
Abstract
Purpose
The aim was to investigate the long-term importance of adjustment latitude for increased work ability and return to work among female human service workers on long-term sick leave.
Methods
A cohort of female human service workers on long-term sick leave (>60 days) was given a questionnaire four times (0, 6, 12, 60 months). Linear mixed models were used for longitudinal analysis of the repeated measurements of work ability and return to work.
Results
Having a higher level of adjustment latitude was associated with both increased work ability and return to work. Adjustments related to work pace were strongly associated with increased work ability, as were adjustments to the work place. Having individual opportunities for taking short breaks and a general acceptance of taking short breaks were associated with increased work ability. At home, a higher level of responsibility for household work was related to increased work ability and return to work. Individuals with possibilities for adjustment latitude, especially pace and place at work, and an acceptance of taking breaks had greater increased work ability over time and a greater work ability compared with individuals who did not have such opportunities.
Conclusions
This study highlights the importance of opportunities for adjustment latitude at work to increase work ability and return to work among female human service workers who have been on long-term sick leave. The results support push and pull theories for individual decision-making on return to work.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
A broad range of factors explains the frequency and duration of long-term sick leave: working and organisational conditions, health status, motivation, and home-related conditions (Beemsterboer et al. 2009). It has been suggested that prolonged ill health status because of work stress and musculoskeletal pain is dependent on the amount and quality of recuperation; for example, incomplete recovery from work-related stressors can lead to allostatic load, chronic muscular tension, and a pathway to ill health (Geurts and Sonnentag 2006; Veiersted et al. 1993). Thus, the interplay between recovery opportunities at work and during leisure time may have importance (Geurts and Sonnentag 2006). With the sickness flexibility model (Johansson and Lundberg 2004) as a theoretical base, the importance of adjustment latitude at work and at home for return to work (RTW) or improved health and work ability among female human service organisation (HSO) workers on long-term sick leave was studied.
Adjustment latitude at work
Pulling conditions for RTW have often been considered in economic analyses and related to individual decision-making, while pushing conditions for RTW are often studied as work-related forces from the labour market (Stattin 2005). According to the sickness flexibility model, RTW can be considered as a decision process wherein conditions such as work situation, adjustment latitude, requirements, and incentives for individual choice whether to attend at work or not are pushing and pulling (Johansson and Lundberg 2004). Adjustment latitude, as pushing or pulling conditions, means opportunities to adjust work because of ill health (Johansson and Lundberg 2004). Earlier empirical studies have demonstrated the importance of high adjustment latitude in relation to paid work: for sick leave among both female and male workers (Hultin et al. 2010), long-term sick leave (Johansson and Lundberg 2004), work ability (Johansson et al. 2012), RTW (Johansson et al. 2006), and staying at work (de Vries et al. 2011).
The importance of adjustment latitude may be due to recuperation, e.g. the short recovery that takes place during unscheduled, needed breaks. Musculoskeletal pain, which is the most common reason for long-term sick leave (Larsson et al. 2014), is empirically indicated and related to sustained muscle activity, overload, and lack of breaks (Hagg and Astrom 1997; Visser and van Dieen 2006). However, little research has been done on the importance of breaks for reducing work stress and muscular tension. Associations between taking a rest and musculoskeletal pain have been shown (Janga and Akinfenwa 2012), and another study has shown an association between taking a rest and performance (Tucker 2003). In line with this reasoning, there are also studies showing associations between flexible working time and RTW (Krause et al. 1998).
Adjustment latitude at home
There is reasonable and important interplay between recovery opportunities at work and during leisure time (Geurts and Sonnentag 2006). Individual health can be seen as a product of the family’s decisions and negotiations regarding time and resources (Bolin et al. 2002). The family’s gathered resources can be a source of economic, emotional, and social support for a family member—positively affecting individuals’ health. Conversely, they can affect the individual so she ends up with fewer individual resources (Bolin et al. 2002). Thus, adjustment latitude at home may be related to the family situation, and the decision of RTW may be due to individuals’ health needs as well as opportunities and conditions for recovery. A hypothesis in line with the sickness flexibility model suggests that conditions that are beneficial for individuals’ needs to adjust to their poor health are pulling and conditions that mean poor adjustment latitudes are pushing individuals in individuals’ decisions to RTW. Nevertheless, the way in which adjustment latitude at home may affect work ability and return to work has been poorly studied.
Work ability and return to work
The link between adjustment latitude and return to work may be mediated by perceived work ability. Self-assessed work ability, which may be judged in relation to health capacity and work adjustment opportunities, can predict return to work (Ahlstrom et al. 2010, 2012). The concept of work ability is conceptualised as the dynamic relation or balance between individual resources and demands at work (Ilmarinen 2006; Tuomi et al. 2001). It originates in the World Health Organisation’s (WHO) characterisation of health and, later, in their definition of functioning and health (ICF), which describes how people live with their health conditions (WHO 2001). This is useful for understanding the wider perspectives of health and work ability and looking at work functioning on a contextual basis.
Female HSO workers on long-term sick leave
The importance of adjustment latitude for RTW has been investigated in a group that have prolonged sick leave and RTW, i.e. female HSO workers (Dellve et al. 2006a; Leijon et al. 2004; Whittaker et al. 2012). The physical work and work stress conditions, observed in this group, contribute to long-term sick leave (Holmgren et al. 2009; Melchior et al. 2005). The most prevalent reasons for long-term sick leave in this group are musculoskeletal and/or mental health symptoms (Dellve et al. 2006b; Laaksonen et al. 2010). These symptoms may be interrelated, which may also prolong the RTW (Savikko et al. 2001; Vaez et al. 2007).
Yet, only a few studies on taking breaks have been conducted among HSO workers. For example, nurses’ difficulties in obtaining adequate rest breaks have been demonstrated in a diary study (Rogers et al. 2004). Conformist workplace thinking and attitudes that all individuals should be treated equally and similarly despite differences in individual needs may be important obstacles for return to work (Dellve and Hallberg 2008).
Aim
The aim of the study was to generate knowledge about the importance of adjustment latitude at work and at home for return to work or regaining work ability for female HSO workers on long-term sick leave. The hypotheses are that (a) higher levels of adjustment opportunities at work are related to increased work ability and pulling return to work; (b) adjustment latitude that increases opportunities for recovery, e.g. adjustments regarding place and pace of work, is associated with increased work ability and is pulling RTW; (c) low adjustment latitudes at home are pushing RTW.
Methods
Design
A cohort of female human service workers on long-term sick leave was followed three times at 6-month intervals (baseline, 6, and 12 months, T1–T3) and thereafter with long-term 6-year follow-up (T4). Longitudinal analyses were conducted to assess whether adjustment latitude determined increased work ability and return to work.
Study sample
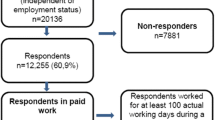
A cohort of female HSO workers who were employed by a major city in Sweden began the study in August 2005. Of the more than 20 independent city municipalities, 12 municipalities that represented various socio-economic statuses were included in the cohort. All employees who fulfilled our inclusion criteria could be included. These criteria were as follows: being female and being on long-term sick leave (>60 days) of at least 50 % sick leave of full time. All the employees who met these criteria (n = 633) at this point in time received written information about the study and were asked whether they were interested in taking part or not. About 51 % (n = 324) decided to participate and replied to a baseline questionnaire. Of the individuals who decided to participate (n = 324), 72 % (n = 233) replied in the second wave and 60 % (n = 194) in the third wave. One hundred and eighty-five individuals (n = 185) decided to participate in the long-term follow-up at 6 years after baseline. At the long-term follow-up, 41 individuals were retired because of age or illness/injury and thus excluded from the analysis for the present study. In total, there were 283 individuals included from the baseline in this study (n = T1, 283; T2, 192; T3, 153; T4, 144). The majority of the study group were 45–54 years of age, cohabiting or married, employed within home care, and on full-time sick leave (85–100 %) at baseline (Table 1). Most of the females had musculoskeletal and/or mental health disorders, stress symptoms, and/or neck pain. Only 5 % of the females had neither stress symptoms nor neck pain.
Explanatory variables
Numbers of adjustment latitudes at work were measured by a multi-part question developed from Johansson et al. (2006): “What opportunities do you have to adjust your work on days when you do not feel well? (Judge the work you had before being off sick)”. Nine ways of adjusting were presented: (1) can do necessary work and postpone the rest; (2) can choose among work tasks; (3) can get help from workmates; (4) can work at a slower pace than usual; (5) can take longer breaks; (6) can shorten the work day; (7) can go home and do the work later; (8) can work without being disturbed at the work place; and (9) can work from home. The three possible answers for each of the nine ways were “always”, “sometimes”, or “never”. In the analysis, three index categories were created (having 0–3, 4–6, or 7–9 opportunities) (Johansson et al. 2006). Pace-related adjustments were measured by categorising the above questions 4, 5, and 8. Place-related adjustments were measured by categorising the above questions 6, 7, and 9 into an index.
Taking short breaks was defined as taking a rest of less than two minutes during work at the workplace for muscular relaxation either through relaxation, rest, or doing something else. Two items considered the usual frequency of taking a rest during work at home (e.g. while cleaning) or at work (response scale: never/less than once per hour, 1–3 times per hour, and more than 3 times per hour). Acceptance of breaks at work and acceptance of breaks at home, (I agree totally—I do not agree at all, score 1–6).
Managerial position was defined as being responsible for the work environment, budget, and operations (assessed with a single item).
Adjustment latitudes at home were indicated as follows: single or shared household; responsibility for household work (shared or less than 50 %, >50 %, >75 %); children living at home; and caretaking of family member (<10 h per week or >10 h per week).
For description of the study group, stress was measured by a validated single-item question (Elo et al. 2003), pain in neck/shoulder/back was measured by three items (Von Korff et al. 1992), and musculoskeletal disorder and mental health disorder with items from Work Ability Index (WAI) (Ilmarinen 2009).
Outcome variables
Work ability was assessed by the work ability score (WAS, 0–10) (Ilmarinen 2006), a validated single item from the Work Ability Index (Ahlstrom et al. 2010). WAS can be divided into four categories: poor (0–5), moderate (6–7), good (8–9), and excellent (10) (Gould et al. 2008).
Sick leave and return-to-work status were measured by items of the current status of working degree, 0–100 %.
Analysis
First, the descriptive statistics were calculated for the variables studied. Second, prevalence ratios (PRs) with 95 % confidence intervals (CI) were calculated to examine possible prospective associations between the independent variables and the dependent variables studied. Third, independent variables that were found to be significant (p < 0.05) were further analysed with mixed models repeated measurements. These analyses were done with different models; the explaining variables for the models were adjustment latitude at work and home, acceptance of breaks at work and home, and time (T1, T2, T3, T4). The outcome variables were work ability and working degree, and the variables were presumed to be continuous variables. Data for assessment were assumed to be normally distributed. All least square mean analyses were statistically significant at p ≤ 0.001. Data were analysed using version 11 of the JMP ® software package (SAS Institute Inc., Cary, NC, USA).
Results
Work ability and return to work
Most subjects (69 %) were on full-time sick leave at baseline and had been on sick leave for more than 1 year (63 %). At the 6-month follow-up, 37 % worked 50 % or more. About half (52 %) worked 50 % or more at the 12-month follow-up, while at the long-term follow-up, only 13 % of the individuals were not working and 54 % worked full time.
Most subjects were classified as having poor (67 %) or moderate (19 %) work ability according to WAS categories at baseline, while only a few (11 %) had a good or excellent work ability (Table 2). At the long-term follow-up, T4, more than half (54 %) scored poor or moderate work ability, and 10 % scored excellent work ability at the 6-year follow-up. WAS had increased among 29 % at the first follow-up and among 51 % in the second follow-up. The mean WAS of the individuals changed from 3.90 at baseline to 6.7 at the 6-year follow-up.
Adjustment latitudes
A high level of adjustment latitude at work was associated with increased work ability and return to work (Table 3). Adjustments related to work pace were strongly associated with increased working degree and increased work ability. Workplace adjustments were also associated with increased work ability. Perceiving a general acceptance at work for taking short breaks was associated with increased return to work. Associations between having good opportunities to take short breaks at work and increased work ability were also indicated. Of the adjustment latitudes investigated at home, a greater responsibility for household work was associated with increased return to work. Acceptance of taking breaks at home was negatively associated with increased work ability and return to work.
The same patterns of results were shown in the long-term importance of adjustment latitude, which were estimated by repeated measurement mixed models. The results showed that working conditions that allowed the individual to make a high degree of adjustments, and a workplace that accepted breaks, were related to a greater increase in work ability (Table 4) and return to work (Table 5) over time, and scored higher on WAS and working degree compared to those individuals not having these conditions. Regarding the acceptance of breaks at home, in the long-term, individuals who reported acceptance of taking breaks at home scored lower on working degree than the group reporting no acceptance for taking breaks at home.
One-way ANOVA was used to investigate the importance of adjustment latitude for increased work ability and working degree. The result showed that these conditions did not significantly change the importance of adjustment latitude on increased work ability or working degree (T1–T3). In other words, the outcome did not differ significantly with or without these conditions. However, prolonged pain had an interactive effect on decreased work ability. Adjustment latitude was associated with increased work ability [mean difference 6.7 (2.1; 11.7)] and working degree [mean difference 27 (7.0; 49.0)] between T1 and T3 among individuals with persisting pain. However, there was an indicated difference in increased work ability between high levels of adjustment latitude with or without prolonged pain [mean difference 4.8 (0.5; 9.1)].
Discussion
Challenges related to the return-to-work process from long-term sick leave due to musculoskeletal and mental health symptoms are generally described as multi-factorial. This study, which focused on adjustment latitudes, showed the importance of flexibility for adjustments for return to work among female HSO workers on sick leave. Taking the results together, the results support RTW as a decision process, wherein the individual chooses to be in an environment where the individual best can handle his or her health (e.g. where the household work is shared or there is acceptance of short breaks when needed). Accordingly, the individual stays where there are opportunities to take needed breaks and make the desirable work adjustment. These findings support the push and pull theories for individual decisions on taking or staying on sick leave (de Vries et al. 2011; Hultin et al. 2010; Johansson et al. 2012) and extends the definitions of pushing and pulling conditions as a protection of self (Stikeleather 2004) or as related to economic or labour market conditions (Stattin 2005). The concept Margin of Manoeuvre is in line with the concept of adjustment latitudes for RTW (Durand et al. 2009); however, it also includes employers’ perspectives of prioritising worker productivity and achievement of company goals.
Most of the earlier studies were cross-sectional, and this study contributes by identifying the importance of adjustment latitude over time. This study also analysed the importance of types of adjustments, for example, pace- and place-related adjustments and adjustment-related conditions at home. Work pace adjustments showed the strongest relation to return to work. In addition, adjustment latitude of the workplace, as well as workplace acceptance of taking short breaks, was associated with increased work ability and return to work. The result supports earlier findings of the importance of work-time flexibility (Krause et al. 1998) and opportunities to take unscheduled breaks for maintaining or improving health. This may also add knowledge that can be related to earlier findings showing that different types of rest break activities, such as undisturbed relaxation in comparison with socialising, lead to different levels of recuperation and reduced strain (Krajewski et al. 2010).
Earlier studies have highlighted the individual’s sense of control as being important for the return-to-work process (Ahrberg et al. 2010). Individuals’ attitudes and beliefs about return to work (Heymans et al. 2006) and having a high degree of influence over one’s own rehabilitation process have explained why workers on long-term sick leave return to work (Landstad et al. 2009). The individuals’ control may be supported, or less hindered, by organisational flexibility with a high degree of adjustment latitude. Thus, it seems important to organise working life in a manner that allows individuals with decreased work ability because of health problems to make the necessary adjustments. Organisational flexibility for high individual adjustment latitude may enhance an inclusive working life and contribute to explaining the differences in long-term sick leave because of occupation and position. The results suggest the importance of dialogue between the person on sick leave, the employer, and the occupational health service regarding the necessary organisational flexibility and work adjustments.
Methodological limitations
The focus on a female occupation group in a gender-segregated sector was deliberate in order to gain more knowledge about conditions for females from one of the first generations where the combination of paid work and domestic work is common. Further, this group also has a comparable high degree of long-term sick leave. Many conditions influence return to work, but this study only focussed on one conceptual condition. It is both a strength to have a narrow focus and a limitation not to control for all other important aspects. However, the analysis was strengthened by repeated measurements. Strengths are also the prospective design with a long-term follow-up. Further, the questionnaire comprised internationally used validated instruments.
Presumably, some jobs and positions have more adjustment latitude than others. However, there was great variation in adjustment latitude in the sample of human service workers. In this study, there were some conditions that can be related to adjustment latitude that were non-significant. Having a managerial position usually implies higher work control that could imply high adjustment latitude. However, managers in Swedish human service organisation have, during the last decade, been put under high pressure due to new public management reforms (Skagert et al. 2008). These conditions have, however, not been associated with managerial turnover (Skagert et al. 2012). This could be a reason for the non-significant associations with RTW. Further, caring needs could be a condition that are pulling the female to stay at home and not return to work (Voss et al. 2008). The non-significant associations with caring needs in this study could, among other aspects, be explained by a well-functioning social insurance support in Sweden regarding these issues.
Conclusions
To improve return to work and increase working degree, it is important that occupational medicine professionals consider the whole life situation regarding opportunities to recover for female human service workers on long-term sick leave. These results support push and pull theories for individual decision-making on return to work.
References
Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L (2010) The work ability index and single-item question: associations with sick leave, symptoms, and health-a prospective study of women on long-term sick leave. Scand J Work Environ Health 36(5):404–412. doi:10.5271/sjweh.2917
Ahlstrom L, Hagberg M, Dellve L (2012) Workplace rehabilitation and supportive conditions at work: a prospective study. J Occup Rehabil. doi:10.1007/s10926-012-9391-z
Ahrberg Y, Landstad BJ, Bergroth A, Ekholm J (2010) Desire, longing and vanity: emotions behind successful return to work for women on long-term sick leave. Work 37(2):167–177. doi:10.3233/WOR-2010-1067
Beemsterboer W, Stewart R, Groothoff J, Nijhuis F (2009) A literature review on sick leave determinants (1984–2004). Int J Occup Med Environ Health 22(2):169–179. doi:10.2478/v10001-009-0013-8
Bolin K, Jacobson L, Lindgren B (2002) The family as the health producer—when spouses act strategically. J Econ 21(3):475–495. doi:10.1016/S0167-6296(01)00135-7
de Vries H, Brouwer S, Groothoff J, Geertzen J, Reneman M (2011) Staying at work with chronic nonspecific musculoskeletal pain: a qualitative study of workers’ experiences. BMC Musculoskelet Disord 12(1):126
Dellve L, Hallberg LRM (2008) “Making it work in the frontline” explains female home care workers’ defining, recognizing, communicating and reporting of occupational disorders. Int J Qual Stud Health Well-being 3(3):176–184
Dellve L, Karlberg C, Allebeck P, Herloff B, Hagberg M (2006a) Macro-organisational factors, the incidence of work disability and work ability among the total work force of home care workers in Sweden. Scand J Public Health 34:17–25
Dellve L, Samuelsson L, Tallborn A, Fasth A, Hallberg LR (2006b) Stress and well-being among parents of children with rare diseases: a prospective intervention study. J Adv Nurs 53(4):392–402. doi:10.1111/j.1365-2648.2006.03736.x
Durand M, Vézina N, Baril R, Loisel P, Richard M, Ngomo S (2009) Margin of manoeuvre indicators in the workplace during the rehabilitation process: a qualitative analysis. J Occup Rehabil 19(2):194–202. doi:10.1007/s10926-009-9173-4
Elo AL, Leppanen A, Jahkola A (2003) Validity of a single-item measure of stress symptoms. Scand J Work Environ Health 29(6):444–451
Geurts SAE, Sonnentag S (2006) Recovery as an explanatory mechanism in the relation between acute stress reactions and chronic health impairment. Scand J Work Environ Health 32(6):482–492
Gould R, Ilmarinen J, Järvisalo J, Koskinen S (2008) Dimensions of work ability—results of the health 2000 survey. Waasa Graphics, Waasa
Hagg GM, Astrom A (1997) Load pattern and pressure pain threshold in the upper trapezius muscle and psychosocial factors in medical secretaries with and without shoulder/neck disorders. Int Arch Occup Environ Health 69(6):423–432
Heymans MW, de Vet HC, Knol DL, Bongers PM, Koes BW, van Mechelen W (2006) Workers’ beliefs and expectations affect return to work over 12 months. J Occup Rehabil 16(4):685–695. doi:10.1007/s10926-006-9058-8
Holmgren K, Dahlin-Ivanoff S, Bjorkelund C, Hensing G (2009) The prevalence of work-related stress, and its association with self-perceived health and sick-leave, in a population of employed Swedish women. BMC Public Health 9:73. doi:10.1186/1471-2458-9-73
Hultin H et al (2010) Low level of adjustment latitude—a risk factor for sickness absence. Eur J Public Health 20(6):682–688. doi:10.1093/eurpub/ckp240
Ilmarinen J (2006) Towards a longer and better working life: a challenge of work force ageing. Med Lav 97:143–147
Ilmarinen J (2009) Work ability-a comprehensive concept for occupational health research and prevention. Scand J Work Environ Health 35(1):1–5. doi:10.5271/sjweh.1304
Janga D, Akinfenwa O (2012) Work-related repetitive strain injuries amongst practitioners of obstetric and gynaecological ultrasound worldwide. Arch Gynecol Obstet 286(2):353–356. doi:10.1007/s00404-012-2306-6
Johansson G, Lundberg I (2004) Adjustment latitude and attendance requirements as determinants of sickness absence or attendance. Empirical tests of the illness flexibility model. Soc Sci Med 58(10):1857–1868. doi:10.1016/S0277-9536(03)00407-6
Johansson G, Lundberg O, Lundberg I (2006) Return to work and adjustment latitude among employees on long-term sickness absence. J Occup Rehabil 16(2):185–195. doi:10.1007/s10926-006-9020-9
Johansson G, Hultin H, Möller J, Hallqvist J, Kjellberg K (2012) The impact of adjustment latitude on self-assessed work ability in regard to gender and occupational type. Scand J Occup Ther 19(4):350–359. doi:10.3109/11038128.2011.603354
Krajewski J, Wieland R, Sauerland M (2010) Regulating strain states by using the recovery potential of lunch breaks. J Occup Health Psychol 15(2):131–139. doi:10.1037/a0018830
Krause N, Dasinger L, Neuhauser F (1998) Modified work and return to work: a review of the literature. J Occup Rehabil 8(2):113–139. doi:10.1023/a:1023015622987
Laaksonen M, Mastekaasa A, Martikainen P, Rahkonen O, Piha K, Lahelma E (2010) Gender differences in sickness absence—the contribution of occupation and workplace. Scand J Work Environ Health 36(5):394–403
Landstad BJ, Wendelborg C, Hedlund M (2009) Factors explaining return to work for long-term sick workers in Norway. Disabil Rehabil 31(15):1215–1226. doi:10.1080/09638280802510999
Larsson TJ, Normark M, Weigelt A, Åhlgren M, Åkerström T (2014) Allvarliga arbetsskador och långvarig sjukfrånvaro [Serious occupational disorders and long term sickness absence] AFA Försäkring
Leijon M, Hensing G, Alexanderson K (2004) Sickness absence due to musculoskeletal diagnoses: association with occupational gender segregation. Scand J Public Health 32(2):94–101
Melchior M, Krieger N, Kawachi I, Berkman LF, Niedhammer I, Goldberg M (2005) Work factors and occupational class disparities in sickness absence: findings from the GAZEL cohort study. Am J Public Health 95(7):1206–1212. doi:10.2105/AJPH.2004.048835
Rogers AE, Hwang WT, Scott LD (2004) The effects of work breaks on staff nurse performance. J Nurs Adm 34(11):512–519
Savikko A, Alexanderson K, Hensing G (2001) Do mental health problems increase sickness absence due to other diseases? Soc Psychiatry Psychiatr Epidemiol 36(6):310–316
Skagert K, Dellve L, Eklöf M, Ljung T, Pousette A, Ahlborg G (2008) Leadership and stress in public human service organisations: acting shock absorber and sustaining own integrity. Appl Ergon 39(6):803–811
Skagert K, Dellve L, Ahlborg G Jr (2012) A prospective study of managers’ turnover and health in a healthcare organization. J Nurs Manag 20(7):889–899. doi:10.1111/j.1365-2834.2011.01347.x
Stattin M (2005) Retirement on grounds of ill health. Occup Environ Med 62(2):135–140. doi:10.1136/oem.2004.015669
Stikeleather J (2004) An older worker’s decision to “push or protect self” following a work-related injury. Work 22(2):139–144
Tucker P (2003) The impact of rest breaks upon accident risk, fatigue and performance: a review. Work Stress 17(2):123–137. doi:10.1080/0267837031000155949
Tuomi K, Huuhtanen P, Nykyri E, Ilmarinen J (2001) Promotion of work ability, the quality of work and retirement. Occup Med (Lond) 51(5):318–324
Vaez M, Rylander G, Nygren A, Asberg M, Alexanderson K (2007) Sickness absence and disability pension in a cohort of employees initially on long-term sick leave due to psychiatric disorders in Sweden. Soc Psychiatry Psychiatr Epidemiol 42(5):381–388. doi:10.1007/s00127-007-0189-9
Veiersted KB, Westgaard RH, Andersen P (1993) Electromyographic evaluation of muscular work pattern as a predictor of trapezius myalgia. Scand J Work Environ Health 19(4):284–290
Visser B, van Dieen J (2006) Pathophysiology of upper extremity muscle disorders. J Electrom Kinesiol 16:1–16
Von Korff M, Ormel J, Keefe FJ, Dworkin SF (1992) Grading the severity of chronic pain. Pain 50(2):133–149
Voss M et al (2008) The influence of household work and of having children on sickness absence among publicly employed women in Sweden. Scand J Public health 36(6):564–572. doi:10.1177/1403494807088459
Whittaker W et al (2012) The effect of mental ill health on absence from work in different occupational classifications: analysis of routine data in the British Household Panel Survey. J Occup Environ Med 54(12):1539–1544. doi:10.1097/JOM.0b013e3182677d12
WHO (2001) International classification of functioning, disability and health (ICF). Word Health Organization, Geneva
Acknowledgments
We are grateful to the Swedish Research Council for Health, Working Life and Welfare (FORTE) for financial support.
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical standards
The project was approved by the Ethics Committee for Gothenburg Region in 2005 and supplemented regarding the 6-year long-term follow-up in 2012.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dellve, L., Fallman, S.L. & Ahlstrom, L. Return to work from long-term sick leave: a six-year prospective study of the importance of adjustment latitudes at work and home. Int Arch Occup Environ Health 89, 171–179 (2016). https://doi.org/10.1007/s00420-015-1061-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00420-015-1061-y