
Abstract
Maximum strength training induces various improvements in the rate of force development (RFD) on a group level, but no study has investigated inter-individual adaptations in RFD. Fourteen men (28 ± 6 years old) performed the same 10-week maximum strength and then a 10-week power training program. Maximal force and RFD were recorded during maximal isometric leg extension voluntary contractions repeatedly before every 7th training session (2 sessions/week). After the intervention, subjects were retrospectively divided into three groups based on their RFD improvements: (1) improved only during the maximum strength period (MS-responders, + 100 ± 35%), (2) improved only during the power period (P-responders, + 53 ± 27%) or (3) no improvement at all (non-responders, + 3 ± 9%). All groups increased dynamic 1RM equally, but baseline 1RM was greater (p < 0.05) in responder vs non-responder groups. MS-responders had higher electrical stimulation-induced torque at baseline and they improved (+ 35 ± 28%) power production at 50% 1RM load more than P- (− 7 ± 20%, p = 0.052) and non-responders (+ 3 ± 6%, p = 0.066) during the maximum strength training period. MS-responders increased vastus lateralis cross-sectional area (+ 12 ± 9%, p < 0.01) as did P-responders (+ 10 ± 7%, p = 0.07), whereas non-responders were unchanged. Free androgen index (FAI) in responders was higher (+ 34%, p < 0.05) compared to non-responders at baseline. The maximum strength period decreased testosterone (− 17 ± 12; 17 ± 22%), FAI ratio (− 12 ± 14; − 21 ± 23%) and testosterone/cortisol ratio (− 17 ± 25; − 31 ± 20%) in MS and P-responders, respectively. During the P-period hormonal levels plateaued. To conclude, periodized strength training induced different inter-individual physiological responses, and thus RFD development may vary between individuals. Therefore, RFD seems to be a useful tool for planning and monitoring strength training programs for individual neuromuscular performance needs.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Rapid force production is critical for sport performance and important for normal muscular function. When it is impaired, muscular function is compromised in individuals of various populations; e.g., elderly, patients, or it separates the medalists from non-successful athletes. Interestingly, rapid force production ability seems to be more sensitive to determine acute and chronic adaptations in the neuromuscular system compared to maximal voluntary contraction force (e.g.,, Angelozzi et al. 2012; Crameri et al. 2007; Jenkins et al. 2014; Penailillo et al. 2015). This is one of the reasons why the rate of force development (RFD) has recently become quite popular for characterizing changes in different physiological mechanisms due to strength training programs (Maffiuletti et al. 2016). Typically, RFD is derived from force– or torque–time curves during explosive/rapid isometric contractions, and it is a measure of how fast an individual can develop force.
It is well known that identical strength training programs may cause diverse responses between individuals, and it has been demonstrated that one-repetition maximum (1RM) and muscle cross-sectional area (CSA) increases may differ or even not respond at all in some individuals undergoing training (Ahtiainen et al. 2016). Possibly, these different responses to training may be due to the trainees’ genetic make-up and/or exercise training background. Recent speculations suggest that individual training responses can also vary between different (specific) aspects of neuromuscular performance and muscle morphology, thus training may still improve other outcome variables other than the main measure (Churchward-Venne et al. 2015). From another perspective, different training stimuli could evoke similar chronic training responses between individuals. That is, trainees’ individual physical qualities may benefit from a specific stimulus at a particular moment (in time) depending on his/her previous training adaptations, using such principles of the periodization continuum.
The benefits of the current training stimuli might be observable through acute training session responses at specific points in the training period for targeted exercises. Physical readiness to respond to training and the exercise stimulus might be feasible to evaluate based on exercise-induced fatigue. Previous studies have shown that stronger athletes (Ahtiainen and Häkkinen 2009) obtained greater maximal strength fatigue levels, and power athletes (Häkkinen and Myllylä 1990) obtained greater fatigue levels in fast force production compared to their endurance-trained counterparts. In addition, some physiological indicators reflect acute (e.g., metabolic/lactate) and chronic (e.g., endocrine/basal testosterone and cortisol) adaptations in performance capacity due to long-term, progressive strength training (Busso et al. 1990; Fry et al. 1994). In other words, the same strength training program may optimally stress some of the trainees, but other trainees could be under- or over-trained.
With the above points in mind, the aim of the present study was to investigate individual variation in the improvement of RFD and identify underlying adaptations during both a maximum strength training and a subsequent power training period. Both of these training modes have been shown to activate fast muscle fibers maximally, and to fatigue both the neural system and the phosphocreatine system. These training modes have been shown to enhance RFD at a group level; each program creates different dynamic training stimuli through which (potentially) some individuals respond and some do not. We hypothesized that physiological differences and individual acute responses after identical exercise in different individuals will help to explain divergences between responders and non-responders to such training programs. Consequently, the focused aims of the study were to determine whether (1) the timing of the individual improvements in RFD were related to partly similar training-induced stimuli due to maximum strength and power strength training (responders vs non-responders) and (2) these training modes were sensitive enough to induce specific stimulus (MS vs P responders).
Methods
All subjects received written and verbal descriptions of the study. All risks and benefits were explained to participants and written informed consent was obtained. The University Ethics Committee gave approval for all experimental procedures in the study, which was conducted according to the Declaration of Helsinki.
Subjects
Twenty-four healthy physically active male subjects, but with no regular background in strength training, volunteered to participate in this study. Fourteen subjects were in the training group (age 28 ± 5 years; height 179 ± 5 cm; BMI 25 ± 4) and ten subjects (age 30 ± 4 years; height 178 ± 7 cm; BMI 25 ± 2) completed only the familiarization session and pre- and post-study measurements. This group continuing their normal life during the study acted as non-training controls. The subjects were not allowed to train with endurance exercises more than two times per week during the study. The subjects were instructed to follow the Finnish national nutrition recommendations and avoid smoking.
Strength training
All subjects completed a progressive strength training program for 20 weeks including exercises for all body parts, however, leg exercises (leg press, knee extension and flexion) were performed in every training session in the gym twice per week. All leg exercises were performed always before the other exercises and leg press was the first exercise. The strength training program was periodized to a 10-week maximum strength training period followed by a 10-week power strength training period (with separate maximum strength sessions maintained every fourth session). The overall volume of training loads decreased from the maximal strength period to the power strength period, while the concentric velocity of repetitions was high. Training volume decreased in the final sessions before the laboratory measurements at the end of both training periods, in the form of pre-testing tapering. All subjects followed the same training program under direct supervision and their relative loads were equal. In addition, the study design was double-blinded, because subjects, trainers or researches did not know the subgroup of the training subjects during training or measurements.
Training monitoring
After warm-up, all training subjects performed isometric voluntary bilateral leg extension (Fig. 1) contractions with maximal effort at the beginning of every 7th training session in the gym, matching the laboratory measurement methods. Maximum RFD over the steepest 10 ms and peak force (MVC) were analyzed from the recorded force–time curves at 107° knee joint angle in the isometric leg extension device (University of Jyväskylä, Finland). Ankle joint angle was 90° and back support of the isometric chair was at 110° from horizontal. At least two isometric trials were performed and if the final trial improved more than 5% from the previous trial, then the subject was asked to perform one more trial. The highest values from each monitored session were used in analyses. This was used as a basis to categorize each training individual into maximum strength (MS) or power strength (P) responders (based on the timing of their RFD improvements during the intervention) or into the non-responder group after the completed training intervention.

Isometric training monitoring leg extension device
During these monitored training sessions, the subjects always performed the allocated leg press exercise (M16, David Health Solution Ltd, Finland) before the other exercises. The isometric leg extension test was also repeated after the last leg press set to determine loading-induced fatigue based on changes in RFD and MVC parameters. In addition, volume load [load (kg) × repetitions] of the leg press was calculated, as well as fingertip blood samples were collected before and after the exercise to determine blood lactate concentration (see “Biochemistry measurements”).
Laboratory measurements
Neuromuscular, hematological and performance characteristics were measured in the laboratory before and after 10 and 20 weeks of training. All laboratory measurements were performed following 48 h of rest and at the same time of day (± 1 h) for each time point.
Performance measurements
The subjects were familiarized with the tests 2 weeks before the first testing session to adjust the devices used during testing and determine EMG electrode placements. The isometric leg extensions were performed in the beginning of the laboratory measurements and matching the tests performed in the gym. Dynamic 1RM and power at the load of 50% 1RM repetitions were determined by a leg press device (D210, David Health Solution, Finland) that has been modified to include distance and force sensors. The range of movement began at a knee angle of 60° and 110° hip angle and continued until the legs were fully extended (full extension = 180°) with a belt fixed at the hip. The subjects performed at least two (but no more than five) trials with the load increased after each successful repetition. In addition, in the power tests, the subjects performed at least two trials and if the final power value was more than 5% higher than the previous trial, an additional repetition was performed. The subjects were encouraged to push as fast and hard as possible with correct performance technique during all trials.
In the performance measurements, dynamic (leg press) and isometric force (leg extension), as well as torque (knee extension with electrical stimulation) were sampled at 2000 Hz and raw data were low-pass filtered at 20 Hz offline. Displacement data during dynamic leg press trials were low-pass filtered at 75 Hz.
Electrical stimulation procedures
Unilateral isometric knee extensions at 107° knee joint angle were used to assess voluntary activation level (AL) via the interpolated twitch technique (ITT) on an isometric chair (University of Jyväskylä). Four, galvanically paired, self-adhesive muscle stimulation electrodes (6.98 cm VTrodes, Mettler Electronics Corp, USA) were positioned on the proximal, and middle regions of the quadriceps muscle belly and surface electromyography signals were collected from vastus lateralis (VL) and medialis (VM). The stimulation protocol included increasing constant-current single 1 ms rectangular pulses (Model DS7AH, Digitimer Ltd, UK) until a torque plateau was observed. Based on this stimulation current, 25% was added to ensure supramaximal stimulus intensity. During the plateau of peak force in maximal voluntary isometric trials, the same supramaximal single-pulse stimulus was delivered and then one further pulse 2 s after cessation of contraction to the relaxed muscles for voluntary activation assessment. The stimulation protocol did not stimulate antagonist muscles based on EMG of biceps femoris (BF). The percentage of AL was calculated based on the formula of Bellemare and Bigland-Ritchie (1984); AL% = [1 − (superimposed twitch torque/passive twitch torque)] × 100.
Surface electromyography (EMG)
Bipolar surface Ag/AgCl EMG electrodes (diameter 10 mm, inter-electrode distance 20 mm, common mode rejection ratio > 100 dB, input impedance > 100 MΩ, baseline noise < 1 µV rms; University of Jyväskylä, Finland) were placed on the VL, VM and BF of the right leg after shaving and skin abrasion according to SENIAM guidelines (Hermens et al. 2000). EMG signals were sampled at a 2000 Hz frequency and amplified at a 500 gain with 10–500 Hz bandwidth filtering. Signals were AD converted (Micro1401, Cambridge Electronic Design, UK) in real-time and recorded by Signal software (Version 4.04, Cambridge Electronic Design, UK). During the analysis, EMG signals were band-pass (20–350 Hz) filtered and root mean square (rms) converted for EMG amplitude.
Muscle cross-sectional area
Cross-sectional area (CSA) of VL was assessed by extended-field-of-view ultrasound (B-mode, model SSD-α10, Aloka Co Ltd, Japan) with a linear array probe (10 MHz; 60 mm width), including the extended-field-of-view mode (Ahtiainen et al. 2010). The probe was oriented in the axial plane and moved slowly and continuously from the lateral to medial side of the right thigh along the skin via a marked line avoiding excessive compression of the muscle tissue. Three panoramic images of CSA were taken at 50% femur length from the lateral aspect of the distal diaphysis to the greater trochanter. The panoramic CSA images were composed by an in-built software of the ultrasound device based on adjacent images throughout the movement. The border of VL was tracked manually using Image-J software (version 1.37, National Institute of Health, USA). The mean of the two closest CSA values was taken as the result.
Biochemistry measurements
Venous blood samples (10 ml) for the determination of hormone concentrations in serum were obtained in the morning after 12 h fast and analyzed by a qualified laboratory technician. Collected whole blood samples were centrifuged (Megafuge 1.0 R, Heraus, Germany) at 3500 rpm for 10-min before serum was separated and stored at − 80 °C until analysis. Total testosterone (TT), cortisol (C), sex hormone binding globulin (SHBG) analyses were performed using chemical luminescence techniques (Immulite 2000 XPi, Siemens, Llanberis, UK) with hormone-specific immunoassay kits (Siemens) [analytical sensitivity and assay precision values for TT (0.5 nmol/l, 10.6%), C (5.5 nmol/l, 7.7%) and SHBG (0.2 nmol/l, 7.6%)]. Both TT/C ratio and free androgen index (FAI = 100 × T/SHBG) were calculated based on these results. Concentration of free testosterone (FT) was derived from TT, SHBG and albumin concentration, calculated according to the Vermeulen formula (1999).
To determine blood lactate concentrations during training monitoring, capillary blood samples (20 µl) were taken from the fingertip before and after the leg press exercise into a reaction tube containing an anticoagulant and a hemolyzing agent. These samples were analyzed using a lactate analyzer (Biosen, S-line Lab + EFK, Magdeburg, Germany).
Statistical analyses
Mean and standard deviation (SD) are presented as descriptive statistics. The Shapiro–Wilk test was used to test normality of the data and Levene’s test was used to analyze homogeneity of variance in the data samples. One-way variance analyze with Bonferroni post hoc tests were used to analyze differences between the training response groups at the baseline. Wilcoxon matched-pairs was used to test within-group comparisons due to the low number of subjects in each group. Effect sizes for the mean differences between the subgroups were made by Hedge’s g where < 0.2 is a small effect, 0.2–0.8 is a medium effect and > 0.8 is a large effect. The level of significance was set at p < 0.05. In day-to-day measurements, intraclass correlation coefficient was 0.981 for isometric force production. All statistical analysis was performed with SPSS software (version 24, IBM SPSS Statistics).
Results
RFD over the steepest 10 ms on the leg extension dynamometer was used to categorize subgroups for responders to maximum strength (MS, n = 6) and to power (P, n = 4) training or neither both, as non-responders (non, n = 4). Background anthropometrics were similar between the subgroups, only BMI was lower (p < 0.05) in non (22 ± 2) compared to MS (25 ± 3) and P (29 ± 4).
Rate of force development
RFD from the monitoring sessions (averaged over week 3½ to week 10) during the maximum strength training period increased by + 100 ± 35%, (p < 0.001) in the MS-responders, P-responders increased only by + 11 ± 8% (p < 0.001) and non-responders showed decreases of − 17 ± 11% (p < 0.001) in their RFD during this period. Following the power training period (week 13½ to week 20), RFD of P-responders increased by + 53 ± 27% (p < 0.001) compared to their initial level, while MS-responders maintained their RFD improvements (+ 103 ± 46%, p < 0.001) and the non-responders were unchanged from their initial levels (Fig. 2a, b). RFD of the untrained subjects did not change (+ 4 ± 22%; n.s) during the 20–week intervention, which did not differ from the values of non-responders (Fig. 4). After MVC normalization, RFD improvements in the MS- and P-responders matched those without normalization, but in the non-responders, the RFD responses followed those of P-responders (R2 = 0.66) (Fig. 2c, d).

The changes in a individual RFD (average of two best time points), b RFDs in subgroups, c MVCs in subgroups, and d MVC-normalized RFDs in subgroups during the MS and P training periods
Baseline characteristics
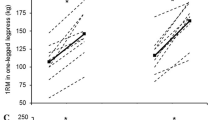
Before the study, leg press 1RM loads were significantly lower (p < 0.05) in the non-responders (149 ± 21 kg) compared to the combined responder groups (MS- 202 ± 20 kg, P-responders 178 ± 23 kg), but the differences in CSA of the VL muscle were not statistically significant before the study (non- 23 ± 4 cm2, MS- 27 ± 7 cm2, P-responders 29 ± 5 cm2). In MS-responders, electrical stimulation-induced resting twitch force (+ 25% vs P-responders; + 47% vs non), twitch force/time ratio (+ 18% vs P-responders; + 45% vs non) and twitch force/CSA ratio (+ 30% vs P-responders; + 26% vs non) were higher compared to other groups. At baseline, the mean FAI ratio of the MS and P groups was significantly higher than that of the non-responder group.
Training-induced changes
Relative changes in 1RM were similar between the groups throughout both training periods, but CSA significantly increased only in the responders (+ 12 ± 8%, p < 0.05) during the maximum strength training period, while non-responders maintained their pre-training CSA. Leg press 1RM was improved during the maximum strength period only, without improvements during the power training period in any subgroups. However, only MS-responders enhanced their EMG (+ 113 ± 76%, p < 0.01) even though their 1RM was unchanged during the power training period (Table 1).
During dynamic explosive leg press movement at a 50% 1RM load from the beginning of the study, the MS-responders improved peak power (+ 35 ± 28%, p < 0.05) during the maximum strength period compared to the other two groups (− 2 ± 15%). The initial EMG of the P-responders decreased (− 22 ± 12%, p = 0.06) during the maximum strength period, but then EMG increased (+ 57 ± 10%, p = 0.077) during power training (+ 35 ± 18% from 0 to 20 weeks, p < 0.01) at the first half of the explosive movement during the power training period. However, already before the power training period, AL in P-responders was higher (+ 5%, p < 0.05) compared to non-responders.
Serum TT (MS − 17 ± 12%, P − 17 ± 22%; p < 0.05) and FT (MS − 11 ± 10%, P − 19 ± 24%; p < 0.05), as well as FAI (MS − 12 ± 14%, P − 21 ± 23%; p < 0.05) and T/C-ratios (MS − 17 ± 25%, P − 31 ± 20%; p < 0.05) were depressed in the responder groups, but not in non-responders during the maximum strength training period only (Table 2).
Exercise-induced fatigue
The maximum strength training leg press exercise (in the gym; averaged weeks 3½ and 7) induced greater acute decrements (p = 0.068) in MVC of MS-responders (− 29 ± 9%) compared to the other groups (P − 17 ± 6%, non − 18 ± 8%) during the maximum strength training period. In addition, at the same time, the averaged RFD of MS-responders decreased (− 31 ± 6%), which differed almost significantly (p = 0.088) compared to the other groups (P − 19 ± 13%, non − 23 ± 11%). However, blood lactate levels in P-responders were elevated (+ 8.8 ± 1.7 mmol/l) significantly more than in non- (+ 5.0 ± 1.3 mmol/l, p < 0.05) or MS-responders (+ 5.5 ± 1.8 mmol/l, p = 0.056) (Fig. 3).

The average volumes of leg press exercises between sessions at weeks 3½ and 7 during the MS period and at weeks 13½ and 17 during the P period. The averaged acute decreases in RFD and MVC in the bottom and the averaged blood lactate levels in the top of the figure after leg press exercises. *p < 0.05, #p = 0.056, ¤p = 0.068
The power training leg press exercise (in the gym; averaged weeks 13½ and 17) induced significantly (p < 0.05) greater acute decrements in MVC productions of responders (MS − 21 ± 5%, P − 20 ± 8%) compared to non-responders (− 13 ± 3%). No significant differences in RFD or blood lactate levels were observed between the groups after leg press exercise during the power training period (Fig. 3).
The effect sizes (Hedges’ g) for the mean differences between responder and non-responder groups in several parameters showed large effects favoring the intervention-induced changes during the maximum strength and power training periods. The RFD improvements of responders were also compared to untrained counterparts (Fig. 4).

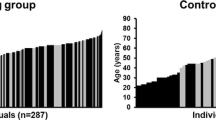
Hedges’ g effect size (95% confidence intervals) for the unadjusted mean differences between individuals without (non-responders) and with RFD response during maximum strength (1–10 weeks, MS-responders) and power (11–20 weeks, P-responders) training periods. In addition, responders RFD responses were compared also to untrained individual RFD responses
Discussion
The present study highlights the individualized improvements in the RFD, even though the strength training protocols were identical in all groups and used the same relative training volumes. Changes in RFD have previously been shown to be closely related to several critical neuromuscular adaptations both peripherally and centrally (Häkkinen et al. 1985; Maffiuletti et al. 2016), and thus, in the present study, RFD was selected as a criterion to categorize subgroups (i.e., responders vs non-responders). This study design was novel, since previous “individual response” studies were based on maximum strength or muscle mass changes during strength training (Erskine et al. 2010; Ahtiainen et al. 2016). In this study, the periodized strength training program was created in an attempt to enhance both maximal strength and rapid force production, because these properties have been previously shown to affect RFD (Andersen et al. 2010). Moreover, it is well known that maximal strength and rapid force production are closely linked (Andersen and Aagaard 2010), and thus, delivered altered/varying stimuli to the same training target. Due to this consideration, the present study was designed to follow this linear periodization continuum from maximum strength to power training.
The initial dynamic 1RM strength and CSA of VL were similar in both MS- and P-responders. It should be noted, however, that baseline maximal strength and muscle size were lower in non-responders. This could be related to lower (p = 0.019) free androgen index (FAI) compared to responders. In all training groups, relative improvements in 1RM were similar throughout the maximum strength training period, although the changes in CSA were minimal in the non-responders compared to MS- and P-responders. Interestingly, basal serum hormonal concentrations such as total testosterone, free testosterone, and testosterone/cortisol and FAI ratios were depressed (p = 0.01–0.03) during the maximum strength period in the responders, but this was not observed in non-responders.
Initially, MS-responders showed the highest resting twitch (RT) force and RT force/time ratio, compared to the other groups before the training intervention. Furthermore, RT force and RT force/time ratio in P-responders increased to the same level as MS-responders throughout the maximum strength period (before their state of being RFD responsive during power training), while non-responders only maintained their levels. However, these observations need more scientific research to confirm these potential causal relationships.
Interestingly, MS-responders had a higher (26–30%) RT force/CSA ratio compared to non- and P-responders. Since MS-responders did not differ in maximal voluntary force production, but differed in involuntary force production, this may indicate that neural deficiencies were specific to initial activation and potentially gave these subjects a greater potential to improve power production from the beginning of the training intervention compared to others. These findings possibly reflect part of the mechanisms behind previous observations that stronger individuals possess more favorable neuromuscular characteristics for superior improvements in maximal power production (Cormie et al. 2010, 2011). Moreover, at the pre-, mid- and post-measurements in the present study, power determination was performed using 50% 1RM from the pre-training loads. Due to the enhanced 1RM during the mid- and post-measurements, these relatively lower loads, possibly required the subjects to improve power via higher contraction velocities. Therefore, it may be assumed that MS-responders possess a better peripheral ‘readiness’ to train as assessed by the above-mentioned ITT test, which might partly explain their enhanced power productions. This suggestion is in-line with the findings of Baker (2001) who concluded that higher power production requires adequate strength qualities before velocity-specific power improvements are established.
The present study is novel by investigating the separate training sessions during the overall training program and using the differences between the acute responses to identify mechanisms for individual adaptations (Foster et al. 2017). Greater training volume loads due to higher absolute training loads might create stronger stimuli for peripheral adaptations (e.g.,, CSA, RT parameters) to reflect alternative demands of the training modes between the non-responder vs the MS- and P-responder groups. Although the overall training program and even absolute volume were the same in MS- and P-responders during the maximum strength training period, physiological stress induced by training may have been optimal for some subjects, while the stimulus may have been either too intense or not sufficiently intense for others, e.g., depending on the training background and/or genetics of the individual. The blood lactate values observed in P-responders after the maximum strength leg press exercise indicated a greater metabolic stress, where the anaerobic glycolytic system was challenged. In some cases, this continued high exertion level might lead to possible states of overreaching or even early level overtraining, which might explain the observed decreasing trend in anabolic hormone levels and testosterone/cortisol and FAI -ratios parallel with a maladapted RFD. It has been suggested that hormonal regulations may be one important factor for trainability (Häkkinen et al. 1985; Kraemer et al. 1990). Therefore, delayed RFD improvement of the P-responders compared to MS responders might be a consequence of their greater training-induced fatigue during every maximum strength training session. In other words, it is possible that maximum strength training induces such a high level of fatigue in these individuals that potential increases in performance are suppressed during the monitoring tests. This premise is support by the work of Hackney et al. who proposed neuroendocrine dysregulation, in particular anabolic hormone suppression, may compromise select exercise training adaptation (Hackney and Lane 2015; Hackney 2006). Thus, power training, with a marked reduction in volume load (decreased to 60%), might have been more suitable for the individuals in the P group to realize training-induced RFD adaptations.
Improvement in RFD has been linked to neural enhancements (Maffiuletti et al. 2016). In the current experiment muscular activity of P-responders at the first 20° joint angles in the 50% 1RM power test reduced (− 22 ± 14%, p = 0.06) after the maximum strength period and recovered (57 ± 10%, p = 0.077) during the power strength training period. This reduction was specific only for explosive power production not for 1RM, which may represent reduced activation of fast motor units with low fatigue resistance capacity as well as reflect a more non-functional fatigue or an overreaching (Meeusen et al. 2013). Along this line, Mujika and Padilla (2003) concluded that the effect of decreased training volume (decreased to 50–70%) for 7–21 days could result in increases in power production, depending on the individual as well as their training programs and backgrounds. Such events might influence a delayed training effect (Zatsiorsky and Kraemer 2006) as observed in the RFD of P-responders (Fig. 2b).
The aforementioned higher initial hormonal levels (Table 2) could also indicate higher tolerance for training, and thus an ability to reach greater power training-induced fatigue and ultimately adaptation (Ryushi et al. 1988). In addition, Ahtiainen and Häkkinen (2009) showed that stronger individuals are capable of producing greater fatigue levels than their weaker counterparts as in non-responders in this study. Alternatively, the observed minor fatigue levels after acute exercise, as well as an unchanged velocity component of power and RFD due to training periods could be a sign of a greater composition of slower muscle fibers in the non-responder individuals. Parallel and perhaps the strongest indirect evidence of this assumption is by the lower responses to muscle stimulation-induced RT parameters. That is, this method primarily activates superficial muscle fibers and thus mainly the fast motor units (Stephens et al. 1978; Garnett and Stephens 1981).
This study was not able to fully explain the origin of lack of adaptation in non-responders to the training stimuli. Individually tailored training programs might create more effective training outcomes and endocrine responses compared to generic training programs. Ahtiainen et al. (2016) showed that 29% of traditional resistance trainees were low-responders with regard to gains in muscle size changes, which is in-line with the number of non-responders (~ 1/3) during the maximum and power strength training segments in the present study. In addition, the data of Haff et al. (2008) showed that 1/3 of their subjects were unable to improve isometric peak RFD; and their testosterone levels were also not positively adaptive in the changes, although these points were not the focus in their study. One limitation of the present study was rather a low number of subjects in each group. It also needs to be noted that the nutritional practices of the subjects were not controlled. However, subjects were instructed to follow national nutrition recommendations, which included guidance on required protein intake for strength training. Furthermore, these nutritional practices were conducted across all the groups, responders and non-responders alike.
Conclusions
Strength training induces differences in physiological responses, and thus force production varied between individuals, which create a need for tailored training programs. Isometric peak RFD seems to be one useful tool to categorize physical deficiencies of trainee before the planning of a periodized strength training program and monitoring training progress between training sessions. Determination of training session-induced acute responses might therefore be helpful in controlling the amount and type of fatigue, which allows more appropriate adaptation.
References
Ahtiainen JP, Häkkinen K (2009) Strength athletes are capable to produce greater muscle activation and neural fatigue during high-intensity resistance exercise than nonathletes. J Strength Cond Res 23(4):1129–1134
Ahtiainen JP, Hoffren M, Hulmi JJ, Pietikäinen M, Mero AA, Avela J, Häkkinen K (2010) Panoramic ultrasonography is a valid method to measure changes in skeletal muscle cross-sectional area. Eur J Appl Physiol 108(2):273–279
Ahtiainen JP, Walker S, Peltonen H, Holviala J, Sillanpää E, Karavirta L, Sallinen J, Mikkola J, Valkeinen H, Mero A, Hulmi JJ (2016) Heterogeneity in resistance training-induced muscle strength and mass responses in men and women of different ages. AGE 38(1):1–3
Andersen JL, Aagaard P (2010) Effects of strength training on muscle fiber types and size; consequences for athletes training for high-intensity sport. Scand J Med Sci Sports 20(Suppl. 2):32–38
Andersen LL, Andersen JL, Zebis MK, Aagaard P (2010) Early and late rate of force development: differential adaptive responses to resistance training? Scand J Med Sci Sports 20:e162–e169
Angelozzi M, Madama M, Corsica C, Calvisi V, Properzi G, McCaw ST, Cacchio A (2012) Rate of force development as an adjunctive outcome measure for return-to-sport decisions after anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther 42:772–780
Baker D (2001) Comparison of upper-body strength and power between professional and college-aged rugby league players. J Strength Cond Res 15(1):30–35
Bellemare F, Bigland-Ritchie B (1984) Assessment of human diaphragm strength and activation using phrenic nerve stimulation. Respir Physiol 58:263–277
Busso T, Häkkinen K, Pakarinen A, Carasso C, Lacour JR, Komi PV, Kauhanen H (1990) A systems model of training responses and its relationship to hormonal responses in elite weight-lifters. Eur J Appl Physiol Occup Physiol 61(1–2):48–54
Churchward-Venne TA, Tieland M, Verdijk LB, Leenders M, Dirks ML, de Groot LC, van Loon LJ (2015) There are no non-responders to resistance-type exercise training in older men and women. J Am Med Dir Assoc 16(5):400–411
Cormie P, McGuigan MR, Newton RU (2010) Influence of strength on magnitude and mechanisms of adaptation to power training. Med Sci Sports Exerc 42(8):1566–1581
Cormie P, McGuigan MR, Newton RU (2011) Developing maximal neuromuscular power: part 2—training considerations for improving maximal power production. Sports Med 41(2):125–146
Crameri RM, Aagaard P, Qvortrup K, Langberg H, Olesen J, Kjaer M (2007) Myofibre damage in human skeletal muscle: effects of electrical stimulation versus voluntary contraction. J Physiol 583:365–380
Erskine RM, Jones DA, Williams AG, Stewart CE, Degens H (2010) Inter-individual variability in the adaptation of human muscle specific tension to progressive resistance training. Eur J Appl Physiol 110:1117
Foster C, Rodriguez-Marroyo JA, de Koning JJ (2017) Monitoring training loads: the past, the present, and the future. Int J Sports Perform 12(S2):2–8
Fry AC, Kraemer WJ, Stone MH, Warren BJ, Fleck SJ, Kearney JT, Gordon SE (1994) Endocrine responses to overreaching before and after 1 year of weightlifting. Can J Appl Physiol 19(4):400–410
Garnett R, Stephens JA (1981) Changes in the recruitment threshold of motor units produced by cutaneous stimulation in man. J Physiol 311:463–473
Hackney AC (2006) Stress and the neuroendocrine system: the role of exercise as a stressor and modifier of stress. Expert Rev Endocrinol Metab 1(6):783–792
Hackney AC, Lane AR (2015) Exercise and the regulation of endocrine hormones. Prog Mol Biol Transl Sci 135:293–311
Haff GG, Jackson JR, Kawamori N, Carlock JM, Hartman MJ, Kilgore JL, Morris RT, Ramsey MW, Sands WA, Stone MH (2008) Force-time curve characteristics and hormonal alterations during an eleven-week training period in elite women weightlifters. J Strength Cond Res 22(2):433–446
Häkkinen K, Myllylä E (1990) Acute effects of muscle fatigue and recovery on force production and relaxation in endurance, power and strength athletes. J Sports Med 30(1):5–12
Häkkinen K, Pakarinen A, Alén M, Komi PV (1985) Serum hormones during prolonged training of neuromuscular performance. Eur J Appl Physiol Occup Physiol 53(4):287–293
Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10(5):361–374
Jenkins ND, Housh TJ, Traylor DA, Cochrane KC, Bergstrom HC, Lewis RW, Schmidt RJ, Johnson GO, Cramer JT (2014) The rate of torque development: a unique, non-invasive indicator of eccentric-induced muscle damage? Int J Sports Med 35:1190–1195
Kraemer WJ, Marchitelli L, Gordon SE, Harman E, Dziados JE, Mello R, Frykman P, McCurry D, Fleck SJ (1990) Hormonal and growth factor responses to heavy resistance exercise protocols. J Appl Physiol 69(4):1442–1450
Maffiuletti NA, Aagaard P, Blazevich AJ, Folland J, Tillin N, Duchateau J (2016) Rate of force development: physiological and methodological considerations. Eur J Appl Physiol 116(6):1091–1116
Meeusen R, Duclos M, Foster C, Fry A, Gleeson M, Nieman D, Raglin J, Rietjens G, Steinacker J, Urhausen A (2013) Prevention, diagnosis, and treatment of the overtraining syndrome: joint consensus statement of the European College of Sport Science and the American College of Sports Medicine. Med Sci Sports Exerc 45(1):186–205
Mujika I, Padilla S (2003) Scientific bases for precompetition tapering strategies. Med Sci Sports Exerc 35(7):1182–1187
Penailillo L, Blazevich A, Numazawa H, Nosaka K (2015) Rate of force development as a measure of muscle damage. Scand J Med Sci Sports 25:417–427
Ryushi T, Hakkinen K, Kauhanen H, Komi PV (1988) Muscle fiber characteristics, muscle cross-sectional area and force production in strength athletes, physically active males and females. Scand J Sports Sci 10(1):7–15
Stephens JA, Garnett R, Bulli NP (1978) Reversal of recruitment order of single motor units produced by cutaneous stimulation during voluntary muscle contraction in man. Nature 272:362–364
Vermeulen A, Verdonck L, Kaufman JM (1999) A critical evaluation of simple methods for the estimation of free testosterone in serum. J Clin Endocrinol Metab 84:3666–3672
Zatsiorsky VM, Kraemer WJ (2006) Science and practice of strength training. Hum Kinet
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by William J. Kraemer.
Rights and permissions
About this article

Cite this article
Peltonen, H., Walker, S., Hackney, A.C. et al. Increased rate of force development during periodized maximum strength and power training is highly individual. Eur J Appl Physiol 118, 1033–1042 (2018). https://doi.org/10.1007/s00421-018-3836-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-018-3836-9