
Abstract
Objective
This study aims to investigate the association between the diurnal temperature range (DTR) and allergic rhinitis (AR) outpatient visits in Lanzhou, China, utilizing more than 7 years of participant surveys.
Methods
Our study used the distributed lag non-linear model (DLNM) aimed to evaluate the association between DTR and AR outpatient visits. We also performed subgroup analyses in order to find susceptible populations by gender and age groups.
Results
In 2013–2019, DTR in Lanzhou demonstrates a non-linear correlation with outpatient visits for AR, which is S-shaped. In addition, when DTR was located in the 0.9–5.3 °C and 12–20 °C compared with 12 °C, the risk of outpatient visits for AR increased. Moreover, males appeared to be more vulnerable to the DTR effect than females, the risk of children visits exceeded both the adult and the elderly groups at the higher DTR.
Conclusion
Our study adds to the evidence that DTR is a possible risk factor for outpatient visits for AR; therefore, the public health sector and medical staff should take DTR into account when it comes to preventing AR onset.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Allergic rhinitis (AR) is an IgE-mediated inflammatory reaction condition of the nasal mucosa (Kakli and Riley 2016), which predominantly manifests as nasal obstruction, itching, a runny nose, and sneezing. It is often accompanied by allergic conjunctivitis. AR may induce asthma and may aggravate adenoid hypertrophy in children (Evcimik et al. 2015; Khan 2014; Okubo et al. 2017). Epidemiological studies show that AR significantly impacts the health of many adults and children globally, claiming a prevalence of 10–40% (de Marco et al. 2012; Pawankar et al. 2012). A multi-city research in China found that its prevalence 8.7–34.3%, which is continually rising (Zhang 2014). The World Allergy Organization (WAO) white book on allergy, Update shows that AR has a significant socioeconomic impact on patients and their family members, and the general society; it reported its serious impact on patients’ quality of life, as well as their physical, psychological, and social functions (Pawankar et al. 2013).
The occurrence of AR is mainly affected by the interaction of genetic and environmental meteorological factors (Kim et al. 2018). Considering the stability and uncontrolled ability of genetic factors, environmental meteorological factors play an increasingly important role in the onset of AR. Many studies have found that the onset of AR is often seasonal and closely related to environmental meteorological factors. Among many meteorological factors, temperature change has the most significant impact on human health. There is a threshold interval for the effect of temperature on human health. When the adaptive capacity of the human body cannot bear the impact of temperature changes, the stress response of the physical functions will become induced in some people, leading to the occurrence or worsening of corresponding diseases. The temperature change has a direct impact on the incidence rate of various respiratory diseases, such as asthma (Hu et al. 2022; Wei et al. 2020), pneumonia (Xu et al. 2014), and bronchitis (Xie et al. 2017). However, there are few studies that focus on the relationship between temperature change and the onset of AR. Moreover, by comprehensively looking into published studies, the daily temperature range (DTR), which reflects the change of temperature within a day, has been found to be related to the occurrence of diseases as well as respective deaths.
DTR refers to the difference between the maximum and the minimum temperatures in 1 day. It is used to indicate the range of daily temperature changes and is one of the indicators that reflect short-term temperature changes. At present, there have been some studies on the relationship between DTR and respiratory diseases globally; however, most studies focus on the influence of DTR on mortality from a respiratory diseases’ perspective, and less from the perspective of the relationship between DTR and the incidence of allergic rhinitis.
Lanzhou City is deeply located in the northwest region of China and belongs to a typically temperate continental semi-arid climate. It has remarkable climate characteristics such as a late spring, short summer, early autumn, long winter, drought seasons, and a large DTR. Up to now, there has been no report on the impact of temperature in Lanzhou, especially regarding DTR, on the number of outpatients with allergic rhinitis. This study explored the exposure–response relationship between the DTR and the number of outpatient visits to allergic rhinitis clinics in Lanzhou using the distributed lag non-linear model. This study intends to provide a scientific basis for formulating effective intervention measures and reducing health problems induced by temperature changes.
Materials and methods
Study area
Lanzhou (36°03 N, 103°4 E) is situated in the middle of Gansu Province, with four districts, the city territory is geographical orientated on the slopes of the mountains and descends from the southern side to the northern side with a 40 km urban line stretching along the river from the west to the east (see Supplementary S.Fig. 1). Lanzhou has a typical temperate semi-arid climate with four distinct seasons, and large temperature difference between day and night, morning or evening and daytime, and thus, the extreme temperatures–diseases relationship in Lanzhou needs particular research attention.
Data collection
According to the outpatient visits and geographical location of general hospitals in Lanzhou, all outpatient visit records for patients seeking care for AR records were obtained from three large general hospitals between 2013 and 2019 (Fig. 1). Affected by the topography of Lanzhou City, the settlement is mainly spread in a strip from east to west, and these three hospitals are seated in the central districts with convenient transportation, which are surrounded by densely populated residential areas. These hospitals are also one of the highest level hospitals for allergic diseases, and they cover the largest number of patients in the city. We selected these three hospitals for this study mainly due to their reputable levels of medical care, sophisticated medical departments, and their proven capabilities to diagnose and treat patients with allergic diseases. The collected outpatient data were intact with no missing values.

The locations of air pollutants monitoring stations and hospitals
All patients with allergic rhinitis were diagnosed according to the 10th edition of the International Classification of Diseases (ICD-10) code J30. The record includes general personal information (gender, age, and address), the date of outpatient visits, clinical diagnosis, and ICD code.
We obtained hourly data on air pollutants (particles < 2.5 μm [PM2.5], particles < 10 μm [PM10], sulfur dioxide [SO2], and nitrogen dioxide [NO2], from 3 monitoring sites operated by Lanzhou Ecological Environment Bureau for the same period (Fig. 1), and the average of the above three air quality monitoring stations in Lanzhou was used as the daily mean concentrations for each pollutant. Daily meteorological data including daily mean temperature, minimum temperature (Tmin), maximum temperature (Tmax), and mean relative humidity (RH) were obtained from Gansu Meteorological Bureau for the same period. DTR was calculated by the maximum temperature minus the minimum temperature within the same day.
Statistical analyses
Since Daily AR outpatient visits are generally regarded as rare events, which approximately obey a Poisson distribution. Meanwhile, previous studies reported that there is a delay and a non-linear effect of DTR on AR (Song et al. 2018; Wang et al. 2020). Thus, we used the distributed lag non-linear model (DLNM) based on the Poisson generalized additive model to assess and analyze the effect of DTR on daily outpatient visits for AR and DTR.
A model was built, in which mean temperature, relative humidity, air pollutants (PM2.5, SO2, and NO2), long-term trend, day of the week (DOW) and public holiday (Holiday) were considered as the potential confounders, suggested by the results of Spearman correlation analysis, and previous studies (Song et al. 2018; Wang et al. 2020). We examined the relationship between each environmental factor and AR case using Spearman correlation analysis. According to the results of Spearman correlation analysis, Spearman’s correlation coefficients < 0.8 were used to select covariates to avoid multicollinearity, and considering the co-linearity of PM10 and PM2.5, we excluded PM10 in the model. Finally, we selected those factors that were significantly associated with the AR case into the main model, which included temperature, relative humidity, PM2.5, SO2, and NO2. Spearman correlations of different meteorological factors, air pollution, and AR case are shown in Table 2. The model used in the analysis was as follows:
where α is the intercept, t denotes the data of observation, μt represents the observed daily outpatient visits for AR on day t; DTRt,l is the matrixes produced by DLNM to model DTR; l represents the lag days, β represents the vector of the coefficients for DTRt,l, ns means a smooth function based on the natural cubic spline, df represents the degree of freedom (df), and we used “natural cubic spline–natural cubic spline” DLNM for cross-basis between DTR and lag function to investigate non-linear and lagged effects of DTR on AR. Temt is the daily average temperature on day t; rht is the daily average relative humidity on day t; PM2.5t, SO2t, and NO2t are the daily average concentrations of air pollutants on day t. The “Timet” variable was used to control for unmeasured long-term trends and seasonal trends, Dow is an indicator for the day of the week, and Holiday represents a binary variable for the public holiday.
We used the minimum value of the Akaike information criterion for Poisson models to determine the best df values for the models. Thereafter, the dfs for DTR and lag were set to 3, and we chose 7 df per year for temporal trends and 3 df for the daily mean temperature, relative humidity, and PM2.5, SO2, and NO2.
According to the preliminary analysis, the effects of DTR on AR outpatient visits could persist for 21 days (Song et al. 2018), so we calculated the relative risk of DTR with lags up to 21 days. Based on previous studies (Xu et al. 2013b), the median value of DTR was defined as the reference for calculating all the relative risk (RR) and 95% confidence intervals (CIs). Thus, we chose median value of DTR (12 °C) as the reference for calculating all the relative risk. The 5th percentile (4 °C) and 95th percentile (18 °C) of the DTR were then chosen as the model low and high DTR for comparison, respectively. Due to the potentially delayed harmful impacts of DTR, we also analyzed the relative risk (RR) and 95% confidence interval (CI) of the 5th and 95th percentiles of DTR compared with the reference value in single-day lag effects (lag0 ~ lag21) and cumulative-lag effects (lag0–1 ~ lag0–21).
Finally, a subgroup analysis incorporating both gender and age was completed. We divided the OPD visits datasets into subgroups according to gender (male vs. female) and age (child, 0–14 years; adult, 14–60 years; and elderly, ≥ 60 years), after that, we analyzed the effects of DTR on OPD visits for AR in each subgroup respectively.
All the statistical analyses were performed using the R (version 4.0.2) software; the DLNM was built using the “dlnm” package (version 2.4.2); the Spearman’s rank correlation statistic was used, and P < 0.05 was considered to be statistically significant.
Results
Table 1 shows the basic characteristics of daily AR outpatient visits, meteorological factors, and ambient air pollutants in Lanzhou, China, from 2013 to 2019. There was a total of 50,602 outpatient visits with AR during the study period, with a daily mean of 20 cases. Male, female, children (0–14 years), adult (15–59 years), and elderly (≥ 65 years) were 9, 10, 5, 10, and 5 cases per day, respectively. Daily average values of DTR, temperature and relative humidity were, respectively, 11.50 °C, 11.39 °C, and 50.63% during the study period. Moreover, those of PM2.5, PM10, SO2, and NO2 were 50.33, 113.82, 22.54, and 45.51 μg/m3, respectively.
To explore the relationship between each variable, we calculated the Spearman correlations between meteorological variables, air pollutants, and daily AR outpatients (Table 2). The results of Spearman rank correlation analysis showed that the daily AR outpatient visits were moderately positively correlated with temperature, DTR, relative humidity, PM2.5, PM10, SO2, and NO2. DTR was positively correlated with Tmax, PM10, and PM2.5 while being negatively correlated with relative humidity. Although DTR has a positive relationship with Tmin, there is no comparison.
Figure 2 shows the three-dimensional relationship between DTR and AR outpatient visits by lag period (lag 0–21st days) with the reference DTR of 12 °C. The effect of DTR on hospital outpatient visits for AR was non-linear, both low and high ambient DTR could increase the frequency of daily AR outpatient visits.

Three-dimensional graphs of RR along diurnal temperature range (DTR) and lags, with reference at 11.6 °C
Figure 3 depicts the overall cumulative effect (21 days) of DTR on daily outpatient visits for AR. It suggested that DTR was significantly associated with AR outpatient visits. The curve is S-shaped, in addition, compared with 12 °C, the risk of outpatient visits for AR increased when DTR is in interval DTR of 0.9–5.3 °C and 12–20 °C, with the peak at 0.9 °C (RR 4.102, 95% CI 2.353–7.151%) and 16.6 °C (RR 2.095, 95% CI 1.740–2.522%). Subsequently, we calculated the number of days when DTR in 0.9–5.3 °C was mostly in winter, while the DTR in 12–20 °C was mostly in summer (S.Fig. 2).

Overall effects of exposure–response associations between DTR change and daily outpatient visits for AR
Table 3 shows the lag effects for DTR of low DTR (4 °C) and high DTR (18 °C) with the reference of 12 °C. For low DTR, the lag effect initially appeared on lag day 9 (RR 1.102, 95% CI 0.995–1.029) and the risk elevation generally lasted for 21 days (RR 1.060, 95% CI 1.034–1.087). The cumulative-lag effect of the AR outpatient visits was significant only at lag 0–21 (RR 1.851, 95% CI 1.473–2.326). For high DTR, the lag effect of AR outpatient visits decreased from lag 0 (RR 1.019, 95% CI 0.988–1.051) to lag 6 (RR 1.006, 95% CI 0.992–1.020), and then it starts to go up until lag 21 (RR 1.080, 95% CI 1.056–1.106). The cumulative-lag effect of AR outpatient visit decreased from lag 0 (RR 1.019, 95% CI 0.988–1.051) to lag 0–3 (RR 1.055, 95% CI 0.963–1.156) and then starts to rise until lag 0–21 (RR 1.851, 95% CI 1.473–2.326).
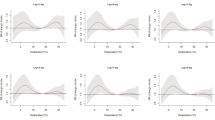
Figure 4 illustrates the cumulative effects of DTR on the gender-specific and age-specific AR over 21 days. The curve is also S-shaped. The risk of AR visits among male and female individuals reached a peak when DTR was at 0.9 °C, followed by a second peak at 16.6 °C; however, the male risk (RR 2.172, 95% CI 1.764–2.674) was higher than that of females (RR 2.022, 95% CI 1.659–2.464). In the stratification of age, the first peak DTR was at 0.9 °C in children, adults and children. Notably, the risk of OUTPATIENT visits among children had no statistical significance (RR 1.349, 95% CI 0.581–3.130). The second peak of DTR was about 17.5 °C in children (RR 2.311, 95% CI 1.688–3.162), 16.6 °C in adults (RR 2.805, 95% CI 1.728–2.517), and 18.1 °C in the elderly (RR 1.565, 95% CI 1.100–2.227).

The overall relative risks of DTR for gender- and age-specific AR cases over 21 days
Discussion
In this study, the DLNM model was used to elaborate the effect of DTR on outpatient visits for AR in Lanzhou. In this way, the results revealed a non-linear relationship between the DTR and the AR patient volumes. Especially when DTR was between 0.9–5.3 °C and 12–20 °C, compared with 12 °C, the risk of outpatient rate increased. Although the underlying mechanism remains unclear, these possibilities cannot be ruled out. When the DTR is 0.5–5.3 °C, the weather tends to be relatively more cloudy and rainy (Davis et al. 2020) in Lanzhou. During this time, people prefer to live and work indoors, increasing the likelihood of contact with dust mites from carpets, sofas and mattresses. When the DTR is 12–20 °C, commonly occurring in summer, light and temperature are more coordinated and there is sufficient water, which are ideal conditions for the growth of autumn crops and fruits. Crimi found that an increase in DTR could dehydrate pollen, reduce its mass and help it spread by wind, while the lightness and volatility of the grain would be ascertained for ultimately diffusing in the atmosphere if there is significant wind speed (Crimi et al. 2004). However, in Lanzhou, this needs further study. Besides that, Graudenz et al. (2006) declared that the sudden changes in the temperature of inhaled air might lead to a more pronounced inflammatory nasal response in the rhinitis group through the recruitment and activation of eosinophils. Diesel et al. (1991) noticed that the decline in the temperature of respiratory epithelium would weaken the effectiveness of local respiratory defence, such as mucociliary clearance and leukocyte phagocyte. However, Professor Xu did not catch sight of the correlation of the incidence of AR and DTR value, which might be due to the lower DTR in Hefei (8.4 ± 3.9 °C) compared with Lanzhou (11.50 ± 4.28 °C) in our study (Wang et al. 2020).
The single-day lag effect and cumulative-lag effect of extremely low DTR on outpatient visits for AR was longer compared with the extremely high DTR, which is consistent with the study of Ye et al. (2012). As mentioned above, the extremely low DTR relates to more cloudy and rainy weather, or winter, and it may take a few days to induce the subsequent symptoms in AR with underlying conditions. People are not willing to consult a doctor; thus, there may be another delay between the onset of symptoms and obtaining medical attention. However, further research on these lagged effects is still warranted to understand key components of prevention strategies and treatments.
When comparing the differences in susceptibility among genders, we found out that there were a higher fraction of outpatient visits attributable to DTR, in males compared with females. This might be referred to the different biological and physiological characteristics of females and males, and general speaking, males take part in more outdoor activities than females, which means they are easily exposed to hot or cold air. Likewise, the risk of children visits had no statistical significance at the lower DTR, yet at the higher DTR, the risk exceeded both the adults and the elderly groups. One contributing factor is that their breathing rates are faster though their immune system is relatively underdeveloped compared with the adults and the elderly. Another contributing explanation is that they spend more time engaging in vigorous physical activities outside with less self-care (Kim 2004; Xu et al. 2013a).
As per this study, completing self-protection under the specific DTR might be an effective prevention measure for AR patients. Equally important, medical professionals should be made aware of DTR ranges that are associated with the onset of AR to prepare for an influx of patients.
Nevertheless, there are several weaknesses to be acknowledged in this study, First, the prevalence of AR showed marked geographic variation (Wise et al. 2018). Our data, related to allergic rhinitis cases, came from one city only and in the temperate continental climate zones, to avoid representing different geographical zones. Second, there were many other confounding variables, such as, airborne pollen being a risk factor of allergic rhinitis was negligible in our data analyses. Last but not least, this study design was ecologically friendly; in other words, it limited our capacity for causal inference.
Conclusion
The conclusion could be drawn that the risk of outpatient visits existed when DTR was at 0.9–5.3 °C and 12–20 °C, compared with 12 °C, in Lanzhou. Moreover, a lagged effect could be retained when the DTR was extremely low. What is more, DTR had more influence on the risk of male outpatient visits compared with females, and a higher DTR would have a greater impact on children. Our findings highlighted when developing effective health strategies whereupon AR patients should be aware of the influence of a particular DTR in order to take preventive measures.
Data Availability
Some or all data or models generated or analyzed during the study are available from the corresponding author upon reasonable request.
References
Crimi P et al (2004) Correlation between meteorological conditions and Parietaria pollen concentration in Alassio, north-west Italy. Int J Biometeorol 49(1):13–17. https://doi.org/10.1007/s00484-004-0212-8
Davis RE, Hondula DM, Sharif H (2020) Examining the diurnal temperature range enigma: why is human health related to the daily change in temperature? Int J Biometeorol 64(3):397–407. https://doi.org/10.1007/s00484-019-01825-8
de Marco R et al (2012) Trends in the prevalence of asthma and allergic rhinitis in Italy between 1991 and 2010. Eur Respir J 39(4):883–892. https://doi.org/10.1183/09031936.00061611
Diesel DA, Lebel JL, Tucker A (1991) Pulmonary particle deposition and airway mucociliary clearance in cold-exposed calves. Am J Vet Res 52(10):1665–1671
Evcimik MF, Dogru M, Cirik AA, Nepesov MI (2015) Adenoid hypertrophy in children with allergic disease and influential factors. Int J Pediatr Otorhinolaryngol 79(5):694–697. https://doi.org/10.1016/j.ijporl.2015.02.017
Graudenz GS et al (2006) The role of allergic rhinitis in nasal responses to sudden temperature changes. J Allergy Clin Immunol 118(5):1126–1132. https://doi.org/10.1016/j.jaci.2006.07.005
Hu Y, Cheng J, Yin Y (2022) Association of childhood asthma with intra-day and inter-day temperature variability in Shanghai China. Environ Res 204(Pt D):112350. https://doi.org/10.1016/j.envres.2021.112350
Kakli HA, Riley TD (2016) Allergic Rhinitis. Prim Care 43(3):465–475. https://doi.org/10.1016/j.pop.2016.04.009
Khan DA (2014) Allergic rhinitis and asthma: epidemiology and common pathophysiology. Allergy Asthma Proc 35(5):357–361. https://doi.org/10.2500/aap.2014.35.3794
Kim JJ (2004) Ambient air pollution: health hazards to children. Pediatrics 114(6):1699–1707. https://doi.org/10.1542/peds.2004-2166
Kim H, Kim H, Lee JT (2018) Assessing the cold temperature effect on hospital visit by allergic rhinitis in Seoul, Korea. Science Total Environ 633:938–945. https://doi.org/10.1016/j.scitotenv.2018.03.166
Okubo K et al (2017) Japanese guidelines for allergic rhinitis 2017. Allergol Int 66(2):205–219. https://doi.org/10.1016/j.alit.2016.11.001
Pawankar R, Bunnag C, Khaltaev N, Bousquet J (2012) Allergic rhinitis and its impact on asthma in Asia Pacific and the ARIA update 2008. World Allerg Organ J 5(Suppl 3):S212–S217. https://doi.org/10.1097/WOX.0b013e318201d831
Pawankar R, Canonica GW, Holgate ST et al (2013) World Allergy Organization (WAO) white book on allergy, Update 2013. World Allergy Organization, Milwaukee
Song X et al (2018) The impact of heat waves and cold spells on respiratory emergency department visits in Beijing, China. Science Total Environ 615:1499–1505. https://doi.org/10.1016/j.scitotenv.2017.09.108
Wang X, Cheng J, Ling L, Su H, Zhao D, Ni H (2020) Impact of temperature variability on childhood allergic rhinitis in a subtropical city of China. BMC Public Health 20(1):1418. https://doi.org/10.1186/s12889-020-09531-6
Wei Q et al (2020) Diurnal temperature range and childhood asthma in Hefei, China: does temperature modify the association? Science Total Environ 724:138206. https://doi.org/10.1016/j.scitotenv.2020.138206
Wise SK et al (2018) International consensus statement on allergy and rhinology: allergic rhinitis. Int Forum Allerg Rhinol 8(2):108–352. https://doi.org/10.1002/alr.22073
Xie MY et al (2017) Effect of diurnal temperature range on the outpatient visits for acute bronchitis in children: a time-series study in Hefei, China. Public Health 144:103–108. https://doi.org/10.1016/j.puhe.2016.12.016
Xu Z, Huang C, Su H, Turner LR, Qiao Z, Tong S (2013a) Diurnal temperature range and childhood asthma: a time-series study. Environ Health 12:12. https://doi.org/10.1186/1476-069x-12-12
Xu Z, Huang C, Turner LR, Su H, Qiao Z, Tong S (2013b) Is diurnal temperature range a risk factor for childhood diarrhea? PLoS ONE 8(5):e64713. https://doi.org/10.1371/journal.pone.0064713
Xu Z, Hu W, Tong S (2014) Temperature variability and childhood pneumonia: an ecological study. Environ Health 13(1):51. https://doi.org/10.1186/1476-069x-13-51
Ye X, Wolff R, Yu W, Vaneckova P, Pan X, Tong S (2012) Ambient temperature and morbidity: a review of epidemiological evidence. Environ Health Perspect 120(1):19–28. https://doi.org/10.1289/ehp.1003198
Zhang Y (2014) Prevalence of allergic rhinitis in china. Allergy Asthma Immunol Res 6(2):105–113. https://doi.org/10.4168/aair.2014.6.2.105
Acknowledgements
This study was supported by the Science and Technology Plan of Gansu Province (21JR7RA864); Hospital Fund of Lanzhou University First Affiliated Hospital (ldyyyn2020-57).
Author information
Authors and Affiliations
Contributions
KC and JJ contributed to the study conception and design. Material preparation, data collection and analysis were performed by KC and YL. The first draft of the manuscript was written by KC and YW, and all the authors commented on previous versions of the manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Chen, K., Li, Y., Ji, J. et al. Diurnal temperature range impacts on outpatients department visits for allergic rhinitis in Lanzhou, China. Int Arch Occup Environ Health 96, 587–595 (2023). https://doi.org/10.1007/s00420-023-01951-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-023-01951-2