
Abstract
Purpose
It has been suggested that flexibility training may reduce the total volume of training during resistance trainings. The purpose of this study was to compare the effect of flexibility training immediately before resistance training (FLEX-RT) versus resistance training without flexibility training (RT) on maximum strength and the vastus lateralis muscle cross-sectional area (CSA).
Methods
Participants had each leg assigned to RT or FLEX-RT. Both groups performed four sets of leg extensions to voluntary failure of 80% of one repetition maximum (1RM); however, FLEX-RT performed two sets of 25 s of static stretching before resistance training. Number of repetitions and total volume were calculated during weeks 1–5 and 6–10. Vastus lateralis muscle CSA, 1RM, and flexibility were assessed at baseline and after 10 weeks.
Results
The number of repetitions and total training volume were greater for RT than FLEX-RT for weeks 1–5 and 6–10. Regarding the vastus lateralis muscle CSA, a main time effect was observed, however, greater change was observed for RT than FLEX-RT (12.7 and 7.4%, respectively). A main time effect for 1RM was also observed with similar changes for RT and FLEX-RT (12.7 and 12.9%, respectively). Flexibility was increased pre- to post-training for FLEX-RT with greater change for FLEX-RT (10.1%) than RT (2.1%).
Conclusion
These results show that performing flexibility training immediately before resistance training can contribute to a lower number of repetitions, total volume, and muscle hypertrophy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Performed by athletes and non-athletes, flexibility training allows for improving joint range of motion (Behm et al. 2016; Garber et al. 2011). It has been shown that flexibility training also may attenuate indirect markers of muscle damage before eccentric exercise (Chen et al. 2015, 2011), as well as improve postural stability and balance (Costa et al. 2009). Despite these benefits, it has been suggested that flexibility training performed prior to resistance exercise may reduce important neuromuscular adaptations, such as maximum strength and muscle hypertrophy (Barroso et al. 2012).
The negative interference of flexibility training on muscle strength and muscle hypertrophy may be related to a decrease in the number of repetitions (Barroso et al. 2012; Franco et al. 2008; Gomes et al. 2011; Nelson et al. 2005) and the total training volume of resistance training (Barroso et al. 2012). Nelson et al. (2005) showed a decrease of 24% in the number of repetitions when resistance exercise until concentric failure (60% 1RM) was performed after static stretching. Likewise, Barroso et al. (2012) observed that when stretching exercises (proprioceptive neuromuscular facilitation, static and ballistic stretching) are performed prior to resistance training session (80% 1RM, until concentric failure) there is a reduction in the number of repetitions as well as total training volume (18 and 23%, respectively). Additionally, it has been suggested that low total training volume of resistance training may be associated with less improvement in the maximum strength and hypertrophy compared to higher total training volume (Krieger 2009, 2010; Schoenfeld et al. 2016).
Contradictory results were observed in two studies investigating the influence of flexibility training performed before resistance training in women (Leite et al. 2015; Simao et al. 2011). Simao et al. (2011) showed that after 16 weeks of intervention in untrained women, flexibility training before resistance training did not affect the 10RM test compared to resistance training without stretching. However, Leite et al. (2015) observed a lower improvement magnitude in the 10RM test for flexibility training performed before resistance training compared to resistance training without stretching in trained women. Additionally, with respect to the divergent responses, both studies did not investigate the effect of these protocols on maximum strength and muscle hypertrophy.
Therefore, this study aimed to compare the effect of flexibility training performed immediately before resistance training (FLEX-RT) versus resistance training without flexibility training (RT) on muscle hypertrophy, maximum strength, and flexibility. Our hypothesis is that RT will promote greater improvement in strength and hypertrophy compared with FLEX-RT, while FLEX-RT will promote greater improvement in flexibility compared to RT.
Methods
Participants
Nine healthy males (age 25.4 ± 5.3 years, weight 76.3 ± 6.3 kg, height 176 ± 6.1 cm, body mass index 24.6 ± 2.4 kg/m2) volunteered to participate in this study. Participants were not engaged in any sports activities and resistance and/or endurance training at least 6 months prior to the study, and were free of any musculoskeletal disorders. All participants were informed about the potential risks involved and gave their written consent before participation. The investigation was carried out in accordance with all ethical standards for research involving human participants set by the Declaration of Helsinki and was approved by Ethics and Research Committee of the local university.
Experimental procedures
Prior to the experimental (pre-control) period, the vastus lateralis muscle cross-sectional area (CSA) was assessed by mode-b ultrasound and flexibility was assessed by a goniometer for each leg of the participants. Afterward, two familiarisation sessions (with 2 days’ interval between them) were conducted that consisted of three sets of ten repetitions with a submaximal load in the unilateral leg extension machine. Additionally, the positions of each participant in the exercise (e.g. position of the feet, backrest, and range of motion) were noted. Two days after the familiarisation session, using the same exercise (unilateral leg extension machine) participants performed the maximum dynamics strength test by one repetition maximum (1RM) for each leg. After 72 h, the 1RM test was repeated to determine test–retest reliability. After the pre-control period, the participants remained in the control period for 10 weeks (i.e., no exercise was undertaken). The control period was realised to obtain the measures of reliability (vastus lateralis muscle CSA, flexibility, and 1RM). Ten weeks later (post-control period), the participants performed the assessments for each leg: vastus lateralis muscle CSA, flexibility, and 1RM (1RM was performed only once because the participants were familiar with the test; 1RM was performed 24 h after flexibility assessment). Posteriorly, each leg of the participants was randomly assigned to resistance training without flexibility (RT) and flexibility training before resistance training (FLEX-RT) (the values after the control period were used as pre-training ones). The randomisation of each leg to the training protocols was brought about to reduce inter-subject variability. Participants completed 10 weeks of training (two weekly sessions, with 48 h rest). After 5 weeks, the 1RM test was assessed to adjust training load. Seventy-two hours after the last training session, vastus lateralis muscle CSA, flexibility, and 1RM were assessed (1RM was performed 24 h after the flexibility assessment).
Vastus lateralis muscle cross-sectional area
The vastus lateralis muscle CSA for each leg was assessed using mode-B ultrasound with a 7.5 MHz linear array probe (Nanomaxx, Sonosite, Bothell, USA) according to Lixandrao et al. (2014). Briefly, the participants laid in supine position with their muscles as relaxed as possible for 20 min. Afterwards, measurements were collected at the midpoint between the lateral epicondyle and greater trochanter of the femur. At this point, the skin was transversally marked every 2 cm from the reference point toward the medial and lateral aspects of the thigh to orient probe displacement. Additionally, water-based conductive gel was used to avoid pressure on the muscle tissue. Sequential ultrasound images were acquired and posteriorly were reconstructed and manually rotated until the whole vastus lateralis cross-section was reconstructed. Then, the vastus lateralis muscle CSA was measured using computerised planimetry (i.e., the vastus lateralis muscle CSA was contoured following the muscle fascia using an 800 dpi mouse) (Madena 3.2.5, EyePhysics, Los Paladinos, USA). The images were collected and analysed by an experienced investigator. The investigator realised the analysis in a blind way.
Maximum dynamic strength
Maximum dynamic strength for each leg was tested by the 1RM test in the unilateral leg extension machine (Matrix, São Paulo, Brazil), according to Brown and Weir (2001). Briefly, the participants performed a general warm-up on a cycle ergometer at 60 rpm and 25 W for 5 min. Then, a specific warm-up was performed consisting of two sets. During the first set, the subjects performed eight repetitions with 50% of the estimated 1RM obtained during the familiarisation sessions; 1 min later, the second set was performed with three repetitions to 70% of the estimated 1RM. After a 3 min interval, the 1RM test was performed in five trials with 3 min rest between them, and with the aim of obtaining the maximum amount of weight (kg) in a complete cycle (flexion–extension of the knee joint with total range of motion of 90°). Strong verbal encouragement was provided during all attempts.
Flexibility assessment
Unilateral flexibility was assessed for each leg according to Monteiro et al. (2008). A flexometer (Sanny, São Bernardo do Campo, Brazil) was fixed at the ankle by an elastic belt. The participants remained standing with both thighs leaning against a support to avoid anteroposterior movement of the thigh. After, the participants were instructed to support their body weight on the contralateral leg to be assessed, with both knees and hips completely extended. Then, the participants performed knee flexions with the highest range of motion possible in three attempts with a 30 s rest. The higher range of motion achieved was considered for analysis.
Training protocols
Training protocols were performed twice a week for 10 weeks (a total of 20 sessions). Each one of the participants’ legs was randomly assigned to resistance training without flexibility (RT) and flexibility training before resistance training (FLEX-RT). In addition, the order of execution of the protocols (i.e. FLEX-RT and RT) during the training period was alternated. Thus, in each training session, the participant started with a different leg.
The RT group performed four sets of unilateral leg extensions (Matrix, São Paulo, Brazil) to a voluntary failure of 80% 1RM, with a 90 s rest between sets. The contralateral leg (FLEX-RT) performed flexibility training and immediately after (i.e. after 30 s), it performed the same RT protocol. The flexibility training (FLEX-RT) consisted of two 25 s sets of static stretching with 60 s of rest between sets. The participants were placed in the prone position and both the knee flexion and hip extension were performed passively by an experienced instructor. A visual analogue pain scale from 0 to 10, where 0 represents ‘no pain’ and 10 represents ‘maximal pain’, was used to monitor flexibility training. When the participant indicated values between 8 and 10 on the visual analogue pain scale, this position was maintained for 25 s.
Statistical analysis
Initially, data normality (Shapiro–Wilk test) and equality of variance (Levene test) were assessed. After being randomly assigned to the RT and FLEX-RT groups, paired t tests were performed to verify pre-training differences between groups for all dependent variables. Additionally, paired t test for weeks 1–5 and 6–10 were performed to compare total volumes between RT and FLEX-RT. After 10 weeks’ intervention, two-way repeated measures ANOVA was performed for each dependent variable to verify differences between times (pre- and post-training) and groups (RT and FLEX-RT). When a significant F value was obtained, a Tukey post hoc test was performed. P values <0.05 were considered to be significant. Additionally, different percentage values between RT and FLEX-RT were compared by paired t tests for all dependent variables. The effect size (ES) magnitude (the difference between pre-training and post-training values divided by the baseline SD) for vastus lateralis muscle CSA, maximum dynamic strength, and flexibility assessment was also determined. An ES lower than 0.3 was considered as ‘small’, between 0.3 and 0.8 as ‘moderate’ and greater than 0.8 as ‘large’. Finally, typical error and coefficient of variation (Hopkins 2000) of the control period for vastus lateralis muscle CSA, maximum dynamic strength and flexibility assessment of each groups were also evaluated. Data are presented as mean ± standard deviation (SD).
Results
Mean number of repetitions and total training volume
FLEX-RT negatively affected the mean number of repetitions, as well as mean total training volume (kg × repetitions) when compared to RT (Table 1). During weeks 1–5, the RT group performed a higher mean number of repetitions (17.8%) than FLEX-RT (P = 0.001), and also had higher mean total training volume (20.9%) than FLEX-RT (P = 0.001). Similar results were observed during weeks 6–10. RT performed a higher mean number of repetitions (15.3%) than FLEX-RT (P = 0.001) and also had a higher mean total training volume (18.7%) than FLEX-RT (P = 0.001).
Vastus lateralis muscle CSA
One participant did not carry out the assessment of the vastus lateralis muscle CSA due to personal problems; thus, only for vastus lateralis muscle CSA, eight participants, not nine participants, were assessed. At baseline, no between-group difference was found in vastus lateralis muscle CSA (P = 0.608). After 10 weeks of training, no interaction time × group was observed for vastus lateralis muscle CSA (P = 0.075), however, a main time effect (P = 0.001) in which the post-training values were greater than the pre-training values (Fig. 1) was observed. The values ranged from 25.8 ± 2.7 to 29.4 ± 2.7 for the RT group and from 25.1 ± 2.7 to 27.1 ± 2.5 for the FLEX-RT group from pre- to post-training, respectively. However, a percentage difference was observed between RT and FLEX-RT (P = 0.038; RT = 12.7 ± 7.2 and FLEX-RT = 7.4 ± 3.7). ES analysis showed a large improvement for RT (ES = 1.17), and only a moderate improvement for FLEX-RT (ES = 0.75).

Pre- and post-training vastus lateralis muscle cross-sectional area (CSA) for the resistance training without flexibility (RT) and flexibility training before resistance training (FLEX-RT). Inset delta percentage (pre to post-training) of each group. Data are presented as mean ± SD. †Main time effect, post-training greater than pre-training (P < 0.05). *Significant difference between RT and FLEX-RT (P < 0.05)
Maximum dynamic strength
At baseline, no between-group difference was found in maximum dynamic strength (P = 0.701). After 10 weeks of training, no interaction time × group was detected for 1RM (P = 0.956), however, a main time effect (P = 0.001) in which the post-training values were greater than the pre-training values (Fig. 2) was observed. The values ranged from 30.2 ± 4.1 to 34.1 ± 3.7 for the RT group and from 29.5 ± 3.6 to 33.2 ± 3.1 for the FLEX-RT group from pre- to post-training, respectively. There was no percentage difference between RT and RT-FLEX (P = 0.371; RT = 12.7 ± 7.4 and FLEX-RT = 12.9 ± 8.1). ES analysis showed a large improvement for RT and FLEX-RT (ES = 0.90 and 0.96, respectively).

Pre- and post-training one repetition maximum (1RM) for the resistance training without flexibility (RT) and flexibility training before resistance training (FLEX-RT). Inset delta percentage (pre to post-training) of each group. Data are presented as mean ± SD. †Main time effect, post-training greater than pre-training (P < 0.05)
Flexibility assessment
At baseline, no between-group difference was found in the flexibility assessment (P = 0.548). After 10 weeks of training, interaction time × group was observed for 1RM (P = 0.002). There was no significant difference for RT (P = 0.818; 128.3 ± 11.8 to 130.6 ± 9.5, pre- and post-training respectively), however, a significant increase for the FLEX-RT group (P = 0.009; 124.3 ± 9.7 to 136.7 ± 9.8, pre- and post-training, respectively) was noted. Additionally, percentage differences between RT and FLEX-RT (P = 0.001; RT = 2.1 ± 6.5 and FLEX-RT = 10.1 ± 5.8) (Fig. 3) were observed. ES analysis showed a small improvement for RT (ES = 0.19), and a large improvement for FLEX-RT (ES = 1.27).

Pre- and post-training flexibility for the resistance training without flexibility (RT) and flexibility training before resistance training (FLEX-RT). Inset delta percentage (pre to post-training) of each group. Data are presented as mean ± SD. †Significant within-group differences for the FLEX-RT (pre to post-training) (P < 0.05). *Significant difference between RT and FLEX-RT (P < 0.05)
Individual response
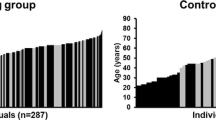
Figure 4 shows the individual response for the vastus lateralis muscle CSA (A), 1RM (B) and flexibility (C). For the vastus lateralis CSA, it was observed that seven of the eight participants assessed (one participant was not assessed) had a larger increase in RT than FLEX-RT, while for the 1RM, four participants had larger increase when they performed RT, and five participants did when they performed FLEX-RT. All participants had a greater increase in flexibility for FLEX-RT than RT.

Individual response to: a vastus lateralis muscle cross-section area (n = 8), b one repetition maximum (n = 9) and c flexibility (n = 9)
Typical error and coefficient of variation
Typical error and coefficient of variation between the pre- and post-control period were 1.1 cm2 and 4.3% for vastus lateralis CSA, 2.0 kg and 6.5% for 1RM and 9.9° and 7.7% for flexibility in RT, respectively. In the FLEX-RT, typical error and coefficient of variation were 0.5 cm2 and 2.7% for vastus lateralis CSA, 2.1 kg and 7.7% for 1RM and 5.8° and 4.6% for flexibility, respectively.
Discussion
The aim of the present study was to compare the effect of flexibility training performed immediately before resistance training versus resistance training without stretching. Our main findings are: (1) RT promoted greater increases in vastus lateralis muscle CSA than FLEX-RT, (2) RT and FLEX-RT were equally effective in increasing 1RM and, (3) FLEX-RT promoted greater increases in flexibility than RT.
Regarding the improvements in muscle hypertrophy, our data showed greater improvement for the RT (12.7%) compared FLEX-RT (7.2%) (Fig. 1). ES also confirmed this result, as large improvements in RT (ES = 1.17) and moderate improvements in FLEX-RT (ES = 0.75) were observed. At last, it is also interesting to note that seven out of eight people had leg muscle hypertrophy when they performed RT rather than FLEX-RT (individual responses, Fig. 4a). This finding may be explained by the number of repetitions and the total training volume, both of which were significantly higher in RT than FLEX-RT. A decrease of 17.8 and 15.3% in the number of repetition (weeks 1–5 and 6–10, respectively) and of 20.9 and 18.7% in total volume (weeks 1–5 and 6–10, respectively) were observed in FLEX-RT compared to RT. Other studies have also observed decreases in the number of repetitions and total training volume when flexibility training was performed before resistance exercise (Barroso et al. 2012; Franco et al. 2008; Gomes et al. 2011; Nelson et al. 2005). Similar to the results of our study, Barroso et al. (2012) observed a decrease in the number of repetitions (21%) and total training volume (22%) after flexibility training (3 sets of 30 s). This result confirms that flexibility training interferes with resistance training, by decreasing the number of repetitions and total training volume. The decrease mainly of the total training volume may attenuate muscle hypertrophy. In a recent meta-analysis, Schoenfeld et al. (2016) showed a dose–response between increases in the weekly volume of the RT group and greater gains in muscle hypertrophy. Thus, our results are in accordance with the literature as RT promoted high total volume and hence greater muscle hypertrophy than FLEX-RT. However, we suggest that the decrease in the number of repetitions and in the total training volume can be avoided. In our study, the resistance exercise was performed 30 s after flexibility training. A recent study showed that the maximal isometric torque was restored 10 min after flexibility training (Mizuno et al. 2014). Although the maximal isometric torque has been assessed, we hypothesise that a longer rest period between flexibility training and RT does not affect the number of repetitions and total training volume. Thus, future studies should investigate the appropriate rest (e.g. 5 or 10 min) between flexibility training and RT on muscle hypertrophy.
Although a greater improvement in vastus lateralis muscle CSA for the RT group compared to FLEX-RT was noted, both groups increased similarly the 1RM (12.7 and 12.9%, respectively) (Fig. 2). In addition, ES analysis showed large improvements in both training protocols (ES = 0.90 and 0.96 for RT and FLEX-RT, respectively). Individual response analysis showed that four legs had a greater increase in 1RM when they performed RT, while the other five had a greater increase when they performed FLEX-RT (Fig. 4b). Although, the same result has been shown in other studies, (i.e. differences between groups regarding muscle hypertrophy, but with similar strength gains) (Küüsmaa et al. 2016; Lixandrao et al. 2015; Vikne et al. 2006), this similar improvement in 1RM between groups was surprising. Quadriceps muscle CSA is associated with maximum strength (de Souza et al. 2012; Izquierdo et al. 2004). In addition, high total volume is related to greater improvements in the maximum strength compared with low total volume (Krieger 2009). However, it is important to note that quadriceps muscle CSA explains approximately only 38% of maximum strength (de Souza et al. 2012; Izquierdo et al. 2004). Thus, 62% of muscle strength is influenced by other factors(e.g. neural factors) (Duchateau et al. 2006; Sale 1988). We also suggest that a cross-education effect (i.e. strength training of one limb and increased strength of the contralateral limb) might have affected the results of the muscle strength. In a meta-analysis, Munn et al. (2004) showed an increase of 7.8% in muscle strength in the contralateral limb. Therefore, future studies should investigate groups that perform bilateral exercise models (i.e. FLEX-RT or RT).
Our study also observed a greater increase in flexibility for the FLEX-RT group (10.1%) compared with RT one (2.1%) (Fig. 3). In addition, ES analysis showed large improvement for FLEX-RT (ES = 1.27) and small improvement for RT (ES = 0.19). All legs that performed FLEX-RT had greater flexibility compared with performing RT (Fig. 4c). These results are contradictory to the findings of Leite et al. (2015) and Simao et al. (2011). Both studies observed that resistance training was as effective as flexibility training to increase the sit-and-reach test (Leite et al. 2015; Simao et al. 2011). The exact reason for the different responses among the studies is not clear, however, we speculate that different samples and protocols of training (flexibility training and resistance exercise) may have influenced them. Furthermore, it is important to highlight that both studies mentioned above used the sit-and-reach test to evaluate flexibility, while in the present study we used the range of motion of the knee joint by flexometer.
Finally, it is important to note some limitations. First, although it is valid to assess the vastus lateralis muscle CSA (Lixandrao et al. 2014), ultrasound does not reflect the change in the overall muscle volume. Second, to minimise inter-subject variability, each participant performed both exercise protocols (i.e. RT on one leg and FLEX-RT on the other leg). However, this fact may have contributed to a cross-education effect and thus may have influenced the results of muscle strength. Third, the results of this study must be limited only young resistance-untrained men and cannot be generalised to other populations (e.g. women, the elderly, or those with resistance training experience).
Conclusion
Based on the findings of the present study, it is possible to conclude that performing FLEX-RT attenuates muscle hypertrophy compared to resistance training; however, FLEX-RT did not affect muscle strength and contributed to an increase in flexibility. Thus, if muscle hypertrophy is the main objective, flexibility training immediately before resistance training should not be performed.
Abbreviations
- ANOVA:
-
Analysis of variance
- CSA:
-
Cross-sectional area
- FLEX-RT:
-
Flexibility training immediately before of the resistance training
- RT:
-
Resistance training without flexibility training
- 1RM:
-
One repetition maximum
References
Barroso R, Tricoli V, Santos Gil SD, Ugrinowitsch C, Roschel H (2012) Maximal strength, number of repetitions, and total volume are differently affected by static-, ballistic-, and proprioceptive neuromuscular facilitation stretching. J Strength Cond Res 26:2432–2437
Behm DG, Blazevich AJ, Kay AD, McHugh M (2016) Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review. Appl Physiol Nutr Metab 41:1–11
Brown LE, Weir JP (2001) Procedures recommendation I: accurate assessment of muscular strength and power. J Exerc Physiol 4:1–21
Chen CH, Nosaka K, Chen HL, Lin MJ, Tseng KW, Chen TC (2011) Effects of flexibility training on eccentric exercise-induced muscle damage. Med Sci Sports Exerc 43:491–500
Chen CH, Chen TC, Jan MH, Lin JJ (2015) Acute effects of static active or dynamic active stretching on eccentric-exercise-induced hamstring muscle damage. Int J Sports Physiol Perform 10:346–352
Costa PB, Graves BS, Whitehurst M, Jacobs PL (2009) The acute effects of different durations of static stretching on dynamic balance performance. J Strength Cond Res 23:141–147
de Souza EO et al (2012) Multivariate analysis in the maximum strength performance. Int J Sports Med 33:970–974
Duchateau J, Semmler JG, Enoka RM (2006) Training adaptations in the behavior of human motor units. J Appl Physiol 101:1766–1775
Franco BL, Signorelli GR, Trajano GS, de Oliveira CG (2008) Acute effects of different stretching exercises on muscular endurance. J Strength Cond Res 22:1832–1837
Garber CE et al (2011) American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 43:1334–1359
Gomes TM, Simao R, Marques MC, Costa PB, da Silva Novaes J (2011) Acute effects of two different stretching methods on local muscular endurance performance. J Strength Cond Res 25:745–752
Hopkins WG (2000) Measures of reliability in sports medicine and science. Sports Med 30:1–15
Izquierdo M, Ibanez J, Hakkinen K, Kraemer WJ, Ruesta M, Gorostiaga EM (2004) Maximal strength and power, muscle mass, endurance and serum hormones in weightlifters and road cyclists. J Sports Sci 22:465–478
Krieger JW (2009) Single versus multiple sets of resistance exercise: a meta-regression. J Strength Cond Res 23:1890–1901
Krieger JW (2010) Single vs. multiple sets of resistance exercise for muscle hypertrophy: a meta-analysis. J Strength Cond Res 24:1150–1159
Küüsmaa M, Schumann M, Sedliak M, Kraemer WJ, Newton RU, Malinen JP, Nyman K, Häkkinen A, Häkkinen K (2016) Effects of morning vs. evening combined strength and endurance training on physical performance, muscle hypertrophy and serum hormone concentrations. Appl Physiol Nutr Metab 41:1285–1294
Leite T, de Souza Teixeira A, Saavedra F, Leite RD, Rhea MR, Simao R (2015) Influence of strength and flexibility training, combined or isolated, on strength and flexibility gains. J Strength Cond Res 29:1083–1088
Lixandrao ME et al (2014) Vastus lateralis muscle cross-sectional area ultrasonography validity for image fitting in humans. J Strength Cond Res 28:3293–3297
Lixandrao ME et al (2015) Effects of exercise intensity and occlusion pressure after 12 weeks of resistance training with blood-flow restriction. J Strength Cond Res 115:2471–2480
Mizuno T, Matsumoto M, Umemura Y (2014) Stretching-induced deficit of maximal isometric torque is restored within 10 min. Stretching-induced deficit of maximal isometric torque is restored within 10 min. J Strength Cond Res 28:147–153
Monteiro WD, Simao R, Polito MD, Santana CA, Chaves RB, Bezerra E, Fleck SJ (2008) Influence of strength training on adult women’s flexibility. J Strength Cond Res 22:672–677
Munn J, Herbert RD, Gandevia SC (2004) Contralateral effects of unilateral resistance training: a meta-analysis J Appl Physiol 96:1861–1866
Nelson AG, Kokkonen J, Arnall DA (2005) Acute muscle stretching inhibits muscle strength endurance performance. J Strength Cond Res 19:338–343
Sale DG (1988) Neural adaptation to resistance training. Med Sci Sports Exerc 20:S135–S145
Schoenfeld BJ, Ogborn D, Krieger JW (2016) Dose–response relationship between weekly resistance training volume and increases in muscle mass: a systematic review and meta-analysis. J Sports Sci 19:1–10
Simao R, Lemos A, Salles B, Leite T, Oliveira E, Rhea M, Reis VM (2011) The influence of strength, flexibility, and simultaneous training on flexibility and strength gains. J Strength Cond Res 25:1333–1338
Vikne H, Refsnes PE, Ekmark M, Medbo JI, Gundersen V, Gundersen K (2006) Muscular performance after concentric and eccentric exercise in trained men. Med Sci Sports Exerc 38:1770–1781
Acknowledgements
The authors are grateful to National Council for Scientific and Technological Development (CNPq) for the financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Communicated by Toshio Moritani.
Rights and permissions
About this article

Cite this article
Junior, R.M., Berton, R., de Souza, T.M.F. et al. Effect of the flexibility training performed immediately before resistance training on muscle hypertrophy, maximum strength and flexibility. Eur J Appl Physiol 117, 767–774 (2017). https://doi.org/10.1007/s00421-016-3527-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-016-3527-3