
Abstract
Characterization of critical power/torque (CP/CT) during voluntary exercise requires maximal effort, making difficult for those with neuromuscular impairments. To address this issue we sought to determine if electrically stimulated intermittent isometric exercise resulted in a critical end-test torque (ETT) that behaved similar to voluntary CT. In the first experiment participants (n = 9) completed four bouts of stimulated exercise at a 3:2 duty cycle, at frequencies of 100, 50, 25 Hz, and a low frequency below ETT (Sub-ETT; ≤ 15 Hz). The second experiment (n = 20) consisted of four bouts at a 2:2 duty cycle—two bouts at 100 Hz, one at an intermediate frequency (15–30 Hz), and one at Sub-ETT. The third experiment (n = 12) consisted of two bouts at 50 Hz at a 3:2 duty* cycle with proximal blood flow occlusion during one of the bouts. ETT torque was similar (p ≥ 0.43) within and among stimulation frequencies in experiment 1. No fatigue was observed during the Sub-ETT bouts (p > 0.05). For experiment 2, ETT was similar at 100 Hz and at the intermediate frequency (p ≥ 0.29). Again, Sub-ETT stimulation did not result in fatigue (p > 0.05). Altering oxygen delivery by altering the duty cycle (3:2 vs. 2:2; p = 0.02) and by occlusion (p < 0.001) resulted in lower ETT values. Stimulated exercise resulted in an ETT that was consistent from day-to-day and similar regardless of initial torque, as long as that torque exceeded ETT, and was sensitive to oxygen delivery. As such we propose it represents a parameter similar to voluntary CT.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Critical power (CP) is an integrative measure/concept that represents the “critical” or upper boundary of work output that can be maintained at metabolic steady state without leading to fatigue and task failure (Jones et al. 2010). As such it represents an important, but understudied, aspect of aerobic metabolic function. Exercise performed above CP inevitably results in fatigue in a time-predictable manner, often termed the power–duration relationship, where the higher the work rate is above CP, the shorter the exercise duration. Fatigue during exercise above CP is associated with depletion of creatine phosphate (PCr) stores, declines in pH, and accumulation of inorganic phosphate (Pi) (Jones et al. 2008; Poole et al. 1988).
The CP/power-duration concept has been shown to hold across exercise modalities such as cycling (Vanhatalo et al. 2007; Moritani et al. 1981; Poole et al. 1988), running (Broxterman et al. 2013; Pettitt et al. 2012), and intermittent isometric exercise (Kellawan et al. 2014; Burnley 2009; Burnley et al. 2012; Szczyglowski et al. 2017)—in which case the threshold is termed critical torque (CT). Burnley (2009) validated a protocol using the performance of 60 intermittent maximal isometric contractions over 5-min (at a 3:2 work to rest cycle) to evaluate CT in a single testing visit. Torque was shown to decline and then plateau over the final 30 s of this “all out” test, and yield CT values similar to those determined using multiple tests to failure above CT (Burnley 2009). When assessed in this manner both voluntary activation, assessed via twitch-interpolation, and potentiated doublet torque declined during the test indicating a role for both central and peripheral fatigue in the attainment of CT (Burnley 2009; Burnley et al. 2012). The development of central fatigue highlights the necessity of participants providing a maximal effort in order for a valid assessment of CT to be achieved—perhaps limiting the utility of assessing CT in populations such as older, sedentary individuals and those with neuromuscular impairments (e.g. multiple sclerosis, Parkinson’s) who are known to have difficulty maximally activating their muscles during exercise (Kent-Braun et al. 1994; Olive et al. 2003; Sabatier et al. 2006). Determining the distinct contribution(s) of central and peripheral factors to CT, especially during single session, all-out tests (where the central and peripheral contributions to fatigue might differ from tests employing multiple bouts), could provide important information regarding the specific loci of functional impairments/limitations in clinical populations and could lead to better and more specific exercise interventions.
The use of neuromuscular electrical stimulation (NMES) to evoke skeletal muscle contractions can provide information regarding the contribution of peripheral factors in fatigue because it bypasses the central nervous system. NMES is thought to activate muscle in a non-selective, spatially fixed manner (Gregory and Bickel 2005) which likely contributes to the heightened fatigue observed with NMES compared to force-matched voluntary contractions. Interestingly, several previous studies using intermittent NMES during isometric exercise have demonstrated a hyperbolic torque–duration relationship (Bickel et al. 2003; Russ and Binder-Macleod 1999; Slade et al. 2003), with torque declining over time and then reaching a plateau, that appears qualitatively similar to the relationship observed during voluntary exercise (Burnley 2009; Burnley et al. 2010; Kellawan et al. 2014; Szczyglowski et al. 2017). The observed plateau in torque likely represents a torque at which a metabolic steady-state, dependent solely on a host of peripheral factors contributing to fatigue, was achieved.
The initial purpose of the present study was to test whether intermittent isometric exercise evoked by NMES reaches a “critical” steady-state in end-test torque (ETT). Once this was established we sought to examine whether this ETT: (1) was reliable across multiple testing days; (2) occurred at a similar torque level regardless of initial torque; and (3) was sensitive to oxygen delivery, which was manipulated by altering the work-to-rest (duty cycle) of the intermittent contractions and by occluding blood flow to the exercising muscles.
Methods
Participants
The study consisted of three separate experiments. Nine healthy volunteers (5 men, 4 women; 23 ± 1.6 years, 176.0 ± 10.7 cm, 82.9 ± 15.6 kg) participated in experiment 1, 20 healthy volunteers (10 men, 10 women; 25.0 ± 2.8 years, 174.5 ± 9.1 cm, 77.5 ± 16.8 kg) participated in experiment 2, which was part of a larger study, and 12 healthy males (24.2 ± 2.1 years, 182.4 ± 6.8 cm, 89.2 ± 13.4 kg) participated in experiment 3, which was part of another larger study. All participants provided written informed consent prior to participation in the study, which was approved by the University of Oklahoma Institutional Review Board and complied with the Declaration of Helsinki. Participants were instructed to refrain from strenuous lower body exercise in the 24-h preceding each visit. Participants were also asked to refrain from caffeine consumption 8 h prior to testing and to be food-fasted 2 h before testing.
Dynamometry
All testing was performed using a KinCom isokinetic dynamometer (KinCom, Chattanooga, TN, USA). Participant positioning was similar to previous studies (Bickel et al. 2003; Burnley 2009). Briefly, participants were seated in the dynamometer and positioned with the hip joint of 85° (with 0° being full extension) and the knee joint angle of 70° below horizontal. The lower leg was strapped to the lever arm at the ankle using an inelastic Velcro strap, and the participant was firmly strapped to the seat at the waist and chest. Participant position was marked and recorded to ensure continuity throughout the study.
Maximal voluntary isometric contractions
On each testing day for all three experiments participants’ maximal voluntary contraction strength (MVC) with their knee extensors of their dominant leg was initially assessed. Each contraction lasted 3 s, and 2 min of rest was provided between each successive attempt. Participants were cued to contract and relax by a metronome and verbal instruction from the researcher. Strong verbal encouragement was also provided during each effort. The peak torque value from the plateau region of the force tracing was calculated. Values from two efforts that differed by ≤ 5% were averaged and served as the criterion value for MVC.
Train current determination
Following determination of their MVC, a current determination protocol was completed to determine the amplitude of stimulation used during each of the 5-min tests. Stimulating electrodes (3ʺ × 4ʺ; PALS Platinum; Axelgaard; Fallbrook, CA, USA) were placed over the proximal vastus lateralis and over the distal vastus medialis. Stimulation electrode positions were marked with indelible ink to ensure continuity throughout the duration of each study. A constant current stimulator (model DS7AH; Digitimer, Hertfordshire, England) controlled by a custom-written program in Biopac Acknowledge software was used for electrical stimulation. Pulse duration was held constant at 200 µs. Participants initially received a single 100 Hz train, for 3 s (experiments 1 and 3) or 2 s (experiment 2) at a current of 30 mA. Stimulation intensity was then progressively increased by 10 mA and additional stimulations were applied every 20 s until the evoked force produced equaled 25% of the participant’s MVC. All participants tolerated the intensity of stimulation. For all experiments the current that was sufficient to elicit 25% of MVC during 100 Hz stimulation was used for all subsequent stimulation bouts. This was done as previous research has demonstrated that stimulation current determines the amount of muscle mass recruited during stimulated exercise (Adams et al. 1993) and that when current is held constant altering stimulation frequency does not alter recruited muscle mass (Black et al. 2008).
Stimulated exercise
Each participant completed NMES tests using constant frequency, constant current trains with initial torque varying by altering the stimulation frequency—depending on the experiment. Stimulated exercise was well tolerated by all participants regardless of whether the duty cycle was 3:2 or 2:2 with all participants completing all exercise bouts with minimal complaint of discomfort.
For experiment 1, volunteers completed a familiarization visit and two identical testing visits. During the testing visits participants completed the train current determination protocol and four separate 5-min NMES bouts using a 3:2 duty cycle (3 s of stimulation followed by 2 s of rest) with a total of 60 contractions per bout. Participants received 20 min of rest between each bout. The frequency used during the first bout was 100 Hz. During the second bout, a frequency that elicited a torque value below the ETT during the 100 Hz test (Sub-ETT; ≤ 15 Hz) was used. The third and fourth tests were at 50 and 25 Hz, applied in a random order. Following at least 24 h of rest, participants returned to the lab and the four exercise bouts were repeated.
For experiment 2, volunteers completed two testing visits. During each visit, participants completed two separate 5-min NMES bouts using a 2:2 duty cycle (2 s of stimulation followed by 2 s of rest) with a total of 75 contractions per bout. The first testing visit consisted of tests at 100 Hz and a low frequency (Sub-ETT; ≤ 15 Hz), with 30 min of rest between each test. A frequency that elicited an initial torque value below the ETT during the 100 Hz test was used for this bout. The second visit consisted of tests at 100 Hz and an intermediate frequency (15–30 Hz), again, with 30 min of rest between each test. A frequency eliciting a torque equal to 50% of the difference between peak torque and ETT from the 100-Hz protocol was used for the intermediate frequency.
For experiment 3, volunteers also completed two testing visits. During each visit, participants completed a 5-min NMES test at a 3:2 duty cycle (60 contractions per bout) at 50 Hz. During one of the visits, vascular blood flow in the dominant leg was occluded by inflating a pneumatic pressure cuff (Hokanson, Bellevue, WA) placed around the proximal portion of the thigh. The cuff was inflated to 220 mmHg for every participant. The cuff was inflated for 5 min prior to the start of the NMES test while the participant rested and remained inflated until the completion of the 5-min test.
Data analysis
Peak force of each contraction was determined for every 5-min test. Force output was converted to torque by multiplying the measured force by the moment arm at the knee and expressed as an absolute torque value (N m). In order to aid in comparisons among experiments and stimulation frequencies relative torque (%) was expressed as a percentage of starting torque at 100 Hz for experiments 1 and 2 and of starting torque at 50 Hz for experiment 3. ETT was calculated as the average torque of the final six contractions (30 s) for the 3:2 duty cycle (experiment 1 and 3) and the final seven contractions (28 s) for the 2:2 duty cycle (experiment 2). Impulse above the end-test torque (∫T Total) was calculated as the area under the torque–time curve that was above ETT. The area for each contraction was summed to yield the criterion value for ∫T Total.
Statistics
All statistical tests were performed using SPSS 24 (IBM, Armonk, NY, USA). For each stimulated exercise bout, a one-way analysis of variance (ANOVA) was initially performed on the final six contractions (experiment 1 and 3) and final seven contractions (experiment 2) to determine if a plateau in torque occurred. Once this was confirmed, absolute and relative ETT as well as ∫T Total were compared among the different stimulation protocols. For experiment 1, a 2 (visit 1, 2) × 4 (100, 50, 25 Hz, and Sub-ETT) repeated measures ANOVA within participant analysis was performed to determine if ETT differed among the protocols or between testing visits. For experiment 2, a one-way ANOVA was performed to compare absolute and relative ETT, and ∫T Total among the 100 Hz protocol from visit 1 and visit 2, the intermediate protocol and the Sub-ETT protocol. Main effects were only interpreted in the absence of a significant interaction. Post-hoc comparisons among the protocols were performed using a paired samples t test. Absolute and relative ETT and ∫T Total between the control and occluded conditions in experiment 3 were analyzed using a two-tailed paired samples t test. The effect of duty cycle (3:2 vs. 2:2) on ETT at 100 Hz was examined using an independent samples t test to compare vales from experiment 1 and experiment 2. Since no differences were found between 100 Hz testing visits in both experiments 1 and 2, the values from each visit were averaged for this analysis. Significance was set a priori at p ≤ 0.05.
Results
Experiment 1
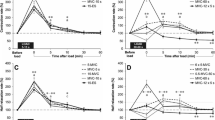
Stimulated torque declined (p < 0.001) over the course of the 5-min protocol during both testing visits at 100, 50, and 25 Hz stimulation (Fig. 1; Table 1). No changes (p ≥ 0.43) were observed in the Sub-ETT protocol during either visit when the final contractions were compared to initial. Torque plateaued during the final six contractions of each protocol during both testing visits (Fig. 1). The visit × stimulation protocol interaction for absolute ETT was not significant (p = 0.39), nor was the main effect for visit (p = 0.18). A main effect for protocol was found (p < 0.001) with values from the Sub-ETT protocol being lower than ETT from 100, 50, and 25 Hz (p ≤ 0.004; Table 1). Similar results were found for relative ETT (normalized to starting torque at 100 Hz) with the interaction (p = 0.44) and main effect for visit (p = 0.65) not being significant while a main effect for protocol (p < 0.001) was found with the Sub-ETT protocol (p ≤ 0.001) being reduced from 100, 50, and 25 Hz protocols (Fig. 1). No differences were found among the 100, 50, and 25 Hz protocols (p ≥ 0.13). ∫T Total did not differ between testing visits (p = 0.84 for the interaction and p = 0.42 for the main effect). A significant main effect for stimulation protocol was found (p = 0.002; Table 1) with values from 100 and 50 Hz not differing (p = 0.98), while values from 25 Hz were reduced compared to 100 Hz (p = 0.02) and 50 Hz (p = 0.001).

Mean (n = 9) contraction by contraction peak torque normalized to the starting torque during 100 Hz stimulation over two testing visits (a, b) during 100, 50, and 25 Hz stimulation at a 3:2 duty cycle. During the Sub-ETT bout, the stimulation frequency was lowered (typically 5–15 Hz) to elicit an initial torque lower than the determined ETT of the other stimulation frequencies. Error bars are not shown for the sake of clarity
Experiment 2
Stimulated torque declined (p < 0.001) over the course of the 5-min protocol during both 100 Hz stimulations (visit 1 and visit 2), and during the intermediate stimulation frequency protocol (Fig. 2; Table 2). No changes were observed over time in the Sub-ETT protocol (p = 0.71). Torque plateaued during the final seven contractions of each protocol during both testing visits (Fig. 2). Absolute ETT did not differ among both 100 Hz protocols and the intermediate protocol (p ≥ 0.29; Table 2), but values from the Sub-ETT protocol were lower than those from 100 Hz and the intermediate protocol (p ≤ 0.001; Table 2). Similar results were found for relative ETT (normalized to starting torque at 100 Hz) with differences observed among the 100 Hz protocols and the intermediate protocol (p ≥ 0.11), but the Sub-ETT protocol was reduced (p < 0.001) from the 100 Hz and intermediate protocols (Table 2). ∫T Total did not differ between the 100 Hz protocols (p = 0.36), but values from the intermediate protocol were reduced compared to both 100 Hz protocols (p < 0.001; Table 2).

Mean (n = 20) contraction by contraction peak torque normalized to starting torque during 100 Hz stimulation using a 2:2 duty cycle for both visits at 100 Hz, at an intermediate stimulation frequency (typically 15–30 Hz) and a Sub-ETT bout (typically 5–15 Hz) eliciting an initial torque lower than the determined ETT from the other stimulation frequencies. Error bars not shown for clarity
Experiment 3
Stimulated torque declined (p < 0.001) over the course of the 5-min protocol using 50 Hz stimulation in both the control and occluded conditions (Fig. 3). Additionally, torque plateaued during the final six contractions in each condition (Fig. 3). Absolute (p < 0.001) and relative (p < 0.001) ETT were significantly reduced in the occluded condition (Fig. 3; Table 3). ∫T Total increased (p = 0.03) by ~ 39% in the occluded condition compared to control.

Contraction by contraction peak torque normalized to starting torque during 50 Hz stimulation at a 2:2 duty cycle between control (closed circle) and occluded (open circle) conditions. *Significant difference in ETT (mean of the final six contractions) between conditions (p < 0.05)
Effects of duty cycle
When data from 100 Hz stimulation in experiment 1 were compared to 100 Hz stimulation in experiment 2, reducing the duty cycle of stimulation from 3:2 to 2:2 resulted in a 31% increase (13.0 ± 4.0 vs. 17.2 ± 4.1 N m; p = 0.02; Fig. 4) in absolute ETT. Relative ETT increased 30% (29.9 ± 4.6 vs. 31.2 ± 5.7 N m; p = 0.002; Fig. 4) in the 2:2 condition compared to the 3:2 duty cycle condition.

Comparison of group peak torque during 100 Hz stimulation between the 3:2 (n = 9) and 2:2 (n = 20) duty cycles relative to starting torque. Since no differences were observed between visit 1 or visit 2 for either stimulation duty cycle, the visits were averaged for this comparison. Error bars represent SEM (for clarity). *Significant difference in ETT between duty cycles (p < 0.05)
Discussion
In the current study, we have demonstrated that torque output during contractions evoked by intermittent electrical stimulation mirrors the hyperbolic decline and subsequent plateau observed during voluntary contractions—suggesting attainment of a critical end-test torque. Additionally, the observed ETT was found to be reliable over multiple testing days, was similar regardless of starting torque, and was reduced when oxygen delivery altered by increasing the contraction duty cycle and when proximal blood flow occlusion was applied, again mimicking findings under voluntary conditions.
In our initial experiment we found that ETT plateaued at a similar torque value during stimulation at 100, 50, and 25 Hz and that ETT values were similar from day-to-day. The attainment of a plateau in ETT is consistent with observations from previous studies (Bickel et al. 2003; Russ and Binder-Macleod 1999; Slade et al. 2003) employing intermittent stimulated exercise. Under voluntary conditions submaximal work performed above CP/CT results in fatigue that occurs in a predictable manner that is inversely related to how far the work rate exceeds CP/CT (Jones et al. 2008; Burnley 2009). In the present study, contraction torque was manipulated by altering stimulation frequency while holding stimulation amplitude constant. This enabled us to alter work rate and metabolic intensity without altering activated skeletal muscle mass (Black et al. 2008; Gorgey et al. 2009). Four stimulation frequencies were employed, three of which resulted in a starting torque that was above ETT and one where initial torque was below ETT. The finding that torque declined to a similar ETT when initial torque was above ETT, regardless of how far, and that no fatigue occurred when starting torque was below ETT of 100, 50, and 25 Hz stimulation supports the supposition that a critical threshold exists for repeated intermittent stimulated exercise. In experiment 2 we found similar results for day-to-day reproducibility and for the effects of altering initial torque on ETT while employing a 2:2 duty cycle. Again, the findings support the idea of a critical torque threshold where a metabolic steady-state can be achieved.
As the voluntary critical threshold represents an oxygen-dependent, metabolic steady-state, changes in blood flow to working skeletal muscle, either via occlusion or changes in the work-to-rest cycle, have been shown to affect CP/CT (Broxterman et al. 2015, 2014). In experiment 3 occluding blow flow to contracting skeletal muscle resulted in a 68% reduction in ETT compared to the control, unoccluded condition. When expressed relative to the initial torque, ETT occurred at only 12% of starting torque. Our findings under occluded conditions are consistent with those of Broxterman et al. (2015) who demonstrated that during voluntary exercise occlusion resulted in a reduction of CP to essentially zero. Broxterman et al. (2014) also demonstrated that increasing the work-to-rest cycle during intermittent exercise lead to greater oxygen desaturation and a concomitant reduction in CP. Given this, we compared ETT during 100 Hz stimulation in experiment 1 (employing a 3:2 duty cycle) and experiment 2 (employing a 2:2 duty cycle). Reducing the work-to-rest cycle from 3:2 to 2:2 resulted in ETT values that were ~ 30% higher. Taken together our findings that altering oxygen delivery to working muscles by increasing the duty cycle and by applying occlusion indicate, much like voluntary CP/CT, that stimulated ETT is also sensitivity oxygen delivery.
During voluntary cycling exercise, the finite amount of work that can be performed above CP is represented by the term W′ with task failure being closely associated with the depletion of W′. Under isometric conditions the summed impulse above critical torque (IACT) calculated for each contraction may represent a physiological parameter similar to W′ (Kellawan et al. 2014), although data from Burnley (2009) disagree with this assertion. In the present study we found that the summed area under the torque–time curve (∫T Total) was similar from day-to-day in both experiment 1 and experiment 2 when the initial torque value was greater than ETT. When initial torque was reduced by reducing stimulation frequency (the 25 Hz protocol in experiment 1 and the intermediate protocol in experiment 2) ∫T Total declined compared the 100 and 50 Hz protocols which yielded higher initial torques. This finding was somewhat unexpected as under voluntary conditions the magnitude of W′ (Broxterman et al. 2015; Jones et al. 2008; Monod and Scherrer 1965) and IACT (Kellawan et al. 2014) was conserved across bouts of exhaustive exercise above CP/CT. The most likely explanation of this finding is that the reduction in ∫T Total is a consequence of the reduced starting torque, and relatively similar pattern of torque decline over time to a similar ETT among the different stimulation frequencies. These findings provide additional evidence that the physiological determinants of ∫T Total are likely not identical to those of W′. Interestingly, under conditions of blood flow occlusion ∫T Total was increased 39%. Broxterman et al. (2015) found W′ also increased (an average of 49%) under conditions of blood flow occlusion. It has been suggested (Coats et al. 2003; Ferguson et al. 2010) W′ may be determined by the integration of several mechanisms and may not solely be due to the performance of a finite amount of work. The modeling performed by Broxterman et al. (2015) suggests that especially at low power outputs that a portion of W′ may be used for factors that are not related to external work performance. The similar increase in ∫T Total in the occluded condition in the present study suggests that ∫T Total is also an integrative measure and might be used for factors unrelated to external work—although future studies specifically designed to test this supposition are needed.
We believe our findings can be particularly useful in furthering the understanding of peripheral and central factors in fatigue in populations who have difficulty performing maximal contractions such as those with neuromuscular disorders and the aged. Critical power represents an important, but understudied, parameter of aerobic metabolic function. It has been shown to be a better predictor of functional performance tasks than more commonly assessed parameters such as \(\dot {V}\)O2 peak and lactate threshold (Ade et al. 2014). Despite its usefulness, few studies have attempted to determine CP in clinical populations—likely due the necessity of sustained maximal efforts for its determination. The NMES exercise test employed in the present study provides a potential alternative test to study aspects of peripheral metabolic function in individuals for whom a maximal voluntary effort is difficult and/or contraindicated. The NMES test was well tolerated in our participants using the 2:2 and 3:2 stimulation duty cycles with all participants completing all of the 5-min exercise tests with little to no complaints of discomfort. Additionally, ETT plateaued before the final 30-s regardless of the duty cycle and stimulation frequency used (at approximately 4 min and 25 s at the 2:2 duty cycle and at approximately 3 min and 45 s at the 3:2 duty cycle)—suggesting the NMES test could be shortened if the length of the test is an issue in clinical populations.
In summary, we have demonstrated that intermittent exercise evoked by NMES yields a steady-state ETT, that is similar across both multiple testing sessions, yields similar values regardless of initial torque as long as that torque exceeds ETT, and when evoked torque is below ETT that no fatigue is observed. When taken together with our findings that ETT is sensitive to oxygen delivery we propose that ETT during NMES exercise represents a parameter similar to critical torque during voluntary exercise. We believe that this NMES protocol has the potential to be a useful tool in furthering our understanding of peripheral and central factors in fatigue during exercise and may prove especially useful in populations who have difficulty performing maximal contractions such as those with neuromuscular disorders and the aged.
Abbreviations
- ANOVA:
-
Analysis of variance
- CP:
-
Critical power
- CT:
-
Critical torque
- ETT:
-
End-test torque
- H+ :
-
Hydrogen ions
- IACT:
-
Impulse above critical torque
- ∫T Total :
-
Impulse above the end-test torque
- MVC:
-
Maximal voluntary contraction
- NMES:
-
Neuromuscular electrical stimulation
- PCr:
-
Creatine phosphate
- Pi :
-
Inorganic phosphate
- W′:
-
Finite amount of work that can be performed above CP
References
Adams GR, Harris RT, Woodard D, Dudley GA (1993) Mapping of electrical muscle stimulation using MRI. J Appl Physiol (Bethesda, MD: 1985) 74(2):532
Ade CJ, Broxterman RM, Craig JC, Schlup SJ, Wilcox SL, Barstow TJ (2014) Relationship between simulated extravehicular activity tasks and measurements of physical performance. Respir Physiol Neurobiol 203:19–27. https://doi.org/10.1016/j.resp.2014.08.007
Bickel CS, Slade JM, Warren GL, Dudley GA (2003) Fatigability and variable-frequency train stimulation of human skeletal muscles. (Research report). Phys Ther 83(4):366
Black CD, Elder CP, Gorgey A, Dudley GA (2008) High specific torque is related to lengthening contraction-induced skeletal muscle injury. J Appl Physiol (1985) 104(3):639–647. https://doi.org/10.1152/japplphysiol.00322.2007
Broxterman RM, Ade CJ, Poole DC, Harms CA, Barstow TJ (2013) A single test for the determination of parameters of the speed–time relationship for running. Respir Physiol Neurobiol 185(2):380–385. https://doi.org/10.1016/j.resp.2012.08.024
Broxterman RM, Ade CJ, Wilcox SL, Schlup SJ, Craig JC, Barstow TJ (2014) Influence of duty cycle on the power–duration relationship: observations and potential mechanisms. Respir Physiol Neurobiol 192:102–111. https://doi.org/10.1016/j.resp.2013.11.010
Broxterman RM, Ade CJ, Craig JC, Wilcox SL, Schlup SJ, Barstow TJ (2015) Influence of blood flow occlusion on muscle oxygenation characteristics and the parameters of the power–duration relationship. J Appl Physiol (Bethesda, MD: 1985) 118(7):880. https://doi.org/10.1152/japplphysiol.00875.2014
Burnley M (2009) Estimation of critical torque using intermittent isometric maximal voluntary contractions of the quadriceps in humans. J Appl Physiol 106(3):975
Burnley M, Vanhatalo A, Fulford J, Jones AM (2010) Similar metabolic perturbations during all-out and constant force exhaustive exercise in humans: a (31)P magnetic resonance spectroscopy study. Exp Physiol 95(7):798–807. https://doi.org/10.1113/expphysiol.2010.052688
Burnley M, Vanhatalo A, Jones AM (2012) Distinct profiles of neuromuscular fatigue during muscle contractions below and above the critical torque in humans. J Appl Physiol (Bethesda MD 1985) 113(2):215. https://doi.org/10.1152/japplphysiol.00022.2012
Coats E, Rossiter H, Day J, Miura A (2003) Intensity-dependent tolerance to exercise after attaining \(\dot {V}\)O2max in humans. J Appl Physiol 95(2):483–490
Ferguson C, Rossiter HB, Whipp BJ, Cathcart AJ, Murgatroyd SR, Ward SA (2010) Effect of recovery duration from prior exhaustive exercise on the parameters of the power–duration relationship. J Appl Physiol (Bethesda MD 1985) 108(4):866. https://doi.org/10.1152/japplphysiol.91425.2008
Gorgey AS, Black CD, Elder CP, Dudley GA (2009) Effects of electrical stimulation parameters on fatigue in skeletal muscle. J Orthop Sports Phys Ther 39(9):684–692. https://doi.org/10.2519/jospt.2009.3045
Gregory CM, Bickel CS (2005) Recruitment patterns in human skeletal muscle during electrical stimulation. Phys Ther 85(4):358
Jones A, Wilkerson D, Dimenna F, Fulford J, Poole D (2008) Muscle metabolic responses to exercise above and below the “critical power” assessed using 31P-MRS. Am J Physiol 294(2):R585
Jones AM, Vanhatalo A, Burnley M, Morton RH, Poole DC (2010) Critical power: implications for determination of \(\dot {V}\)O2max and exercise tolerance. (Report). Med Sci Sports Exerc 42(10):1876–1890
Kellawan JM, Tschakovsky ME, Alway SE (2014) The single-bout forearm critical force test: a new method to establish forearm aerobic metabolic exercise intensity and capacity. PLoS ONE 9(4). https://doi.org/10.1371/journal.pone.0093481
Kent-Braun JA, Sharma KR, Weiner MW, Miller RG (1994) Effects of exercise on muscle activation and metabolism in multiple sclerosis. Muscle Nerve 17(10):1162–1169. https://doi.org/10.1002/mus.880171006
Monod H, Scherrer J (1965) The work capacity of a synergic muscular group. Ergonomics 8(3):329–338. https://doi.org/10.1080/00140136508930810
Moritani T, Nagata A, Devries HA, Muro M (1981) Critical power as a measure of physical work capacity and anaerobic threshold. Ergonomics 24(5):339
Olive JL, Slade JM, Dudley GA, McCully KK (2003) Blood flow and muscle fatigue in SCI individuals during electrical stimulation. J Appl Physiol (1985) 94(2):701–708. https://doi.org/10.1152/japplphysiol.00736.2002
Pettitt RW, Jamnick N, Clark IE (2012) 3-min all-out exercise test for running. Int J Sports Med 33(6):426–431. https://doi.org/10.1055/s-0031-1299749
Poole DC, Ward SA, Gardner GW, Whipp BJ (1988) Metabolic and respiratory profile of the upper limit for prolonged exercise in man. Ergonomics 31(9):1265
Russ DW, Binder-Macleod SA (1999) Variable-frequency trains offset low-frequency fatigue in human skeletal muscle. Muscle Nerve 22(7):874
Sabatier MJ, Stoner L, Mahoney ET, Black C, Elder C, Dudley GA, McCully K (2006) Electrically stimulated resistance training in SCI individuals increases muscle fatigue resistance but not femoral artery size or blood flow. Spinal Cord 44(4):227–233. https://doi.org/10.1038/sj.sc.3101834
Slade JM, Bickel CS, Warren GL, Dudley GA (2003) Variable frequency trains enhance torque independent of stimulation amplitude. Acta Physiol Scand 177(1):87–92. https://doi.org/10.1046/j.1365-201X.2002.01053.x
Szczyglowski MK, Ade CJ, Campbell JA, Black CD (2017) The effects of exercise-induced muscle damage on critical torque. Eur J Appl Physiol 117(11):2225–2236. https://doi.org/10.1007/s00421-017-3710-1
Vanhatalo A, Doust JH, Burnley M (2007) Determination of critical power using a 3-min all-out cycling test. Med Sci Sports Exerc 39(3):548
Acknowledgements
The authors are thankful for the University of Oklahoma Graduate College Robberson Research and Creative Endeavors Grant and the Central States Chapter of the American College of Sports Medicine for their monetary support of this project. Thanks are also due to Jaisa Evanoff for her assistance with data collection and analysis.
Author information
Authors and Affiliations
Contributions
NJ and CB conceived of the experiments. NJ, CB, JC, and RL contributed to experimental design. NJ, RH, and DP collected the data. NJ, RH, DP, and CB performed data analysis. NJ and CB wrote the manuscript. All authors read approved the submitted version of the manuscript.
Corresponding author
Additional information
Communicated by Anni Vanhatalo.
Rights and permissions
About this article

Cite this article
Janzen, N.R., Hight, R.E., Patel, D.S. et al. Estimation of critical end-test torque using neuromuscular electrical stimulation of the quadriceps in humans. Eur J Appl Physiol 118, 1407–1414 (2018). https://doi.org/10.1007/s00421-018-3872-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-018-3872-5