
Abstract
Background
Occupational wood dust causes chronic respiratory health problems as well as a decline in lung function. However, data on the prevalence of chronic respiratory symptoms and lung function parameters among large-scale wood factories workers in Ethiopia producing furniture are limited. The objective of this study was to determine the prevalence of chronic respiratory symptoms, lung function measures, and associated factors among large-scale wood industry workers in Addis Ababa, Ethiopia.
Methods
An institution-based cross-sectional study was conducted among 232 wood workers and 232 controls. Participants for the study were selected using stratified and systematic sampling from soft drink and wood factories. The chronic respiratory symptoms were assessed using a modified American Thoracic Society (ATS) questionnaire, and lung function tests were performed using an Easy on PC spirometer in accordance with the ATS standards for spirometry. The data were imported into Epi-data version 4.4.2 and analyzed with SPSS version 23. Poisson regression, Multivariate linear regression and multivariable logistic regression analysis were used.
Results
The prevalence ratio of overall chronic respiratory symptoms was significantly higher among woodworkers (65.7%) compared to controls (23.3%) in this study (PR = 2.17, 95% CI: 1.51–3.12). Current chronic respiratory symptoms were associated with gender, and previous chronic respiratory disease. Woodworkers had significantly lower Forced vital capacity (FVC) and Forced expiratory volume in the first second (FEV1) when compared to controls.
Conclusion
Woodworkers had a higher prevalence of chronic respiratory symptoms and lower lung function measures, which lowered lung capacity when compared to controls. To reduce workers' exposure to wood dust, engineering control methods should be implemented.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Wood is one of the world's most important renewable natural resources, with an estimated 1700 million m3 of forest extracted for industrial purposes each year (World Health Organization 1995). Every day, at least 2 million people are exposed to wood dust around the world. Moreover, approximately 3.6 million workers in the European Union are exposed to wood (World Health Organization 1995; Kauppinen et al. 2006).
According to the global estimate of occupational accidents and work-related illness 2017, 2.78 million people die each year from work-related accidents and diseases, including woodworkers around the world (Hämäläinen et al. 2017). Occupational respiratory disorders are a serious global public health problem, accounting for up to 30% of all documented work-related deaths and having a 50% prevalence among employees in high-risk sectors, such as mining, construction, and dust-generating works (Fedotov 2011). Approximately 12,000 people die each year as a result of occupational respiratory diseases in industrialized countries such as the United Kingdom (Health and Safety Excutive 2017).
Wood processing from furniture factory caused wood dust and other health hazards. The dust is divided into two groups according to their size: total dust with particle size larger than 10 micron (PM > 10), mainly are soft dust (Rosenberg et al. 2002); and respirable dust with particle size smaller than 10 micron (PM < 10), mainly from hardwood (Schlünssen et al. 2002). In addition, both hardwoods and softwoods are used in furniture factory (World Health Organization 1995). Wood dust exposure has been linked to nasal adenocarcinoma, chronic bronchitis, lung cancer, nasal obstruction, increased risk of respiratory symptoms, and asthma (Alonso-Sardón et al. 2015; Jacobsen et al. 2009; Vallières et al. 2015; Schlünssen et al. 2002; Wiggans et al. 2016). Furthermore, the International Agency for Research on Cancer has classified wood dust as carcinogenic to humans (Group 1) and causes cancer of the nasal cavity, paranasal sinuses, Nasopharyngeal cancer (World Health Organization 1995).
Previous studies from industrial countries have indicated that workers in wood processing sectors exposed to wood dust in their working environment have a greater risk of respiratory complaints than control groups (Bhatti et al. 2011; Jacobsen et al. 2009, 2008; Löfstedt et al. 2017; Neghab et al. 2018; Osman and Pala 2009). A study conducted in Iran showed an increase chronic respiratory symptoms of wheezing, chest tightness, cough, phlegm, dyspnea, and reduced lung function among exposed groups (Neghab et al. 2018). In low- and middle-income countries, including Africa, where there is no effective legislative enforcement to reduce the levels of dust, workers exposed to wood dust might suffer chronic respiratory symptoms, such as persistent cough, sputum, wheezing, chest pain, and associated with a reduction of lung function parameters (Bosan and Okpapi 2004; Ugheoke et al. 2006; Ennin et al. 2015; Tobin et al. 2016). The American Conference of Governmental Industrial Hygienists (ACGIH) recommends an 8-h time-weighted average (TWA) of 1 mg/m3 for hard wood dust and 5 mg/m3 for soft wood dust, while OSHA proposed an 8-h TWA of 1 mg/m3 for hard wood dust and 5 mg/m3 for soft wood dust, with the exception of Western red cedar (Martin and Zalk 1997; Scheeper et al. 1995). In addition, the European Union (EU) in 1999, decided the permissible limit for the exposure to inhalable wood dust to be 5 mg/m3 (Magagnotti et al. 2013), and the European Unions (EU’s) Scientific Committee for Occupational Exposure Limits (SCOEL), exposure to wood dust above 0.5 mg/m3 causes lung function effects (Schulze et al. 2003).
Despite increased furniture production in Ethiopia (Edwards 2010), little is known about worker occupational health and safety (Kumie et al. 2016). Three studies from Ethiopian wood factories were published between 2015 and 2019 (Ayalew et al. 2015; Fentie et al. 2019; Asgedom et al. 2019). The two Ethiopian studies, like most previous studies in wood factories across the world, focused on small-scale wood factories, with one focusing on particleboard companies that used eucalyptus trees as a raw material. A recent study in medium-scale wood factories in Ethiopian found a high level of geometric mean dust exposure (GM = 10.3 mg/m3) (Awoke et al. 2021) which was higher than the ACGIH wood dust levels standard. Other studies conducted in Ethiopia among small-scale and particleboard workers investigated the prevalence of chronic respiratory symptoms (Fentie et al. 2019; Asgedom et al. 2019), and personal wood dust concentration level of workers in small-scale and medium wood workers (Ayalew et al. 2015; Awoke et al. 2021).
Previous studies, on the other hand, did not investigate the prevalence of chronic respiratory symptoms, lung function parameters, and associated factors in large-scale wood furniture factories that employ substantial number of people and produce a variety of wood products. The aim of the study was to determine whether respiratory symptoms and lung function among large-scale woodworkers were associated with wood dust exposure in Addis Ababa, Ethiopia.
Materials and methods
Study setting, design and period
The study was carried out in wood factories in Addis Ababa, Ethiopia. There are eight large-scale wood factories in Addis Ababa which produce final goods for instance furniture production, and four of them were included in the study. The wood factories have four operational units. These are the machine operating unit, which generates a significant amount of dust while machining, the carpentry unit, which is responsible for cutting wood into the standard sizes required for further machining using sawing, the sanding unit, which is responsible for smoothing the surface of wood, and the painting unit, which uses surface treating chemicals. Moreover, in these wood factories, they have used dry wood and other adhesive chemicals.
The study also includes comparison workers from soft drink factories in Addis Ababa. We assumed that workers in soft drink plants were less exposed to dust and used them as a control group. There are three soft drink factories in Addis Ababa, Ethiopia. An institutional-based comparative cross-sectional study was conducted from February to April 2019 among these workers.
Study population and selection criteria
Two hundred and thirty two wood factory workers who have worked for at least 1 year at the factory were included in this study. In addition, as a control group, we recruited 232 soft drink industry workers. Due to limited resources, lung function tests were only performed on 104 randomly selected male workers (52 from the wood factory and 52 from the soft drink factory) out of 464 study participants. We included workers, over the age of 18, who have been actively involved in the production of wood and soft drinks for at least one year. Workers with recent abdominal or chest surgery, heart failure, TB, emphysema, and acute illness were all excluded from the lung function test.
Sampling procedure
First, in both the wood and soft drink factories, we divided the work process into production units, assuming that workers in different production units would be exposed to varying levels of dust. The sample was then determined using systematic sampling techniques. The workers' roster was used as a sampling frame. The first study participant was chosen at random from each production unit. Then, every 3rd worker was selected from the workers' rosters in each production unit.
Data collection procedure
Interviews
An interview was conducted to assess chronic respiratory symptoms using American Thoracic society questionnaires (ATS) (Liard and Neukirch 2000). The questionnaire's components included socio-demographic variables, the use of respiratory protective devices while working (yes/no) and the reason for not using respiratory protective devices (RPD). To maintain consistency with the original, the questionnaire was translated from English to Amharic and then back to English using standard translation procedures.
Prior to the actual data collection, the data collection tool was validated. Questions that were difficult for participants to understand were rephrased. The study participant was given a brief explanation about the purpose of the study prior to the interview, and the interview was conducted (face to face) for the selected woodworkers and controls in an office located at their workplaces in private.
Spirometry and anthropometric measurements
The American Thoracic Society-recommended NDD Easy on PC spirometer linked to a laptop was used to evaluate lung function parameters, such as FVC, FEV1, and FEV1/FVC in both woodworkers, and controls in a sitting (Miller et al. 2005). Spirometry was performed early in the morning, before the workers went to work. The technique was demonstrated to each participant prior to the actual lung function testing and supervised throughout the test process. FVC, FEV1, and the FEV1/FVC ratio were the lung function parameters studied. The participants' weight (kg) was measured using a standardized electronic weighing machine while they stood and wore light clothing, and their height (cm) was measured using a stadiometer with portable field survey scales, as recommended by the American Thoracic Society (Miller et al. 2005), and body mass index (BMI) was also calculated using NDD Medical technologies software. In this study, the lung function parameters are presented only in the absolute values because there are no reference equations for the Ethiopia population for obtaining predicted values.
Statistical analysis
During the data collection period, collected data were double-checked for completeness and consistency. We organized and entered the data in Epi-data version 4.4.2 and has been exported to SPSS version 23 for analysis. To summarize the data, descriptive statistics were used. The Pearson’s Chi-square test or Fisher's exact test (if the expected value was less than 5) was used to compare categorical responses of the difference between woodworkers and controls, while an independent t test was used to compare means of continuous variables. A Poisson regression model with a robust estimator was used to estimate prevalence ratio (PR) after controlling for confounders; age, education, income, previous respiratory disease, working experience, working hour per week, previous dust exposure, safety training. Prevalence ratio (PR) was chosen instead of prevalence odds ratio (POR) due to the high chronic respiratory symptom prevalence in this study (Tamhane et al. 2016).
Logistic regression analysis was used to determine whether or not exposure variables were significantly associated with respiratory symptom. After adjusted for confounding variables, such as gender, age, educational status, income, religion, previous respiratory disease, previous dust exposure, and safety training, variables with p ≤ 0.2 were included in the multivariable analysis. A p value of < 0.05 was considered a significant predictor variable for the current chronic respiratory symptoms. For continuous data, a multivariate linear regression model was used to compare the lung function parameters between woodworkers and controls adjusted for sex, age, and height.
Results
Socio-demographic characteristics
In this study, 230 (99%) of woodworkers and 227 (98%) of controls were included. Two woodworkers and three controls refused to participate, and among controls, one worker was terminated and one was on sick leave. The majority of the study participants were male, accounting for 356 (77.9%), and the (Mean ± SD) age of woodworkers was 32.9 (9.6), while control workers were 31.5 (7.9). A total of 131 woodworkers (57.0%) and 121 (53.3%) controls were married. A total of 151 (65.7%) of woodworkers and 187 (86.5%) of controls had completed secondary school. Regarding age, educational level, and monthly income, there were significant differences between woodworkers and controls. The two groups did not differ in terms of gender, religion, or marital status (Table 1).
Previous respiratory disease and behavioral factors
Before starting work in the factory, 47 (20.4%) of woodworkers and 18 (12.3%) of controls had previous chronic respiratory disease confirmed by physicians. About 14 (6.1%) of woodworkers had ever smoked, compared to 16 (7%) of controls. Furthermore, 13 (5.7%) of woodworkers and 22 (9.7%) of controls smoked less than 7 packs of cigarettes per week among ever and current smokers. In this study, only 30 (13.0%) of woodworkers wore RPD while on the job. In terms of previous chronic respiratory disease, and current smoking, there were significant differences between woodworkers and controls (Table 2).
Work-related factors
About 86 (37.4%) of woodworkers had ten years or more of factory experience, while about 84 (37.0%) of controls had between 4 and 5 years of factory experience on the current job. Eighty-two woodworkers (79.1%) and 159 controls (70.0%) worked less than 48 h per week. Before starting the current job, about 55 (23.9%) of woodworkers and 21 (9.3%) of controls had been exposed to coffee dust, cement dust, wood dust and cotton dust. There were a significant difference between woodworkers and controls in terms of working experience, working hour per week, previous dust exposure, and safety training (Table 3).
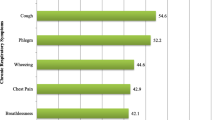
Prevalence of chronic respiratory symptoms
After adjusting for age, education, income, previous respiratory disease, working experience, working hour per week, previous dust exposure, and safety training, woodworkers had a significantly higher prevalence of chronic respiratory symptoms than controls (65.7% vs 23.3%). The prevalence ratio of all respiratory symptoms was significantly higher in woodworkers than in controls, parameters are cough (PR 2.18, 95% CI 16–4.08), sputum (PR 2.48, 95% CI 1.42–4.34), wheezing (PR 2.05, 95% CI 1.09–3.86), breathlessness (PR 2.64, 95% CI 1.47–4.78), and chest tightness (PR = 3.89, 95% CI 2.05–7.38). Because the number of smokers was small, the analysis was undertaken both including and excluding smokers. However, the outcome stayed the same (Table 4).
Factors associated with chronic respiratory symptoms
A multivariable logistic regression model was used to identify independent predictor variables for current chronic respiratory symptoms. Variables with a significant association at the bi-variate level, p value ≤ 0.2 were added to a multivariable logistic regression model. In this study, male participants had 1.9 times the odds of having current chronic respiratory symptoms as compared to female participants (AOR 1.9, 95% CI 1.09–3.30).
Previous respiratory disease was another factor that was found to be significantly associated with the current chronic respiratory symptoms. The odds of current chronic respiratory symptoms among workers who had previous respiratory disease were 3.9 times that of the workers who had no previous respiratory disease (AOR 3.9, 95% CI: 2.08–7.19). Moreover, we have performed analysis on previous dust exposure, use of RPD and safety training within the woodworker’s only. But we did not found significant association with current respiratory symptoms (Table 5).
Anthropometric measurements
The anthropometric parameters of woodworkers and controls were compared using an independent t test. In terms of weight and height, we found significant differences between groups (Table 6).
Lung function test
We tested the lung function of 104 male workers (52 from the woodworkers and 52 from controls). We excluded four spirometer results (two from woodworkers and two from controls) from the analysis due to unacceptable readings. Lung functions (FVC, and FEV1/FVC) between the woodworkers and the controls were significantly different (p = when adjusted for sex, age and height using multivariate regression. However, the ratio of FEV1/FVC was not significantly difference between woodworkers and controls (Table 7).
Discussion
The current study found that the prevalence of chronic respiratory symptoms was higher among woodworkers than in the control group, including cough (35.2% vs 10.1%), phlegm (44.3% vs 11.5%), wheezing (29.6% vs 11.9%), breathlessness (40.0% vs 11.0%), and chest tightness (37.4% vs 7.9%). Furthermore, gender, and previous respiratory disease were found to be independent predictors of the current chronic respiratory symptoms. When compared to controls, woodworkers had significantly lower FVC and FEV1.
The current study showed a higher prevalence of phlegm among woodworkers than the controls. This result is consistent with a study conducted in Iran among woodworkers and controls (Hosseini et al. 2020). But the prevalence of phlegm in this study is higher than previous studies done among woodworkers and controls in Iran (Neghab et al. 2018), South South of Nigeria (Tobin et al. 2016), Macedonia (Bislimovska et al. 2015), and Ethiopia (Fentie et al. 2019; Asgedom et al. 2019). The possible reasons for the difference might be due to the difference in uses of RPD which only 13.0% woodworkers were used in the present study. The findings of this study are consistent with those of a study conducted among woodworkers in Benin City, Nigeria, and Ethiopia, which found a high prevalence of chronic cough compared to controls (Ugheoke et al. 2006; Asgedom et al. 2019). All of these studies reported that woodworkers had a high prevalence of chronic cough compared to controls. But the present study showed a lower prevalence of chronic cough compared to the study done among woodworkers and controls in Iran and Southwest Ethiopia (Hosseini et al. 2020; Fentie et al. 2019). The observed difference could also be due to the difference by the study setting in which the study was done.
Similarly, the increased prevalence of wheezing among woodworkers in our study was also consistent with the findings among woodworkers in Iran (Hosseini et al. 2020). But the prevalence of wheezing in our study is higher than the studies done among woodworkers and controls in South of Thailand, Macedonia, Benin City, Nigeria, and Southwest Ethiopia (Thepaksorn et al. 2017; Bislimovska et al. 2015; Ugheoke et al. 2006; Fentie et al. 2019). Woodworkers working in wood factory had an increased risk of chest tightness compared to office workers (Hosseini et al. 2020), which is also consistent with our study. But the increasing prevalence of chest tightness in the present study is higher than previous studies done among woodworkers and controls in Iran, South of Thailand, Macedonia, Benin, City Nigeria, and Southwest Ethiopia (Neghab et al. 2018; Thepaksorn et al. 2017; Bislimovska et al. 2015; Ugheoke et al. 2006; Fentie et al. 2019). But the prevalence of chest tightness in this study is lower than the study in South South Nigeria (Tobin et al. 2016). The observed difference could also be explained by the difference in the ventilation system.
Regarding associated factors with the current chronic respiratory symptoms, only gender was independently associated with the current chronic respiratory symptoms from socio-demographic factors when added in the multivariable analysis model. Men were 1.90 times more likely than women to have current chronic respiratory symptoms (AOR 1.9, 95% CI 1.09–3.30). This finding contradicts a study conducted in Thailand, which found a link between being a female worker and the current chronic respiratory symptoms (Chaiear et al. 2018). Furthermore, a longitudinal study conducted in Danish also found a link between wood dust exposure and chronic respiratory symptoms in female woodworkers (Jacobsen et al. 2009). This could be due to the fact that women were assigned to areas with reduced wood dust exposure.
Previous respiratory disease was also associated with the current respiratory symptoms in this study. Workers who had the previous respiratory disease were 3.9 times (AOR 3.9, 95% CI 2.08–7.19) higher odds of current chronic respiratory symptoms compared to those who were free of previous respiratory disease. This study is similar to a study conducted in Thailand, which stated that workers who had family history of asthma were 3.95 times more likely to have current chronic respiratory health symptoms than workers who had no family history of asthma (Chaiear et al. 2018). This underlines the importance of previous respiratory disease on the current respiratory symptoms. In the present study, no use of RPD was not associated with current chronic respiratory symptoms among woodworkers. This finding contradicts with a study conducted in Northeast Thailand, which stated that woodworkers who did not use RPD were 2.26 times more odds of current chronic respiratory health symptoms than woodworkers who had use respiratory protective devices while working (Soongkhang and Laohasiriwong 2015), This evidenced that, to avoid dust exposure, a respiratory protective device is required. This difference could be attributed to differences in the types of dust produced, and the amount of dust each worker exposed to. The observed difference might also be explained by ventilation systems. Furthermore, the present study did not also find a significant association between education and the current chronic respiratory symptoms. This might be education alone and is not enough in areas where the ventilation system is limited as observed.
Woodworkers had significantly lower FVC and FEV1 compared to controls in this study. This finding indicated that occupational exposure to wood dust may cause a decrease in lower FVC and FEV1, as found in previous studies conducted in Turkey, Sulaimani, Iraq, South of Thailand, and Norway (Osman and Pala 2009; Mahmood et al. 2016; Færden et al. 2014; Thepaksorn et al. 2017). Similar with our findings, a study done in South South Nigeria showed a significant reduction of FVC and FEV1 among woodworkers when compared with the control groups (Tobin et al. 2016). However, the result of our study is inconsistent with study done in Ethiopia among particleboard workers, which showed an insignificant difference in lung function between exposed and control groups (Asgedom et al. 2019). This might be due to the difference in dust control mechanisms and the use of RPD.
Despite the fact that woodworkers were exposed to wood dust, as evidenced by the workplace survey, there was no significant difference in ratio of FEV1/FVC reduction between woodworkers and controls in this study. Our result agrees with results in Norway, Sulaimani, Iraq (Færden et al. 2014; Mahmood et al. 2016), which showed an insignificant difference in FEV1/FVC ratio reduction between woodworkers and controls. But the results of the this study contradict with other previous studies conducted in Iran (Neghab et al. 2018; Badirdast et al. 2017), South Thailand (Thepaksorn et al. 2017), India (Kacha et al. 2014), Macedonia (Bislimovska et al. 2015), Turkey (Osman and Pala 2009), and Nigeria (Omole et al. 2018; Tobin et al. 2016). All of these studies found that woodworkers had a significant FEVI/FVC ratio reduction than control groups. The possible reason for the difference might be due to the amount of wood dust each worker is exposed to and the type of dust control mechanisms.
Limitations of the study
The study relies on a cross-sectional design and a cause-and-effect relationship could not be established from this study. The amount of wood dust each worker is exposed to during their work time was not measured in this study. The workers may have a recall bias in the respiratory symptom assessment because symptoms are not always easy to remember and the study may also have risk of section bias of the workers. In addition, workers with respiratory health problem might have left their job so a healthy worker effect cannot be excluded.
Conclusion
When compared to controls, woodworkers exposed to wood dust had a significantly higher prevalence of chronic respiratory symptoms and lower FVC and FEV1. Furthermore, gender, and previous respiratory disease were associated with current chronic respiratory symptoms. This study found that woodworkers have lower lung function measures, which lowered lung capacity when compared to controls.
Therefore, engineering control methods should be implemented to reduce workers' exposure to wood dust and, it is preferable to conduct a prospective cohort study that focuses on dust exposure of each woodworker on large-scale wood factories.
Data availability
The data used to support the results of this study are available from the corresponding author upon request.
Abbreviations
- AAU:
-
Addis Ababa University
- AOR:
-
Adjusted odds ratio
- ATS:
-
American Thoracic Society
- COR:
-
Crude odds ratio
- FVC:
-
Forced vital capacity
- FEV1:
-
Forced Expiratory Volume in one second
- RPD:
-
Respiratory protective device
- SPSS:
-
Statistical Packages for Social Science
References
Alonso-Sardón M, Chamorro A-J, Hernández-García I et al (2015) Association between occupational exposure to wood dust and cancer: a systematic review and meta-analysis. PLoS ONE 10:e0133024
Asgedom AA, Bråtveit M, Moen BE (2019) High prevalence of respiratory symptoms among particleboard workers in Ethiopia: a cross-sectional study. Int J Environ Res Public Health 16:2158
Awoke TY, Takele AK, Mekonnen WT et al (2021) Assessment of dust exposure and chronic respiratory symptoms among workers in medium scale woodwork factories in Ethiopia; a cross sectional study. BMC Public Health 21:1–12
Ayalew E, Gebre Y, De Wael K (2015) A survey of occupational exposure to inhalable wood dust among workers in small-and medium-scale wood-processing enterprises in Ethiopia. Ann Occup Hyg 59:253–257
Badirdast P, Azari MR, Salehpour S et al (2017) The effect of wood aerosols and bioaerosols on the respiratory systems of wood manufacturing industry workers in Golestan Province. Tanaffos 16:53
Bhatti P, Newcomer L, Onstad L et al (2011) Wood dust exposure and risk of lung cancer. Occup Environ Med 68:599–604
Bislimovska D, Petrovska S, Minov J (2015) Respiratory symptoms and lung function in never-smoking male workers exposed to hardwood dust. Open Access Macedonian J Med Sci 3:500
Bosan I, Okpapi J (2004) Respiratory symptoms and ventilatory function impairment among wood workers in the Savannah Belt of Northern Nigeria
Chaiear N, Ngoencharee J, Saejiw N (2018) Respiratory symptoms and pulmonary function among workers in a rubber wood Sawmill Factory in Thailand. Am J Public Health Res 6:65–71
Edwards S (2010) Ethiopian Environment (Internet). https://www.phe-ethiopia.org/pdf/Ethiopian_Environment_Review.pdf
Ennin IE, Adzaku FK, Dodoo D et al (2015) A study of lung function indices of woodworkers at the Accra timber market in Ghana. Donnish J Med Med Sci 2:120–124
Færden K, Brit Lund M, Mogens Aaløkken T et al (2014) Hypersensitivity pneumonitis in a cluster of sawmill workers: a 10-year follow-up of exposure, symptoms, and lung function. Int J Occup Environ Health 20:167–173
Fedotov (2011) ILO. Action towards prevention of occupational and non-communicable diseases (Internet). http://www.worldpsi.org/sites/default/files/attachment/news/ilo_presenation.pdf. Accessed
Fentie D, Mulat E, Reta W (2019) Assessment of respiratory symptoms among woodworkers in Jimma Town, Southwest Ethiopia, a comparative cross-sectional study. Biomed J Sci Tech Res 18:13425–13430
Hämäläinen P, Takala J, Kiat TB (2017) Global estimates of occupational accidents and work-related illnesses 2017. World 2017:3–4
Health and Safety Excutive (2017) Occupational lung disease in Great Britain (Internet). http://www.hse.gov.uk/statistics/causdis/respiratory-diseases.pdf
Hosseini KD, Malekshahi Nejad V, Sun H et al (2020) Prevalence of respiratory symptoms and spirometric changes among non-smoker male wood workers. PLoS ONE 15:e0224860
Jacobsen G, Schlünssen V, Schaumburg I et al (2008) Longitudinal lung function decline and wood dust exposure in the furniture industry. Eur Respir J 31:334–342
Jacobsen G, Schlünssen V, Schaumburg I et al (2009) Increased incidence of respiratory symptoms among female woodworkers exposed to dry wood. Eur Respir J 33:1268–1276
Kacha Y, Nayak Y, Varu M et al (2014) Effects of wood dust on respiratory functions in saw mill workers. Int J Basic Appl Physiol 3:122–128
Kauppinen T, Vincent R, Liukkonen T et al (2006) Occupational exposure to inhalable wood dust in the member states of the European Union. Ann Occup Hyg 50:549–561
Kumie A, Amera T, Berhane K et al (2016) Occupational health and safety in Ethiopia: a review of situational analysis and needs assessment. Ethiopian J Health Dev 30:17–27
Liard R, Neukirch F (2000) Questionnaires: a major instrument for respiratory epidemiology. Eur Respir Monograph 5:154–166
Löfstedt H, Hagström K, Bryngelsson I-L et al (2017) Respiratory symptoms and lung function in relation to wood dust and monoterpene exposure in the wood pellet industry. Upsala J Med Sci 122:78–84
Magagnotti N, Nannicini C, Sciarra G et al (2013) Determining the exposure of chipper operators to inhalable wood dust. Ann Occup Hyg 57:784–792
Mahmood N, Karadaky K, Hussain SA et al (2016) Respiratory function among sawmill workers in different areas of Sulaimani city. Int J 5:351
Martin JR, Zalk DM (1997) Carpenter shop wood dust control: practical experience to reduce hardwood dust exposures below the American Conference of Governmental Industrial Hygienists Threshold Limit Values. Appl Occup Environ Hyg 12:595–605
Miller MR, Hankinson J, Brusasco V et al (2005) Standardisation of spirometry. Eur Respir J 26:319–338
Neghab M, Jabari Z, Kargar Shouroki F (2018) Functional disorders of the lung and symptoms of respiratory disease associated with occupational inhalation exposure to wood dust in Iran. Epidemiol Health 40:e2018031. https://doi.org/10.4178/epih.e2018031
Omole JO, Fabunmi AA, Akosile CO (2018) Respiratory function of sawmill workers and their relationship to duration of exposure to wood dust seen in Nigeria. J Environ Occup Health 7:9–16
Osman E, Pala K (2009) Occupational exposure to wood dust and health effects on the respiratory system in a minor industrial estate in Bursa/Turkey. Int J Occup Med Environ Health 22:43
Rosenberg C, Liukkonen T, Kallas-Tarpila T et al (2002) Monoterpene and wood dust exposures: work-related symptoms among Finnish sawmill workers. Am J Ind Med 41:38–53
Scheeper B, Kromhout H, Boleij JS (1995) Wood-dust exposure during wood-working processes. Ann Occup Hyg 39:141–154
Schlünssen V, Schaumburg I, Andersen N et al (2002) Nasal patency is related to dust exposure in woodworkers. Occup Environ Med 59:23–29
Schulze J, Brüning T, Donhuijsen K et al (2003) Comments on the recommendation of the Scientific Committee on Occupational Exposure Limits (SCOEL) for wood dust. Gefahrstoffe Reinhalt Luft 63:99–104
Soongkhang I, Laohasiriwong W (2015) Respiratory tract problems among wood furniture manufacturing factory workers in the northeast of Thailand. Kathmandu Univ Med J 13:125–129
Tamhane AR, Westfall AO, Burkholder GA et al (2016) Prevalence odds ratio versus prevalence ratio: choice comes with consequences. Stat Med 35:5730–5735
Thepaksorn P, Fadrilan-Camacho VFF, Siriwong W (2017) Respiratory symptoms and ventilatory function defects among Para rubber wood sawmill workers in the South of Thailand. Hum Ecol Risk Assess Int J 23:788–797
Tobin EA, Ediagbonya TF, Okojie OH, Asogun DA (2016) Occupational exposure to wood dust and respiratory health status of sawmill workers in South-South Nigeria. J Pollut Eff Cont 4:154. https://doi.org/10.4172/2375-4397.1000154
Ugheoke AJ, Ebomoyi MI, Iyawe VI (2006) Influence of smoking on respiratory symptoms and lung function indices in sawmill workers in Benin City, Nigeria. Niger J Physiol Sci 21(1–2):49–54. https://doi.org/10.4314/njps.v21i1-2.53957
Vallières E, Pintos J, Parent M-E et al (2015) Occupational exposure to wood dust and risk of lung cancer in two population-based case–control studies in Montreal, Canada. Environ Health 14:1–9
Wiggans R, Evans G, Fishwick D et al (2016) Asthma in furniture and wood processing workers: a systematic review. Occup Med 66:193–201
World Health Organization (1995) IARC Monographs on the Evaluation of Carcinogenic Risk to Humans, Wood Dust and Formaldehyde (Internet). http://monographs,iarc,fr/ENG/Monographs/vol62/volume62.pdf.
Acknowledgements
We kindly thank the wood factory management teams and data collectors, Workers for their permission to conduct the study and for participating in the study heart fully.
Funding
Addis Ababa University. “The funder has no role in study design, data collection and analysis, decision to publish, preparation of the manuscript”.
Author information
Authors and Affiliations
Contributions
BJ designed the study, conducted fieldwork, analyze the data, interpret the data, and wrote the manuscript SW supervised the development of the proposal, data analysis, and procedure of spirometer measurement and ZA contributed to the interpretation and reviewing of results and drafting the manuscript. All authors read the manuscript and agreed to its content.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflicts of interest.
Ethical approval and concent
We conduct the study after having an ethical clearance from the Institutional Review Board of the College of Health Sciences of Addis Ababa University. In addition, permission to conduct the study was also obtained from the factory managers. Before performing the lung function tests, written informed consent was obtained from each participant, and participants were informed that they have full right to refuse and withdraw at any time in the study. The study participants with lung function impairments were advised and linked to the nearest health facility.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Jabur, B., Ashuro, Z. & Abaya, S.W. Chronic respiratory symptoms and lung function parameters in large-scale wood factory workers in Addis Ababa, Ethiopia: a comparative cross-sectional study. Int Arch Occup Environ Health 95, 1221–1230 (2022). https://doi.org/10.1007/s00420-022-01857-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-022-01857-5