
Abstract
Purpose
The purpose of this experiment was to study breathing pattern and operating lung volume during 45 min of exercise with a heavy backpack (25 kg) and examine the effect of this exercise on respiratory muscle strength.
Methods
Fifteen males completed randomly ordered graded exercise tests on a treadmill with and without a correctly sized and fitted 25 kg pack. Subsequently, each subject completed, in random order, on separate days, 45 min of treadmill walking with and without the pack. Oxygen demand was matched between conditions (loaded: 3.01 ± 0.11 and unloaded 3.02 ± 0.11 L min−1).
Results
With load, breathing frequency (f B) and minute ventilation increased by 21.7 and 15.1 % (P < 0.05), respectively, while tidal volume (V T) and end-inspiratory lung volume (EILV) were reduced by 6.3 and 6.4 % (P < 0.05), respectively, compared to unloaded. Following loaded exercise, maximal inspiratory pressure decreased by 6.7 % (P < 0.05) with no change in maximal expiratory pressure. No changes in maximal inspiratory or expiratory pressures were observed following unloaded exercise. Despite equivalent oxygen demand, perceived exercise stress and breathing discomfort was higher (P < 0.05) in the loaded condition.
Conclusions
The mechanical disadvantage placed on the respiratory system during exercise with a heavy pack led to compensatory changes in breathing pattern and EILV, and a reduction in maximal inspiratory pressure post-exercise. We suggest that in an attempt to minimize the work of breathing, subjects adopted a shallow and frequent breathing pattern. However, this pattern increased deadspace and minute ventilation, which likely contributed to altered perceptions of exercise stress and breathing discomfort.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Carrying a heavy load is common to many occupations such as infantry, wildland firefighting, and search and rescue. Although a fitted backpack is one of the most efficient forms of load carriage (Abe et al. 2004), the added weight on the thorax can have adverse affects on biomechanical factors such as stride length and trunk positioning (Al-Khabbaz et al. 2008). The added mass increases metabolic rate and alterations in biomechanical efficiency can further increase oxygen uptake (\({\dot{\text{V}}}\)O2) leading to premature whole-body fatigue and decreased occupational effectiveness (Beekley et al. 2007; Dominelli et al. 2012; Taylor et al. 2012). Workers in physically demanding occupations are usually required to carry absolute loads, consisting of essential equipment for duty, rather than a relative load (e.g., a fraction of the individual’s body mass).
During exercise in young healthy males, the normal response from rest to moderate exercise is an increase in minute ventilation to match alveolar ventilation with the metabolic demand. Minute ventilation is increased by changes in tidal volume (V T) and breathing frequency (f B). Tidal volume is increased through reduced end-expiratory lung volume (EELV) and increased end-inspiratory lung volume (EILV) (Sheel and Romer 2012; Stickland et al. 2013). Changes in breathing pattern and operating lung volume serve to optimize the diaphragm length and minimize the energy cost of respiration.
Load carriage places additional strain on the respiratory system at rest and during exercise. The mass of the pack, combined with mild chest wall restriction from the straps has been shown to negatively effect resting pulmonary function (Dominelli et al. 2012; Muza et al. 1989). Dominelli et al. (2012) also demonstrated an alteration in ventilatory mechanics during brief bouts (2.5 min) of exercise with thoracic load carriage at fixed external workloads. The authors suggested that the energy cost of breathing was maintained at higher ventilation rates during load carriage by a compensatory change in operating lung volumes. Faghy and Brown (2014) found that 60 min of light treadmill exercise at 40 % \({\dot{\text{V}}}\)O2peak with heavy load carriage led to reduced maximal inspiratory pressure after exercise. The authors suggested that the altered ventilatory mechanics resulting from thoracic load carriage during prolonged bouts of light exercise decreased respiratory muscle strength.
Due to the time-sensitive nature of emergency response occupations (e.g., infantry, search and rescue, firefighting), longer bouts of exercise around the anaerobic threshold are common (Patton et al. 1991). While the cardiovascular and biomechanical responses to thoracic load carriage during prolonged low-intensity exercise have been previously investigated, the effects of load carriage on exercise ventilation, breathing pattern, and operating lung volume during prolonged exercise near the anaerobic threshold are not well understood. We suggest that for many emergency response occupations, work at or near the anaerobic threshold is particularly relevant for time-sensitive operational effectiveness and safety. Previous research (e.g., Dominelli et al. 2012) has been helpful in understanding the effects of short periods of work with load carriage on selected aspects of the ventilatory system. However, prolonged exercise around anaerobic threshold typically results in a slow rise in ventilation (Hopkins et al. 1998; Stickland et al. 2004) and may compound the reduction in respiratory muscle strength, alter breathing mechanics and potentiate perception of effort and/or breathlessness. Occupationally relevant work times and intensities should be explored to understand the physiological impact of load carriage during arduous work conditions.
The purpose of this investigation was to study components of ventilation, specifically: breathing pattern and operating lung volume during 45 min of vigorous exercise with heavy load carriage (experimental condition) compared to unloaded exercise (control condition) at the same oxygen demand. It was hypothesized that continuous exercise with a properly sized and fitted backpack weighing 25 kg would result in a compensatory change in breathing pattern. Specifically, V T and EILV would decrease and f B would increase, with the differences becoming greater over time, compared to the unloaded condition. The progressive alteration in breathing pattern would increase deadspace ventilation requiring minute ventilation to increase in order to maintain alveolar ventilation. As a result of the increased ventilation and altered breathing pattern, we also hypothesized that maximal voluntary inspiratory pressure would be decreased following exercise in the loaded condition.
Methods
Subjects
Fifteen healthy, active males (Mean ± SD, age 29 ± 3, stature 182.3 ± 5.4 cm, mass 83.5 ± 9.5 kg) with no known history of cardiovascular or respiratory disease provided written informed consent to participate in the study, which had been approved by the appropriate institutional Research Ethics Board. Subjects were screened for safe exercise with the Physical Activity Readiness Questionnaire (PAR-Q+) and also by a physician for safe ingestion of a temperature-transmitting capsule. The participants wore a properly sized and fitted backpack (Arc’Teryx Bora 80, North Vancouver BC) during loaded phases of the study. Total weight was 25 kg (pack plus load) and care was taken to maintain consistent volume, load distribution and fit (e.g., strap tightness) for all packs used in the experiment. The control condition involved unloaded exercise. In both conditions, participants were dressed in shorts, t-shirt and running shoes.
Design
Four distinct experimental steps were completed over a 2-week period in the following order: (1) pulmonary function tests in unloaded and loaded conditions (order randomized) (2) graded exercise tests in unloaded and loaded conditions (order randomized), (3) practice of the experimental protocols (4) experimental protocols in unloaded and loaded conditions (order randomized). All tests were carried out in an air-conditioned laboratory (21–23° C) with low humidity.
Pulmonary function tests
Each subject completed randomly ordered resting pulmonary function testing (Vmax Encore, Carefusion, Yorba Linda, California, USA) in both conditions. Total lung capacity (TLC) was calculated by nitrogen washout. Pulmonary function testing was performed according to the guidelines of the American Thoracic Society (2005). Maneuvers were completed while standing upright with minimal forward lean.
Graded exercise tests
On separate days subjects completed in random order, a graded exercise test in both conditions to determine ventilatory threshold and measure \({\dot{\text{V}}}\)O2peak. The graded exercise test consisted of a constant speed (1.5 m s−1) walking protocol on a motorized treadmill (Standard Industries, Fargo, ND). The test began at 0 % grade with step increases of 2 % grade every 2 min until ventilatory threshold was detected. Subsequently the grade increased by 2 % each minute until volitional exhaustion. Ventilatory threshold was identified by an increase in the ventilatory equivalent for oxygen (\({\dot{\text{V}}}\) E/\({\dot{\text{V}}}\)O2) while the ventilatory equivalent for carbon dioxide (\({\dot{\text{V}}}\) E/\({\dot{\text{V}}}\)CO2) remained steady (Wasserman 1987). Post exercise spirometry was performed to rule out exercise-induced bronchoconstriction. After at least 24-hours of recovery, the subject completed the second graded exercise test in the alternate condition.
A two-way breathing valve was used to collect expired gases (Hans Rudolph, Kansas City, MO, USA). Expired gases and ventilatory parameters were analyzed and calculated using a metabolic measurement system (TrueOne, ParvoMedics, Salt Lake City, UT, USA). The system was calibrated according to manufacturer’s guidelines prior to each test. Calibration of the gas analyzers was verified immediately following each test. Heart rate was monitored continuously using telemetry and was recorded at the end of each minute (Polar Beat, Electro, Lachine, QC).
Practice session
Prior to commencing the actual experiment, each subject completed a practice session which accomplished several purposes. First, the exercise intensities, determined from the results of the two graded exercise tests were evaluated to ensure that the oxygen demand of the loaded and unloaded conditions was satisfactorily matched (±0.1 L min−1). Second, the subject exercised for 20 min in each condition to evaluate tolerance for the predetermined workloads. Third, the subject was fully oriented to all experimental procedures (e.g., measurement of inspiratory capacity during exercise, measurement of maximal voluntary inspiratory and expiratory pressures before and after exercise).
The specific exercise intensities for the experimental protocols were determined according to the following method. For the loaded condition, the treadmill grade was set at 2 % below the grade that elicited ventilatory threshold during the loaded graded exercise test. This \({\dot{\text{V}}}\)O2 value was considered the “target \({\dot{\text{V}}}\)O2” for the experimental trials. Linear regression established the relationship between oxygen uptake and treadmill grade from the unloaded test, and subsequently, the regression equation was used to solve for the grade (unloaded) that corresponded to the target \({\dot{\text{V}}}\)O2. Treadmill speed was the same as the walking pace during the graded exercise test and remained constant (1.5 m s−1) throughout the prolonged exercise bouts for both conditions.
Experimental protocol
Subjects were randomly assigned to either the loaded or unloaded condition for the first trial. During the experimental protocol, subjects completed 45 min of exercise at a constant speed (1.5 m s−1) and grade. As described above, the treadmill grade for each condition was pre-determined and verified during the practice to ensure that \({\dot{\text{V}}}\)O2 was matched between conditions. Subjects completed a brief warm-up and cool-down before and after exercise. Inspiratory capacity maneuvers were completed at baseline and at 5-minute intervals during exercise. Perceptual responses (exercise stress, breathing discomfort and leg fatigue) were recorded in the first 5-minute measurement cycle and were repeated every 10 min throughout the experimental trial. Blood pressure was taken by auscultation at rest and at 5, 25 and 45 min of exercise during the experimental protocol.
Deadspace ventilation
Deadspace ventilation was calculated from the difference between minute ventilation and alveolar ventilation (\({\dot{\text{V}}}\) A) (West 2008). Alveolar ventilation was estimated using the equation:
The K is a conversion factor and is used to adjust \({\dot{\text{V}}}_{\text{A}}\) to body temperature and pressure. Due to the difficulty of determining arterial carbon dioxide partial pressure (PaCO2), pressure of end-tidal carbon dioxide (PETCO2) was assumed to be equal to PaCO2 (Stickland et al. 2013).
End-tidal CO2 was measured (R-1 pump, P-61B sensor and CD-3A CO2 analyzer, AEI technologies Naperville, IL, USA) from a small port off of the mouthpiece collected through a drying line. End-tidal CO2 data were recorded with a data acquisition system (Powerlab 8/35, AD Instruments, New South Wales, Australia) and displayed in real-time on a laptop computer.
Lung volume
Changes in operating lung volume were estimated from measurements of inspiratory capacity (IC) taken at rest and at 5-minute intervals during exercise. An inspiratory pneumotach attached to the two-way breathing valve was used to measure inspired volume. End-expiratory lung volume was calculated by subtracting IC from TLC obtained at rest. It was assumed that TLC does not change with exercise (O’Donnell et al. 2001). End-inspiratory lung volume was then estimated by adding V T and EELV. Tidal volume was recorded in the minute leading up to the IC maneuver and then averaged. Changes in EELV and EILV were expressed as a percentage of TLC. The determination of operating lung volume is dependent on the correct performance and analysis of the IC maneuver. To improve the likelihood of valid and reliable results, each subject had extensive practice of the IC maneuver prior to the experimental protocols. During analysis, volume was corrected for any pneumotachometer drift that may have occurred by selecting six breaths prior to the maneuver and “zeroing” end-expiratory volume (Johnson et al. 1999; Dominelli et al. 2012).
Maximal voluntary respiratory muscle pressures
Maximal voluntary inspiratory pressure (MIP) and maximal voluntary expiratory pressure (MEP) were measured as indices of respiratory muscle strength before exercise and within 4 min of exercise completion. Maximal inspiratory and expiratory pressures were measured by having the subject produce a maximal inspiration or expiration through a mouthpiece into an occluded rigid tube (Butcher et al. 2007). A small leak (1 mm diameter) was used to prevent glottis closure. The tube was attached to a positive or negative pressure gauge (Cole Parmer Co, Stratford, USA). Measurement of MIP was initiated at residual volume (RV) and MEP at TLC. Measurements were repeated until there were two maximal values within 5 cmH2O. It is well known that maximal volitional pressures are highly dependent on subject motivation and effort. However, each subject had a comprehensive familiarization and numerous opportunities to practice the technique prior to the experimental trials.
Perceptual responses
Perceived exercise stress, breathing discomfort and leg fatigue were measured using three separate 11-point systems. The scales were anchored such that 0 represented “no exercise stress, breathing discomfort or leg fatigue” and 10 represented “maximal exercise stress, breathing discomfort or leg fatigue.” (Borg 1982; O’Donnell et al. 2000).
Core temperature
For the first 10 subjects, core temperature was monitored continuously by telemetry and recorded at 5-minute intervals (VitalSense™, Mini Mitter, Bend, OR). The temperature capsule was ingested 5 h prior to the start of the experimental trial.
Data analysis
Data are presented as mean ± standard error (SE) unless otherwise indicated. Two-way, repeated-measures analysis of variance (ANOVA) was used to detect any differences within and between the loaded and unloaded conditions at rest and 5-minute intervals during exercise. If a significant change or interaction effect was found, Tukey’s post hoc test was used to locate each difference. Student’s t test was used to detect any differences in pulmonary function, MIP and MEP, and peak exercise data between conditions. All statistical analyses were performed using Sigma Plot Software version 12.0 (Systat Software Inc., Chicago, USA). Significance was set a priori at P < 0.05.
Results
Table 1 shows the pulmonary function and graded exercise test results, in both unloaded and loaded conditions. All subjects had normal spirometry values. As shown in Table 1, there were small but significant reductions in forced vital capacity (FVC), forced expired volume in 1 s (FEV1) and peak oxygen consumption (\({\dot{\text{V}}}\)O2peak) when subjects were tested with the 25 kg pack.
Table 2 displays the responses during the 45 min experimental trials. Oxygen consumption was the same (approximately 66 % VO2peak) for both conditions through the experimental trials with the exception of a small increase in the loaded condition at 45 min compared to the unloaded condition. Respiratory exchange ratio, core temperature and blood pressure were not different between conditions at any point during the experimental trials. All subjects exercised at a constant treadmill speed (1.5 m s−1), however, treadmill grade was always significantly higher in the unloaded condition (15.6 ± 0.7 vs. 9.1 ± 0.5 %) between unloaded and loaded conditions, respectively.
Gas exchange and lung volumes
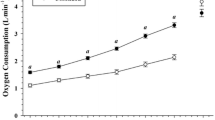
In the loaded condition, minute ventilation became significantly higher than the unloaded condition at 25 min and remained higher thereafter. As expected, the difference became greater over time throughout the exercise trial (Fig. 1a). Calculated deadspace ventilation was the same between conditions during the first 25 min of exercise; however, it became significantly higher at 30 min. Similar to minute ventilation, the difference between conditions became greater over time throughout the exercise trial (Fig. 1b).

Mean (±SE) minute ventilation (a), deadspace ventilation (b) and breathing frequency (c) during exercise in loaded (closed circles) and unloaded (open circles) conditions. Lower case letter “a” indicates significant difference (P < 0.05) between conditions; lower case letter “b” indicates significant difference between 15 and 45 min within conditions, n = 15
Breathing frequency progressively increased within both conditions throughout the experimental trials. Breathing frequency was significantly higher in the loaded condition compared to unloaded after 10 min and the difference became greater over time (Fig. 1c). In the loaded condition, V T decreased throughout the exercise trial with a significant decrease between conditions occurring at 35 min. In the unloaded condition, V T did not change throughout the experimental trial (Fig. 2).

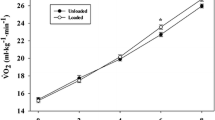
Mean (±SE) resting and operating lung volume in loaded (closed symbols) and unloaded (open symbols) conditions, shown as a percentage of the measured total lung capacity. Lower case letter “a” indicates a significant difference (P < 0.05) in EILV (end-inspiratory lung volume) between conditions; lower case letter “b” indicates a significant difference in EELV (end-expiratory lung volume) between conditions, n = 15
At rest, loaded EELV and EILV were 15.1 and 8.5 % lower compared to the unloaded condition, indicating that subjects were breathing at a lower lung volume. End expiratory lung volume was not different between conditions and did not change within either condition during the exercise trials (Fig. 2). Inspiratory capacity was also not different between conditions and did not change within either condition throughout the exercise trials. End inspiratory lung volume was significantly lower in the loaded condition at 15 min and again at 35 min until the end of exercise compared to the unloaded condition. In summary, the decrease in V T during loaded exercise was the result of decreased EILV while EELV remained constant.
Respiratory muscle strength
Prior to exercise, MIP and MEP values were the same in both conditions. Table 3 illustrates that after 45 min of exercise, MIP decreased significantly in the loaded condition compared to the pre-exercise value. We found no associations between the change in MIP following loaded exercise and either body size or fitness. There was no change in MEP values between pre and post exercise in the either condition or in MIP in the unloaded condition.
Perceptual responses
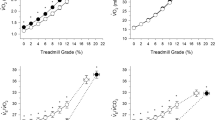
Perceived exercise stress, breathing discomfort and leg fatigue were significantly higher in the loaded condition at 25 and 45 min, respectively, compared to the unloaded condition, with the differences becoming greater over time (Table 2). Breathing discomfort increased proportionally to increased ventilation in both conditions (Fig. 3).

Mean (±SE) breathing discomfort compared to minute ventilation during exercise in loaded (closed circles) and unloaded (open circles) conditions, n = 15
Discussion
Major findings
The major findings from this experiment are twofold. First, while the ventilatory response to short duration (up to 10 min) exercise was similar between unloaded and loaded conditions at matched oxygen demand, sustained exercise resulted in a progressive alteration in operating lung volume and development of a rapid and shallow breathing pattern. These changes were likely compensatory adjustments to minimize the increased elastic work of breathing. However, this pattern increased deadspace and minute ventilation, leading to altered perceptions of exercise stress and breathing discomfort. Second, the extra burden placed on the respiratory system during prolonged exercise with thoracic load carriage resulted in decreased maximal inspiratory muscle strength immediately following exercise, which is suggestive of respiratory muscle fatigue.
Ventilatory responses to thoracic load carriage
We found no difference in operating lung volume or minute ventilation between conditions in the first 10 min of exercise at matched oxygen demand. To our knowledge, we are the first to demonstrate the ventilatory response to exercise when oxygen demand is matched, between unloaded and loaded conditions. Dominelli et al. (2012) observed a decrease in EELV during very brief exercise (2.5 min), at fixed external workloads, with various loads ranging from 15 to 35 kg. In their experiment, treadmill speed and grade were consistent for all conditions, resulting in significantly greater oxygen demand for the loaded conditions. Therefore, it is likely that the decreased EELV observed in their study may be partly explained by the increased metabolic rate and thus the greater increase in tidal volume to achieve higher minute ventilation compared to the unloaded control. The novel result from our study is the similarity in EILV and EELV between conditions in the first 10 min of exercise suggesting that at the onset of exercise there was little effect of thoracic load carriage on operating lung volumes and minute ventilation. It is likely that during short-term exercise, the respiratory system can overcome the extra load placed on the thorax and avoid compensatory alterations in operating lung volume and ventilation. However, as exercise continued, compensatory changes in ventilatory responses were required.
The rise in minute ventilation in the loaded condition appears to be driven mainly by a progressive increase in f B and decrease in V T and is characteristic of a rapid and shallow breathing pattern. The progressive rapid, shallow breathing may have been adopted as a strategy to minimize the elastic work of breathing. In the final 15 min of exercise, there was a significant increase in deadspace ventilation in the loaded condition, which logically would lead to a corresponding increase in minute ventilation to maintain alveolar ventilation. The increased minute ventilation would have placed an additional load on the respiratory muscles and likely resulted in higher work of breathing (Dominelli et al. 2012; Sheel et al. 2002; Tomczak et al. 2011).
Minute ventilation has been shown to increase during prolonged unloaded exercise (Hopkins et al. 1998; Stickland et al. 2004) and/or in response to heat stress (White 2006). Core temperature and systemic blood pressure were the same between conditions throughout the experimental trials (Table 2). These results provide assurance that any changes in ventilatory responses to exercise between conditions were likely due to the backpack and not secondary to differences in thermal, hemodynamic or metabolic state.
Respiratory muscle strength
Maximal voluntary inspiratory muscle pressure was significantly reduced (7 %) after 45 min of exercise in the loaded condition only, while there were no changes in expiratory muscle pressure in either condition (Table 3). The reduction in MIP is suggestive of inspiratory muscle fatigue, presumably related to load carriage because there were no changes following exercise in the unloaded condition. Our results differ from Faghy and Brown (2014) who demonstrated a decrease in maximal inspiratory (11 %) and expiratory pressure (13 %) generation after 60 min of light exercise with thoracic load carriage (25 kg). Faghy and Brown (2014) interpreted their observation of decreased respiratory muscle strength as global respiratory muscle fatigue. The decrease in inspiratory muscle strength in the current study is suggestive of peripheral muscle fatigue rather than whole-body reductions in motor output from the central nervous system. Reductions in both inspiratory and expiratory muscle strength would be expected with central fatigue. Respiratory muscle fatigue has been defined as an exercise-induced reduction in respiratory muscle force generation (Sheel and Romer 2012). It is impossible to determine precisely when inspiratory muscle strength decreased in the current study; however, the progressive changes in breathing pattern, decreased EILV and increased minute ventilation suggest a compensatory strategy to minimize inspiratory elastic work. Further study is required to precisely quantify respiratory muscle fatigue during prolonged exercise under load using techniques such as bilateral phrenic nerve simulation.
Perceptual responses
While breathing discomfort was greater during the loaded condition in the final 20 min of exercise, the breathing discomfort vs. minute ventilation pattern was the same in both conditions (Fig. 3). The results illustrate that increased perception of breathing discomfort during the loaded condition is likely secondary to the increase in minute ventilation. Measuring work of breathing at similar ventilation rates could aid our understanding of the relationship between ventilatory mechanics and perceived breathing discomfort during prolonged exercise with heavy load carriage.
It is also possible that the increased perception of exercise stress in the loaded condition is the result of greater muscle recruitment throughout the body. Previous research suggests that rectus abdominis muscle activity increases when carrying heavy load carriage (Al-Khabbaz et al. 2008). The increase in muscle recruitment and change in posture during exercise with heavy load carriage could contribute to the greater perceived exercise stress. Our results show that perceptions of exercise stress and leg fatigue are greater with heavy load carriage despite matched oxygen demand with the unloaded control.
Pulmonary function
The small reductions in FVC and FEV1 are consistent with previous reports of resting spirometry with and without backpacks (Muza et al. 1989; Dominelli et al. 2012). At rest, TLC was the same between loaded and unloaded conditions. The increased transpulmonary pressure as a result of chest wall loading is known to increase closing volume and effectively increase closing capacity (West 2008). This may explain why forced expired flow volumes were decreased even though TLC did not change while wearing the pack.
Heart rate during exercise with heavy load carriage
An interesting finding of this experiment was that during loaded exercise heart rate was always higher than the unloaded condition at matched oxygen demands (Table 2). Assuming that cardiac output was not significantly different between conditions, it is possible that the elevated heart rate in the loaded condition is indicative of a corresponding reduction in stroke volume. One possible explanation could be that the load on the thorax altered intra-thoracic pressure swings and consequently, either preload and/or afterload (Miller et al. 2006; Nelson et al. 2009). Sagiv et al. (1994) suggested that left ventricular function was maintained during prolonged exercise in two heavy load carriage conditions (38 and 50 kg); however, the highest metabolic rate was less than 30 % \({\dot{\text{V}}}\)O2max and changes in cardiac output, between conditions, were due entirely to HR. Unfortunately in that experiment there was no unloaded control condition and the results do not help to explain our observations. Further research will be required explain the cardiovascular implications of heavy load carriage.
Methodological considerations
We have suggested that altered ventilatory responses during prolonged thoracic load carriage were the result of altered energy cost of breathing; however, because we did not measure intra-thoracic pressures, this suggestion remains speculative. Further research will be required to quantify the effect of prolonged thoracic load carriage on ventilatory mechanics and objectively assess respiratory muscle fatigue.
Conclusion
The results of this study demonstrate the impact of heavy load carriage on the respiratory system during 45 min of exercise. Breathing pattern, operating lung volume and minute ventilation were altered to support exercise in the loaded condition and apparently the extra load placed on the thorax burdened the inspiratory muscles. The disadvantage placed on the respiratory system and the ventilatory responses to exercise under load are suggestive of respiratory muscle fatigue, which could have implications for physically demanding occupations. If the work is time sensitive and load carriage is required for a prolonged period, the ventilatory impairments could intensify breathing and peripheral muscle discomfort and ultimately decrease occupational effectiveness and safety.
Abbreviations
- fB :
-
Breathing frequency
- EELV:
-
End expiratory lung volume
- EILV:
-
End inspiratory lung volume
- FEV1 :
-
Forced expired volume in 1 s
- FVC:
-
Forced vital capacity
- IC:
-
Inspiratory capacity
- MIP:
-
Maximal inspiratory pressure
- MEP:
-
Maximal expiratory pressure
- TLC:
-
Total lung capacity
- VC:
-
Vital capacity
- \({\dot{\text{V}}}\)CO2 :
-
Carbon dioxide production
- \({\dot{\text{V}}}\)O2 :
-
Oxygen consumption
- V T :
-
Tidal volume
References
Abe D, Yanagawa K, Niihata S (2004) Effects of load carriage, load position, and walking speed on energy cost of walking. Appl Ergon 35(4):329–335
Al-Khabbaz YSSM, Shimada T, Hasegawa M (2008) The effect of backpack heaviness on trunk-lower extremity muscle activities and trunk posture. Gait Posture 28(2):297–302
American Thoracic Society (2005) Standardization of spirometry. Eur Respir J 26:319–338
Beekley MD, Alt J, Buckley CM, Duffey M, Crowder TA (2007) Effects of heavy load carriage during constant-speed, simulated, road marching. Mil Med 172(6):592–595
Borg GA (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14(5):377–381
Butcher SJ, Rl Jones, Mayne JR, Hartley TC, Petersen SR (2007) Impaired exercise ventilatory mechanics with the self-contained breathing apparatus are improved with heliox. Eur J Appl Physiol 101(6):659–669
Dominelli PB, Sheel AW, Foster GE (2012) Effect of carrying a weighted backpack on lung mechanics during treadmill walking in healthy men. Eur J Appl Physiol 112(6):2001–2012
Faghy MA, Brown PI (2014) Thoracic load carriage-induced respiratory muscle fatigue. Eur J Appl Physiol 114(5):1085–1093
Hopkins SR, Gavin TP, Siafakas NM, Haseler LJ, Olfert IM, Wagner H, Wagner PD (1998) Effect of prolonged, heavy exercise on pulmonary gas exchange in athletes. J Appl Physiol 85(4):1523–1532
Johnson BD, Weisman IM, Zeballos RJ, Beck KC (1999) Emerging concepts in the evaluation of ventilatory limitation during exercise: the exercise tidal flow-volume loop. Chest 116(2):488–503
Miller JD, Hemauer SJ, Smith CA, Stickland MK, Dempsey JA (2006) Expiratory threshold loading impairs cardiovascular function in health and chronic heart failure during exercise. J Appl Physiol 101:213–227
Muza SR, Latzka WA, Epstein Y, Pandolf KB (1989) Load carriage induced alterations of pulmonary function. Int J Ind Ergon 3(3):221–227
Nelson MD, Haykowsky MJ, Mayne JR, Jones RL, Petersen SR (2009) Effects of the self-contained breathing apparatus on ventricular function during strenuous exercise. J Appl Physiol 106:395–402
O’Donnell DE, Hong HH, Webb KA (2000) Respiratory sensation during chest wall restriction and dead space loading in exercising men. J Appl Physiol 88(5):1859–1869
O’Donnell DE, Revill MR, Webb KA (2001) Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am J Respir Crit Care Med 164(5):770
Patton JF, Kaszuba J, Mello RP, Reynolds KL (1991) Physiological responses to prolonged treadmill walking with external loads. Eur J Appl Physiol 63(2):9–93
Sagiv M, Ben-Sire D, Sagiv A, Werber G, Rotstein A (1994) Left ventricular responses during prolonged treadmill walking with heavy load carriage. Med Sci Sports Exerc 3:285–288
Sheel AW, Romer LM (2012) Ventilation and respiratory mechanics. Compr Physiol 2(2):1093–1142
Sheel AW, Derchak PA, Pegelow DF, Dempsey JA (2002) Threshold effects of respiratory muscle work on limb vascular resistance. Am J Physiol Heart Circ Physiol 282(5):H1732–H1738
Stickland MK, Anderson WD, Haykowsky MJ, Welsh RC, Petersen SR, Jones RL (2004) Effects of prolonged exercise to exhaustion on left-ventricular function and pulmonary gas exchange. Respir Physiol Neurobiol 142(2–3):197–209
Stickland MK, Lindinger MI, Olfert IM, Heigenhauser GJF, Hopkins SR (2013) Pulmonary gas exchange and acid-base balance during exercise. Compr Physiol 3(2):693–739
Taylor NAS, Lewis MC, Notley S, Peoples GE (2012) A fractionation of the physiological burden of the personal protective equipment worn by firefighters. Eur J Appl Physiol 112(8):2913–2921
Tomczak SE, Guenette JA, Reid WD, McKenzie DC, Sheel AW (2011) Diaphragm fatigue after submaximal exercise with chest wall restriction. Med Sci Sports Exerc 43(3):416–424
Wasserman K (1987) Determinants and detection of anaerobic threshold and consequences of exercise above it. Circulation 76(6):29–39
West JB (ed) (2008) Respiratory physiology: the essentials, 8th ed. Baltimore, MD
White MD (2006) Components and mechanisms of thermal hyperpnea. J Appl Physiol 101:655–663
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
There are no conflicts of interest.
Additional information
Communicated by Susan Hopkins.
Rights and permissions
About this article

Cite this article
Phillips, D.B., Stickland, M.K. & Petersen, S.R. Ventilatory responses to prolonged exercise with heavy load carriage. Eur J Appl Physiol 116, 19–27 (2016). https://doi.org/10.1007/s00421-015-3240-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00421-015-3240-7