato Digerente (GIPAD), Società Italiana di Anatomia Patologica e Citopatologia Diagnostica/International Academy of Pathology, Italian division (SIAPEC/IAP) (2011) Colorectal tumors: the histology report. Dig Liver Dis 43:S344–S355. https://doi.org/10.1016/S1590-8658(11)60590-2
Loughrey MB, Quirke P, Shepherd NA (2017) G049 Dataset for histopathological reporting of colorectal cancer. The Royal College of Pathologists, London. https://www.rcpath.org/profession/guidelines/cancer-datasets-and-tissue-pathways.html. Accessed 25 Sept 2018
Kakar S, Shi C, Berho ME, Driman DK, Fitzgibbons P, Frankel WL et al (2017) Protocol for the examination of specimens from patients with primary carcinoma of the colon and rectum. Arch Pathol Lab Med 133:1539–1551. https://doi.org/10.1043/1543-2165-133.10.1539
Ryan R, Gibbons D, Hyland JMP, Treanor D, White A, Mulcahy HE, O’Donoghue DP, Moriarty M, Fennelly D, Sheahan K (2005) Pathological response following long-course neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Histopathology 47:141–146. https://doi.org/10.1111/j.1365-2559.2005.02176.x
Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A (eds) (2010) AJCC cancer staging handbook, 7th edn. Springer, New-York
Sobin LH, Fleming ID (1997) TNM classification of malignant tumors, fifth edition. Cancer 80:1803–1804. https://doi.org/10.1002/(SICI)1097-0142(19971101)80:9<1803::AID-CNCR16>3.0.CO;2-9
Nederland VKG (2015) Richtlijn: Erfelijke darmkanker (2.0) https://www.mdl.nl/sites/www.mdl.nl/files/richlijnen/Erfelijke_darmkanker_-_december_2015_def.pdf. Accessed January 17, 2018
Chang GJ, Rodriguez-Bigas MA, Skibber JM, Moyer VA (2007) Lymph node evaluation and survival after curative resection of colon cancer: systematic review. J Natl Cancer Inst 99(6):433–441
Gavioli M, Luppi G, Losi L, Bertolini F, Santantonio M, Falchi AM, D’Amico R, Conte PF, Natalini G (2005) Incidence and clinical impact of sterilized disease and minimal residual disease after preoperative radiochemotherapy for rectal cancer. Dis Colon Rectum 48(10):1851–1857
Lim SB, Yu CS, Jang SJ, Kim TW, Kim JH, Kim JC (2010) Prognostic significance of lymphovascular invasion in sporadic colorectal cancer. Dis Colon Rectum 53(4):377–384
Labianca R, Nordlinger B, Beretta GD et al (2013) Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 24:vi64–vi72. https://doi.org/10.1093/annonc/mdt354
Betge J, Pollheimer MJ, Lindtner RA, Kornprat P, Schlemmer A, Rehak P, Vieth M, Hoefler G, Langner C (2012) Intramural and extramural vascular invasion in colorectal cancer: prognostic significance and quality of pathology reporting. Cancer 118(3):628–638
Liebig C, Ayala G, Wilks J, Verstovsek G, Liu H, Agarwal N, Berger DH, Albo D (2009) Perineural invasion is an independent predictor of outcome in colorectal cancer. J Clin Oncol 27(31):5131–5137
Lugli A, Kirsch R, Ajioka Y, Bosman F, Cathomas G, Dawson H, el Zimaity H, Fléjou JF, Hansen TP, Hartmann A, Kakar S, Langner C, Nagtegaal I, Puppa G, Riddell R, Ristimäki A, Sheahan K, Smyrk T, Sugihara K, Terris B, Ueno H, Vieth M, Zlobec I, Quirke P (2017) Recommendations for reporting tumor budding in colorectal cancer based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod Pathol 30:1299–1311. https://doi.org/10.1038/modpathol.2017.46
Bori R, Sejben I, Svébis M, Vajda K, Markó L, Pajkos G, Cserni G (2009) Heterogeneity of pT3 colorectal carcinomas according to the depth of invasion. Pathol Oncol Res 15(3):527–532 https://doi.org/10.1007/s12253-009-9149-x
Birbeck KF, Macklin CP, Tiffin NJ, Parsons W, Dixon MF, Mapstone NP, Abbott CR, Scott N, Finan PJ, Johnston D, Quirke P (2002) Rates of circumferential resection margin involvement vary between surgeons and predict outcomes in rectal cancer surgery. Ann Surg 235(4):449–457
Nagtegaal ID, Tot T, Jayne DG et al (2011) Lymph nodes, tumor deposits, and TNM: are we getting better? J Clin Oncol 29:2487–2492. https://doi.org/10.1200/JCO.2011.34.6429
Brierley JD, Gospodarowicz MK, Wittekind C (eds) (2016) International Union Against Cancer (UICC). TNM classification of malignant tumours, 8th edn. New York, Wiley-Blackwell
Amin MB, Edge SB, Greene FL et al (eds) (2017) American Joint Committee on Cancer (AJCC) cancer staging manual, 8th edn. New York, Springer
Molecular testing strategies for Lynch syndrome in people with colorectal syndrome in people with colorectal cancer (2017) https://www.nice.org.uk/guidance/dg27/resources/molecular-testing-strategies-for-lynch-syndrome-in-people-with-colorectal-cancer-pdf-1053695294917. Accessed December 8, 2017
Balmana J, Balaguer F, Cervantes A, Arnold D, ESMO Guidelines Working Group (2013) Familial risk-colorectal cancer: ESMO Clinical Practice Guidelines. Ann Oncol 24:vi73–vi80. https://doi.org/10.1093/annonc/mdt209
Umar A, Boland CR, Terdiman JP, Syngal S, Chapelle A, Ruschoff J, Fishel R, Lindor NM, Burgart LJ, Hamelin R, Hamilton SR, Hiatt RA, Jass J, Lindblom A, Lynch HT, Peltomaki P, Ramsey SD, Rodriguez-Bigas MA, Vasen HFA, Hawk ET, Barrett JC, Freedman AN, Srivastava S (2004) Revised Bethesda Guidelines for hereditary nonpolyposis colorectal cancer (Lynch syndrome) and microsatellite instability. J Natl Cancer Inst 96:261–268
Vasen HF, Watson P, Mecklin JP, Lynch HT (1999) New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology 116:1453–1456
Van Cutsem E, Cervantes A, Adam R et al (2016) ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol 27:1386–1422. https://doi.org/10.1093/annonc/mdw235
RCPA (Royal College of Pathologists of Australasia) (2009) Guidelines for authors of structured cancer pathology reporting protocols. RCPA, Surry Hills
Palmer K, Nairn N, Guideline Development Group (2008) Management of acute gastrointestinal blood loss: summary of SIGN guidelines. BMJ 337:a1832
Appleton MA, Douglas-Jones AG, Morgan JM (1998) Evidence of effectiveness of clinical audit in improving histopathology reporting standards of mastectomy specimens. J Clin Pathol 51:30–33
Sluijter CE, van Lonkhuijzen LR, van Slooten NID, Overbeek LI (2016) The effects of implementing synoptic pathology reporting in cancer diagnosis: a systematic review. Virchows Arch 468(6):639–649. https://doi.org/10.1007/s00428-016-1935-8
Srigley JR, McGowan T, Maclean A, Raby M, Ross J, Kramer S, Sawka C (2009) Standardized synoptic cancer pathology reporting: a population-based approach. J Surg Oncol 99(8):517–524. https://doi.org/10.1002/jso.21282
International Collaboration on Cancer Reporting Guidelines for the Development of ICCR Datasets International Collaboration on Cancer Reporting (2016). http://www.iccr-cancer.org/ICCR/media/Documents/Guidelines-for-the-development-of-ICCR-datasets-2-6.pdf. Accessed January 16, 2018
Acknowledgements
The responders: Federica Grillo, Frank Carey, Snjezana Frkovic-Grazio, Camille Boulagnon-Rombi, Maurice Loughrey, Francois Paraf, Katerina Kamaradova, Peggy Dartigues, Bettina Rees, Timo Gaiser, Clare Fuller, Marie-Christine Saint-Paul, Rui Oliveira, Stefania Landolfi, Emyr Wyn Benbow, Billaud Elsa, Ricardo Fonseca, Anne Jouret-Mourin, Kevin West, Remi Picot, Eugene Mutijima, Cinzia Giacometti, Rob Goldin, Michael Taris, Yolanda Rodriguez-Gil, Ruth Düttmann, Nigel Scott, Marie-Danièle Diebold, Alejandro García-Varona, Dina Tiniakos, Luca Albarello, Flora Poizat, Marnix Jansen, Lígia Castro, Angus McGregor, Gorana Aralica, Branko Dmitrovic, Nevine El Deeb, Fulop Emoke, Caroline Gabignon, Paul Barrett, Norman Carr, Bruno Sinn, Sophie Michalak, Simona Gurzu, Giovanni De Petris, Danny Goudkade, Julia Rees, Isabelle Focke-Snieders, Michael Vieth, Adriana Martinez, Anne Couvelard, Antonella Savio, Desislava Tashkova, Caitlin Beggan, María-Luisa Sánchez-Bernal, Alessandro D’Amuri, Eugeniu Cazacu, Veena Shinde, Valeria Barresi, Kamran Ghaffarzadehgan, Jaroslaw Wejman,Ann Fleming, Maria-Jose Paules, Parag Dabir, Roberto Fiocca, Meleri Morgan, Olivia Cambero, Ioannis Provatas, Antonio Ieni, Ray McMahon, Catherine Julie, Roberto Salgado, Viorica Crisan, Izhar Bagwan, Gonca Ozgun, Bence Kővári, Carine De Prez, Adam Christian, Ana Cunha, Hajnalka Gyorffy, Andreea-Cristina Iogrescu, Marek Grega, Houria Belkralladi, Maria Brito, Leroux Agnès, Renata Chmelova, Florence Renaud, Felix Lasitschka, Nina Zidar, Karthik Kalyanasundaram, Armelle Bardier, Fiebo ten Kate, Jera Jeruc, Catherine lo Polito, Marie-Louise van Velthuysen, Nick West, Mukul Vij, Joost van Gorp, Vincenzo Villanacci, Frederic Bibeau, Ari Ristimäki, Nicholas Mapstone, Yasmine Lahoubi, Issam Abd-Alsmad, Xavier Sanjuan, Miriam Cuatrecasas, Carolina Ibarrola, Cecilia Egoavil Rojas, Eva Sticova, Fred Bosman, Manuela Vivario, Julian Ananiev, Maysa Al-Hussaini, Nathalie Guedj, Ana Dias, Christine Sempoux, Nicole van Grieken, Valentini Tzioufa-Asimakopoulou, Maria Gomez-Galdon, Maria Diodoro, Namor Williams, Kristina Tõnismäe, Calypso Barbatis,Fatima Carneiro, Elvira Gonzalez-Obeso, Gaetan MacGrogan, Isinsu Kuzu, Jens Neumann, Ratnadeep Ganguly, Daniel Val-Garijo, and those who did not submit their names. Technical support: Leonardo Perez-Aranda Alonso, Aida Molero-Bermejo, Vinciane Vincx, Katherine Hartmann, Jennifer Crespo, Francoise Meunier, Jouri Van Den Bergh, Jonathan O’Sullivan, Denis Lacombe, and Raed Al Dieri.
Contributions
Maria Urbanowicz, Heike I Grabsch, and Jean-François Fléjou conceived and designed the study and wrote, edited, and reviewed the manuscript. All authors researched and analyzed data and wrote, edited, and reviewed the manuscript and gave final approval for publication. All authors take full responsibility for the work as a whole, including the study design, access to data, and the decision to submit and publish the manuscript.
Funding
No funding was destined for this publication. Maria Urbanowicz’s work as Fellow at EORTC Headquarters was supported by a grant from the ESP and the EORTC Cancer Research Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Electronic supplementary material
ESM 1
(DOCX 26 kb)
Rights and permissions
About this article

Cite this article
Urbanowicz, M., Grabsch, H.I., Fiteni, F. et al. An international survey-based study on colorectal cancer pathology reporting—guidelines versus local practice. Virchows Arch 473, 697–708 (2018). https://doi.org/10.1007/s00428-018-2457-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00428-018-2457-3