
Abstract
Objective
We investigated the contribution of physical and psychosocial work factors to social inequalities in self-rated health (SRH) in a sample of Danish 40 and 50 years old occupationally active women and men.
Methods
In this longitudinal study, the study population consisted of 3338 Danish women and men. Data were collected by postal questionnaires in 2000 (baseline) and 2006 (follow-up). The independent variable, socioeconomic position (SEP), was assessed by the highest achieved educational level at baseline. We conducted gender-stratified parallel multiple mediation analyses. In the mediation analyses, SEP was categorised as SEP I, II, III, VI and V among men. Among women, SEP was dichotomised into SEP I–IV and V. The outcome, SRH, was assessed at baseline and follow-up. A wide range of physical and psychosocial work factors were included as potential mediators.
Results
We found a social gradient in SRH across all levels of SEP among men. Among women, we only found a poorer SRH among those with the lowest SEP. Mediation analyses showed that work factors together accounted for 56% of the social inequalities in SRH among men and 44% among women. In both genders, ergonomic exposures and job insecurity seemed to play the major role for social inequalities in SRH. For women only, we also found noise to contribute to the social inequalities in SRH.
Conclusion
Physical and psychosocial work factors partially explained social inequalities in SRH among both genders. Improvement of the working environment can potentially contribute to the reduction of social inequalities in health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Social inequalities in health have been widely documented, for example, in terms of higher morbidity and mortality among individuals with lower socioeconomic position (SEP) compared with individuals with higher SEP (Lahelma et al. 2015; Mackenbach et al. 2008; Marmot and Bell 2016). Moreover, even though morbidity and mortality have been decreasing for several years, social inequalities in health persist and may even have widened (Diderichsen et al. 2012; Mortensen et al. 2016). Social inequalities have been studied in regards to a wide range of health outcomes including self-rated health (SRH) (Baldi et al. 2013; Cockerham 2017; Torsheim et al. 2018). SRH has been shown to be a good predictor of subsequent mortality in numerous studies across different countries and populations (Idler and Benyamini 1997; Jylhä 2009; Mossey and Shapiro 1982). In recent years, several studies have found that SRH is also a good predictor of objective health outcomes such as cardiovascular diseases and sickness absence (Roelen et al. 2018; Veromaa et al. 2017; Wu et al. 2013).
Research on health inequalities has attempted to identify mechanisms that explain the effects of SEP on adverse health outcomes (Aartsen et al. 2017; Borg and Kristensen 2000; Marmot et al. 2008). One mechanism may be differential exposure to risk factors for disease (Diderichsen et al. 2001). For example, many adverse work factors tend to cluster among individuals with lower SEP (Bauer et al. 2009; Borg and Kristensen 2000; Borrell et al. 2004; Ferrie 2003; Hämmig et al. 2014; Hämmig and Bauer 2013; Mustard et al. 2003; Niedhammer et al. 2008). Therefore, such work factors may contribute to social inequalities in health.
Previous studies have found that physical work factors partly explain social inequalities in SRH (Bauer et al. 2009; Borg and Kristensen 2000; Borrell et al. 2004; Hämmig et al. 2014; Hämmig and Bauer 2013; Niedhammer et al. 2008). In contrast, studies examining the contribution of psychosocial work factors to social inequalities in SRH have produced mixed results (Bauer et al. 2009; Borg and Kristensen 2000; Hämmig and Bauer 2013). Six of the previous studies were conducted in representative samples of a working population (Bauer et al. 2009; Borg and Kristensen 2000; Borrell et al. 2004; Hämmig et al. 2014; Mustard et al. 2003; Niedhammer et al. 2008) while only two studies were conducted in middle-aged populations (Schmitz 2016; Warren et al. 2008).
Importantly, most studies have only examined one or few dimensions of the working environment (Ferrie 2003; Mustard et al. 2003) or they have been cross-sectional (Hämmig et al. 2014; Hämmig and Bauer 2013; Niedhammer et al. 2008). Thus, only three studies have examined the contribution of a wide range of physical and psychosocial work factors to social inequalities in SRH using a longitudinal study design (Borg and Kristensen 2000; Schmitz 2016; Warren et al. 2008). A recent literature review concluded that about one third of social inequalities in SRH could be explained by work factors, but also that knowledge on the contribution of specific work factors was limited (Dieker et al. 2019). This gap in the literature hinders the implementation of targeted interventions.
Taking these limitations of previous research into account, the overall aim of this longitudinal study was to investigate the contribution of physical and psychosocial work factors to social inequalities in SRH during a 6-year follow-up period in a sample of Danish 40 and 50 years old occupationally active women and men.
Methods
Study sample
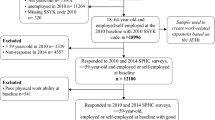
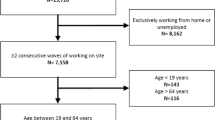
In this longitudinal study, we used data from the Danish Longitudinal Study on Work, Unemployment, and Health. This is a population-based study with a baseline postal survey carried out in 2000. The baseline survey was based on a stratified random sample consisting of a group of individuals aged 40 and 50 years by 1 October 1999 (response rate 69%, n = 7588). The sample was initially drawn from the ‘AKF Longitudinal Register’, but is now kept by ‘VIVE—The Danish Center for Social Science Research’ and contains a representative sample of 10% of the Danish population aged 15 years or older by 1 January 1981. Non-participants consisted of a significantly higher proportion of men, non-native-born Danes, and persons with low educational attainment (Christensen et al. 2004). A follow-up questionnaire was sent by postal mail in 2006 to baseline participants who were alive by 2006, still living in Denmark and who did not refuse to participate in scientific research (n = 6937). In total, 4893 (71%) filled in and returned the follow-up questionnaire. Among those who participated in both surveys, we excluded those who did not report the duration of their main education (missing: n = 45; other: n = 613; unknown: n = 11), and were missing on any of the main study variables (SEP, SRH at baseline and follow-up, gender and age; n = 87) and work factors; n = 799. The final study population consisted of 3338 occupationally active participants representing various job groups. The largest job groups were skilled workers: n = 483, unskilled workers; n = 457 and salaried employees; n = 2045. The rest constituted assisting spouses, self-employed within agriculture, self-employed professionals (medical doctors, lawyers and accountants) and other self-employed.
In our data, excluded individuals with missing values on the main variables, were more likely to have a lower SEP, poor SRH in 2000 and 2006, to report exposure to ergonomic exposures, particle pollution, low variation, low social support and job insecurity and less likely to report emotional and quantitative demands compared with included study participants. There were no significant differences in age and gender between excluded and included individuals.
Self-rated health
SRH was assessed in 2000 (baseline) and 2006 (follow-up) using a single question: "How do you assess your health in general?" The response options were: "Excellent" (0), "Very good" (1), "Good" (2), "Poor" (3) and "Very poor" (4). This measure is frequently used to assess the general health of an individual (Idler and Benyamini 1997; Jylhä 2009; Mossey and Shapiro 1982), thus it does not refer specifically to either physical or mental health. The variable was treated as a continuous variable in the statistical analyses.
Socioeconomic position
SEP was assessed by the highest achieved educational level in 2000 (baseline). Highest achieved educational level was originally categorized on an 8-point scale and later combined into five educational levels (SEP I–V): SEP I: "Long theoretical training, > 4 years (e.g., doctor, economist, high school teacher, civil engineer)”; SEP II: "Theoretical training, 3–4 years (e.g., primary school teacher, nurse, journalist, bachelor of engineering)”; SEP III: "Theoretical training, < 3 years (e.g., AP graduate in marketing management, AP graduate in Production Technology, catering manager)”; SEP IV: "Semi-skilled" and "Skilled workers (e.g., social- and healthcare assistant, nursing assistant, technical assistant)”; SEP V: "No vocational training". The participants responding “other vocational training” and “do not know” were excluded, because the duration of education in these groups is unknown and the participants are likely to be heterogeneous in terms of their SEP.
Physical work factors
Physical work factors included 10 items assessed in 2000 (baseline). The 10 items were combined into two multiple-item scales, ergonomic exposures (6 items, α = 0.811) and particle pollution (2 items, α = 0.596) and two single-item scales: noise and indoor climate. Ergonomic exposures at the workplace were assessed by six items regarding daily exposures to (1) “Work in stooping posture”, (2) “Work in which you have to twist your back”, (3) “Lift of more than 30 kg”, (4) “Pull or push heavy burdens”, (5) “Repetition of the same working procedures several times every hour”, and (6) "Vibrations”. Exposure to particles was assessed by two items measuring daily exposures to (1) “Dust and smoke” and (2) “Tobacco smoke from others smoking”. Exposure to noise was assessed by one item: “Are you exposed to noise in your daily work?” Poor indoor climate was assessed by one item: “Are you exposed to poor indoor climate in your daily work?” Responses for all scales were given on a 4-point Likert-scale ranging from "Never" (0) to "Always" (3). The total score for each scale was calculated as the mean score (i.e., total sum score divided by the number of items in the scale). Respondents who answered to less than half of the items in the scales were excluded.
Psychosocial work factors
Psychosocial work factors included 22 items assessed in 2000 (baseline). The 22 items were combined into five multiple-item scales: quantitative demands (2 items, α = 0.664), low skill discretion (3 items, α = 0.745), meaning of work (3 items, α = 0.790), job insecurity (3 items, α = 0.680) and discrimination (5 items, α = 0.641) and six single-item scales: high work pace, emotional demands, social support from colleagues, social support from supervisors, variation of work and social community at work. All scales, except the scale for discrimination, were derived from the Copenhagen Psychosocial Questionnaire (COPSOQ-I) (Kristensen et al. 2005). COPSOQ is a validated tool to assess the psychosocial working environment and has been widely used in Danish and international research (Berthelsen et al. 2018; Kristensen et al. 2005). Responses for discrimination were given on a 6-point Likert-scale ranging from "Never" (0) to "Almost every day" (5). Responses for job insecurity were given on a 4-point Likert-scale ranging from "Not at all" (0) to "Very much" (3). Responses for all other scales were given at a 4-point Likert-scale ranging from "Never" (0) to "Always" (3). The score was calculated in the same way as for the physical work factors. Skill discretion, meaning of work, social support from colleagues and supervisors, variation of work and social community at work were scored with reversed scoring, i.e., a higher score equaled less skill discretion, etc.
Statistical analyses
Chi-square tests were performed to examine the distribution of SRH in 2000 (baseline) and 2006 (follow-up) by SEP. In preliminary analyses, we explored the association between five categories of SEP (at baseline) and SRH (at follow-up) using a general linear regression model and adjusting for age and baseline SRH (Fig. 1). These analyses revealed a social gradient in SRH across all levels of SEP among men, whereas for women there were only social inequalities between the group of women with the lowest SEP compared with the remaining four groups with higher SEP. Therefore, in the main analyses, we used SEP as a continuous variable for men, while we dichotomized the SEP variable for women (SEP V vs. SEP I–IV). Furthermore, we used ANOVA-test to compare the mean scores of physical and psychosocial work factors by baseline SEP and linear regression analyses to explore the association between work factors and SRH at follow-up. Work factors significantly associated with both SEP and SRH were included in the main analyses. Multicollinearity between these work factors was tested using Spearman’s rank order correlation.

Association between socioeconomic position (SEP) and self-rated health (SRH). Beta values and 95% CI among men and women. a Beta values and 95% CI for the association between SEP and SRH among men. b Beta values and 95% CI for the association between SEP and SRH among women. Note: Reference group is SEP I. Higher scores for SRH equal poorer SRH. Analyses are adjusted for age and SRH at baseline
To explore the contribution of work factors to social inequalities in SRH, we applied a parallel multiple mediation analysis method, which allows for several mediators to be tested at the same time (Preacher and Hayes 2008). We estimated the direct effect (i.e., not through work factors), indirect effect (i.e., through work factors) and total effect (direct and indirect effect combined) of SEP on SRH (Hayes 2017). All work factors significantly associated with SEP and SRH at follow-up were included in the model at the same time. Furthermore, using this method we conducted a series of pairwise comparison analyses, which allowed us to investigate whether the indirect effect through the specific work factors were statistically different from each other. These analyses were conducted using the PROCESS macro for SAS. Bootstrapping (5000 repetitions) were used to calculate 95% confidence intervals (95% CI). All analyses were adjusted for age and SRH at baseline. Furthermore, as SEP was categorized differently among men and women, and since SRH and some work factors have shown to vary by gender (Bauer et al. 2009; De Sio et al. 2017; Mustard et al. 2003), we stratified all analyses by gender. We used a statistical significance level of 5%.
Results
Among the physical work factors, poor indoor climate among men and ergonomic exposures, noise and particle pollution among both genders increased with lower SEP (Tables 1 and 2). Among the psychosocial work factors, low social support from colleagues and low meaning of work among women, and low skill discretion and job insecurity among both genders increased with lower SEP. In contrast, social community at work among women, high work pace among men and emotional and quantitative demands among both genders increased with higher SEP. Testing the association between work factors and SRH showed that ergonomic exposures, noise, skill discretion, variation of work, job insecurity, and discrimination were significantly associated with poor SRH among both genders. Poor indoor climate, particle pollution, high work pace and social support from colleagues among men, and social support from supervisors among women were significantly associated with poor SRH (Tables 3 and 4).
We observed several significant correlations among the work factors for both genders with most of these correlations being weak (Tables 5 and 6). The strongest correlations were between ergonomic exposures and noise (ρ = 0.53) among men and low skill discretion and low variation (ρ = 0.51) among women.
Tables 7 and 8 demonstrate the findings of the parallel mediation analyses investigating the contribution of work factors to social inequalities in SRH. Among men, the total effect of SEP was estimated to 0.064 (95% CI 0.035–0.092), whereas the total indirect effects of the work factors collectively are estimated to 0.036 (95% CI 0.020–0.053), i.e., 56% of the total effect (Table 5). Thus, two cases that differ by one unit in SEP are estimated to differ by 0.036 in SRH score through work factors, with those from lower SEP having higher SRH (i.e., worsening in SRH). Results for the specific work factors were significant for ergonomic exposures, 0.023 (95% CI 0.007–0.040), and job insecurity, 0.005 (95% CI 0.001–0.009). Pairwise comparisons between these work factors showed that the mediating effects of ergonomic exposures were stronger than the mediating effect of job insecurity (data not shown).
Among women, the total effect was estimated to 0.208 (95% CI 0.104–0.312), whereas the total indirect effects was estimated to 0.092 (95% CI 0.047–0.137), i.e., 44% of the total effect (Table 6). Results for the specific work factors were significant for ergonomic exposures, 0.038 (95% CI 0.014–0.065), noise, 0.025 (95% CI 0.008–0.047), and job insecurity, 0.018 (95% CI 0.001–0.038). Pairwise comparisons between these work factors were all insignificant, thus they did not differ significantly in their contribution (data not shown).
Discussion
We found a clear social gradient in SRH among men, while there were only social inequalities in SRH between women with the lowest SEP compared with the four remaining groups of SEP among women. These findings are in accordance with previous studies examining social inequalities in SRH (Bauer et al. 2009; Borrell et al. 2004; Hämmig et al. 2014; Mustard et al. 2003; Niedhammer et al. 2008). Indeed, previous studies suggest that social inequalities in various health outcomes are less pronounced among women than men (Arber 1997; Koskinen and Martelin 1994). However, some studies have also found social inequalities in SRH among women (Matthews et al. 1999; Schrijvers et al. 1998).
We also found that exposure to adverse work factors was unequally distributed across SEP among both genders. Thus, our findings were in line with previous studies showing that most adverse work factors tend to cluster among individuals with lower SEP (Bauer et al. 2009; Borg and Kristensen 2000; Borrell et al. 2004; Ferrie 2003; Hämmig et al. 2014; Hämmig and Bauer 2013; Mustard et al. 2003; Niedhammer et al. 2008). Quantitative and emotional demands and high work pace, however, exhibited a positive gradient, i.e., they were more prevalent in individuals with higher SEP. These findings were also in line with previous studies (Borg and Kristensen 2000; Niedhammer et al. 2008; Schrijvers et al. 1998).
Our main finding was that work factors partly explained approximately half of the social inequalities in SRH. Overall, these results add to the existing evidence showing that the working environment accounts for some of the social inequalities in SRH (Borg and Kristensen 2000; Ferrie 2003; Mustard et al. 2003; Parker et al. 2013; Schmitz 2016; Warren et al. 2008). In line with our findings, a Danish cohort showed that a wide range of work factors together explained almost two-thirds of the social inequalities in changes in SRH, when testing a combination of five different work factors (ergonomic exposures, repetitive work, skill discretion, climatic exposures, and job insecurity) (Borg and Kristensen 2000).
Regarding the contribution of the individual work factors to social inequalities in SRH, our results suggested that noise (particularly among women) and ergonomic exposures and job insecurity (among both genders) partly explained social inequalities in SRH. Results from the pairwise comparison analyses suggested that ergonomic exposures accounted for more of the social inequalities in SRH than the remaining work factors among men. In contrast, the contribution of ergonomic exposures, job insecurity, and noise did not differ significantly among women. The findings regarding ergonomic exposures and job insecurity are in line with several other studies showing that these work factors substantially contribute to social inequalities in SRH (Bauer et al. 2009; Borg and Kristensen 2000; Borrell et al. 2004; Ferrie 2003; Hämmig et al. 2014; Hämmig and Bauer 2013; Niedhammer et al. 2008).
Strengths and limitations
This study has important strengths. First, the present study uses a longitudinal design. To our knowledge, only three other studies have investigated the contribution of a wide range of physical and psychosocial work factors to social inequalities in SRH using a longitudinal design (Borg and Kristensen 2000; Schmitz 2016; Warren et al. 2008). Second, by using a parallel multiple mediation model as described by Preacher and Hayes (Hayes 2017; Preacher and Hayes 2008), we were able to estimate the contribution of the individual work factors. Third, we used a validated tool to assess the dimensions of the psychosocial working environment (Berthelsen et al. 2018; Kristensen et al. 2005) with the exception of the scale for discrimination. Finally, our study population consisted of a large group of occupationally active participants representing various job groups.
The main limitation of this study is that despite the longitudinal design, SEP, SRH at baseline and work factors were assessed at the same time. Therefore, in principle, we were not able to determine the temporal relationship between these factors at baseline. The temporal separation is a crucial assumption when performing mediation analyses, as we did in our study (Oude Groeniger and Burdorf 2020). Nevertheless, although SEP and work factors were assessed at the same time, we assume that most of the study participants obtained their highest education before obtaining their current occupational position. Regarding the association between SRH and SEP, we used the highest achieved education instead of occupational status, since educational level is typically obtained earlier in life. Hence, we minimized the risk of reverse causation, i.e., that health influences the highest obtained educational level. However, a longitudinal study has shown that poor childhood health could influence later educational position (Mensah and Hobcraft 2008). Thus, we cannot rule out the possibility that poor health has led to a shorter education. By taking baseline SRH into account, we partly handle this bias, and as such our analyses resemble studies that investigate changes over time. Regarding the association between SRH and work factors, participants with poor SRH may have left the labor force or have shifted into a less demanding job. This healthy worker effect and selection of workers into jobs with fewer demands might result in an underestimation of the relationship between SEP and SRH and the contribution of work factors to social inequalities in health. In a similar way, it is plausible that our results might be underestimated, as excluded individuals were more likely to have a lower SEP, poor SRH in 2000 and 2006, and to report ergonomic exposures and job insecurity compared with included study participants.
In contrast to several other studies, we deliberately chose not to adjust for adverse health behavior, which can be more common among subjects with low SEP (Borg and Kristensen 2000; Power et al. 1998; Warren et al. 2004). Our main rationale is that an unhealthy lifestyle has been demonstrated to be a consequence of adverse work factors, among which job strain is the most well-studied (Heikkilä et al. 2013). Thus, if work factors execute their effect on health through lifestyle factors, these should not be included in the statistical analyses. Furthermore, from an occupational health perspective, it is interesting that occupational factors explain about one third of social inequalities in health, whereas lifestyle factors explain one fifth (Dieker et al. 2019).
Our assessment of work factors is limited by the lack of information on the duration of these exposures (e.g., in terms of seniority). Furthermore, work factors may change during follow-up and therefore be misclassified. Yet, to avoid a reverse effect of health on work factors, e.g., due to selection into or out of demanding jobs or because health affects how work factors are perceived and reported, we did not include information about work factors at follow-up. It is also possible that the reporting of work factors was influenced by the participants' personality, mental health status, and global workability. For example, study participants being depressed might over-report adverse work factors (Rugulies et al. 2009), and it has been claimed that questionnaire-based assessment of psychosocial work factors captures individual factors rather than occupational exposures (Persson et al. 2012). Besides, the accordance between self-reports and objective measures of physical job demands seems poor (Stock et al. 2005). However, if it indeed is the perception of the working environment that determines the effect on health, the use of subjective reports will be superior when estimating health consequences. Nevertheless, from an intervention perspective, knowledge about objective, occupational exposures is necessary.
The indirect effects of the different work factors included in the analyses might also be influenced by multicollinearity. Even though we only found low to moderate correlations, a study showed that correlations below 0.5 can produce multicollinearity (Vatcheva and Lee 2016). Hence, it is likely that correlation between several work factors have produced multicollinearity in the models, which may artificially have reduced the beta coefficients for both variables and made them statistically insignificant.
The observed differences in social inequalities in exposure to work factors and in SRH between men and women should be interpreted cautiously. For example, in some occupations, there is an overrepresentation of men or women, meaning that some of the differences in work-related exposures may be related to occupation rather than gender. Furthermore it has been argued that SRH fails to address the psychological aspects of health and that certain aspects of the psychological health is more important among women with low SEP than men with low SEP (Phillips 2015). If this hypothesis is true, SRH may be a less valid measure of health problems in women, and this may explain why we did not find a social gradient across all levels of SEP in this group.
For both men and women, however, the observed effect sizes for SEP on SRH were relatively small. For men, the effect sizes ranged between 0.163 and 0.371. This corresponded to 20–50% of the SD of SRH at baseline. In comparison, the effect size was 0.223 among women in the lowest SEP and this corresponded with approximately 25% of the SD of SRH at baseline. A follow-up period of 6 years might be too short to expect a larger effect, and it is reasonable to assume that the contribution of work factors to social inequalities in health is larger in a life-course perspective. Another possible explanation is that the study population might be less vulnerable to the harmful effects of work factors due to their relatively good health (around 60% among both men and women reported an “Excellent” or “Very good” health at baseline). Finally, as we used a sample of 40- and 50-year-old men and women, it is possible that work factors have already exerted the majority of their adverse effects before this age. This hypothesis is supported by the fact that there was a social gradient in SRH at baseline.
Finally, although we started out with the hypothesis that physical and psychosocial work factors contributed to the social inequalities in SRH, our analyses were largely data driven as explained in the Methods section. Furthermore, we tested the mediating effect of a range of work factors increasing the risk of chance findings. These limitations stress the necessity of testing our results in other populations.
The study population consisted of a sample of 40 and 50 years old, occupationally active men and women living in Denmark. Hence, we propose that the findings in this study can be generalized to the Danish working population. However, as previous studies have shown that age can moderate the association between work factors and SRH (Burr et al. 2017; Cheng et al. 2013), our findings might not be applicable to other age groups than a middle-aged population.
Conclusion
With this study, we found arguments that the working environment plays a role in social inequalities in health. Overall, we found that work factors together explained approximately half of the social inequalities in SRH among both genders. More specifically, our findings suggest that the most influential factors seem to be ergonomic exposures and job insecurity among both genders and noise among women. Thus, this study contributes to the understanding of the pathways from SEP to poor health. Further work is needed to clarify the mediating role of work factors to social inequalities in SRH including also younger participants at the beginning of their working life and with other more specific health outcomes of high public health relevance, such as musculoskeletal disorders or depression. Importantly, this study also provides knowledge that can direct interventions aiming at reducing social inequalities in health.
References
Aartsen M, Veenstra M, Hansen T (2017) Social pathways to health: on the mediating role of the social network in the relation between socio–economic position and health. SSM Popul Health 3:419–426. https://doi.org/10.1016/j.ssmph.2017.05.006
Arber S (1997) Comparing inequalities in women’s and men’s health: Britain in the 1990s. S Sci Med 1982(44):773–787
Baldi I, Costa G, Foltran F, Spada V, Chiffi D, Sacerdote C, Gregori D (2013) Effect of educational attainment on incidence and mortality for ischemic heart and cerebrovascular diseases: a systematic review and trend estimation. Int J Cardiol 168:4959–4963. https://doi.org/10.1016/j.ijcard.2013.07.142
Bauer GF, Huber CA, Jenny GJ, Müller F, Hämmig O (2009) Socioeconomic status, working conditions and self-rated health in Switzerland: explaining the gradient in men and women. Int J Public Health 54:23–30. https://doi.org/10.1007/s00038-008-7077-2
Berthelsen H, Hakanen JJ, Westerlund H (2018) Copenhagen Psychosocial Questionnaire—a validation study using the Job Demand-Resources model. PLoS ONE 13:e0196450. https://doi.org/10.1371/journal.pone.0196450
Borg V, Kristensen TS (2000) Social class and self-rated health: can the gradient be explained by differences in life style or work environment? Soc Sci Med 1982(51):1019–1030
Borrell C, Muntaner C, Benach J, Artazcoz L (2004) Social class and self-reported health status among men and women: what is the role of work organisation, household material standards and household labour? Soc Sci Med 58:1869–1887. https://doi.org/10.1016/S0277-9536(03)00408-8
Burr H, Hasselhorn HM, Kersten N, Pohrt A, Rugulies R (2017) Does age modify the association between psychosocial factors at work and deterioration of self-rated health? Scand J Work Environ Health 43:465–474. https://doi.org/10.5271/sjweh.3648
Cheng Y, Chen I-S, Chen C-J, Burr H, Hasselhorn HM (2013) The influence of age on the distribution of self-rated health, burnout and their associations with psychosocial work conditions. J Psychosom Res 74:213–220. https://doi.org/10.1016/j.jpsychores.2012.12.017
Christensen U, Lund R, Damsgaard MT, Holstein BE, Ditlevsen S, Diderichsen F, Due P, Iversen L, Lynch J (2004) Cynical hostility, socioeconomic position, health behaviors, and symptom load: a cross-sectional analysis in a Danish population-based study. Psychosom Med 66:572–577. https://doi.org/10.1097/01.psy.0000126206.35683.d1
Cockerham WC (2017) The social determinants of chronic disease. Am J Prev Med 52:S5–S12
De Sio S, Cedrone F, Sanità D, Ricci P, Corbosiero P, Di Traglia M, Greco E, Stansfeld S (2017) Quality of life in workers and stress: gender differences in exposure to psychosocial risks and perceived well-being. BioMed Res Int 2017:7340781. https://doi.org/10.1155/2017/7340781
Diderichsen F, Evans T, Whitehead M (2001) Challenging inequities in health: from ethics to action. Oxford University Press, Oxford, New York
Diderichsen F, Andersen I, Manuel C, Working Group of Danish Review on Social Determinants of Health, Andersen A-MN, Bach E, Baadsgaard M, Brønnum-Hansen H, Hansen FK, Jeune B, Jørgensen T, Søgaard J (2012) Health inequality—determinants and policies. Scand J Public Health 40:12–105. https://doi.org/10.1177/1403494812457734
Dieker AC, Ijzelenberg W, Proper KI, Burdorf A, Ket JC, van der Beek AJ, Hulsegge G (2019) The contribution of work and lifestyle factors to socioeconomic inequalities in self-rated health—a systematic review. Scand J Work Environ Health 45:114–125. https://doi.org/10.5271/sjweh.3772
Ferrie JE (2003) Future uncertainty and socioeconomic inequalities in health: the Whitehall II study. Soc Sci Med 57:637–646
Hämmig O, Bauer GF (2013) The social gradient in work and health: a cross-sectional study exploring the relationship between working conditions and health inequalities. BMC Public Health 13:1170. https://doi.org/10.1186/1471-2458-13-1170
Hämmig O, Gutzwiller F, Kawachi I (2014) The contribution of lifestyle and work factors to social inequalities in self-rated health among the employed population in Switzerland. Soc Sci Med 1982(121):74–84. https://doi.org/10.1016/j.socscimed.2014.09.041
Hayes AF (2017) Introduction to mediation, moderation, and conditional process analysis: a regression-based approach
Heikkilä K, Fransson EI, Nyberg ST, Zins M, Westerlund H, Westerholm P, Virtanen M, Vahtera J, Suominen S, Steptoe A, Salo P, Pentti J, Oksanen T, Nordin M, Marmot MG, Lunau T, Ladwig K-H, Koskenvuo M, Knutsson A, Kittel F, Jöckel K-H, Goldberg M, Erbel R, Dragano N, DeBacquer D, Clays E, Casini A, Alfredsson L, Ferrie JE, Singh-Manoux A, Batty GD, Kivimäki M (2013) Job strain and health-related lifestyle: findings from an individual-participant meta-analysis of 118 000 working adults. Am J Public Health 103:2090–2097. https://doi.org/10.2105/AJPH.2012.301090
Idler EL, Benyamini Y (1997) Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 38:21–37
Jylhä M (2009) What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med 1982(69):307–316. https://doi.org/10.1016/j.socscimed.2009.05.013
Koskinen S, Martelin T (1994) Why are socioeconomic mortality differences smaller among women than among men? Soc Sci Med 1982(38):1385–1396
Kristensen TS, Hannerz H, Høgh A, Borg V (2005) The Copenhagen Psychosocial Questionnaire—a tool for the assessment and improvement of the psychosocial work environment. Scand J Work Environ Health 31:438–449
Lahelma E, Pietiläinen O, Rahkonen O, Kivimäki M, Martikainen P, Ferrie J, Marmot M, Shipley M, Sekine M, Tatsuse T, Lallukka T (2015) Social class inequalities in health among occupational cohorts from Finland, Britain and Japan: a follow up study. Health Place 31:173–179. https://doi.org/10.1016/j.healthplace.2014.12.004
Mackenbach JP, Stirbu I, Roskam A-JR, Schaap MM, Menvielle G, Leinsalu M, Kunst AE, European Union Working Group on Socioeconomic Inequalities in Health (2008) Socioeconomic inequalities in health in 22 European countries. N Engl J Med 358:2468–2481. https://doi.org/10.1056/NEJMsa0707519
Marmot M, Bell R (2016) Social inequalities in health: a proper concern of epidemiology. Ann Epidemiol 26:238–240. https://doi.org/10.1016/j.annepidem.2016.02.003
Marmot M, Friel S, Bell R, Houweling TAJ, Taylor S, Commission on Social Determinants of Health (2008) Closing the gap in a generation: health equity through action on the social determinants of health. Lancet Lond Engl 372:1661–1669. https://doi.org/10.1016/S0140-6736(08)61690-6
Matthews S, Manor O, Power C (1999) Social inequalities in health: are there gender differences? Soc Sci Med 1982(48):49–60
Mensah FK, Hobcraft J (2008) Childhood deprivation, health and development: associations with adult health in the 1958 and 1970 British prospective birth cohort studies. J Epidemiol Community Health 62:599–606. https://doi.org/10.1136/jech.2007.065706
Mortensen LH, Rehnberg J, Dahl E, Diderichsen F, Elstad JI, Martikainen P, Rehkopf D, Tarkiainen L, Fritzell J (2016) Shape of the association between income and mortality: a cohort study of Denmark, Finland, Norway and Sweden in 1995 and 2003. BMJ Open 6:e010974. https://doi.org/10.1136/bmjopen-2015-010974
Mossey JM, Shapiro E (1982) Self-rated health: a predictor of mortality among the elderly. Am J Public Health 72:800–808
Mustard C, Vermeulen M, Lavis J (2003) Is position in the occupational hierarchy a determinant of decline in perceived health status? Soc Sci Med 57:2291–2303. https://doi.org/10.1016/j.socscimed.2003.08.001
National Committee on Health Research Ethics (2011) Guidelines about Notification etc. of a Biomedical Research Project to the Committee System on Biomedical Research Ethics
Niedhammer I, Chastang J-F, David S, Kelleher C (2008) The contribution of occupational factors to social inequalities in health: findings from the national French SUMER survey. Soc Sci Med 1982(67):1870–1881. https://doi.org/10.1016/j.socscimed.2008.09.007
Oude Groeniger J, Burdorf A (2020) Advancing mediation analysis in occupational health research. Scand J Work Environ Health 46:113–116. https://doi.org/10.5271/sjweh.3886
Parker V, Andel R, Nilsen C, Kåreholt I (2013) The association between mid-life socioeconomic position and health after retirement—exploring the role of working conditions. J Aging Health 25:863–881. https://doi.org/10.1177/0898264313492822
Persson R, Hansen ÅM, Garde AH, Kristiansen J, Nordander C, Balogh I, Ohlsson K, Ostergren P-O, Ørbæk P (2012) Can the job content questionnaire be used to assess structural and organizational properties of the work environment? Int Arch Occup Environ Health 85:45–55. https://doi.org/10.1007/s00420-011-0647-2
Phillips SP (2015) Women’s relative immunity to the socio-economic health gradient: artifact or real? Glob Health Action 8:27259
Power C, Matthews S, Manor O (1998) Inequalities in self-rated health: explanations from different stages of life. Lancet Lond Engl 351:1009–1014. https://doi.org/10.1016/S0140-6736(97)11082-0
Preacher KJ, Hayes AF (2008) Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods 40:879–891. https://doi.org/10.3758/BRM.40.3.879
Roelen C, Thorsen S, Heymans M, Twisk J, Bültmann U, Bjørner J (2018) Development and validation of a prediction model for long-term sickness absence based on occupational health survey variables. Disabil Rehabil 40:168–175. https://doi.org/10.1080/09638288.2016.1247471
Rugulies R, Aust B, Siegrist J, von dem Knesebeck O, Bültmann U, Bjorner JB, Burr H (2009) Distribution of effort-reward imbalance in Denmark and its prospective association with a decline in self-rated health. J Occup Environ Med 51:870–878. https://doi.org/10.1097/JOM.0b013e3181a9086c
Schmitz LL (2016) Do working conditions at older ages shape the health gradient? J Health Econ 50:183–197. https://doi.org/10.1016/j.jhealeco.2016.10.002
Schrijvers CT, van de Mheen HD, Stronks K, Mackenbach JP (1998) Socioeconomic inequalities in health in the working population: the contribution of working conditions. Int J Epidemiol 27:1011–1018
Stock SR, Fernandes R, Delisle A, Vézina N (2005) Reproducibility and validity of workers’ self-reports of physical work demands. Scand J Work Environ Health 31:409–437
Torsheim T, Nygren JM, Rasmussen M, Arnarsson AM, Bendtsen P, Schnohr CW, Nielsen L, Nyholm M (2018) Social inequalities in self-rated health: a comparative cross-national study among 32,560 Nordic adolescents. Scand J Public Health 46:150–156. https://doi.org/10.1177/1403494817734733
Vatcheva P, Lee M (2016) Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiol Open Access. https://doi.org/10.4172/2161-1165.1000227
Veromaa V, Kautiainen H, Juonala M, Rantanen A, Korhonen PE (2017) Self-rated health as an indicator of ideal cardiovascular health among working-aged women. Scand J Prim Health Care 35:322–328. https://doi.org/10.1080/02813432.2017.1397299
Warren JR, Hoonakker P, Carayon P, Brand J (2004) Job characteristics as mediators in SES-health relationships. Soc Sci Med 1982(59):1367–1378. https://doi.org/10.1016/j.socscimed.2004.01.035
Warren JR, Carayon P, Hoonakker P (2008) Changes in health between ages 54 and 65: the role of job characteristics and socioeconomic status. Res Aging 30:672–700. https://doi.org/10.1177/0164027508322639
Wu S, Wang R, Zhao Y, Ma X, Wu M, Yan X, He J (2013) The relationship between self-rated health and objective health status: a population-based study. BMC Public Health 13:320. https://doi.org/10.1186/1471-2458-13-320
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
None declared.
Human subject research approval
According to Danish law, research studies that use solely questionnaire and register data do not need approval from the National Committee on Health Research Ethics (National Committee on Health Research Ethics, 2011).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Brønholt, R.L.L., Hansen, M.B., Islamoska, S. et al. Physical and psychosocial work factors as explanations for social inequalities in self-rated health. Int Arch Occup Environ Health 94, 335–346 (2021). https://doi.org/10.1007/s00420-020-01582-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-020-01582-x