
Abstract
Purpose
A decline in physical capacity takes place with increasing age that negatively affects overall physical function including work ability and the ability to perform typical activities of daily living (ADL). The overall aim of the present study was to determine the neuromuscular adaptations to long-term (1 year) football and strength training in older untrained adults, and to assess the concurrent effect on functional ADL capacity.
Methods
Twenty-seven healthy elderly males (68.2 ± 3.2 years) were randomly assigned to 12 months of either recreational football training (FT: n = 10), strength training (ST: n = 9) or served as inactive controls (CON: n = 8). Recreational football training consisted of small-sided training sessions whereas strength training consisted of high intensity exercises targeting the lower extremity and upper body. Maximal thigh muscle strength and rate of force development (RFD) were assessed with isokinetic dynamometry, while postural balance and vertical jumping performance were evaluated using force plate analysis. Furthermore, functional ability was evaluated by stair-ascent and chair-rising testing.
Results
A total of nine, nine and seven participants from FT, ST and CON, respectively, were included in the analysis. Both exercise regimens led to substantial gains in functional ability, evidenced by 24 and 18 % reduced stair-ascent time, and 32 and 21 % increased chair-rising performance in FT and ST, respectively (all P < 0.05). Long-term strength training led to increased concentric (14 %; P < 0.01) and isometric (23 %; P < 0.001) quadriceps and isometric hamstring strength (44 %; P < 0.0001), whereas football training mainly resulted in enhanced hamstring strength (18 %, P < 0.05) and RFD (89 %, P < 0.0001).
Conclusions
Long-term (1 year) strength training led to increased quadriceps and hamstring strength, whereas the adaptations to football training mainly included enhanced strength and rapid force capacity of the hamstring muscles. Gains in functional ability were observed in response to both training regimens, evidenced by reduced stair-ascent time and increased chair-rising performance. Long-term football exercise and strength training both appear to be effective interventional strategies to improve factors of importance for ADL by counteracting the age-related decline in lower limb strength and functional capacity among old male adults. This could potentially be a way to improve work ability of senior workers.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
With increasing age, a decline in physical capacity takes place consequently affecting overall physical function including the ability to perform typical activities of daily living (ADL) (Christensen et al. 2006; Larsen et al. 2008). The progressive reductions in muscle performance, bone mass, cardiorespiratory fitness, along with degenerative alterations in neural function accompanied by aging brings ADL tasks like rising from a chair and climbing stairs, closer to the limit of maximal performance (Larsen et al. 2008). These impairments may eventually lead to loss of functional autonomy, disability and reduced independence (Johannsen et al. 2008). Additionally, aging is associated with a declining level of physical activity where older inactive adults are at greater risk for mortality compared to those who are physically active (Bijnen et al. 1998; Blair et al. 1989; Johannsen et al. 2008; Westerterp and Meijer 2001). Thus, it seems of vital importance to implement physical activity that can preserve factors of importance for ADL by counteracting the age-related decline in physical capacity and consequently improving the quality of life in the elderly.
Numerous activities of daily living in the elderly population, such as walking, stair-climbing and regaining balance in situations of sudden postural perturbation require the ability of the neuromuscular system to exert high contractile rate of force development (RFD) (Aagaard et al. 2010, 2002; Bassey et al. 1992; Fleming et al. 1991). Rapid force capacity (i.e. RFD) is especially compromised by aging (Häkkinen et al. 1995; Izquierdo et al. 1999; Klass et al. 2008) and this progressive decline has been associated with impaired neuromuscular response in controlling postural balance (Izquierdo et al. 1999). Additionally, elderly people with reduced knee extensor muscle strength and accompanied depressed RFD show an impaired ability to avoid tripping over unexpected obstacles during level walking (Pijnappels et al. 2008), suggesting that, increasing strength and rapid force capacity may prevent the risk of falling. Heavy resistance strength training seems to be an effective countermeasure to the age-related deterioration in physical capacity by inducing muscle growth and evoking substantial changes in neuromuscular function (Aagaard et al. 2010; Caserotti et al. 2008a; Seynnes et al. 2004; Suetta et al. 2004). Seynnes et al. (2004) found that 10 weeks of high intensity strength training (80 % of 1RM) for the knee extensors elicited increased strength, muscular endurance and chair-rising time in frail elders compared with low intensity strength training (40 % of 1RM) (Seynnes et al. 2004). In line with this, Caserotti et al. (2008a) showed that 12 weeks of explosive heavy-resistance strength training (75–80 % of 1RM) in old (60 years) and very old (80 yeas) women led to substantial gains in isometric muscle strength, rapid force capacity (i.e. RFD) and counter movement jump performance, which all are variables known to be associated with an elevated risk of falls and disability (Caserotti et al. 2008a). Thus, strength training seems to induce changes in neuromuscular function that are of potential importance for the functional performance during activities of daily living.
Recreational football training has been shown to be an effective exercise modality for stimulating physiological adaptations of importance for health promotion in both young, middle-aged and older adults (Jakobsen et al. 2010; Krustrup et al. 2010a, b; Randers et al. 2010a; Schmidt et al. 2014). In concert, the physiological adaptations induced by football training comprise both cardiovascular, metabolic and musculoskeletal factors, making it not only a potent regimen for general health but also a sound strategy in rehabilitation of specific lifestyle diseases (e.g. type 2 diabetes, hypertension, cardiovascular disease) (Andersen et al. 2014; Krustrup et al. 2010a, b, c; Schmidt et al. 2014). However, it remains unknown whether recreational football training can improve mechanical muscle function (MVC strength, RFD) to benefit ADL to the same extent as strength training in older adults. In terms of neuromuscular capacity, short-term (12 weeks) recreational football training in middle-aged adults (20–43 years) was found to increase isometric hamstring strength and postural balance, the latter evidenced by decreased sway area, sway length and number of falls in the flamingo balance test (Jakobsen et al. 2010; Krustrup et al. 2010a). No longitudinal studies have previously examined the adaptability in maximal muscle strength, functional ADL capacity and rapid force capacity (contractile RFD and impulse) in older adults in response to football training. Based on cross-sectional data, elderly individuals exposed to lifelong football training demonstrated superior RFD and postural stability compared with age-matched untrained controls (Sundstrup et al. 2010). Whether these differences could be ascribed to the participation in lifelong football training or rather represent a systematic selection of individuals initially characterized by high levels of RFD and postural stability remains unknown. Thus, longitudinal intervention studies investigating the long-term neuromuscular adaptations to football training in older adults are needed.
Consequently, the overall aim of the present study was to determine and compare neuromuscular adaptation to long-term (1 year) football or strength training in older untrained adults, and to assess the concurrent effect on functional ADL capacity.
Methods
Study design
The present study represents a secondary analysis of a larger interventional protocol carried out in Copenhagen, Denmark, from 2012 to 2014. Primary and secondary outcome measures have been reported elsewhere (Andersen et al. 2014; Schmidt et al. 2014). The focus of the current paper is neuromuscular adaptations and functional performance following 1 year of recreational football training or strength training in elderly males. All participants were informed about the purpose and content of the project and gave their written informed consent to participate in the study. The study conformed to the Ethical standards of the World Medical Association (Declaration of Helsinki) and was approved by the local Ethical Committee of Copenhagen (H-1-2011-013). The study was reported at ClinicalTrials.gov.: NCT01530035.
Subjects
Twenty-seven healthy old males (68.2 ± 3.2 years) participated in the study. Recruitment and flow of participants have been described elsewhere (Andersen et al. 2014; Schmidt et al. 2014). In brief, participants were randomly assigned to either recreational football training (FT: n = 10), strength training group (ST: n = 9) or an inactive control group (CON: n = 8) stratified for maximal oxygen uptake (VO2max) and body mass index. Except for one participant, a recreational golfer, all subjects self-reported to have been physically inactive for the past 5–10 years. Inclusion criteria were (1) age between 65 and 75 years and (2) eligibility to participate in the testing battery and the training interventions. Exclusion criteria were (1) a medical history of cardiovascular disease, (2) hyperglycemia or (3) hypertension. No baseline differences existed between the groups for age (FT: 68.0 ± 4.0; ST: 69.1 ± 3.1; CON: 67.4 ± 2.7 years), body weight (FT: 77.7 ± 9.4; ST: 85.8 ± 12.0; CON: 89.3 ± 12.4 kg), height (FT: 173.3 ± 7.8; ST: 176.7 ± 9.8; CON: 179.0 ± 6.2 cm), VO2max (FT: 27.5 ± 5.4; ST: 28.9 ± 5.5; CON: 30.8 ± 3.3 mL/min/kg) or body mass index.
Flow of participants
Figure 1 illustrates the overall flow of participants. One subject in the FT group experienced an Achilles tendon rupture during the initial phase of the intervention period and was therefore treated as a drop out, meaning that all his data were excluded from the study analysis. Additionally, one person from the control group did not meet for any of the neuromuscular test rounds and was excluded from analysis. Two persons also in the control group never showed up for the final neuromuscular test round at 1-year follow-up and were only tested at baseline and at 4 months follow-up. Because the statistical analysis (Proc Mixed; see below) inherently accounts for missing values, participants with missing values at follow-up were also included in the present analyses, thus adhering to an intention-to-treat test design. Thus, the subjects included in the overall statistical analysis comprised nine football trained individuals, nine strength trained individuals and seven controls (Fig. 1).

Participant flow
Interventions
Football and strength training were supervised and performed in 1-h sessions for 12 months. Controls were instructed to continue with their daily routines and not to change lifestyle habits during the study period. The football and strength training were intended to be carried out twice a week for the first 4 months and three times a week for the last 8 months. The FT and ST group performed on average 1.7 (range 1.2–2.2) and 1.9 (1.4–2.2), respectively, of the intended weekly training sessions during the 1-year intervention period. None of the subjects reported any changes in habitual physical activity levels during the intervention period besides participation in strength training or football training.
Recreational football training (FT) was performed using an outside natural grass area from April to November while using an indoor Gym from November to March. Each training session over the first three months was initiated with 15 min of low intensity warm-up (inspired by the injury prevention programme 11+; F-MARC) followed by 3 × 15 min of 4v4 and 5v5 games on small pitches. The playing periods were interspersed by 2-min rest periods. For the following 9 months, warm-up was performed prior to the 1-h football training session and the training sessions consisted of 4 × 15 min of active play interspersed by 2-min rest periods. The intensity of the training sessions, estimated as mean heart rate, was 138 ± 3 and 143 ± 3 bpm during training in week 1 and week 16, respectively (Andersen et al. 2014). During the initial phase of the training period, one subject in the football training group left the study due to an Achilles tendon injury. The data from this subject have been excluded.
Strength training (ST) was performed in a dedicated weight training Gym (University of Copenhagen) with each training session initiated by 5 min of low-intensity warm-up. Subjects performed high-intensity strength training with five exercises targeting the muscles in the lower extremity and upper body (leg press, seated leg extension, prone hamstring curl, pull-down and lateral raise). Each training session was additionally completed with 5 min of body-weight exercises for the core muscles (back extension and abdominal crunch). Training was performed in a progressive manner with weights ranging from 16 to 20RM (~50–60 % 1RM) during the first months and 12–8RM (~70–80 % 1RM) during the last 11 months. During the first 3 months, three sets of each exercise were performed whereas four sets were performed for the remainder of the intervention period. Rest periods between sets were 1:30 min for the entire period. To promote motivation and variation to the strength training protocol, two additional upper body exercises were introduced and added to the training program at week 25 (lunges with dumbbells and seated rows), both performed with four sets of 8RM (80 % 1RM). All exercises were performed until exhaustion without compromising lifting technique and safety.
For more details on subject recruitment, flow of participants and specific intervention procedures, see Schmidt et al. (Schmidt et al. 2014).
Outcome measures
Participants underwent a comprehensive testing protocol at baseline (early March), after 4 months (late June) and 12 months (early March) of the intervention period. Outcome measures described in this article are all related to neuromuscular capacity and functional performance, and represent an independent part of the larger interventional study. Thus, the outcome measures obtained in the present study were performed on a separate day (neuromuscular test round), than the cardiovascular and metabolic outcomes previously reported (Andersen et al. 2014; Schmidt et al. 2014). Subjects were asked not to perform any strenuous physical activity 2 days before testing. The following physical tests are described in the chronological order in which they were performed on the day of testing.
Postural balance
Subjects were instructed to perform a single-leg static stance on an instrumented force plate (AMTI OR6, Watertown, MA, USA) using their dominant leg (without shoes) while standing as still as possible for 15 s. During data acquisition, the participants were instructed to focus their vision on a fixed circle on the wall in front of them, with the non-stance leg lifted above the platform and arms crossed over the chest. Vertical ground reaction force (Fz), anterior–posterior (AP) moment (Mx) and medio-lateral (ML) moment (My) were sampled (100 Hz) using custom-made Matlab (Mathworks) acquisition software (16-bit A/D conversion, DT9804, Data translation, Marlboro, MA, USA). All Fz, Mx and My-signals were digitally low-pass filtered with a 4th order zero-lag Butterworth filter (8 Hz cutoff frequency) (Winter, 1990). Displacement of the center of pressure (CoP) was calculated as (x, y) = (x 0 + M y /F z , y 0 + M x /F z ), where (x 0, y 0) was the geometrical center of the force plate (Jakobsen et al. 2010; Oliveira et al. 2013). Participants performed two trials separated by a rest period of 30 s, and the trial with the lowest CoP sway area was selected for statistical analysis (Baier and Hopf 1998; Jakobsen et al. 2010).
Countermovement jumping
Maximal vertical jump height was assessed during countermovement jumping on a force plate (AMTI OR6, Watertown, MA, USA). Subjects performed between three and five bilateral jumps interspersed with at least 30 s of rest, until jump height could not be improved any further. The subjects were instructed to jump as high as possible and the trial with the highest jump height was selected for statistical analysis. Maximum jump height was derived by time integration of the force signal to yield vertical take-off velocity (Vto) and subsequently using the equation: jump height = Vto2/(2 g), where g = gravitational acceleration = 9.82 m/s2 (Andersen et al. 2014; Jakobsen et al. 2012).
Sit-to-stand
The standardized 30-s chair stand test (STS) was used as a functional performance measure (Andersen et al. 2014; Jones et al. 1999). Subjects were instructed to sit in a rigid chair (43 cm seat height) with straight back, arms crossed over the chest and both feet flat on the floor. On the signal “Go”, participants were to rise to full standing position (knees fully extended) and then sit back down again. This movement was repeated for as many times as possible during 30 s and the number of stands was measured by an electronic switch located in the seat and connected to a laptop. Prior to actual data acquisition, the correct technique was first demonstrated by the test leader and then rehearsed by the participant.
Muscle strength and rapid force capacity
An isokinetic dynamometer (Biodex System 3 Pro, Brookhaven R&D Plaza, New York, USA) was used for strength testing of the quadriceps and hamstring muscles. The rotational axis of the dynamometer was aligned to the lateral femoral epicondyle, and the lower leg was attached to the dynamometer lever arm above the medial malleolus, with no static fixation of the ankle joint. For each subject, identical positioning of the seat, backrest, dynamometer head, and lever arm length were used for baseline, 4 and 12 months follow-up. All measurements were performed using the dominant leg and all recorded torque signals were corrected for the effect of gravity (Aagaard et al. 2000).
Maximal concentric and eccentric quadriceps strength (peak torque) was obtained during slow (60°/s) knee extensions as described previously by Aagaard et al. (2000). In brief, after warm-up and preconditioning, consisting of submaximal and near maximal contractions, subjects performed several trials interspersed by at least 30 s of rest, until peak torque (provided to the subject by online visual feedback on a pc screen) could not be improved any further. Typically, 3–5 trials were performed for each contraction mode. The trial with highest torque (i.e. peak torque) was identified in each subject and selected for statistical analysis.
Additionally, each subject performed maximal isometric knee extensor and flexor contractions at a 70° knee joint angle (0° = full extension). To obtain the steepest time–torque-curve as possible, subjects were instructed to contract the muscles as fast and hard as possible. Typically, 3–5 trials were performed for both isometric knee extension and knee flexion contractions. Rapid force capacity (contractile RFD) was determined from the trial with maximal isometric torque (maximal MVC) and was derived as the steepest slope of the torque–time curve (Aagaard et al. 2002).
Stair ascent
Participants were instructed to ascent a nine-step staircase (17-cm step height) as fast as possible without the use of handrail. Following a familiarization procedure (involving at least one trial of stair walking at near maximal speed), two trials were performed separately interspersed by 30 s of rest and the trial with the fastest time was used for statistical analysis. Time was recorded with a stop-watch and started when the subject touched the first step and ended when the plateau of the 9th step was touched. Because of safety precautions, descending as fast as possible was not carried out. Strong verbal encouragement was given to each subject during all trials to motivate for maximal performance.
Statistical analysis
All statistical analyses were performed using the SAS statistical software for Windows (SAS Institute, Cary, NC). Outcome variables were analyzed according to the intention-to-treat principle using a repeated measures 3 × 3 mixed-factorial design (Proc Mixed), with time (0, 4, 12 months), group (FT, ST and CON), and time by group as independent categorical variables (fixed factors). Each patient was entered as a random effect. The baseline value of the outcome variables was included as a covariate in the linear mixed model to adjust for any potential between-group difference at baseline. Because the Proc Mixed model inherently accounts for missing values, participants with missing values at follow-up were also included in the analyses. P values from post hoc tests were only reported when a significant main effect or interaction effect was found. An alpha level of 0.05 was used for statistical significance. Outcome variables are reported as least square means ± standard error (SE) unless otherwise stated.
Results
Strength and rapid force capacity
A group-by-time interaction was found for concentric quadriceps strength (P < 0.05). Compared to FT and CON, dynamic quadriceps strength improved to a greater extent in ST (P < 0.001 and P < 0.01, respectively). Specifically, concentric quadriceps strength increased by 14 % (P < 0.01; Table 1; Fig. 2) in ST from baseline to follow-up. No within-group changes were observed in FT or CON. No group-by-time interaction was observed for eccentric quadriceps strength (P = 0.40).

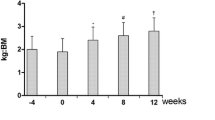
Maximal isometric muscle strength (top panels), rapid force capacity (RFD; mid panels) and dynamic muscle strength (60°/s; bottom panels) obtained before (baseline), during (4 months) and after 12 months of football training (FT), strength training (ST) or when serving as inactive controls (Con). Least square means ± SE. *Different from baseline (P < 0.05). †Different from 4 months (P < 0.05). C different relative change compared to CON (P < 0.05). F different relative change compared to FT (P < 0.05). S different relative change compared to ST (P < 0.05)
A strong group-by-time interaction was also observed for isometric quadriceps strength (P < 0.0001) where ST improved more than both FT (P < 0.0001) and CON (P < 0.0001). Isometric strength increased by 23 % in ST (P < 0.001) from baseline to 1 year follow-up with no change between baseline and 4 months (Table 1; Fig. 2). CON showed an 18 % decrease in isometric quadriceps strength from baseline to 1 year follow-up (P < 0.05) whereas no changes were observed in FT. A group-by-time interaction was observed for quadriceps RFD (P < 0.05). Compared to CON, RFD increased in ST (P < 0.001). No within-group changes in RFD were observed for participants in FT or ST whereas RFD decreased from baseline to 12 months in CON (P < 0.05).
A group-by-time interaction was also observed for isometric hamstring strength (P < 0.05). FT and ST improved hamstring strength from baseline to 12 months follow-up by 18 % (P < 0.05) and 44 % (P < 0.0001), respectively, whereas no changes were observed for CON. Additionally, a change in FT was observed from 4 to 12 months (P < 0.05) and in ST group from baseline to 4 months (P < 0.01) (Table 1; Fig. 2). Isometric hamstring RFD also showed a group-by-time interaction from baseline to follow-up (P < 0.001) revealing that FT increased RFD by 89 % from baseline to follow-up and thus improved to a greater extent than both ST (+39 %) and CON (−18 %) (P < 0.05 and P < 0.0001, respectively). The improvement in RFD observed in FT was also present from 4 to 12 months (P < 0.0001) whereas no change was observed from baseline to 4 months (P = 0.63). A tendency (P = 0.07) towards an increase in hamstring RFD was observed for ST whereas no within-group change was observed for CON (Fig. 2).
Functional capacity
A group-by-time interaction was found for the sit-to-stand test (P < 0.05). FT and ST increased sit-to-stand performance following 12 months of training by 32 % (P < 0.0001) and 21 % (P < 0.05), respectively, with changes observed in FT being greater than in CON (P < 0.05). Further, both FT and ST improved sit-to-stand performance from baseline to 4 months (P < 0.01 and P < 0.01, respectively) whereas no within-group changes were observed for CON (Fig. 3).

Functional capacity assessed as sit-to-stand performance (top panel), stair ascent time (mid panel) and maximal vertical jump height (bottom panel) before (baseline), during (4 months) and after 12 months of football training (FT), strength training (ST) or when serving as inactive controls (Con). Least square means ± SE. *Different from baseline (P < 0.05). †Different from 4 months (P < 0.05). C different relative change compared to CON (P < 0.05)
Additionally, a strong group-by-time interaction was observed for the stair test (P < 0.001) with both FT and ST improving stair climbing time (and hence increasing stair climbing power) to a greater extent than CON (P < 0.0001 and P < 0.0001, respectively). Participants in FT reduced time by 24 % and observed changes were significant from 0 to 4 months (P < 0.05), 0–12 months (P < 0.0001) and 4–12 months (P < 0.0001), respectively (Table 1). Changes in ST occurred from 0 to 12 months (P < 0.0001) and 4–12 months (P < 0.001) resulting in an 18 % reduction in stair climbing time from baseline to follow-up.
Maximal CMJ jump height increased by 50 % following 12 months training in both FT and ST, with no changes observed in CON (Table 1). In contrast, postural sway area remained unchanged with training. No group-by-time interaction was observed for either postural sway area (P = 0.93) or CMJ jump height (P = 0.39, Table 1).
Discussion
The present study examined changes in neuromuscular capacity and functional ability evoked by 12 months of football or strength training in untrained elderly males. The main study findings were that contractile quadriceps and hamstring strength increased following strength training, whereas football training led to elevated strength and rapid force capacity of the hamstring muscles. Both regimens led to substantial gains in functional capacity evidenced by improved sit-to-stand performance and elevated stair walking speed. No changes were observed for either of the groups in postural balance or jump performance. Thus, long-term football and strength training appear to represent effective interventional strategies in old male adults to preserve factors of importance for ADL and could potentially be a way to improve work ability of senior workers.
Reduced muscle strength of the lower limb is considered as a major risk factor for falls, and elevated leg extensor strength has been associated with fall prevention in healthy older adults (Lord et al. 2003; Pijnappels et al. 2008; Rubenstein 2006; Skelton et al. 2002). In the present study, the regime of strength training led to improved quadriceps strength (isometric and concentric) when compared to football training and non-trained controls. This is in line with previous studies demonstrating positive effects of strength training on knee extensor muscle strength among elderly adults (Caserotti et al. 2008a; Seynnes et al. 2004; Suetta et al. 2004). In contrast, football training did not lead to alterations in quadriceps strength, which conforms to previous cross-sectional observations of no difference in maximum quadriceps contraction strength between lifelong football-trained elderly and untrained age-matched controls (Sundstrup et al. 2010). Thus, it seems that the high contraction forces applied during strength training is a necessary stimulus for fully reversing the age-related decline in quadriceps muscle strength (Aagaard et al. 2010).
In the present study, both football and strength training led to increased hamstring muscle strength, however, the time-course of adaptation appeared to differ between the two exercise modalities. While ST led to early significant improvements (0–4 months) in hamstring muscle strength development, a longer period (12 months) was needed to achieve positive adaptations in hamstring strength with FT. Thus, it seems that longer intervention periods are needed with football exercise involving forceful muscle action such as accelerations, decelerations, rapid turns and tackles to promote gains in contractile hamstring strength (Bradley et al. 2009; Krustrup et al. 2010c; Mohr et al. 2003). This notion is supported by recent findings of only minor improvements in muscle strength following 3–4 months of recreational football training in men (Krustrup et al. 2010c) and women (Helge et al. 2010), whereas 16 months of football training in premenopausal women were found to produce substantial gains in concentric and eccentric hamstring muscle strength (Krustrup et al. 2010c).
Compared with maximal strength, the ability to rapidly develop muscle force during the initial contraction phase (0–100 ms) is particularly compromised by aging (Izquierdo et al. 1999; Korhonen et al. 2006). As several tasks of daily living require the ability of the neuromuscular system to exert high contractile RFD (stair climbing, regaining balance in situations of sudden postural perturbation), interventions aiming at maintaining or increasing rapid force capacity can be of vital importance for maintaining independency in old adults (Fleming et al. 1991). In the present study, rapid force capacity of the quadriceps muscle was improved following both football and strength training, when compared with non-trained age-matched controls. However, within-group changes indicated that these between-group differences were in part caused by the reduction in RFD observed in the control group. Most likely, the decrease in RFD demonstrated by our non-trained control subjects might have appeared as a result of the general decline in RFD known to occur with increasing age (Häkkinen et al. 1995; Hvid et al. 2010; Izquierdo et al. 1999; Klass et al. 2008; Korhonen et al. 2006), while potentially also influenced by seasonal variations (Shephard and Aoyagi, 2009). Notably, the present data suggest that long-term football or strength training is able to fully prevent such age-related deterioration in rapid force capacity, at least when evaluated over a full 1-year period.
With respect to hamstring muscle function, football training appeared superior in increasing rapid force capacity (RFD) compared to both strength training and a non-active lifestyle (controls). Like the observed gain in isometric hamstring strength, this adaptation was only detectable after 12 months of intervention since no increases were observed after 4 months of football training. This supports the notion of a delayed time-course of adaptation with football training, in turn suggesting that extended training periods (>3–4 months) are needed to attain significant improvements in mechanical muscle function. The stimuli responsible for the observed gain in hamstring RFD with FT likely relies on the frequent execution of forceful frontal body accelerations during the football training sessions (Terje et al. 2015; Varley and Aughey, 2013), which typically require a high force production in the hip extensors (Thelen et al. 2005) and, hence, are likely to place substantial loading on the biarticular hamstring muscles. In terms of the adaptive mechanism(s) involved, muscle exercise involving maximal intentional limb acceleration and/or high maximal rate of force development are known to increase maximal MU firing rates and increase doublet discharge firing behavior, altogether contributing to increase RFD (Van Cutsem et al. 1998).
The lack of statistically significant gains in quadriceps RFD following 4 and 12 months of ST was unexpected, since quadriceps RFD has previously been shown to increase in old adults following periods of heavy-resistance strength training (Barry et al. 2005; Caserotti et al. 2008a; Gurjão et al. 2012; Häkkinen et al. 1998; Suetta et al. 2004). However, while a majority of these studies employed explosive-type contraction efforts (i.e. using maximal intentional movement speed), such muscle actions were not emphasized in the present study, which may explain the lack of a statistically significant change in quadriceps RFD in the ST group.
The age-related decrease in isolated muscle strength and rapid force capacity has been associated with reduced postural balance during static stance (Izquierdo et al. 1999), and elderly individuals with reduced RFD and maximal lower limb muscle strength (leg press, knee extension) show an impaired ability to avoid tripping over unexpected obstacles during level walking (Pijnappels et al. 2008). Thus, in theory, the observed changes in muscle strength and rapid force capacity following football training would seem to benefit an improved postural stability. Nevertheless, no-between group changes in postural sway performance were observed following 12 months of football or strength training. In contrast, recent findings show that football training may effectively improve postural stability in sedentary middle-aged men, reflected by decreases in center of pressure sway area and excursion length along with a decreased number of falls during the flamingo balance test (Jakobsen et al. 2010). Additionally, Randers et al. (2010b) observed within-group reduction in number of falls in the flamingo test following long-term (64 weeks) football training in middle-aged males. The reason for the apparent discrepancies between studies remains unknown, but may reside in differences in participant’s age and the specific experimental setups used.
Besides muscular contraction strength and RFD, functional capacity during simulation of every-day tasks is a key variable linking physiological adaptations to ADL. The ability to navigate stairs and rise from a chair represent essential tasks of daily living and may require substantial amounts of muscle strength, power and RFD while also affected by the capacity for postural control. In the present study, sit-to-stand performance was found to improve following both football and strength training. Strength training in combination with aerobic, coordination, balance and flexibility exercises has previously been shown to be effective in enhancing functional motor performance, evidenced by improved chair rise time and maximal walking speed in (75 years) old males (Caserotti et al. 2008b). When short-term training results were obtained in the present group of subjects, we observed 26–29 % improvements in sit-to-stand performance following 4 months of football or strength training (Andersen et al. 2014). Comparable improvements in sit-to-stand performance (21–32 %) were noted following 12 months of training in the present study, where football and strength training also led to a reduction in stair climbing time by 24 and 18 %, respectively. Improved stair-ascent performance has previously been observed in elderly women following 12 weeks of explosive-type strength training (Holsgaard-Larsen et al. 2011). To our best knowledge, no previous data exist on the effect of football training on stair walking ability in elderly adults. In the present study, although jumping ability was improved by 50 % by both football and strength training, respectively, no group-by-time interaction was observed for jump performance, which is in agreement with previous studies on the effect of football training in elderly males (Jakobsen et al. 2012; Randers et al. 2010b). We have previously observed that 12 weeks of progressive ST led to increased CMJ jump height and a more explosive-type (faster) jumping strategy in young adults, compared with football training (Jakobsen et al. 2012). Despite the lack of group-by-time interaction in vertical jump performance, it seems that football training can preserve selected aspects of functional ability related to ADL to the same extent as strength training. A series of recent reviews have described that football training combines elements of endurance training, high-intensity interval training and strength training, and results in broad-spectrum cardiovascular, metabolic and musculoskeletal fitness effects (Bangsbo et al. 2015; Milanović et al. 2015; Oja et al. 2015). The present study showing the benefits of improved mechanical muscle function on ADL is, therefore, in line with the recent literature on the fitness and health effects of recreational football training for untrained healthy participants.
The present study contains both strengths and limitations. The limited number of participants recruited for the study along with the observed drop-out in the control group stresses that the results should be interpreted with caution. On the other hand, conducting long-term longitudinal training studies in the aging population is extremely difficult, which means that valuable information still can be gained from this study. Finally, the exclusion and inclusion criteria used in the present study confine the generalizability of our results to healthy, previously untrained elderly males.
Conclusions
Long-term (1-year) strength training led to increased quadriceps and hamstring strength, whereas the adaptations to football training mainly included enhanced strength and rapid force capacity of the hamstring muscles. Gains in functional ability were observed following both training regimens, evidenced by reduced stair-ascent time and increased chair rising performance. Thus, long-term football and strength training appear to represent effective interventional strategies in old male adults to preserve factors of importance for ADL. Along with other recent investigations, the present study provides evidence that football for sedentary elderly can be organized in a safe and feasible manner by combining warm-up with small-sided football training on small natural grass or artificial turf pitches.
Abbreviations
- ADL:
-
Activities of daily living
- CMJ:
-
Counter movement jump
- CON:
-
Control group
- FT:
-
Football training group
- MVC:
-
Maximal voluntary contraction
- RFD:
-
Rate of force development
- RM:
-
Repetition maximum
- ST:
-
Strength training group
- STS:
-
Sit-to-stand test
References
Aagaard P, Simonsen EB, Andersen JL, Magnusson SP, Bojsen-Moller F, Dyhre-Poulsen P (2000) Antagonist muscle coactivation during isokinetic knee extension 12. Scand J Med Sci Sports 10:58–67
Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre-Poulsen P (2002) Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol 93:1318–1326
Aagaard P, Suetta C, Caserotti P, Magnusson SP, Kjaer M (2010) Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports 20:49–64. doi:10.1111/j.1600-0838.2009.01084.x
Andersen TR, Schmidt JF, Nielsen JJ, Randers MB, Sundstrup E, Jakobsen MD, Andersen LL, Suetta C, Aagaard P, Bangsbo J, Krustrup P (2014) Effect of football or strength training on functional ability and physical performance in untrained old men. Scand J Med Sci Sports 24(Suppl 1):76–85. doi:10.1111/sms.12245
Baier M, Hopf T (1998) Ankle orthoses effect on single-limb standing balance in athletes with functional ankle instability. Arch Phys Med Rehabil 79:939–944
Bangsbo J, Hansen PR, Dvorak J, Krustrup P (2015) Recreational football for disease prevention and treatment in untrained men: a narrative review examining cardiovascular health, lipid profile, body composition, muscle strength and functional capacity. Br J Sports Med 49:568–576. doi:10.1136/bjsports-2015-094781
Barry BK, Warman GE, Carson RG (2005) Age-related differences in rapid muscle activation after rate of force development training of the elbow flexors. Exp Brain Res 162:122–132. doi:10.1007/s00221-004-2127-3
Bassey EJ, Fiatarone MA, O’Neill EF, Kelly M, Evans WJ, Lipsitz LA (1992) Leg extensor power and functional performance in very old men and women. Clin Sci Lond Engl 1979(82):321–327
Bijnen FC, Caspersen CJ, Feskens EJ, Saris WH, Mosterd WL, Kromhout D (1998) Physical activity and 10-year mortality from cardiovascular diseases and all causes: the Zutphen Elderly Study. Arch Intern Med 158:1499–1505
Blair SN, Kohl HW, Paffenbarger RS, Clark DG, Cooper KH, Gibbons LW (1989) Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA 262:2395–2401
Bradley PS, Sheldon W, Wooster B, Olsen P, Boanas P, Krustrup P (2009) High-intensity running in English FA Premier League soccer matches 1. J Sports Sci 27:159–168
Caserotti P, Aagaard P, Larsen JB, Puggaard L (2008a) Explosive heavy-resistance training in old and very old adults: changes in rapid muscle force, strength and power. Scand J Med Sci Sports 18:773–782
Caserotti P, Aagaard P, Puggaard L (2008b) Changes in power and force generation during coupled eccentric-concentric versus concentric muscle contraction with training and aging. Eur J Appl Physiol 103:151–161
Christensen U, Støvring N, Schultz-Larsen K, Schroll M, Avlund K (2006) Functional ability at age 75: is there an impact of physical inactivity from middle age to early old age? Scand J Med Sci Sports 16:245–251. doi:10.1111/j.1600-0838.2005.00459.x
Fleming BE, Wilson DR, Pendergast DR (1991) A portable, easily performed muscle power test and its association with falls by elderly persoms. Arch Phys Med Rehabil 72:886–889
Gurjão ALD, Gobbi LTB, Carneiro NH, Gonçalves R, Ferreira de Moura R, Cyrino ES, Altimari LR, Gobbi S (2012) Effect of strength training on rate of force development in older women. Res Q Exerc Sport 83:268–275. doi:10.1080/02701367.2012.10599857
Häkkinen K, Pastinen UM, Karsikas R, Linnamo V (1995) Neuromuscular performance in voluntary bilateral and unilateral contraction and during electrical stimulation in men at different ages. Eur J Appl Physiol 70:518–527
Häkkinen K, Kallinen M, Izquierdo M, Jokelainen K, Lassila H, Mälkiä E, Kraemer WJ, Newton RU, Alén M (1998) Changes in agonist-antagonist EMG, muscle CSA, and force during strength training in middle-aged and older people. J Appl Physiol 84:1341-1349
Helge EW, Aagaard P, Jakobsen MD, Sundstrup E, Randers MB, Karlsson MK, Krustrup P (2010) Recreational football training decreases risk factors for bone fractures in untrained premenopausal women. Scand J Med Sci Sports 20(Suppl 1):31–39. doi:10.1111/j.1600-0838.2010.01107.x
Holsgaard-Larsen A, Caserotti P, Puggaard L, Aagaard P (2011) Stair-ascent performance in elderly women: effect of explosive strength training. J Aging Phys Act 19:117–136
Hvid L, Aagaard P, Justesen L, Bayer ML, Andersen JL, Ørtenblad N, Kjaer M, Suetta C (2010) Effects of aging on muscle mechanical function and muscle fiber morphology during short-term immobilization and subsequent retraining. J Appl Physiol Bethesda Md 1985(109):1628–1634. doi:10.1152/japplphysiol.00637.2010
Izquierdo M, Aguado X, Gonzalez R, López JL, Häkkinen K (1999) Maximal and explosive force production capacity and balance performance in men of different ages. Eur J Appl Physiol 79:260–267. doi:10.1007/s004210050504
Jakobsen MD, Sundstrup E, Krustrup P, Aagaard P (2010) The effect of recreational soccer training and running on postural balance in untrained men. Eur J Appl Physiol. doi:10.1007/s00421-010-1669-2
Jakobsen MD, Sundstrup E, Randers MB, Kjær M, Andersen LL, Krustrup P, Aagaard P (2012) The effect of strength training, recreational soccer and running exercise on stretch-shortening cycle muscle performance during countermovement jumping. Mov Sci, Hum. doi:10.1016/j.humov.2011.10.001
Johannsen DL, DeLany JP, Frisard MI, Welsch MA, Rowley CK, Fang X, Jazwinski SM, Ravussin E, Louisiana Healthy Aging Study (2008) Physical activity in aging: comparison among young, aged, and nonagenarian individuals. J Appl Physiol Bethesda Md 1985(105):495–501. doi:10.1152/japplphysiol.90450.2008
Jones CJ, Rikli RE, Beam WC (1999) A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport 70:113–119. doi:10.1080/02701367.1999.10608028
Klass M, Baudry S, Duchateau J (2008) Age-related decline in rate of torque development is accompanied by lower maximal motor unit discharge frequency during fast contractions. J Appl Physiol Bethesda Md 1985(104):739–746. doi:10.1152/japplphysiol.00550.2007
Korhonen MT, Cristea A, Alén M, Häkkinen K, Sipilä S, Mero A, Viitasalo JT, Larsson L, Suominen H (2006) Aging, muscle fiber type, and contractile function in sprint-trained athletes. J Appl Physiol Bethesda Md 1985(101):906–917. doi:10.1152/japplphysiol.00299.2006
Krustrup P, Aagaard P, Nybo L, Petersen J, Mohr M, Bangsbo J (2010a) Recreational football as a health promoting activity: a topical review. Scand J Med Sci Sports 20(Suppl 1):1–13. doi:10.1111/j.1600-0838.2010.01108.x
Krustrup P, Christensen JF, Randers MB, Pedersen H, Sundstrup E, Jakobsen MD, Krustrup BR, Nielsen JJ, Suetta C, Nybo L, Bangsbo J (2010b) Muscle adaptations and performance enhancements of soccer training for untrained men. Eur J Appl Physiol 108:1247–1258. doi:10.1007/s00421-009-1319-8
Krustrup P, Hansen PR, Andersen LJ, Jakobsen MD, Sundstrup E, Randers MB, Christiansen L, Helge EW, Pedersen MT, Søgaard P, Junge A, Dvorak J, Aagaard P, Bangsbo J (2010c) Long-term musculoskeletal and cardiac health effects of recreational football and running for premenopausal women. Scand J Med Sci Sports 20(Suppl 1):58–71. doi:10.1111/j.1600-0838.2010.01111.x
Larsen AH, Puggaard L, Hämäläinen U, Aagaard P (2008) Comparison of ground reaction forces and antagonist muscle coactivation during stair walking with ageing. J Electromyogr Kinesiol Off J Int Soc Electrophysiol Kinesiol 18:568–580. doi:10.1016/j.jelekin.2006.12.008
Lord SR, Menz HB, Tiedemann A (2003) A physiological profile approach to falls risk assessment and prevention. Phys Ther 83:237–252
Milanović Z, Pantelić S, Čović N, Sporiš G, Krustrup P (2015) Is recreational soccer effective for improving VO2max—a systematic review and meta-analysis. Sports Med Auckl NZ 45:1339–1353. doi:10.1007/s40279-015-0361-4
Mohr M, Krustrup P, Bangsbo J (2003) Match performance of high-standard soccer players with special reference to development of fatigue 3. J Sports Sci 21:519–528
Oja P, Titze S, Kokko S, Kujala UM, Heinonen A, Kelly P, Koski P, Foster C (2015) Health benefits of different sport disciplines for adults: systematic review of observational and intervention studies with meta-analysis. Br J Sports Med 49:434–440. doi:10.1136/bjsports-2014-093885
Oliveira ASC, Brito Silva P, Farina D, Kersting UG (2013) Unilateral balance training enhances neuromuscular reactions to perturbations in the trained and contralateral limb. Gait Posture 38:894–899. doi:10.1016/j.gaitpost.2013.04.015
Pijnappels M, van der Burg PJCE, Reeves ND, van Dieën JH (2008) Identification of elderly fallers by muscle strength measures. Eur J Appl Physiol 102:585–592. doi:10.1007/s00421-007-0613-6
Randers MB, Nielsen JJ, Krustrup BR, Sundstrup E, Jakobsen MD, Nybo L, Dvorak J, Bangsbo J, Krustrup P (2010a) Positive performance and health effects of a football training program over 12 weeks can be maintained over a 1-year period with reduced training frequency. Scand J Med Sci Sports 20(Suppl 1):80–89. doi:10.1111/j.1600-0838.2010.01091.x
Randers MB, Nielsen JJ, Krustrup BR, Sundstrup E, Jakobsen MD, Nybo L, Dvorak J, Bangsbo J, Krustrup P (2010b) Positive performance and health effects of a football training program over 12 weeks can be maintained over a 1-year period with reduced training frequency: long-term effects of reduced-frequency football training. Scand J Med Sci Sports 20:80–89. doi:10.1111/j.1600-0838.2010.01091.x
Rubenstein LZ (2006) Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing 35(Suppl 2):ii37–ii41. doi:10.1093/ageing/afl084
Schmidt JF, Hansen PR, Andersen TR, Andersen LJ, Hornstrup T, Krustrup P, Bangsbo J (2014) Cardiovascular adaptations to 4 and 12 months of football or strength training in 65- to 75-year-old untrained men: training, aging, and cardiovascular function. Scand J Med Sci Sports 24:86–97. doi:10.1111/sms.12217
Seynnes O, Fiatarone Singh MA, Hue O, Pras P, Legros P, Bernard PL (2004) Physiological and functional responses to low-moderate versus high-intensity progressive resistance training in frail elders. J Gerontol A Biol Sci Med Sci 59:503–509
Shephard RJ, Aoyagi Y (2009) Seasonal variations in physical activity and implications for human health. Eur J Appl Physiol 107:251–271. doi:10.1007/s00421-009-1127-1
Skelton DA, Kennedy J, Rutherford OM (2002) Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing 31:119–125
Suetta C, Aagaard P, Rosted A, Jakobsen AK, Duus B, Kjaer M, Magnusson SP (2004) Training-induced changes in muscle CSA, muscle strength, EMG, and rate of force development in elderly subjects after long-term unilateral disuse. J Appl Physiol Bethesda Md 1985(97):1954–1961. doi:10.1152/japplphysiol.01307.2003
Sundstrup E, Jakobsen MD, Andersen JL, Randers MB, Petersen J, Suetta C, Aagaard P, Krustrup P (2010) Muscle function and postural balance in lifelong trained male footballers compared with sedentary elderly men and youngsters. J Med Sci Sports Scand. doi:10.1111/j.1600-0838.2010.01092.x
Terje D, Jørgen I, Gertjan E, Geir Håvard H, Ulrik W (2015) Player load, acceleration, and deceleration during 45 competitive matches of elite soccer. J Strength Cond Res Natl Strength Cond Assoc. doi:10.1519/JSC.0000000000001063
Thelen DG, Chumanov ES, Best TM, Swanson SC, Heiderscheit BC (2005) Simulation of biceps femoris musculotendon mechanics during the swing phase of sprinting. Med Sci Sports Exerc 37:1931–1938
Van Cutsem M, Duchateau J, Hainaut K (1998) Changes in single motor unit behaviour contribute to the increase in contraction speed after dynamic training in humans. J Physiol 513(Pt 1):295–305
Varley MC, Aughey RJ (2013) Acceleration profiles in elite Australian soccer. Int J Sports Med 34:34–39. doi:10.1055/s-0032-1316315
Westerterp KR, Meijer EP (2001) Physical activity and parameters of aging: a physiological perspective. J Gerontol A Biol Sci Med Sci 56(Spec No 2):7–12
Winter DA (1990) Biomechanics and motor control of human movement. Wiley, New York, pp 11–50
Acknowledgments
The authors would like to thank Stine Dam Søndergaard, Emil Lavard Munksgaard, Micaëla Stener Nielsen and Therese Hornstrup for valuable practical and technical assistance. The study was supported by the FIFA—Medical Assessment and Research Centre (F-MARC), The Danish Ministry of Culture (Kulturministeriets Udvalg for Idrætsforskning) and Nordea-fonden.
Author information
Authors and Affiliations
Corresponding author
Additional information
Communicated by William J. Kraemer.
Rights and permissions
About this article

Cite this article
Sundstrup, E., Jakobsen, M.D., Andersen, L.L. et al. Positive effects of 1-year football and strength training on mechanical muscle function and functional capacity in elderly men. Eur J Appl Physiol 116, 1127–1138 (2016). https://doi.org/10.1007/s00421-016-3368-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-016-3368-0