
Abstract
Pulmonary oxygen uptake (\( {\dot{\mathrm{V}}\mathrm{O}}_2 \)) slowly increases during exercise above the anaerobic threshold, and this increase is called the slow component of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \). The mechanism of the increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) is assumed to be due to increasing energy cost associated with increasingly inefficient muscle contraction. We hypothesized that the increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) would be accompanied by a constant or increasing rate of accumulation of blood lactate, indicating sustained anaerobic metabolism while \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) increased. Ten male subjects performed cycle ergometry for 3, 6, and 9 min at a power output representing 60% of the difference between lactate threshold and maximal \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) while \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) and blood lactate accumulation were measured. Blood lactate accumulation decreased over time, providing the energy equivalent of (mean ± SD) 1586 ± 265, 855 ± 287, and 431 ± 392 ml of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) during 0–3, 3–6, and 6–9 min of exercise, respectively. As duration progressed, \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) supplied 86.3 ± 2.0, 93.6 ± 1.9, and 96.8 ± 2.9% of total energy from 0 to 3, 3 to 6, and 6 to 9 min, respectively, while anaerobic contribution decreased. There was no change in total energy cost after 3 min, except that required by ventilatory muscles for the progressive increase in ventilation. The slow component of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) is accompanied by decreasing anaerobic energy contribution beyond 3 min during heavy exercise.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The slow component of oxygen uptake (SC) is a slow increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) when exercise at a constant intensity, above anaerobic threshold but below maximal \( {\dot{\mathrm{V}}\mathrm{O}}_2 \), is continued past 3 min [2, 9]. The SC, also known as phase III of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) kinetics, will either reach a delayed steady state or continue to rise until maximal \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) is reached [15]. The SC is quantified either by curve fitting of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) kinetics with a three-component model [2] or by objectively quantifying any increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) beyond that achieved at 3 min of exercise, by which time the fast phase of the rise in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) (phase II) would be complete and a steady state would have been reached in sub-threshold exercise [2, 9].
One known factor contributing to the slowly rising \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) during supra-threshold exercise is a progressively increasing ventilation. It is accepted that the amount of air breathed each min (\( \dot{\mathrm{V}} \) E) persistently rises during sustained supra-threshold exercise. The increasing energy required by ventilatory muscles has been estimated to account for approximately 18–25% of the oxygen uptake associated with the SC [13, 32]. The remaining SC is known to occur within the exercising muscles [24]. Grassi [11] has recently discussed the relationship between fatigue and the SC, reviewing evidence that the SC develops in association with progressive fatigue. It was concluded that the SC and the corresponding increase in total energy cost were associated with fatigue.
Attempts to measure ATP turnover using magnetic resonance spectrometry during the development of the slow component have produced mixed results. In some cases, ATP turnover is observed to increase [4] and in others to decrease [33] or remain constant [20]. Cannon et al. [4] reported that the increase in ATP turnover was not correlated with the increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) associated with the slow component, making it difficult to acknowledge an increasing energy cost of exercise as the SC develops. It would be of value to find an alternative way to quantify the total energy cost of exercise in this intensity domain.
We define anaerobic threshold as the highest intensity of exercise that can be sustained by oxidative metabolism, without continued lactate accumulation [30]. Below anaerobic threshold, pulmonary oxygen uptake (\( {\dot{\mathrm{V}}\mathrm{O}}_2 \)) rises to a steady state during the first minutes of exercise; blood lactate may be above resting values, but does not accumulate over time [30]. Accumulation of lactate is evidence of continuing contribution of anaerobic metabolism [7], so if aerobic metabolism can supply all of the required ATP, then lactate concentration will not increase. If the SC is associated with fatigue and decreasing efficiency of muscular exercise, then blood lactate, representing anaerobic metabolism, should continue to accumulate at a constant or increasing rate during constant intensity exercise, while the \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) continues to rise.
In this experiment, we tested this hypothesis by measuring lactate accumulation after 3, 6, and 9 min of constant intensity exercise at 60% of the difference between lactate threshold and maximal \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) (60%∆). The accumulation of lactate in the body can be estimated from peak blood lactate following a bout of exercise and subtraction of the pre-exercise blood lactate. This approach has been used extensively for quantification of anaerobic glycolytic contribution to exercise metabolism [3, 8, 28].
Materials and methods
Ten male cyclists (age 29.3 ± 4.2 years, height 178.1 ± 6.7 cm, weight 76.3 ± 8.3 kg) were recruited from local cycling clubs. All cyclists participated in structured training programs and were competitive at a sub-elite level. Written informed consent was obtained prior to participation in the study, which was approved by the University of Calgary Conjoint Health Research Ethics Board.
Testing occurred on four occasions at similar times of day with sequential visits separated by at least 48 h. Subjects abstained from food for 3 h prior to testing, performed no other physical activity on the day of testing, and were asked to arrive at each session similarly rested and well-hydrated. All visits were completed within 2 weeks to avoid a change in fitness during the period of testing. Data were collected in a quiet, temperature-controlled room using a Velotron cycle ergometer (RacerMate Inc., Seattle, WA, USA), which was calibrated prior to each use. Seat height, handlebar position, and pedal type were adjusted according to personal preference and replicated during each testing session for a given subject.
\( {\dot{\mathrm{V}}\mathrm{O}}_2 \) and ventilatory data were collected breath-by-breath using the Cosmed Quark CPET metabolic cart (Cosmed, Rome, Italy). Prior to each test, sensor and turbine calibrations were completed using a gas mixture of 5% CO2, 16% O2, balance N2 (Cosmed, Rome, Italy), and a 3-l syringe (Hans Rudolph, Shawnee, Kansas, USA), respectively. Sensor calibration was verified following each test.
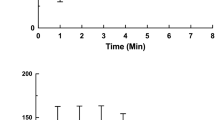
Subjects cycled at a cadence of 85 ± 5 rpm for all tests. A 5-min warm-up at 100 W was completed prior to each exercise bout. At the initial testing session, \( {\dot{\mathrm{V}}\mathrm{O}}_{2 \max } \) and lactate threshold were determined using a two-part incremental protocol. The first part of the incremental test began at a power output of 100–150 W, depending on the perceived fitness of the subject. Power output was increased by 25 W every 3 min with fingertip blood samples obtained at the end of each stage for blood lactate measurement (Lactate Pro, Arkray, Kyoto, Japan). Once a blood lactate concentration of at least 6.0 mM was attained, the first part of the test ended. Lactate threshold was identified as the stage at which the second steep increase in blood lactate concentration occurred, as assessed by three individuals with agreement. This approach is shown in Fig. 1 for a typical subject.

Blood lactate response during an incremental exercise test performed on a cycle ergometer. In this phase of the test, power output was increased by 25 W every 3 min. Lactate threshold was considered to be the second steep increase in blood lactate following a change in power output. In this subject, lactate threshold was considered to occur at 275 W at a blood lactate concentration of 4.0 mM
Following a 10-min rest, during which subjects cycled lightly, a second step incremental test was performed to determine individual maximal \( {\dot{\mathrm{V}}\mathrm{O}}_2 \). Subjects began at the power output that occurred two stages prior to the completion of the first part of the test. Power output was increased by 15 W every minute until exhaustion or the inability to maintain cadence within 5 rpm of the target cadence (85 rpm). Strong verbal encouragement was given. \( {\dot{\mathrm{V}}\mathrm{O}}_{2 \max } \) was measured as the highest 30 s average \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) during this second stage of the test.
On the second, third, and fourth visits, a 3-, 6-, or 9-min ride at a power output equal to 60% of the difference between the subject’s power output at lactate threshold and \( \dot{\mathrm{V}} \)O2max (60%∆) was completed. Two minutes of cycling at 20 W were completed prior to each ride as a direct lead-in. Each subject performed all three cycling durations on separate visits. The 9-min ride was always completed first to ensure that subjects were able to sustain the power output indicated, but the order of the subsequent 3 and 6 min rides was randomized. Pulmonary data were recorded breath-by-breath throughout each ride.
Contribution to energy demand supplied through anaerobic glycolytic pathways was assessed using the quantity of lactate accumulated during the 0–3, 3–6, and 6–9 min time segments of exercise. Lactate at rest was subtracted from peak lactate after 3, 6, or 9 min to determine the accumulation of lactate for each ride. Accumulation from 3 to 6 min was obtained by subtracting accumulation for 0–3 min from the accumulation for the 6-min ride. Accumulation from 6 to 9 min was obtained by subtracting accumulation for 0–6 from that for 0–9 min ride. This calculation is demonstrated in Table 1. The hypothesis was that lactate accumulation, indicative of anaerobic energy contribution, would continue without decreasing over the duration of the 9 min ride. No significant difference in lactate accumulation or a significant increase in sequential 3 min segments would be accepted as satisfying this hypothesis. To obtain an estimate of the energy contribution from anaerobic glycolysis, lactate accumulation was used to estimate an oxygen equivalent using Di Prampero’s suggested equivalent of 3.0 ml kg−1 of oxygen uptake per millimolar lactate accumulation [7, 8].
To assess gross aerobic energetic contributions during 0–3, 3–6, and 6–9 min, breath-by-breath \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) measurements averaged over 10 s were summed to yield total volume of oxygen consumed over each 3 min segment. The SC was considered to be the volume of extra O2 uptake from 3 to 9 min, above the rate that was measured 3 min into exercise [29].
\( {\dot{\mathrm{V}}}_{\mathrm{E}} \) values were also measured breath-by-breath and averaged every 10 s. Work of breathing (WB) and the oxygen cost attributed to the ventilatory muscles (\( {\dot{\mathrm{V}}\mathrm{O}}_2 \) VM) were calculated during each time segment based on \( \dot{\mathrm{V}} \) E measurements according to the following equations [6]
As with \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) data, values in each time segment were summed to yield the total \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) VM for each 3 min time segment.
Total oxygen cost of activity was considered the sum of energy supplied through aerobic oxidative and anaerobic glycolytic pathways, and was expressed as an oxygen equivalent. Because it is already acknowledged that the increasing work performed by ventilatory muscles contributes to the SC, the energy cost of breathing was calculated and subtracted from the total oxygen cost of activity. This provided an “adjusted” oxygen equivalent of the energy demand of activity, which was calculated for 0–3, 3–6, and 6–9 min of the cycling ride. The proportions of energy supplied aerobically and anaerobically during each time segment were then calculated.
Thus, were then calculated as shown in equation 3.
The portions of energy supplied aerobically and adjusted energy costs during each time segment were compared using ANOVA. Post-hoc analysis was performed using Newman-Keuls test. Results are presented as mean ± standard deviation and were considered significant for P < 0.05.
Results
Subjects performed the 60%Δ rides at approximately 88% of the power output achieved at \( {\dot{\mathrm{V}}\mathrm{O}}_{2 \max } \). Fitness characteristics are noted in Table 2. Power output at 60%Δ was 324.6 ± 23.3 W. The mean magnitude of the SC was 8.0 ± 3.5 ml kg−1 O2 at 6 min and 13.6 ± 3.8 ml kg−1 O2 at 9 min. \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) increased an average of 483 ± 215 ml min−1 from 3 to 9 min (Fig. 2).

Mean (± SD) oxygen consumption (black) and oxygen consumption allocated to work of breathing (grey) during 9 min of cycling exercise at 60%Δ. The SC is indicated by the area between the horizontal black line and the data indicated by the black symbols
Given that data were collected on three separate days for each subject, repeatability was paramount in satisfying the assumption that measurements from each testing session represented a typical ride at 60%Δ. At the 3-min time point within the 3, 6, and 9 min cycling trials, the mean \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) was 3875 ± 247, 3915 ± 247, and 3902 ± 254 ml O2 min−1, respectively (50.8 ± 3.7, 51.4 ± 4.0, and 51.2 ± 3.4 ml O2 kg−1 min−1). The average intrasubject difference in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) between the three trials was 113 ± 118 ml O2 min−1 (1.49 ± 1.50 ml O2 kg−1 min−1), which is within the range of reported measurement error for the Cosmed Quark metabolic system [12]. A mean intraclass correlation value of 0.97 for the 3-min time points of every ride indicates high repeatability in data, as does very similar means and standard deviations at the 3-min time point of all cycling trials. As such, it can be assumed that measurements during the 3- and 6-min rides represent intermediate measures during a single 9-min ride. The high reproducibility is illustrated in Fig. 3 for a typical subject.

Oxygen uptake (ml O2 min−1) expressed as 30 s averages for a typical subject cycling for 3, 6, and 9 min at 310 W on separate days. A 2-min lead-in at 20 W preceded the 3, 6, and 9 min trials
Rate of accumulation of lactate was not sustained through the duration of the exercise bout. There was a significant decrease in rate of lactate accumulation during 3 min segments across the rides up to 9 min. The hypothesis was rejected. An analysis of the contributions of aerobic and anaerobic energy provides a detailed novel look at the SC. As exercise progressed, the aerobic contributions to energy demand increased while anaerobic contributions decreased. This is shown in Figs. 4 and 5. In the 0–3, 3–6, and 6–9 min time segments, aerobic metabolism provided 86.3 ± 2.0, 93.6 ± 1.9, and 96.8 ± 2.9% of required energy, respectively, while anaerobic metabolism supplied the remainder. The percent anaerobic contribution to the total energy cost of activity decreased by 53.3% between 0–3 and 3–6 min and by an additional 50.0% between the 3–6 and 6–9 min segments. The proportion of energy supplied aerobically and anaerobically was significantly different between sequential time segments (p < 0.0001), as is shown in Tables 3 and 4.

Mean (±SD) oxygen equivalents of aerobic (dark grey) and anaerobic glycolysis (grey) oxygen cost of activity and the total oxygen cost of activity at 0–3, 3–6, and 6–9 min of cycling exercise at 60%Δ. Oxygen cost of ventilation has been subtracted. There was no significant difference in adjusted oxygen cost between 3–6 and 6–9 min in spite of an increasing \( \dot{\mathrm{V}} \)O2. Anaerobic contribution decreased from 3–6 to 6–9 min. Presumably, the deficiency of oxygen equivalent during the first 3 min was provided by the immediate energy systems (decrease in ATP and creatine phosphate concentrations and the use of oxygen stores), which was not quantified in this study

Oxygen contributions with adjusted and total oxygen cost of exercise over time during 9 min of cycling at 60%∆. Each column represents mean (± standard deviation) oxygen uptake (aerobic contribution) of ten cycling subjects, with the light grey indicating the oxygen uptake estimated specifically for ventilatory muscles. The dark grey columns represent the remainder of measured oxygen consumed which presumably provides energy for exercising muscle. The horizontal line indicates the adjusted oxygen cost of activity over 3 min time segments, calculated as the sum of aerobic and anaerobic glycolytic energy contributions, minus the oxygen cost of ventilation. Thus, the white gap under the horizontal line is indicative of anaerobic contribution. The apparent increase in oxygen equivalent at 3 min is largely due to the lack of consideration for immediate energy sources
\( {\dot{\mathrm{V}}}_{\mathrm{E}} \) increased throughout the duration of exercise; therefore, the energy cost attributable to breathing also increased (Fig. 2). The average \( \dot{\mathrm{V}} \) E after 3, 6, and 9 min was 108.2 ± 14.3, 136.2 ± 22.1, and 158.0 ± 20.1 l min−1, respectively (Fig. 6).

Mean (± standard deviation) ventilation rate of ten subjects during cycling at 60%∆
The average adjusted oxygen cost per minute was 3692 ± 220, 4103 ± 325, and 4073 ± 282 ml O2 min−1. The adjusted oxygen equivalent was significantly different between time segments (p = 0.01). However, post-hoc analysis using the Newman-Keuls test indicated statistical differences only between the 0–3 min and the other two segments; the adjusted oxygen equivalent of activity was unchanged beyond 3 min of exercise. As such, after accounting for the oxygen demand for increasing \( {\dot{\mathrm{V}}}_{\mathrm{E}} \), the increasing \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) representing the SC appears to compensate for the decreasing anaerobic energy contribution.
Discussion
Historically, it has been assumed that as the SC develops, there is a concomitant sustained or continually increasing energy demand to maintain the constant exercise intensity, including increases in both aerobic and anaerobic energy supply. This increase in total energy cost is thought to occur due to decreasing muscle efficiency associated with fatigue, possibly related to recruitment of “less efficient” type II motor units or changes in P/O ratio [11, 15]. Several potential mechanisms for the increased metabolic rate of active muscles have previously been proposed including: increasing type II motor unit recruitment (1), a fatigue-related reduction in efficiency of contraction (15, 19, 34), increasing lactate acidosis (26), and/or increasing core temperature (16). A steadily increasing energy cost would be associated with a constant or increasing rate of lactate accumulation. However, though the measured blood lactate concentration is shown here to increase over time, the rate of lactate accumulation actually decreases, which is consistent with previous observations [19, 20]. Our calculations reveal that the energy deficit created by the decrease in lactate accumulation can be accounted for by the increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) that is the SC, meaning that there is not necessarily a growing inefficiency in the fatiguing muscles. It would appear that the search for a mechanism to explain a rising energy cost of exercise as a mechanism for the SC of oxygen uptake is not necessary.
It has been shown here that \( \dot{\mathrm{V}} \) E can account for the only real increase in energy cost while the SC develops. In this project, the oxygen cost of increasing \( {\dot{\mathrm{V}}}_{\mathrm{E}} \) accounts for 18–21% of the SC, which is consistent with previous research [13, 32]. It has been determined that approximately 80% of the SC originates in the exercising muscles [24], so the oxygen cost of increasing ventilation likely accounts for essentially all of the remaining extra-muscular contribution to the SC.
Our results indicate that the adjusted oxygen cost of exercise, that is, the energy cost of exercise with the estimated energy cost of \( {\dot{\mathrm{V}}}_{\mathrm{E}} \) removed, is essentially unchanging from 3 min to the end of activity. The rising contribution of oxygen uptake during this time is countered by an energetically equivalent decreasing anaerobic contribution. These findings are noteworthy as most previous research on the SC mechanism has been completed with the assumption that extra oxygen uptake is out of necessity to meet rising energy needs. Our observations suggest that the SC has just two underlying mechanisms: (1) the increasing oxygen uptake required by ventilatory muscles due to an increase in \( {\dot{\mathrm{V}}}_{\mathrm{E}} \) and (2) a further increase in \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) while anaerobic contribution continues to decrease.
Several different techniques have been used previously to examine energy cost and rates of aerobic and anaerobic metabolism during a SC. When comparing rates of aerobic and anaerobic ATP production during two consecutive bouts of high intensity knee extension measured using 31P-magnetic resonance spectroscopy and simultaneous pulmonary oxygen uptake, it is noted that total energy cost is not different [20]. However, during the second bout, oxidative energy contribution is greater at exercise onset in conjunction with reduced anaerobic ATP production, and there is no SC [20]. Likewise, Krustrup and colleagues [19] noted an increase in oxygen consumption and decrease in anaerobic energy contribution with unchanging total energy cost during the later stages of heavy intensity cycling. Investigators quantified anaerobic contribution by collecting biopsies of the vastus lateralis prior to and immediately following exercise to measure muscle metabolites [19]. As well, measurements of aerobic and anaerobic energy contributions to intense isometric tetanic contractions in dog muscle also showed no change in ATP turnover in the later parts of the contraction [33]. This constant ATP turnover coincided with an increase in oxidative metabolism and decrease in ATP contributed anaerobically, detected as blood lactate, intracellular lactate, creatine phosphate (PCr), and stored ATP [33].
In our results, the adjusted oxygen cost of activity was approximately 1187 ml O2 lower during the 0–3 min segment than the 3–6 or 6–9 min segments, the latter two of which were not significantly different (Table 4). At exercise onset, immediate energy is provided through phosphocreatine splitting and use of oxygen stores from the blood. These sources of energy do not result in lactate accumulation and would not be represented in oxygen uptake measured at the lungs and therefore were not captured in our calculations. These minor energy sources could readily explain the lower apparent adjusted oxygen equivalent observed between the 0–3 min time segment and the remainder of time as they supply considerable energy only at exercise onset in trained subjects [20]. The contributions of oxygen stores in the blood can be estimated as being approximately 2.3 ml O2 kg−1 [14]. It has been estimated that the oxygen equivalent of energy provided from phosphocreatine breakdown is equal to 37 ml O2 kg−1 active muscle mass [8]. To account for the remaining oxygen cost after oxygen stores have been considered, phosphocreatine in approximately 14 kg of muscle would need to be depleted in a 75-kg subject [14]. Therefore, the total energy cost of sustained supra-threshold exercise at a constant power output may not be changing at any time point beyond that needed for the increasing ventilation.
Though our findings establish that a shift in metabolic system utilization is a major determinant of the SC of oxygen uptake, the precise reason for this slow shift remains unknown. During the initial min of exercise, oxygen uptake increases exponentially. This is referred to as phase II of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) kinetics. During this phase, the difference between ATP supply by aerobic metabolism and total ATP requirement is provided by anaerobic metabolism. When exercise energy demand is below anaerobic threshold, the \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) increases until a steady state is attained where ATP is provided exclusively through aerobic metabolism. When the intensity of exercise exceeds anaerobic threshold, anaerobic energy contributions continue past the 1–3 min typically needed for \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) to reach a steady state [9, 30]. With the exception of one case recently published by Korzeniewski and Zoladz [17], it has not previously been considered that the rate of ATP replenishment by anaerobic metabolism might actually continue to decrease after the time when a steady state for \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) should be achieved. There may be an advantage to minimizing energy provided by anaerobic glycolysis during continued exercise in the heavy exercise domain. It is thought that we have a finite capacity of the anaerobic system [23], so decreasing the rate at which this energy source is used should prolong the duration that the exercise can be tolerated. However, there must be a cellular control mechanism responsible for this continued slow transition to aerobic metabolism.
Aerobic metabolism occurs in the mitochondrial matrix, and is stimulated by ADP transported from the cytosol [31]. The development of the SC has been found to show parallel kinetics to a small decrease in intramuscular PCr concentration during exercise [25]. An increase in creatine concentration following PCr hydrolysis would increase mitochondrial creatine kinase activity [22] and lead to an increase in mitochondrial ADP concentration, which is known to drive aerobic metabolism [22]. Exercise training improves mitochondrial ADP sensitivity, as does prior exercise [21, 31]. There is a reduced SC with increased fitness [32] or prior heavy exercise [27]. The reduced SC relates to a larger change in \( \dot{\mathrm{V}} \)O2 with no change in time constant for phase II kinetics of oxygen uptake resulting in a smaller oxygen deficit [32]. Our results suggest that the reduced SC would relate to the smaller initial anaerobic contribution and the resulting smaller decrease in anaerobic contribution during phase III of the oxygen uptake kinetics. Further research is needed to confirm this suggestion.
In addition to prior heavy exercise, the SC amplitude is also reduced when type II motor units are glycogen-depleted through repeated sprint exercise [5]. The smaller SC may be caused by a faster aerobic compensation required by a compromised anaerobic energy system from glycogen depleted type II fibres, leading to a greater \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) amplitude during the fast component of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) (phase II) and therefore a reduced SC.
The idea of a shift in metabolic energy systems leading to the SC was recently proposed using computer modelling. Korzeniewski and Zoladz [17] modelled the SC with an inhibition of glycolysis, presumably due to increasing acidosis. It is generally accepted that acidosis inhibits two rate-limiting enzymes of anaerobic glycolysis: glycogen phosphorylase and phosphofructokinase. A reduction in anaerobic glycolysis would then necessitate an increase in aerobic metabolism to meet the energy demand. While our results are consistent with the output of this model, we do not feel that an increase in proton concentrations is responsible for this shift. Hydrogen ions have not been shown to cause feedback inhibition of glycolysis in vivo [18]. Furthermore, increasing aerobic metabolism in the face of inhibition of these key enzymes of glycolysis would require a change in substrate to oxidation of more fat. There is no evidence that the SC corresponds with increased fat metabolism, which is known to be minimal during exercise at this high intensity. Alternately, we suggest that the SC is more likely due to a reduction in anaerobic contribution spurred by an increase in mitochondrial ADP concentration, regulating aerobic metabolism.
There is some debate within the literature as to the most appropriate method of estimating anaerobic energy contribution during exercise. Most commonly, blood lactate accumulated during exercise is used to estimate an oxygen equivalent using a conversion factor of 3.0 ml O2 kg−1 mmol−1 of lactate accumulated as classically derived by Di Prampero [7, 8]. However, conversion factors as high as 5.2 ml O2 kg−1 mmol−1 lactate accumulated have been suggested [10]. Using this higher equivalent to calculate the anaerobic contribution, we estimated that glycolysis leading to lactate formation could account for 21.5 ± 2.8, 10.6 ± 3.0, and 5.3 ± 4.6% of energy supply from 0 to 3, 3 to 6, and 6 to 9 min, respectively. Although this is greater than that calculated using di Prampero’s equivalent, it remains clear that the rate of lactate accumulation is decreasing over sequential time segments, indicating a decreasing anaerobic contribution regardless of conversion factor.
Previous observations of a dissociation between the \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) SC and ATP turnover have been reported by Cannon and colleagues [4]. These authors found that ATP turnover and \( \dot{\mathrm{V}} \)O2 both increased similarly during heavy constant work rate exercise; however, there was no relationship amongst individuals between these two variables [4]. This dissociation provides further evidence that the SC is not caused by an increasing energy demand. Authors then attributed the cause of the SC to decreases in mitochondrial efficiency [4]. Our data provide an alternative interpretation. The decrease in anaerobic glycolytic ATP production requires increased aerobic ATP production, even with constant ATP turnover. The concept that total energy cost may not be increasing during high intensity exercise is not a new idea [4, 19, 20]. In further support of a lack of change in efficiency, a decrease in mitochondrial efficiency would not be expected to be associated with decreased rate of lactate accumulation.
It should be noted that subjects in the present study were trained athletes. This group of individuals were chosen due to familiarity to both cycling and the task of performing taxing exercise. As such, findings cannot be generalized to all populations.
Conclusion
In conclusion, we have shown that there is no change in oxygen cost of a constant power cycling ride at 60%∆ after 3 min, other than the additional oxygen uptake required to support the increase in \( \dot{V} \) E. As well, we have shown that the rate of lactate accumulation during the ride, and therefore the proportion of energy supplied anaerobically, decreases over the duration of exercise while that which is supplied aerobically increases to compensate. This is the first time that a shift in energy systems has been demonstrated as a major contributor to the SC, providing insight into this fundamental feature of human physiology.
References
Barstow TJ, Jones AM, Nguyen PH, Casaburi R (1996) Influence of muscle fiber type and pedal frequency on oxygen uptake kinetics of heavy exercise. J Appl Physiol 81:1642–1650
Bell C, Paterson DH, Kowalchuk JM, Padilla J, Cunningham DA (2001) A comparison of modelling techniques used to characterize oxygen uptake kinetics during the on-transient of exercise. Exp Physiol 86:667–676. doi:10.1113/eph 8602150
Bertuzzi R, Nascimento EM, Urso RP, Damasceno M, Lima-Silva AE (2013) Energy system contributions during incremental exercise test. J Sports Sci Med 12(3):454–460
Cannon DT, Bimson WE, Hampson SA, Bowen TS, Murgatroyd SR, Marwood S, Kemp GJ, Rossiter HB (2014) Skeletal muscle ATP turnover by 31P magnetic resonance spectroscopy during moderate and heavy bilateral knee extension. J Physiol 592:5287–5300. doi:10.1113/jphysiol.2014.279174
Carter H, Pringle JS, Boobis L, Jones AM, Doust JH (2004) Muscle glycogen depletion alters oxygen uptake kinetics during heavy exercise. Med Sci Sports Exerc 36:965–972. doi:10.1249/01.MSS.0000128202.73676.11
Coast JR, Krause KM (1993) Relationship of oxygen consumption and cardiac output to work of breathing. Med Sci Sports Exerc 25:335–340. doi:10.1249/00005768-199303000-00007
Di Prampero PE (1981) Energetics of muscular exercise. Rev Physiol Biochem and Pharm 89:143–222
Di Prampero PE, Ferretti G (1999) The energetics of anaerobic muscle metabolism: a reappraisal of older and recent concepts. Resp Physiol 118:103–115. doi:10.1016/S0034-5687(99)00083-3
Gaesser GA, Poole DC (1996) The slow component of oxygen uptake in humans. Exerc Sport Sci Rev 24:35–70. doi:10.1249/00003677-199600240-00004
Gladden LB, Welch HG (1978) Efficiency of anaerobic work. J Appl Physiol 44:564–570
Grassi B, Rossiter HB, Zoladz JA (2015) Skeletal muscle fatigue and decreased efficiency: two sides of the same coin? Exerc Sport Sci Rev 43:75–83. doi:10.1249/JES.0000000000000043
Gullstrand L, Lindberg T, Alonso J (2013) Validity of the COSMED Quark CPET respiratory gas analyzer with breath by breath analysis system. [independent validation study]. http://www.cosmed.com/en/science/validation-papers
Hagberg JM, Mullin JP, Nagle FJ (1978) Oxygen consumption during constant-load exercise. J Appl Physiol 45:381–384
Hill D (1999) Energy system contributions in middle-distance running events. J Sports Sci 17:477–483. doi:10.1080/026404199365786
Jones AM, Grassi B, Christensen PM, Krustrup P, Bangsbo J, Poole DC (2011) SC of oxygen uptake kinetics: mechanistic bases and practical applications. Med Sci Sport Exerc 43:2046–2062. doi:10.1249/MSS.0b013e31821fcfc1
Koga S, Shiojiri T, Kondo N, Barstow TJ (1997) Effect of increased muscle temperature on oxygen uptake kinetics during exercise. J Appl Physiol 83:1333–1338
Korzeniewski B, Zoladz JA (2015) Possible mechanisms underlying slow component of \( {\dot{\mathrm{V}}\mathrm{O}}_2 \) on-kinetics in skeletal muscle. J Appl Physiol 118:1240–1249. doi:10.1152/japplphysiol.00027.2015
Krause U, Wegener G (1996) Control of glycolysis in vertebrate skeletal muscle during exercise. Am J Phys 270:821–829
Krustrup P, Söderlund K, Mohr M, Bangsbo J (2004) The slow component of oxygen uptake during intense, sub-maximal exercise in man is associated with additional fibre recruitment. Pflugers Arch 447:855–866. doi:10.1007/s00424-003-1203-z
Layec G, Bringard A, Yashiro K, Le Fur Y, Vilmen C, Micallef JP, Perry S, Cozzone P, Bendahan D (2012) The SCs of phosphocreatine and pulmonary oxygen uptake can be dissociated during heavy exercise according to training status. Exp Physiol 97:955–969. doi:10.1113/expphysiol. 2011.062927
Ludzki A, Paglialunga S, Smith B, Herbst E, Allison A, Heigenhauser G, Holloway G (2015) Rapid repression of ADP transport by palmitoyl-CoA is attenuated by exercise training in humans. FASEB J 29:824–816. doi:10.2337/db14-1838
Meyer RA (1988) A linear model of muscle respiration explains monoexponential phosphocreatine changes. Am J Phys 254:C548–C553
Monod H, Scherrer J (1965) The work capacity of a synergic muscular group. Ergonomics 8:329–338. doi:10.1080/00140136508930810
Poole DC (1994) Role of exercising muscle in SC of VO2. Med Sci Sports Exerc 26:1335–1340. doi:10.1249/00005768-199411000-00007
Rossiter HB, Ward SA, Kowalchuk JM, Howe FA, Griffiths JR, Whipp BJ (2002) Dynamic asymmetry of phosphocreatine concentration and O2 uptake between the on-and off-transients of moderate-and high-intensity exercise in humans. J Physiol 541:991–1002. doi:10.1113/jphysiol.2001.012910
Roston WL, Whipp BJ, Davis JA, Cunningham DA, Effros RM, Wasserman K (1987) Oxygen uptake kinetics and lactate concentration during exercise in humans. Am Rev Respir Dis 135:1080–1084. doi:10.1164/arrd.1987.135.5.1080
Sahlin K, Sørensen JB, Gladden LB, Rossiter HB, Pedersen PK (2005) Prior heavy exercise eliminates SC and reduces efficiency during submaximal exercise in humans. J Physiol 564:765–773. doi:10.1113/jphysiol. 2005.083840
Sandbakk Ø, Holmberg HC, Leirdal S, Ettema G (2010) Metabolic rate and gross efficiency at high work rates in world class and national level sprint skiers. Eur J Appl Physiol 109:473–481. doi:10.1007/s00421-010-1372-3
Santana MG, Tufik S, Passos GS, Santee DM, Denadai BS, Mello MT (2007) Comparison between different methods of analysis of slow component of oxygen uptake: a view in severe exercise domain. Rev Bras Med Esporte 13:241–244
Svedahl K, Mac Intosh BR (2003) Anaerobic threshold: the concept and methods of measurement. Can J Appl Physiol 28:299–323. doi:10.1139/h03-023
Tonkonogi M, Harris B, Sahlin K (1998) Mitochondrial oxidative function in human saponin-skinned muscle fibres: effects of prolonged exercise. J Physiol 510:279–286. doi:10.1111/j.1469-7793. 1998.279bz.x
Womack CJ, Davis SE, Blumer JL, Barrett EA, Weltman AL, Gaesser GA (1995) SC of O2 uptake during heavy exercise: adaptation to endurance training. J Appl Physiol 79:838–845
Wüst RC, Grassi B, Hogan MC, Howlett RA, Gladden LB, Rossiter HB (2011) Kinetic control of oxygen consumption during contractions in self-perfused skeletal muscle. J Physiol 589:3995–4009. doi:10.1113/jphysiol. 2010.203422
Zoladz JA, Gladden LB, Hogan MC, Nieckarz Z, Grassi B (2008) Progressive recruitment of muscle fibers is not necessary for the slow component of VO2 kinetics. J Appl Physiol 105:575–580. doi:10.1152/japplphysiol.01129.2007
Acknowledgements
We would like to give many thanks to Felipe Maturana, Rafael Fortuna, John Temesi, and Jared Fletcher for their assistance in data collection and processing. Funding was generously provided by NSERC and the Sport Science Association of Alberta.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by the University of Calgary Conjoint Health Research Ethics Board.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
Written informed consent was obtained from all individual participants included in the study.
Additional information
This article is part of the Topical Collection on the Integrative Physiology
Rights and permissions
About this article

Cite this article
O’Connell, J., Weir, J. & MacIntosh, B. Blood lactate accumulation decreases during the slow component of oxygen uptake without a decrease in muscular efficiency. Pflugers Arch - Eur J Physiol 469, 1257–1265 (2017). https://doi.org/10.1007/s00424-017-1986-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00424-017-1986-y