
Abstract
Background
Contemporary nationwide outcomes of gallstone pancreatitis (GSP) managed by cholecystectomy at the index hospitalization are limited. This study aims to define the rate of 30-day morbidity and mortality and identify associated perioperative risk factors in patients undergoing cholecystectomy for GSP.
Methods
Patients from the ACS-NSQIP database with GSP without pancreatic necrosis, who underwent cholecystectomy during the index hospitalization from 2017 to 2019 were selected. Factors associated with 30-day morbidity and mortality were analyzed.
Results
Of the 4021 patients identified, 1375 (34.5%) were male, 2891 (71.9%) were White, 3923 (97.6%) underwent laparoscopic surgery, and 52.4 years (SD ± 18.9) was the mean age. There were 155 (3.8%) patients who developed morbidity and 15 (0.37%) who died within 30 days of surgery. In bivariate regression analysis, both 30-day morbidity and mortality were associated with older age, elevated pre-operative BUN, hypertension, chronic obstructive pulmonary disease, congestive heart failure, acute kidney injury, and dyspnea. ASA of I or II and laparoscopic surgery were protective against 30-day morbidity and mortality. In multivariable regression analysis, factors independently associated with increased 30-day morbidity included preoperative SIRS/sepsis [OR: 1.68 (95% CI: 1.01–2.79), p = 0.048], and age [OR: 1.03 (95% CI: 1.01–1.04), p = 0.001]. Factors associated with increased 30-day mortality included tobacco use [OR: 8.62 (95% CI: 2.11–35.19), p = 0.003] and age [OR: 1.10 (95% CI: 1.04–1.17), p = 0.002].
Conclusions
Patients with GSP without pancreatic necrosis can undergo cholecystectomy during the index admission with very low risk of 30-day morbidity or mortality.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acute pancreatitis is a leading cause for gastrointestinal-related hospital admissions in the USA, and gallstone disease is the most common etiology of acute pancreatitis [1]. Cholecystectomy remains the definitive treatment for gallstone pancreatitis (GSP); however, the recommended timing of surgery has evolved [2]. The most recent evidence supports cholecystectomy during the index hospitalization for mild GSP [3,4,5]. Performing cholecystectomy prior to discharge decreases the risk of patients returning with progressive or recurrent symptoms, which can lead to significant morbidity [6,7,8]. In fact, delayed cholecystectomy has been associated with a 31–53% risk of recurrent biliary events including pancreatitis [5, 9].
Despite the prevalence of GSP, there are few studies analyzing national data on the morbidity and mortality of cholecystectomy at index hospitalization. Given the increasing use of cholecystectomy during the index hospitalization, it is important to understand the predictors of poor surgical outcomes in order to guide risk stratification and patient selection. Therefore, this study aims to define the rate of 30-day morbidity and mortality as well as identify associated perioperative risk factors in patients undergoing cholecystectomy for GSP at the index hospitalization.
Methods
Data source and patient selection
The American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database provides 30-day risk-adjusted surgical outcomes using peer-controlled, validated perioperative clinical data. The database from 2019 included 719 hospitals nationwide that participate on a voluntary basis. The NSQIP database from years 2017 to 2019 was queried for patients who underwent either laparoscopic or open cholecystectomy (CPT codes 47,600, 47,605, 47,610, and 47,562–4) for gallstone pancreatitis during their index hospitalization. Only patients with the diagnosis of gallstone pancreatitis without pancreatic necrosis were included based on the International Classification of Diseases, 10th revision (ICD-10) code K85.10, as patients with necrosis are typically subject to a different management algorithm that includes delayed cholecystectomy. Patients were included if their surgery was performed on an inpatient, non-elective basis. This study was approved by the Institutional Review Board of Lundquist Institute at Harbor-UCLA Medical Center and determined to meet the criteria for non-human subject research.
Variables
Patient demographics, comorbidities, and risk factors were collected. Comorbidities assessed were diabetes mellitus, hypertension requiring medications, congestive heart failure (CHF), renal failure, dialysis dependence, ascites, metastatic cancer, and chronic obstructive pulmonary disease (COPD). NSQIP-defined risk factors included smoking history, chronic steroid use, and recent weight loss. Additional preoperative variables included white blood cell count (WBC), blood urea nitrogen (BUN) level, dyspnea, ascites, acute kidney injury (AKI), preoperative ventilator use, preoperative systemic inflammatory response syndrome (SIRS)/sepsis, preoperative blood transfusion, and American Society of Anesthesiologists (ASA) class. The SIRS/sepsis variable spans patients with relatively mild physiologic abnormalities to septic shock. The primary outcome measures were 30-day mortality and 30-day morbidity. The variables in this study’s composite morbidity variable included any of the following post-operative complications: pneumonia, unplanned intubation, ventilator use greater than 48 h, pulmonary embolism (PE), deep venous thrombosis (DVT), urinary tract infection (UTI), renal insufficiency or failure, superficial, deep or organ space surgical site infection, wound dehiscence, cardiac arrest, myocardial infarction, stroke, or post-operative SIRS/sepsis.
Analysis
Bivariate and multivariate logistic regression analyses were performed to assess whether demographics, comorbidities, and markers of preoperative end-organ dysfunction were associated with 30-day morbidity and mortality. A 2-sided p < 0.05 was considered statistically significant. Any variable with p < 0.10 in initial bivariate analysis was included in a multivariate regression analysis. The Student’s t-test was used to compare continuous data, and Pearson χ2 and Fisher’s exact tests were used to compare categorical data as appropriate. SPSS V24 (IBM Corp, Armonk, New York) was used to perform statistical analysis.
Results
A total of 4021 patients with gallstone pancreatitis without necrosis underwent cholecystectomy. Of those, 1375 (34.5%) were male, 2891 (71.9%) were White, 558 (22.4%) were Hispanic, and 3923 (97.6%) underwent laparoscopic surgery. The mean age was 52.4 ± 18.9 years. There were 37 (0.9%) patients who returned to the operating room. A total of 155 (3.8%) patients developed morbidity and 15 (0.37%) died within 30 days of surgery.
In bivariate regression analysis, 30-day morbidity was associated with older age (63.6 ± 17.3 vs. 51.9 ± 18.9, p < 0.001), male sex (47.1% vs. 33.7%, p = 0.001), BUN (16.5 ± 16.3 vs. 10.2 ± 7.7, p < 0.001), higher WBC (10.3 ± 4.5 vs, 8.8 ± 3.8, < 0.001), and the following comorbid conditions: hypertension (55.5% vs. 38.9%, p < 0.001), COPD (11.6% vs. 2.7%, p < 0.001), CHF (3.9% vs. 1.1%, P = 0.012), AKI (4.5% vs. 0.3%, p < 0.001), dyspnea (7.1% vs 2.8%, p = 0.006), steroid use (5.2% vs. 2.0%, p = 0.018), and preoperative SIRS/sepsis (34.8% vs. 19.3%, p < 0.001). Factors protective against 30-day morbidity were Hispanic ethnicity (9.0% vs. 14.1%, p = 0.032), ASA class I or II (29.7% vs. 56.5%, p < 0.001), laparoscopic surgery (84.5% vs. 98.1%, p < 0.001), and cholecystectomy performed within 3 days of admission (40.0% vs. 48.2%, p = 0.044) (Table 1).
Patients who had higher 30-day mortality were older (75.5 ± 13.2 vs. 52.3 ± 18.9, p < 0.001), had higher rates of current tobacco use (33.3% vs. 13.9%, p = 0.047), and had higher pre-operative BUN (28.1 ± 22.2 vs. 10.4 ± 8.1, p < 0.001). Additionally, they had higher rates of diabetes (40.0% vs. 15.0%, p = 0.017), hypertension (73.3% vs. 39.4%, p = 0.007), COPD (20.0% vs. 3.0%, p = 0.009), CHF (13.3% vs. 1.2%, p = 0.014), dialysis use (13.3% vs. 0.9%, p = 0.008), AKI (13.3% vs. 0.4%, p = 0.002), dyspnea (20.0% vs. 2.9%, p = 0.009), bleeding disorders (26.7% vs. 5.6%, p = 0.009), and lower BMI (29.4 ± 4.7 vs. 32.5. ± 8.2, p = 0.025). ASA class I or II (55.7% vs. 0%, p < 0.001) and laparoscopic surgery (97.6% vs. 80.0%, p = 0.005) were associated with lower 30-day mortality (Table 1).
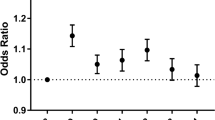
In multivariable regression analysis, factors independently associated with higher 30-day morbidity included pre-operative SIRS/sepsis [OR: 1.68 (95% CI: 1.01–2.79), p = 0.048], and age [OR: 1.03 (95% CI: 1.01–1.04), p = 0.001], whereas laparoscopic surgery [OR: 0.10 (95% CI: 0.055–0.20), p < 0.001] was associated with lower morbidity. Factors associated with higher 30-day mortality included tobacco use [OR: 8.62 (95%CI: 2.11–35.19), p = 0.003] and age [OR: 1.10 (95% CI: 1.04–1.17), p = 0.002], whereas laparoscopic surgery was similarly associated with lower mortality [OR: 0.13 (95% CI: 0.031–0.57), p = 0.007] (Table 2).
Discussion
In this large national study of patients with gallstone pancreatitis without pancreatic necrosis who underwent cholecystectomy during the index admission, 30-day morbidity and mortality were notably low at 3.8% and 0.37%, respectively. The exclusion of patients with pancreatic necrosis in this cohort could contribute to the low overall morbidity and mortality, as severe gallstone pancreatitis, though less common, has an associated mortality risk up to 19% [10]. Our findings are consistent with prior studies demonstrating that patients with mild gallstone pancreatitis who undergo cholecystectomy have a relatively low risk for mortality if they undergo surgery at the index hospitalization.
The findings of our study demonstrating low short-term morbidity and mortality rates using recent nationwide data are consistent with literature that supports early cholecystectomy for gallstone pancreatitis [4,5,6,7]. In the PONCHO trial, a large multicentered randomized prospective study of mild gallstone pancreatitis, same-admission cholecystectomy reduced perioperative morbidity specifically readmissions for recurrent gallstone disease [3]. In a smaller prospective study, mild gallstone pancreatitis patients who underwent early cholecystectomy (within 48 h after admission) did not have increased risk for perioperative complications compared to patients who had cholecystectomy performed later in their hospitalization [7]. Jee et al. performed a randomized prospective trial that found an 8% post-operative complication rate after early laparoscopic cholecystectomy. However, over 80% of these complications were mild surgical site infections, and there were no mortalities [5]. Using a large national database, we confirm that morbidity and mortality are indeed rare events among patients with biliary pancreatitis. Therefore, cholecystectomy during the index hospitalization appears safe, and may be even safer with a laparoscopic approach.
Although a number of factors associated with increased risk for morbidity and mortality in acute pancreatitis have been implicated [11, 12], specific risk factors for post-operative complications following cholecystectomy among patients with gallstone pancreatitis have not been clearly identified. In the present study, we identify an association between preoperative SIRS/sepsis and short-term postoperative morbidity. Overall, 19.8% of the total patients in our study had preoperative SIRS/sepsis. Of note, SIRS and sepsis were categorized under one variable, which the two could not be differentiated in this study. However, sepsis in association with gallstone pancreatitis should raise suspicion for concomitant cholangitis or cholecystitis. While concomitant cholangitis is uncommon, with rates reported as low as 3% [13], and concomitant cholecystitis seen in up to 46% of patients with biliary pancreatitis [14], these patients should be managed appropriately with antibiotics, and for cholangitis, with urgent endoscopic retrograde cholangiopancreatography, prior to surgical intervention. Older age was also found to be a key risk factor for postoperative 30-day morbidity and mortality. Older patients undergoing cholecystectomy have been found to have higher rates of complications and increased hospital length of stay compared to younger patients [15]. Specifically, an age of 75 years or greater has been a reported risk factor for significantly worse outcomes in pancreatitis [16], and age is often included in risk stratification tools [17]. Thus, the findings of older age increasing risk of 30-day morbidity and mortality after cholecystectomy for gallstone pancreatitis are consistent with current evidence.
Additionally, smoking tobacco was identified as an independent risk factor for 30-day mortality following cholecystectomy for gallstone pancreatitis, a novel finding that has not been identified. Smoking within 1 year of any major surgery is associated with risk for post-operative vascular and respiratory events as well as for 30-day mortality [18]. Selvarajah et al. reported that active smokers who undergo cholecystectomy for benign gallbladder disease are at significantly greater risk of developing wound complications and longer hospital stays [19]. Smoking is known to cause more severe pancreatitis, likely due to the effect of nicotine, which disrupts signal transduction pathways in pancreatic acinar cells, and ultimately impairs pancreatic blood flow [20]. Future studies are needed to validate the association between smoking and mortality.
This study was limited by the use of a large retrospective database and thus constrained by the variables available through the database. Specifically, details such as the underlying causes of pre-operative sepsis, causes of death, and complications specific to cholecystectomies were not available. Diagnoses used in this study could not be validated nor was there information on how certain diagnoses were made. Additionally, clinical prognostic scores using published tools for pancreatitis severity could not be calculated given missing data. NSQIP data is populated voluntarily by participating institutions, and therefore may not be generalizable to all hospital settings and patient populations. Further research comparing these findings with cohorts managed non-operatively or with interval surgery is warranted to validate the findings of this present study and to determine whether there are other factors that may justify initial non-operative management of non-necrotic gallstone pancreatitis.
Conclusion
In gallstone pancreatitis without necrosis, patients can undergo cholecystectomy during the index admission with very low risk of 30-day morbidity or mortality. Older age, smoking status, and presence of pre-operative SIRS/sepsis should be considered when weighing the risk and benefits of initial surgery versus non-surgical management strategies.
Data Availability
The data that support the findings of this study are available from the corresponding author, Ashkan Moazzez, upon reasonable request.
Change history
16 February 2023
A Correction to this paper has been published: https://doi.org/10.1007/s00423-023-02824-5
References
Yadav D, Lowenfels AB (2013) The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 144(6):1252–1261. https://doi.org/10.1053/J.GASTRO.2013.01.068
Cucher D, Kulvatunyou N, Green DJ, Jie T, Ong ES (2014) Gallstone pancreatitis: a review. Surg Clin N Am 94(2):257–280. https://doi.org/10.1016/J.SUC.2014.01.006
da Costa DW, Bouwense SA, Schepers NJ et al (2015) Same-admission versus interval cholecystectomy for mild gallstone pancreatitis (PONCHO): a multicentre randomised controlled trial. Lancet 386(10000):1261–1268. https://doi.org/10.1016/S0140-6736(15)00274-3
Dubina ED, de Virgilio C, Simms ER et al (2018) Association of early vs delayed cholecystectomy for mild gallstone pancreatitis with perioperative outcomes. JAMA Surg 153(11):1057–1059. https://doi.org/10.1001/JAMASURG.2018.2614
Jee SL, Jarmin R, Lim KF, Raman K (2018) Outcomes of early versus delayed cholecystectomy in patients with mild to moderate acute biliary pancreatitis: a randomized prospective study. Asian J Surg 41(1):47–54. https://doi.org/10.1016/J.ASJSUR.2016.07.010
Gurusamy KS, Nagendran M, Davidson BR (2013) Early versus delayed laparoscopic cholecystectomy for acute gallstone pancreatitis. Cochrane Database Syst Rev (9):CD010326. https://doi.org/10.1002/14651858.CD010326.pub2
Aboulian A, Chan T, Yaghoubian A et al (2010) Early cholecystectomy safely decreases hospital stay in patients with mild gallstone pancreatitis: a randomized prospective study. Ann Surg 251(4):615–619. https://doi.org/10.1097/SLA.0B013E3181C38F1F
Mueck KM, Wei S, Pedroza C et al (2019) Gallstone pancreatitis: admission versus normal cholecystectomy-a randomized trial (Gallstone PANC Trial). Ann Surg 270(3):519–527. https://doi.org/10.1097/SLA.0000000000003424
Ito K, Ito H, Whang EE (2008) Timing of cholecystectomy for biliary pancreatitis: do the data support current guidelines? J Gastrointest Surg 12(12):2164–2170. https://doi.org/10.1007/S11605-008-0603-Y/TABLES/6
Gullo L, Migliori M, Oláh A et al (2002) Acute pancreatitis in five European countries: etiology and mortality. Pancreas 24(3):223–227. https://doi.org/10.1097/00006676-200204000-00003
Ranson JH, Rifkind KM, Roses DF et al (1974) Objective early identification of severe acute pancreatitis. Am J Gastroenterol 61(6):443–451
Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA (2008) The early prediction of mortality in acute pancreatitis: a large population-based study. Gut 57(12):1698–1703. https://doi.org/10.1136/GUT.2008.152702
Chang L, Lo SK, Stabile BE et al (1998) Gallstone pancreatitis: a prospective study on the incidence of cholangitis and clinical predictors of retained common bile duct stones. Am J Gastroenterol 93(4):527–531. https://doi.org/10.1111/J.1572-0241.1998.159_B.X
Demir U, Yazici P, Bostanci Ö et al (2014) Timing of cholecystectomy in biliary pancreatitis treatment. Ulusal Cerrahi Dergisi 30(1):10–13. https://doi.org/10.5152/UCD.2014.2401
Vaccari S, Lauro A, Cervellera M et al (2019) Cholecystectomy for acute cholecystitis in octogenarians: impact of advanced age on postoperative outcome. Minerva Chir 74(4):289–296. https://doi.org/10.23736/S0026-4733.19.07891-X
Frey CF, Zhou H, Harvey DJ, White RH (2006) The incidence and case-fatality rates of acute biliary, alcoholic, and idiopathic pancreatitis in California, 1994–2001. Pancreas 33(4):336–344. https://doi.org/10.1097/01.mpa.0000236727.16370.99
Żorniak M, Beyer G, Mayerle J (2019) Risk stratification and early conservative treatment of acute pancreatitis. Visc Med 35(2):82–89. https://doi.org/10.1159/000497290
Musallam KM, Rosendaal FR, Zaatari G et al (2013) Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg 148(8):755–762. https://doi.org/10.1001/jamasurg.2013.2360
Selvarajah S, Ahmed AA, Schneider EB et al (2014) Cholecystectomy and wound complications: smoking worsens risk. J Surg Res 192(1):41–49. https://doi.org/10.1016/J.JSS.2014.06.014
Ye X, Lu G, Huai J, Ding J (2015) Impact of smoking on the risk of pancreatitis: a systematic review and meta-analysis. PLoS ONE 10(4):e0124075. https://doi.org/10.1371/JOURNAL.PONE.0124075
Acknowledgements
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not been verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Ashkan Moazzez, Jessica K. Liu, and Caitlyn Braschi. The first draft of the manuscript was written by Jessica K. Liu and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, J.K., Braschi, C., de Virgilio, C. et al. Predictors of poor outcomes after cholecystectomy in gallstone pancreatitis: NSQIP analysis of 30-day morbidity and mortality. Langenbecks Arch Surg 408, 5 (2023). https://doi.org/10.1007/s00423-022-02731-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00423-022-02731-1