
Abstract
Purpose
To verify the influence of different volumes and intensities of aerobic exercise on cardiac autonomic function (CAF) through heart rate variability (HRV) analysis as well the influence of β2 adrenergic receptor (ADRB2) variants in overweight/obese individuals.
Methods
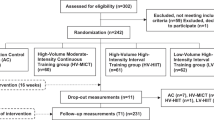
70 physically inactive adults were randomly allocated into the following 16-week training: 1-high-intensity interval training (HIIT) (n = 25, 1 × 4 min bout at 85–95%HR peak, 3×/week), 4-HIIT (n = 26, 4 × 4 min bouts at 85–95%HR peak, interspersed with 3 min of recovery at 50–70%HR peak, 3×/week), and moderate continuous training (MCT) (n = 19, 30 min at 60–70%HR peak, 5×/week). Before and after the exercise training, anthropometric, BP, cardiorespiratory fitness, and HRV measures were evaluated. R–R intervals recorded for 10 min in a supine position at pre- and post-intervention were used to analyze HRV in the plot-Poincare indexes (SD1, SD2), and frequency-domain (LF, HF, LF/HF). Full blood samples were used for genotyping.
Results
4-HIIT and MCT showed positive outcomes for almost all variables while 1-HIIT had a positive influence only on SBP and SD2 index. No associations were observed between isolated ADRB2 variants and changes in HRV. In the analysis of the interaction genotypes, all groups responded positively for the SD1 index of HRV and only the H1 (GG and CC) and H2 (GG and CG + GG) groups presented increases in the RMSSD index. Furthermore, there was an increase in the LF index only in the H3 (CC and AA + AG) and H4 (AA + AG and CG + GG) groups.
Conclusions
ADRB2 variants and aerobic exercise training are important interacting variables to improve autonomic function and other health variables outcomes in overweight or obese individuals.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Cardiovascular disease is a major public health problem and a worldwide leading cause of mortality and morbidity (Ramos et al. 2017). Impaired cardiac autonomic function (CAF), characterized by an imbalance between sympathetic and parasympathetic nervous activity, is considered an important marker of cardiovascular health (Ramos et al. 2017; Matsunaga et al. 2007). Analysis of the heart rate variability (HRV) is used as an index to measure CAF. Increased HRV reflects the ability of the autonomic nervous system and sinoatrial node to dynamically respond to environmental changes, generally indicating a healthy heart, whereas reduced HRV has been associated with poorer cardiovascular health (Kerr et al. 2017).
The genetic variability may be a potentially relevant contributor to CAF. Experimental studies with healthy individuals have demonstrated that adrenergic receptors mediate an important role in modulating vascular tonus (Dessy et al. 2004). A common variant of the β2 adrenergic receptor (ADRB2) occurs at codon16, where the adenine nucleotide is substituted by guanine, resulting in glycine instead of arginine (Arg16Gly). Another common variant occurs at codon 27 where the nucleotide cytosine is substituted by guanine, changing a glutamic acid residue to a glutamine (Gln27Glu) (Hoit et al. 2000). In the general population, the frequency of the wild-type Gly16 variant of Arg16Gly polymorphism represents 52.44% while the wild-type Gln27 variant of Gln27Glu polymorphism represents 20.43% (Kerr et al. 2017). Those polymorphisms might promote vasodilatation, changes in nitric oxide, lipolysis and energy balance and therefore cardiovascular remodelling (Hoit et al. 2000).
Although previous studies have investigated the ADRB2 gene, the results remain inconsistent. Since ADRB2 is an important target for many drugs and management of hypertension and obesity, these variations in the frequency of ADRB2 genotypes may have directly influence in the aerobic exercise responses. Recently, it was demonstrated that individuals who carry the G allele in the Gln27Glu position may have an advantage in reducing body mass (Szendrei et al. 2016), while others studies reported no association between the Gln27Glu or Arg16Gly variant with obesity (Kawamura et al. 2001; Zhang et al. 2014). In fact, the heritability of training responses suggests the possibility that genomic factors may partly determine whether adaptations become more notable (Yang et al. 2011). Despite the fact that in a transversal study was demonstrated that homozygous for the ADRB2 Arg16 allele presented a lower resting HR, higher vagal modulation, and higher baroreflex sensitivity than carriers of the Gly16 allele, without the influence of Gln27Glu genotypes (Atala et al. 2015). Another study showed that in women and men between 40 and 65 years old that the variant genotype for both polymorphisms had a higher BMI at baseline and accentuated advantage to decrease it after adjustment for physical activity level (Meirhaeghe et al. 2001).
Furthermore, it is well established that exercise training improves autonomic balance in humans (Ramos et al. 2017; Goit et al. 2017) and reverses autonomic dysfunction and hypertension in rats (Sordi et al. 2017). However, controversy remains regarding which modalities induce the greatest magnitude of change. The current guidelines of the American College of Sports Medicine (ACSM) for maintenance and improvement of cardiorespiratory fitness and health recommend the practice of aerobic exercise 5–7 days per week, totaling at least 150 min at moderate intensity, such as 60–75% of maximal heart rate (HRmax) or 75 min at vigorous intensity, such as 80–95% of HRmax, or a combination of both, to achieve a total energy expenditure of ≥ 500–1000 MET·min·week−110. However, “lack of time” is one of the most commonly cited barriers to regular participation in physical activity programs (Gibala et al. 2012). Therefore, a modified exercise protocol that is time-efficient and has similar or better effects on cardiovascular health may increase the number of participants in physical activity programs (Alansare et al. 2018).
In the other hand, some studies have shown that high-intensity interval training (HIIT), which consists of repeated exercises at high intensity separated by short recovery periods, is a more effective stimulus for improving cardiorespiratory fitness compared to moderate continuous training (MCT) in individuals with metabolic syndrome (Tjønna et al. 2008), coronary artery disease (CAD) (Rognmo et al. 2004) and hypertension (Molmen-Hansen et al. 2011). However, the superiority of HIIT has not been demonstrated for CAF (Ramos et al. 2017).
In this case, we do not know whether there is a relationship between ADRB2 genetic variants influence on CAF after aerobic exercise training. Therefore, in this study, as a primary outcome we investigated the influence of ADRB2 genetic variants and their interaction on CAF in response to different volumes of HIIT and MCT in overweight or obese individuals. As a secondary outcome, we investigated the effects of HIIT and MCT in health parameters in overweight or obese individuals.
Subjects and methods
This study was approved by the Ethics Committee of the School of Physical Education and Sports of Ribeirão Preto of the University of São Paulo (CAEE 37573114.6.0000.5659). All participants provided written informed consent prior to participation in this study. The inclusion criteria were age ≥ 18 years, body mass index (BMI) ≥ 25 kg/m2, and waist circumference (WC) ≥ 80 cm for women and ≥ 90 cm for men. Exclusion criteria were planned operations during the research period, drug or alcohol abuse, use of any medication that alters autonomic modulation, or participation in a parallel study. Inclusion of participants started in January 2014 to August 2018 by phone, emails, and at the university hospital.
Participants
The study was conducted with 70 participants [47 females with a mean age (SD) of 52.0 (5.8); 23 males with a mean age (SD) of 35.6 (4.2)] years, who were considered sedentary according to the International Physical Activity Questionnaire (Hallal et al. 2010) at the beginning of the intervention. All 47 females’ participants were post-menopausal women.
Anthropometric measures
Weight (kg) was measured with a tetrapolar bioimpedance analyzer (model HBF-510 W, Brazil) (Hasnan et al. 2014) and height (m) using a Welmy stadiometer (model W110 H). BMI was calculated as follows: BMI = weight/height2. Waist circumference was determined using a measuring tape placed around the abdomen at the level of the umbilical scar, while standing relaxed (Fryar et al. 2012).
Blood pressure
Noninvasive systolic (SBP) and diastolic (DBP) blood pressure were measured in the upper arm using a digital manometer (OMRON, HEM-7113, Brazil) after sitting for five minutes at rest (Malachias et al. 2016). Accordingly, the Brazilian guideline for hypertension recommend lower systolic blood pressure of 160 mmHg and diastolic blood pressure under 100 mmHg to begin a physical exercise. In this sense, if the participants arrived to perform the test or the training session with high values of blood pressure, they were oriented to avoid exercise at that time.
Heart rate variability
The heart rate variability (HRV) was obtained using the RR intervals (RR) from the Polar Team2 heart rate (HR) transmitter, (Polar Electro Oy, Kempele, Finland) and recorded at a sampling frequency of 1000 Hz. The data were recorded and stored for further analysis. Prior to all tests, subjects were advised to abstain from drinking any beverages containing caffeine for at least 12 h.
Data collection was performed before of the cardiopulmonary test in a quiet room with a controlled temperature (23 ± 1 ºC) during the morning (7:00–10:00 a.m.). The participants were instructed to remain in the supine position for approximately 15 min to stabilize cardiovascular parameters while breathing spontaneously (Rodrigues et al. 2017). The HRV analyses were performed using custom computer software (CardioSeries v2.0, https://sites.google.com/site/cardioseries) developed by Dias, DPM of the University of São Paulo, Brazil. The RR values were redesigned in 3 Hz cubic spline interpolation, to normalize time interval between the beats. The interpolated RR series were divided into half-overlapping sets of 256 data points, overlapping 50% (Welch Protocol). The stationary segment was visually inspected and those with artifacts or transients were excluded. Each RR stationary segment was submitted to the spectral analysis by Fast Fourier Transform (FFT), after Hanning window. The RR time series were integrated in bands of low frequency (LF 0.04–0.15 Hz) and high frequency (HF 0.15–0.5 Hz) and the results are expressed in absolute values (ms2) and normalized units (nu). Furthermore, each RR stationary segment was used to calculate the plot-Poincare and RMSSD indexes.
The HRV normalized values were obtained by calculating the percentage of LF and HF power related to the total power of spectrum minus the very low frequency band (VLF; < 0.2 Hz). In addition, the normalization procedure was performed to minimize variations of total power in LF and HF absolute value. To assess sympathovagal balance, LF/HF ratio of RR variability was also calculated.
Cardiorespiratory fitness
The procedure to measure cardiorespiratory fitness has been described previously (Rognmo et al. 2004). Briefly, cardiorespiratory fitness was measured as the relative (mL/kg/min) peak oxygen uptake during an incremental treadmill exercise test at Imbramed Super ATL (Porto Alegre, Brazil). Before the test, the Polar Team sensor that records the HRV data was placed at the height of the mesosternal point. The participants performed 10 min of warm-up with the speed individually adjusted to a fast walking speed. Thereafter, the treadmill inclination was increased 2° every minute until voluntary exhaustion, maintaining the selected fast walking speed (Tjønna et al. 2008). A leveling-off of oxygen uptake despite increased work load and a respiratory exchange ratio > 1.05 were used as criteria for reaching the true VO2max, and both were achieved in all individuals in the present study. After achieving voluntary exhaustion, all participants spent at least 2 min in a cool-down period standing on the treadmill. This period was considered the recovery period. The value for the recovery of heart rate was defined as the reduction in heart rate from the rate at peak exercise to the rate 1 min after the cessation of exercise (Lindemberg et al. 2014).
Training protocol
After the 3 days of baseline evaluations, participants were randomized 1:1:1 using the Random Allocation Software (Saghei 2004) into 16 weeks of aerobic exercise of either (1) 1 bout of high-intensity training (1-HIIT), (2) 4 bouts of high-intensity interval training (4-HIIT), or (3) MCT. The MCT group trained five times per week whilst the HIIT groups trained three times a week, with at least 1 day between sessions. An exercise physiologist supervised two of the prescribed MCT and HIIT sessions in an exercise laboratory at the University of Sao Paulo. The residual exercise sessions were undertaken in an unsupervised environment. HR and rate of perceived exertion (RPE) were monitored and recorded during the course of the exercise program using an HR monitor (Polar Team2, Kempele, Finland) and the Borg 6–20 scale (Borg and Noble 1974). Supervised sessions were administered on a treadmill or a cycle ergometer, according to the participants’ orthopedic limitations or preference.
The protocols for each exercise intervention have been previously described (Ramos et al. 2017; Tjønna et al. 2018). Briefly, the MCT sessions were 30 min in duration at a target intensity of 60–70% HRmax or RPE of 11–13. Both HIIT groups were preceded by a 10 min warm-up and terminated with a 5 min cool-down. The 4-HIIT group trained for 40 min per session, consisting of four bouts of 4 min intervals at 85–95% HRmax or RPE of 15–17, separated by 3 min of active recovery at 50–70% HRmax or RPE of 13. The 1-HIIT group completed only one 4-min exercise bout at 85–95% HRmax or RPE of 15–17 (19 min/session). All participants were instructed to reach the target intensity (HR or RPE) within the first 2 min of the 4-min interval. All individuals performed at least 75% of all training sessions. The distribution of men and women in the training groups was as follows:1-HIIT (16 women and 9 men); 4-HIIT (19 women and 7 men); MCT (12 women and 7 men). For the analysis of the interaction of the ADRB2 gene, the HIIT and moderate exercise groups were merged.
Genotyping
On the second day of baseline evaluations, peripheral blood samples were drawn for genotyping. Genomic DNA was extracted by salting out (Lahiri and Nurnberger 1991). The purity and DNA concentration of the sample were evaluated by spectrophotometry (BioDropμlite PC). The ratios 260/280 and 260/230 were evaluated, and the level of purity adopted as a satisfactory minimum was 1.8 and a range of 2.0–2.2, respectively. Briefly, Arg16Gly variants at the position 46G > A (rs1042713) and Gln27Glu at the position 79C > G (rs1042714) were determined by real-time PCR (qPCR). The reaction was carried out using Custom TaqMan allele discrimination assays C 208476420 and C 208476520, respectively (Thermo Fisher, USA) and TaqMan genotyping master mix (Applied Biosystems, USA). Preparation of the reactions was performed according to the manufacturer’s specifications for each sample. The real-time PCR was performed on StepOnePlus equipment (Applied Biosystems, USA). For the polymorphism Arg16Gly rs1042713 the genotypes were identified in 97.1% of the samples while for the genotyping of the polymorphism Gln27Glu rs1042714 it was identified in 94.2% of the samples.
Data analysis
Continuous data are expressed as mean (standard deviation—SD). Linear mixed-effects models (when dependent variables were repeated measures) were performed to verify the associations between the exercise intervention and genetic variants. The sample size of at least ten in each group presented an 80% power to detect a difference between HF power means of 1 ms with a significance level of 0.05 (two-tailed), based on an SD of 0.78 ms obtained from time HRV recordings in a previous cohort of healthy female subjects (Mazurak et al. 2013). The genotypes were assessed according to the recessive genetic model, comprised as follows: the combined group of variant homozygotes and heterozygotes versus wild-type homozygotes. Furthermore, the both genotypes and haplotype analyses were adjusted by gender, age and type of training. Thus, it is possible to verify the effect of the haplotypes on the variables investigated by considering the following groups: H1 (all ancestral alleles), H2 (GG and CG + GG), H3 (CC and AA + AG) and H4 group (AA + AG and CG + GG). Within-group effect sizes of the exercise interventions were calculated using Cohen’s d effect size, interpreted as follows: Cohen’s d effect size (ES), small effect (0.20); small-to-medium effect (0.20–0.50); and medium-to-large effect (0.50–0.80). Differences were considered statistically significant at a p value < 0.05. The statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 23.0 for Windows).
Results
There were no significant differences between the exercise groups for anthropometric measures, BP, or cardiorespiratory fitness at baseline, except between the 1-HIIT and MCT for HR (Table 1). In addition, the 4-HIIT and MCT presented reduced BMI and WC after the intervention. Only the 1-HIIT presented reduced SBP after 16 weeks of training (ES = 0.35). In addition, the 4-HIIT demonstrated improved oxygen uptake in the economy of effort (ES = 0.76) and reduced HRRest (ES = 0.73), while the MCT presented increased peak oxygen uptake (ES = 0.83) and reduced HRRest (ES = 0.73).
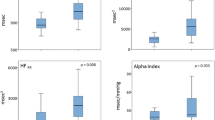
Differences in the HRV for plot-Poincare and time-domain indexes after 16 weeks of training considering the Arg16Gly genotypes are presented in Fig. 1. There was an improved in cardiac autonomic function through increases in RMSSD, SD1, and SD2 indexes after 16 weeks of exercise intervention. Figure 2 shows that there were no significant differences between the groups compared to the baseline condition considering the Arg16Gly genotypes in the frequency-domain analysis of HRV (p > 0.05).

Differences in HRV for the plot-Poincare and time-domain after 16 weeks of training for Arg16Gly genotype groups. RMSSD root mean square of successive differences, SD1 standard deviation of instantaneous beat-to-beat variability, SD2 long-term standard deviation of continuous RR intervals. *Significantly different from before within the group, p < 0.05. Linear mixed-effects models

Differences in HRV frequency domain after 16 weeks of training for Arg16Gly genotype groups. LF low frequency, HF high frequency, LF/HF low frequency and high frequency ratio. *Significantly different from before within the group, p < 0.05. Linear mixed-effects models
Figure 3 presented improved parasympathetic activity after the exercise intervention in all groups through increases in RMSSD, SD1, and SD2 indexes considering Gln27Glu polymorphism. However, considering frequency-domain, there were no significant differences between the groups compared to the baseline condition (p > 0.05) (Fig. 4).

Differences in HRV for the plot-Poincare and time-domain after 16 weeks of training for Gln27Glu genotype groups. RMSSD root mean square of successive differences, SD1 standard deviation of instantaneous beat-to-beat variability, SD2 long-term standard deviation of continuous RR intervals. *Significantly different from before within the group, p < 0.05. Linear mixed-effects models

Differences in HRV frequency domain after 16 weeks of training for Gln27Glu genotype groups. LF low frequency, HF high frequency, LF/HF low frequency and high frequency ratio. *Significantly different from before within the group, p < 0.05. Linear mixed-effects models
The influence of ADRB2 interaction (H1-H4) on health parameters and HRV after 16 weeks of training is presented in Table 2. All groups (H1–H4) demonstrated reduced WC. In addition, the H1, H2, and H3 groups presented reduced DBP after the intervention (Table 2). All groups (H1–H4) improved VO2Ec, VO2Peak, and HRRest. Only the H4 group showed reduced HRRecovery after the intervention. Furthermore, all groups presented significant increases in the SD1 index of HRV. The H1 group (all ancestral alleles) and H2 group (GG and CG + GG) showed increases in the RMSSD index (ES = 0.49 and ES = 0.69, respectively), which is associated with parasympathetic tonus. Only the H1 group demonstrated increases in the LF/HF ratio (ES = 0.36). Finally, the H3 group (CC and AA + AG) and H4 group (AA + AG and CG + GG) presented increases in the LF index of HRV (ES = 0.50 and ES = 0.25, respectively), which is associated with sympathetic tonus.
Discussion
The purpose of this study was to examine the influence of ADRB2 variants and their interaction on HRV in response to different volumes and intensities of aerobic exercise training in healthy individuals. The main findings were as follows: (1) The HRV changes were not influenced by the ADRB2 variants after the intervention; (2) The interaction of the ADRB2 gene analysis demonstrated that all groups responded positively for the SD1 index of HRV and only the H1 and H2 groups presented increases in the RMSSD index, which is associated with parasympathetic tonus. Furthermore, there was an increase in the LF index, which is associated with sympathetic tonus, only in the H3 and H4 groups.
With respect to the effect of exercise on HRV, it was reported that regular moderate-intensity exercise modulates cardiac autonomic control by enhancing vagal tone and lessening sympathetic influence in type 2 diabetes (Goit et al. 2017). For physically inactive adults, some studies have been suggested that the HIIT program is superior to MCT in improving HRV (Alansare et al. 2018) while others reported no significant differences between high-intensity and moderate-intensity exercise, although the authors highlighted that a combination of higher exercise intensity and volume (4-HIIT) had the greatest within group effect after 16 weeks of training in HRV on metabolic syndrome (Ramos et al. 2017).
The discrepancies among these studies may be caused by several factors, including environmental and genetic factors (Chen et al. 2015). In the circulatory system, ADRB2 is a major contributor to heart rate, myocardial contractility, and peripheral vasodilation (Matsunaga et al. 2007; Eisenach and Wittwer 2010). In this sense, our results are in line with the reported previously (Ramos et al. 2017), added to which the variant allele responded positively to exercise training. Our results showed no association between either ADRB2 variant, Arg16Gly and Gln27Glu, in the plot-Poincare and time-domain of HRV after 16 weeks of exercise training (Figs. 1 and 3). In addition, no association with frequency-time of HRV was found in the current study (Figs. 2 and 4). An increase in the SD1index means an increase in parasympathetic activity, while an increase in the SD2 index means a decrease in sympathetic activity (Tulppo et al. 1996). Thus, for the plot-Poincare and time domain analysis of HRV in the current study showed increased parasympathetic activity in healthy individuals after 16 weeks of exercise training.
In the interaction ADRB2 analysis in the present study, 16 weeks of different volumes of HIIT or MCT improved oxygen uptake and HRV, and reduced BMI, WC, HRRest, and DBP (Table 2). An interaction analysis is a combination of alleles at multiple loci that tend to be inherited together within a block of an individual chromosome (Nielsen et al. 2016). Only the H4 group demonstrated no significant difference in reduced DBP (Table 2). In addition, all groups presented reduced BMI and WC after exercise training (Table 2). Furthermore, all groups showed increases in the SD1 index, but only the H1 (GG and CC) and H2 (GG and CG + GG) groups presented increases in the RMSSD index of HRV, while the H3 (CC and AA + AG) and H4 (AA + AG and CG + GG) groups presented increases in the sympathetic tonus through increases in the LF index of HRV (Table 2). In line with our results, previous studies also reported that in supine rest, subjects homozygous for the ADRB2 Arg16 allele demonstrated lower HRV sympathetic indices (LF [%], LF/HF) and a higher HRV parasympathetic index (HF [%]) than carriers of the Gly16 allele. In addition, the BP indices were lower among ADRB2 Arg16 homozygous subjects than among Gly16 carriers, and these effects of the Arg16 homozygote on BP indices were also observed in the ADRB2 diplotype–based analysis for the Arg16Gly and the Gln27Glu variants (Matsunaga et al. 2007). Furthermore, in agreement with our data, other authors reported a significant association of a common ADBR2 variant, Arg16Gly, with a nonlinear HRV measure derived from the information-based similarity method, indicating an impact of this variant on acceleration/deceleration patterns of heart rate oscillations. The authors found that homozygous Arg16 carriers demonstrate lower sympathetic activity and no statistical association was found between the ADRB2 Gln27Glu genotype and HRV indices (Yang et al. 2011).
The ADRB2 gene has also been associated with obesity. However, individual reports regarding genetic variants of this gene with obesity have produced inconsistent results (Zhang et al. 2014; Chen et al. 2015; Costa-Urrutia et al. 2017). In a recent meta-analysis, for example, it was demonstrated that obesity susceptibility is associated with the Gln27Glu variant of ADRB2 rather than the Arg16Gly variant (Zhang et al. 2014). In the analysis of BMI, our data showed the influence of the gene variants interaction (Table 2). In the other hand, other study reported no effect of Gln27Glu on BMI or percentage body fat at baseline and the authors also reported that after supervised exercise, men carrying the Glu27 allele lost more weight and had a lower BMI than the Gln27Gln group, suggesting that supervised exercise and the Glu27 allele together in men can be beneficial to losing more weight (Szendrei et al. 2016). However, in the HERITAGE Study, for example, the authors found that carriers of any Glu27 allele in ADRB2 lost less fat, through computed tomography, than non-carriers following 20 weeks of endurance training (Garenc et al. 2003). The discrepancy between studies is unclear and may be due, in part, to differences in measurement techniques, as well as race, sex, age, BMI, and the intensity and duration of the intervention.
Furthermore, the data of the current study showed improvements of + 9.5%, + 9.6%, and + 14.6% in VO2peak for the 1-HIIT, 4-HIIT, and MCT, respectively (Table 1). The improvements in VO2peak in healthy untrained men after high-intensity and moderate-intensity exercise training (14% and 7%, respectively) has been reported with an advantage in the high-intensity group (Nybo et al. 2010). However, the protocol considered “moderate intensity” by the researchers, was performed at 80% of the maximal heart rate, an intensity considered high by other groups (Heydari et al. 2013). In this sense, others authors also reported that moderate and high-intensity exercise were able to provide similar improvements in cardiorespiratory fitness in 16 healthy adults. The authors observed a 20% increase in VO2peak in the high-intensity group and 15.1% in the moderate intensity group, without statistical significance between them (Gaesser and Rich 1984).
Our results showed that 4-HIIT and MCT are beneficial to increase HRV and cardiorespiratory fitness and also reduce anthropometric measures and blood pressure. The novelty of the current study is the analysis of genetic variants and interaction derived from the ADBR2 gene in response to exercise. Although this was a novel attempt to explore this relationship, the small sample size was an important limitation.
In conclusion, our data demonstrated a positive effect of the aerobic exercise training on the studied health parameters and the response to improve cardiac autonomic function through increased HRV, which seemed to be associated with the interaction between both ADBR2 gene variants.
Perspective
Collectively, the findings from our study provide that the adaptations of the cardiac autonomic nervous system through heart rate variability analysis seems interacting with β2 adrenergic receptor (ADRB2) variants following high-intensity interval training (HIIT) or moderate continuous exercise. In this sense, this study showed the influence of genetic characteristics in response to exercise. The findings of the current investigation have potential implications for the practices and physiological understanding of individuals undertaking long‐term aerobic exercise. Future research in this area is clearly warranted and the authors suggest that the characteristics of genetics should be used to randomize the participants. Variations in the ADRB2 gene can affect responses to drug actions, thereby impacting diseases in which ADRB2 plays a role, such as obesity and hypertension. The results of this study could therefore be of importance for the clinical management of these diseases, including an exercise program as a non-pharmacological treatment considering a customization based on genetic profile.
Abbreviations
- ACSM:
-
American College of Sports Medicine
- ADRB2:
-
β2 Adrenergic receptor
- BMI:
-
Body mass index
- CAD:
-
Coronary artery disease
- CAF:
-
Cardiac autonomic function
- DBP:
-
Diastolic blood pressure
- ES:
-
Effect size
- FFT:
-
Fast Fourier Transform
- HF:
-
High frequency
- HIIT:
-
High-intensity interval training
- HR:
-
Heart rate
- HRV:
-
Heart rate variability
- LF:
-
Low frequency
- LF/HF:
-
Low frequency high frequency ratio
- MCT:
-
Moderate continuous training
- RPE:
-
Perceived exertion
- SBP:
-
Systolic blood pressure
- SD:
-
Standard deviation
- VLF:
-
Very low frequency
- WC:
-
Waist circumference
References
Alansare A, Alford K, Lee S, Church T, Jung HC (2018) The effects of high-intensity interval training vs. moderate-intensity continuous training on heart rate variability in physically inactive adults. Int J Environ Res Public Health 15:1–10
Atala MM, Goulart A, Guerra GM, Mostarda C, Rodrigues B, Mello PR et al (2015) Arg16Gly and Gln27Glu β2 adrenergic polymorphism influence cardiac autonomic modulation and baroreflex sensitivity in healthy young Brazilians. Am J Transl Res 7(1):153–161
Borg G, Noble BJ (1974) Perceived exertion. In: Wilmore J (ed) Exercise and sport sciences reviews. Academic Press, New York, pp 131–153
Chen Y, Wang X, Shen Z, Fan P, Liu R, Liu Y et al (2015) Effect of the beta-3 adrenergic receptor Trp64Arg and uncoupling protein 4-3826 A %3e G genotypes on lipid and apolipoprotein levels in overweight/obese and non-obese Chinese subjects. Lipids in Health Dis 14:34
Costa-Urrutia P, Abud C, Franco-Trecu V, Colistro V, Rodríguez-Arellano ME, Vázquez-Pérez J et al (2017) Genetic obesity risk and attenuation effect of physical fitness in mexican-mestizo population: a case-control study. Ann Hum Genet 81:106–116
de Sordi CC, Lemos MDP, Marocolo M, Chriguer RS, Mendes EL, da Mota GR et al (2017) Exercise training reverse autonomic dysfunction and hypertension in rats fed with high-fat diet. Mot Rev Educ Física 23:1–10
Dessy C, Moniotte S, Ghisdal P, Havaux X, Noirhomme P, Balligand JL (2004) Endothelial β3-adrenoceptors mediate vasorelaxation of human coronary microarteries through nitric oxide and endothelium-dependent hyperpolarization. Circulation 110:948–954
Eisenach JH, Wittwer ED (2010) β-Adrenoceptor gene variation and intermediate physiological traits: prediction of distant phenotype. Exp Physiol 95:757–764
Fryar CD, Gu Q, Ogden CL (2012) Anthropometric reference data for children and adults: United States, 2007–2010. Vital Health Stat 11:1–48
Gaesser GA, Rich RG (1984) Effects of high- and low-intensity exercise training on aerobic capacity and blood lipids. Med Sci Sports Exerc 16:269–274
Garenc C, Pérusse L, Chagnon YC, Rankinen T, Gagnon J, Borecki IB et al (2003) Effects of β2-adrenergic receptor gene variants on adiposity: The HERITAGE Family Study. Obes Res 11:612–618
Gibala MJ, Little JP, Macdonald MJ, Hawley JA (2012) Physiological adaptations to low-volume, high-intensity interval training in health and disease. J Physiol 590:1077–1084
Goit RK, Pant BN, Shrewastwa MK (2017) Moderate intensity exercise improves heart rate variability in obese adults with type 2 diabetes. Indian Heart J 4:486–491
Hallal PC, Gomez LF, Parra DC, Lobelo F, Mosquera J, Florindo AA et al (2010) Lições Aprendidas Depois de 10 Anos de Uso do IPAQ no Brasil e Colômbia. J Phys Act Health 7:259–264
Hasnan M, Shahar S, Zaitun MY, Ahmad Z (2014) Validation of body composition measured by skinfold thickness technique and bioelectrical impedance analysis versus dualenergy X-ray absorptiometry among elderly with sarcopenia. Asian J Gerontol Geriatr 9:85–92
Heydari M, Boutcher YN, Boutcher SH (2013) High-intensity intermittent exercise and cardiovascular and autonomic function. Clinl Auton Res 23(1):57–65
Hoit BD, Suresh DP, Craft L, Walsh RA, Liggett SB (2000) Beta2-adrenergic receptor polymorphisms at amino acid 16 differentially influence agonist-stimulated blood pressure and peripheral blood flow in normal individuals. Am Heart J 139:537–542
Kawamura T, Egusa G, Fujikawa R, Okubo M (2001) Gln27Glu variant of the β2-adrenergic receptor gene is not associated with obesity and diabetes in Japanese–Americans. Metabolism 50:443–446
Kerr KF, Avery CL, Lin HJ, Raffield LM, Zhang QS, Browning BL et al (2017) Genome-wide association study of heart rate and its variability in Hispanic/Latino cohorts. Hear Rhythm 14:1675–1684
Lahiri DK, Nurnberger JI Jr (1991) A rapid non-enzymatic method for the preparationof HMW DNA from blood for RFLP studies. Nucleic Acids Res 19:5444
Lindemberg S, Chermont S, Quintão M, Derossi M, Guilhon S, Bernardez S et al (2014) Heart rate recovery in the first minute at the six-minute walk test in patients with heart failure. Arq Bras Cardiol 102:279–287
Malachias MVB, Souza WKSB, Plavnik FL et al (2016) VII Diretriz Brasileira de Hipertensão Arterial. Arq Bras Cardiol 107:1–83
Matsunaga T, Yasuda K, Adachi T, Gu N, Yamamura T, Moritani T et al (2007) Association of β-adrenoceptor polymorphisms with cardiac autonomic modulation in Japanese males. Am Heart J 154:759–766
Mazurak N, Gü Nther A, Grau F, Muth E, Pustovoyt M, Bischoff S et al (2013) Effects of a 48-h fast on heart rate variability and cortisol levels in healthy female subjects. Eur J Clin Nutr 6732:401–406
Meirhaeghe A, Luan JP, Selberg-Franks S et al (2001) The effect of theGly16Arg polymorphism of the b2-adrenergic receptorgene on plasma free fatty acid levels is modulated byphysical activity. J Clin Endocrinol Metab 86:5881–5887
Molmen-Hansen HE, Stolen T, Tjonna AE, Aamot IL, Ekeberg IS, Tyldum GA, Stoylen A (2011) Aerobic interval training reduces blood pressure and improves myocardial function in hypertensive patients. Eur J Prev Cardiol 19:151–160
Nielsen M, Staalsoe JM, Ullum H, Secher NH, Nielsen HB, Olsen NV (2016) The Gly16 allele of the Gly16Arg single-nucleotide polymorphism in the β2-adrenergic receptor gene augments perioperative use of vasopressors: a retrospective cohort study. Anesth Analg 122:1385–1393
Nybo l, Sundstrup E, Jakobsen MD, Mohr M, Hornstrup T, Simonsen L et al (2010) High-intensity training versus traditional exercise interventions for promoting health. Med Sci Sport Exerc 42:1951–1958
(PDF) Effect of 2-adrenergic receptor polymorphisms on epinephrine and exercise-stimulated lipolysis in humans. Available from: https://www.researchgate.net/publication/262492615_Effect_of_2-adrenergic_receptor_polymorphisms_on_epinephrine_and_exercise-stimulated_lipolysis_in_humans [accessed Nov 20 2019].
Ramos JS, Dalleck LC, Borrani F, Beetham KS, Mielke GI, Dias KA et al (2017) High-intensity interval training and cardiac autonomic control in individuals with metabolic syndrome: a randomised trial. Int J Cardiol 245:245–252
Rodrigues JAL, Ferrari GD, Fernandes IA, Ferezin LP, Trapé ÁA, Bueno Júnior CR (2017) Characterization of the heart rate variability in individuals with metabolic syndrome. Rev Bras Med do Esporte 23:208–2012
Rognmo Ø, Hetland E, Helgerud J, Hoff J, Slørdahl S (2004) High intensity aerobic interval exercise is superior to moderate intensity exercise for increasing aerobic capacity in patients with coronary artery disease. Eur J Cardiovasc Prev Rehabil 11:216–222
Saghaei M (2004) Random allocation software for parallel group randomized trials. BMC Med Res Methodol 4:1–6
Szendrei B, González-Lamuño D, Amigo T, Wang G, Pitsiladis Y, Benito PJ et al (2016) Influence of ADRB2 Gln27Glu and ADRB3 Trp64Arg polymorphisms on body weight and body composition changes after a controlled weight-loss intervention. Appl Physiol Nutr Metab 41:307–314
Tjønna AE, Lee SJ, Rognmo Ø, Stølen TO, Bye A, Haram PM et al (2008) Aerobic interval training versus continuous moderate exercise as a treatment for the metabolic syndrome: a pilot study. Circulation 118:346–354
Tjønna AE, Ramos JS, Pressler A, Halle M, Jungbluth K, Ermacora E et al (2018) EX-MET study: Exercise in prevention on of metabolic syndrome—a randomized multicenter trial: rational and design. BMC Public Health 18(1):437
Tulppo MP, Makikallio TH, Takala TE, Seppanen T, Huikuri HV (1996) Quantitative beat-to-beat analysis of heart rate dynamics during exercise. Am J Physiol Circ Physiol 271:H244–H252
Yang AC, Tsai S-J, Hong C-J, Wang C, Chen T-J, Liou Y-J et al (2011) Clustering heart rate dynamics is associated with β-adrenergic receptor polymorphisms: analysis by information-based similarity index. PLoS ONE 6:e19232
Zhang H, Wu J, Yu L (2014) Association of Gln27Glu and Arg16Gly polymorphisms in Beta2-adrenergic receptor gene with obesity susceptibility: a meta-analysis. PLoS ONE 9:e100489
Acknowledgements
The authors would like to thank all the participants for agreeing to participate in the study.
Funding
The present study was funded by FAPESP (Grant Number 2013/21159-8).
Author information
Authors and Affiliations
Contributions
JALR and CRBJ conceived and designed research. JALR, GDF, TCPG, VNM and SST conducted experiments. AET and HCDS contributed new reagents or analytical tools. JALR and AAT analyzed data. JALR wrote the manuscript. All authors read and approved the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by Keith Phillip George.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rodrigues, J.A.L., Ferrari, G.D., Trapé, Á.A. et al. β2 adrenergic interaction and cardiac autonomic function: effects of aerobic training in overweight/obese individuals. Eur J Appl Physiol 120, 613–624 (2020). https://doi.org/10.1007/s00421-020-04301-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-020-04301-z