
Abstract
Objective
This systematic review and meta-analysis aims to assess the refractive outcomes of the Yamane technique for intrascleral fixation of intraocular lenses (SF-IOL) and compare the predictive ability of the various intraocular lens power calculation formulae commonly used in conjunction with the technique.
Methods
A literature search was conducted in the Medline, Scopus, and Cochrane Library databases for articles published from January 2014 to May 2023. Studies that met the predetermined inclusion criteria were included and subjected to analysis. The primary outcome evaluated was the refractive predictive error, defined as the difference between predicted refraction and post-operative manifest refraction.
Results
Eleven studies met the inclusion criteria, with a cumulative sample size of 615 patients (mean age: 66.6 years). Various IOL formulae were used, with SRK/T being the most frequently adopted formula. The overall mean refractive predictive error for all formulae combined was -0.02 D, which was not statistically significant (p = 0.99). Subgroup analysis for individual formulae also showed no significant difference from predicted error for any formula (p > 0.05).
Conclusion
The Yamane technique for SF-IOL shows promising refractive outcomes, and the choice of IOL power calculation formula should be tailored based on patient characteristics and surgeon preference. No formula demonstrated superior predictive ability over others. Further research is needed to develop formulae specifically for eyes with secondary aphakia and poor capsular support.
Key messages
What is known
-
• The new generation intraocular lens power formulas are very accurate in planning post-operative refractive error in routine phacoemulsification and intraocular lens implants.
-
• Yamane technique is a highly effective and safe technique for secondary intraocular lens implant in patients with insufficient capsular support.
What is new
-
• There is no consensus on which intraocular lens formula gives best predicted post-operative refractive correction after Yamane technique of secondary intraocular lens surgery.
-
• Can we use artificial intelligence and regression analysis based intraocular lens formula for aphakic patients?
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Aphakic eyes with poor capsular support can often not be managed with conventional, in-the-bag IOL placement [1]. Traumatic capsular tears and zonular weakness may be present pre-procedure, or develop intra-operatively during in-the-bag IOL placement [2]. Conditions such as Marfan’s syndrome and Pseudoexfoliation syndrome also pose challenges for intracapsular IOL placement. Luxation of traditionally placed IOLs has been reported to be rising, indicating a greater need for secondary IOL fixation [3].
Intrascleral fixation of IOL (SF-IOL) is a popular technique for secondary IOL fixation [4], and is considered as safe, if not safer than other techniques such as the anterior chamber IOL and the iris claw IOL [5,6,7]. It reduces the risk of damage to the anterior chamber angle and cornea, hence lowering the risk of inflammatory damage to the eye. Further, the technique provides better quality of vision due to the posterior positioning of the lens behind the iris [4]. Various techniques have been reported for SF-IOL, including methods that use conjunctival flaps, fibrin glues, conjunctival sutures, and specially produced IOLs [8,9,10]. However, these may not always be possible due to the unavailability of the specially developed IOL in remote and economically challenged regions, or the complexity of procedure.
Dr. Shin Yamane shared with the world a technique for SF-IOL in 2014 as an easier surgical procedure for sutureless and glueless fixation of the posterior chamber IOL [11]. However, it was his revised technique in 2017 [12], now synonymous with the Yamane technique, that became recognized as a simpler solution for SF-IOL. The key aspects of the technique include two angled sclerotomies, 180º from each other, and 2 mm away from the limbus, each for the externalization of a haptic of the 3-piece IOL. Further, the creation of flanges on the haptics via an ophthalmic cautery device and burying them in the sclerotomies.
Refractive outcomes remain a concern for cataract surgeons, especially in eyes with secondary aphakia. The complicated anatomy and atypical biometry make the use of standard formulae extremely difficult. Errors in IOL power calculation have been associated with patient dissatisfaction and the need for IOL exchange [13]. The associated time, cost, and the risk of intra-operative and post-operative complications makes the extra surgery a challenge and an inconvenience for patient and surgeon. The variety of available formulae and their multiple generations for IOL power calculation all have their caveats and evidence suggests that no single formula outperforms all others for eyes of different characteristics [14, 15]. Some studies have mentioned that the newer generation formulae such as the Barrett Universal II have better accuracy compared to second and third generation formulae such as the SRK/T [16], while others suggest the use of “super-formula” developed from results of multiple formulae for more accurate IOL power calculation [17]. More recent studies have focused on results from artificial intelligence and machine learning models [18, 19].
As with other methods of lens implantation, the correct prediction of effective lens position and refractive power remains essential for optimal outcomes and patient satisfaction with the Yamane technique for SF-IOL. Previous studies have not reported significantly improved accuracy of refractive predictability of any of the common formulae over the others in the setting of SF-IOL post Yamane technique. The results have shown great unpredictability with many of the third generation and newer formulae [20]. Our review and meta-analysis aims to study the predictive ability of the various formulae across studies and compare the refractive predictive error associated to each formula to other formulae in literature.
Methods
We conducted our systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA.) [21] The review was prospectively registered on PROSPERO, International prospective register of systematic reviews under ID: CRD42023429978.
Search strategy
A literature search, using the Medline and Scopus databases, as well as the Cochrane Library was conducted for articles published from January 2014 to May 2023. This timeframe was chosen as the first introduction to a sutureless technique by Dr. Yamane was provided in 2014. Articles pre-dating Yamane’s original presentation were automatically excluded. To ensure no relevant article was missed, no other filter was used for the search. Each database was researched by either of two independent researchers (AHK and ASG) in accordance with the PRISMA guidelines. The key terms utilized to build the search strategy were “Yamane,” “Sutureless,” “flange,” “refractive outcomes,” “refractive error,” “IOL,” and “intraocular lens,” combined using the Boolean operators “AND” and “OR.” The search strategy included relevant MeSH terms of each database and synonyms to ensure comprehensive coverage [Supplement Methods]. All results of the search were downloaded for record and later use.
Screening and selection
The results from each database were uploaded to the software “Rayyan,” (available at Rayyan.ai) an AI based tool for independent collaboration and ease of conducting reviews. The software allows easy removal of duplicates by screening text for similarities and via the use of keywords, highlights important parts of the abstract and title to facilitate efficient screening. Title and abstract based screening was performed independently by AHK and ASG. The reviewers were blinded for screening using the feature available in the software, and this blind was removed once each reviewer had completed their screening. Disagreements were then resolved upon discussion. One reviewer (AHK) was responsible for full-text screening based on the detailed eligibility criteria formulated by consensus of all authors.
Eligibility criteria
The inclusion criteria were:
-
1.
Studies where the IOL placement was performed via the Yamane technique or any similar techniques, where sclerotomies were performed 2 mm posterior to the limbus and the IOL haptics were cauterized to secure the IOL.
-
2.
Studies which mentioned the formula used for pre-surgical IOL power and refractive error calculation.
-
3.
Studies where post-surgical refractive predictive error was reported.
-
4.
Articles in the English Language only.
The exclusion criteria were:
-
1.
Case reports, case series with a sample of < 10 eyes of patients, reviews, abstracts, conference presentations, editorials and expert opinions.
-
2.
Studies which were conducted exclusively on pediatric populations.
-
3.
Studies where additional surgeries, other than total or partial vitrectomy, were performed or scleral flaps were created for fixation of IOL.
-
4.
Studies which did not report a measure of central tendency for mean refractive predictive error.
-
5.
Literature published before January 2014, when Dr. Yamane first shared a technique for Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation, albeit with lamellar scleral dissection.
-
6.
Studies not conducted on humans.
Data extraction
Following full-text review, the same reviewer proceeded with data extraction onto an online-maintained Excel spreadsheet. This allowed the data to be rechecked by a second reviewer (ASG) to ensure accuracy and avoid errors. Data extracted included study characteristics (author, year, design) and patient characteristics, (sample size, mean age) as well as other important data on the details of the procedure such as the machine used to perform biometry, the lens used, and any additional procedures done as part of intervention.
In addition, two reviewers (AHK and ASG) utilized the National Heart, Lung, and Blood Institute (NHLBI) study quality assessment tools, to ensure high quality of studies that were to be included in the review and analysis. In particular, the “Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group” was used.
Outcomes
The primary outcome assessed as part of this systematic review and meta-analysis was the refractive predictive error associated with different IOL formulae. The refractive predictive error is defined as the difference between the manifest refractive error and the predicted refractive error.
Analysis
Following the extraction, cleaning, and verification of data on Microsoft Excel, data was manually exported to Review Manager version 5.4. A Random-effects, Generic-Inverse model was used for analysis of the different refractive predictive errors across studies. The element of myopic or hyperopic surprise, defined as deviation of the values from zero, was plotted on the x-axis of the forest plots. Funnel plots were assessed to understand possible publication bias in the studies. Heterogeneity in the studies was assessed automatically by the software, and a 50% I2 value cut-off was set for unexplained heterogeneity. Sensitivity analysis was done by the leave-one-out method to evaluate robustness of the meta-analysis.
Results
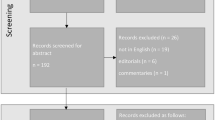
Our initial search strategy resulted in a cumulative 288 articles from the 3 databases we accessed. This was narrowed down to 35 articles for full text review after removing duplicates and performing title and abstract screening. We were finally left with 11 studies [12, 22,23,24,25,26,27,28,29,30,31] to include in our analysis. Details about this process can be found in Fig. 1. The inter-reviewer agreement and reliability was assessed via Cohen’s Kappa coefficient and was found to be 0.73. The 11 included studies all achieved high scores on the NHLBI quality assessment tool and were subsequently included in our study.

The PRISMA 2020 statement: an updated guideline for reporting systematic reviews [21]
Table 1 describes the characteristics of the included studies. The cumulative sample size was 615 and the mean age of the participants was 66.6 years. The mean axial length was found to be 24.88 mm. The type of IOL used varied greatly but the most common were NX-70, CT Lucia 602 and ZA9003, which utilized in 181, 147 and 132 cases respectively. IOL master was the tool most frequently used for ocular biometry. The needle used for the procedure varied between 30 gauge and 27 gauge, but 30 gauge was used in 441 cases as compared to 74 cases for 27 gauge. The Yamane technique was frequently accompanied with pars plana vitrectomy as well as anterior vitrectomy in a few cases. 2 studies (172 cases) had peripheral iridotomy performed for all cases, which is commonly done to prevent iris capture [12].
There were seven different IOL formulae utilized, that included third generation (SRK/T, Holladay I, Hoffer) fourth generation (Holladay II, Haigis) and newer generation formulae (Hill-RBF and Barrett Universal II.) The most commonly utilized formula was SRK-T, which was reported in 9 studies. This was followed by Barrett Universal II and Holladay I, which were reported in 4 and 3 studies respectively. Refractive Predictive errors for the different formulae used in each study can be found in Table 2.
Our meta-analysis found that the mean refractive predictive error in the included studies irrespective of formula used was -0.02 D, which was statistically insignificant with a p-value of 0.99 (Fig. 2). Subgroup analysis was run for individual IOL formulae. SRK/T, which was the most frequently used formula, had a mean refractive predictive error of -0.06 D (p = 0.68), which was statistically insignificant. The mean refractive predictive errors associated with Holladay I and Barrett II were 0.40 D (p = 0.62) and -0.11 D (p = 0.95) respectively. Overall heterogeneity as well as heterogeneity for each subgroup was 0, which is indicative of minimal variability in the data included in our study, suggesting reliability of results. Given the disproportionate weightage of two studies in our analysis, we used the leave-one-out method to evaluate if they significantly skew the analysis. Upon dropping Noguchi’s study [31], the mean predictive error of SRK/T formula and the overall study changed to -0.35 (p = 0.20) and -0.12 (p = 0.58) respectively. Upon dropping Kelkar’s results [22], the predictive error of SRK/T formula and the overall predictive error changed to 0.03 (p = 0.81) and 0.06 (p = 0.64) respectively. Though we see a change in mean values, the findings are still not statistically significant. This reaffirms the reliability of our analysis.

Forest plot displaying mean refractive predictive error associated with Yamane technique. Subgroup analysis was performed for individual formulae
Discussion
This review and meta-analysis is the first to highlight the refractive outcomes of Yamane’s SF-IOL technique. We report the difference between predicted refraction and post-operative manifest refraction for various formulae of IOL power calculation across studies. Multiple generations of power calculation formulae have been developed [32], however, none have been developed specifically for calculations in eyes set to undergo SF-IOL. We report the refractive prediction error for 7 different formulae that have been used in the setting of SF-IOL.
What sets Yamane’s technique apart from other flanged, sutureless techniques, is the standardization of performing the sclerotomy precisely 2.0 mm from the limbus, ensuring a standardized effective lens position is achieved. The effective lens position is a key variable and cause of error in most formulae and this standardization ensures better precision of predicted refraction [33].
A single needle technique modification of the Yamane technique has also been popularized [34], as well as modifications where larger bore needles such as 27-gauge needles have been used instead of the 30-gauge needle in Yamane’s recommendation [35]. The outcomes following these modifications have been well studied, and most have found a similar safety profile and efficacy to the original technique [35, 36]. This potentiates the use of 27-gauge needles and minor modifications like the single needle technique, when the 30-gauge double needle technique may not be feasible. This can be due to various factors including availability of equipment and surgical preference. Providing the operating surgeon with this flexibility should improve acceptance of the flanged SF-IOL technique as a simpler, quicker, and safer approach than the anterior chamber IOL and the iris claw IOL.
Despite its many advantages, the sutureless SF-IOL techniques have their own set of challenges. Early (hypotony, transient rise in IOP, transient corneal edema and vitreous hemorrhage) and late (retinal detachment, pupillary capture, cystoid macular edema, IOL decentration and tilt) postoperative complications are rare, but can greatly affect patient experience. The complications require timely management including topical NSAIDS, anti-glaucoma medications, laser therapies, or surgical correction of tilt and decentration when needed.
Most of the studies (9/11) included in our analysis have used the SRK/T formula, while the next most popular formula, Barrett Universal II, was used in less than half the studies. (4/11) This finding is consistent with literature as SRK/T and BUII are the most used third and fourth generation formulae respectively [32, 37]. No study in our analysis reported the use of Kane’s formula [38], a newer generation formula based on regression and artificial intelligence that has been gaining popularity with great results in literature [39, 40]. However, this finding can be explained by the difficulty measuring anterior chamber depth in aphakic eyes, that is required for Kane’s formula [20]. This problem has also been mentioned for the use of Haigis (fourth generation) and Hill-RBF (newer generation) formulae in a study included in our review [30].
Alignment of achieved refraction with predicted refraction is crucial for ensuring patient satisfaction and accurate visual outcomes. We saw no significant difference from the predicted error for any formula included in our review. (p > 0.05) The weighted mean difference of predicted refraction from manifest refraction (-0.02 [-0.25, 0.21]) for the cumulative result of all formulae did not elicit any significance (p = 0.85.) Similarly, the subgroup difference for all formulae was not significant (p = 0.96.) These findings support the idea that the observed variability in refractive outcomes for the different formulae across studies is not significant, and we fail to identify one formula that outperforms any other based on refractive outcome. This result has also been seen in a different meta-analysis for outcomes of IOL power calculation in primary angle-closure conditions [41]. Two meta-analyses found differences in performance of the IOL formulae in the settings of long eyes, and short eyes respectively [42, 43], however, we do not have the data required to study the groups separately in our analysis. We find that despite some deviation from the predicted refractive error, the manifest refraction across the formulae varies insignificantly and is more likely to be affected by characteristics including inter-surgeon variability, pre and post operative biometry, and measurement equipment. Our finding emphasizes the importance of individualized selection of formula, based on patient characteristics and surgeon preference. We would also like to highlight the need to develop formulae specifically for secondary aphakic eyes, like in the setting of Yamane’s technique for SF-IOL.
Statistically insignificant disparity in the predicted and manifest refraction can still however be a cause of discomfort and dissatisfaction for patients, who at an individual level may still require aided correction of vision. Patient and surgeon both aim to achieve unaided vision, and a review highlights post-surgical refraction as a source of displeasure after IOL placement. It also identifies that patients may pursue laser correction of error, with the extra surgery adding to the burden on health systems and patient [44].
Our analysis was limited by the number of good quality studies available for inclusion. We were only able to find 11 studies that met our criteria. This number would further shrink for subgroup analysis and compromise the quality of analysis possible. Only a few of the studies in our analysis reported the absolute predictive error and the number of readings between ± 0.5D or ± 1.0D of the predicted error, which are other metrics used to compare refractive outcomes. Despite 0% identified heterogeneity, the studies are bound to vary in terms of sample size, follow-up duration, and type of IOL used amongst other factors. We were unable to account for minor variations in surgical technique, patient characteristics, and machines used for biometry. These factors may have influenced outcomes and may also be sources of potential bias in the study.
Conclusion
Our systematic review and meta-analysis highlights the flexibility in performing SF-IOL based on Yamane’s technique. Our analysis of the refractive predictive errors associated with various formulae for IOL power calculation does not find any significant difference between predicted refraction and post-operative manifest refraction and does not identify a formula with outcomes significantly different to the others. The choice of formula remains a decision that must be taken based on patient characteristics and surgeon discretion. In the absence of a universally superior formula, we highlight the need for development of a formula specifically for eyes with secondary aphakia and poor capsular support. The potential of artificial intelligence and machine learning models of IOL power calculations for SF-IOL must be explored to further improve patient outcomes and satisfaction following the innovative surgical intervention.
References
Miller KM, Oetting TA, Tweeten JP et al (2022) Cataract in the Adult Eye Preferred Practice Pattern. Ophthalmology 129:P1–P126
Vounotrypidis E, Schuster I, Mackert MJ et al (2019) Secondary intraocular lens implantation: a large retrospective analysis. Graefe’s Archive Clin Experimental Ophthalmol 257:125
Dabrowska-Kloda K, Kloda T, Boudiaf S et al (2015) Incidence and risk factors of late in-the-bag intraocular lens dislocation: evaluation of 140 eyes between 1992 and 2012. J Cataract Refract Surg 41:1376–1382
Tsatsos M, Vartsakis G, Athanasiadis I et al (2022) Intraocular lens implantation in the absence of capsular support: scleral fixation. Eye 2022 36:9
Kumar DA, Agarwal A, Ali WRK (2019) Uveitis and deficient lens capsules: Effect of glued intraocular lens on the visual outcome and the reactivation of inflammation. Indian J Ophthalmol 67:1610–1616
Madhivanan N, Sengupta S, Sindal M et al (2019) Comparative analysis of retropupillary iris claw versus scleral-fixated intraocular lens in the management of post-cataract aphakia. Indian J Ophthalmol 67:59–63
Chan TCY, Lam JKM, Jhanji V et al (2015) Comparison of outcomes of primary anterior chamber versus secondary scleral-fixated intraocular lens implantation in complicated cataract surgeries. Am J Ophthalmol 159:221–226e2
Agarwal A, Kumar DA, Jacob S et al (2008) Fibrin glue-assisted sutureless posterior chamber intraocular lens implantation in eyes with deficient posterior capsules. J Cataract Refract Surg 34:1433–1438
Monteiro M, Marinho A, Borges S et al (2007) Scleral fixation in eyes with loss of capsule or zonule support. J Cataract Refract Surg 33:573–576
Vaiano AS, Hoffer KJ, Greco A et al (2021) Long-term outcomes and complications of the New Carlevale Sutureless scleral fixation posterior Chamber IOL. J Refract Surg 37:126–132
Yamane S, Inoue M, Arakawa A et al (2014) Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology 121:61–66
Yamane S, Sato S, Maruyama-Inoue M et al (2017) Flanged intrascleral intraocular Lens fixation with Double-Needle Technique. Ophthalmology 124:1136–1142
Jin GJC, Crandall AS, Jones JJ (2007) Intraocular lens exchange due to incorrect lens power. Ophthalmology 114:417–424
Cooke DL, Cooke TL (2016) Comparison of 9 intraocular lens power calculation formulas. J Cataract Refract Surg 42:1157–1164
Aristodemou P, Knox Cartwright NE, Sparrow JM et al (2011) Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refract Surg 37:63–71
Kane JX, Van Heerden A, Atik A et al (2016) Intraocular lens power formula accuracy: comparison of 7 formulas. J Cataract Refract Surg 42:1490–1500
Ladas JG, Siddiqui AA, Devgan U et al (2015) A 3-D Super Surface combining modern intraocular Lens formulas to generate a Super Formula and maximize accuracy. JAMA Ophthalmol 133:1431–1436
Ladas J, Ladas D, Lin SR et al (2021) Improvement of Multiple Generations of Intraocular Lens Calculation Formulae with a Novel Approach using Artificial Intelligence. Transl Vis Sci Technol. ;10
Sramka M, Slovak M, Tuckova J et al (2019) Improving clinical refractive results of cataract surgery by machine learning. PeerJ. ;7
Mcmillin J, Wang L, Wang MY et al (2021) Accuracy of intraocular lens calculation formulas for flanged intrascleral intraocular lens fixation with double-needle technique. J Cataract Refract Surg 47:855–858
Kelkar AS, Fogla R, Kelkar J et al (2017) Sutureless 27-gauge needle-assisted transconjunctival intrascleral intraocular lens fixation: initial experience. Indian J Ophthalmol 65:1450–1453
Randerson EL, Bogaard JD, Koenig LR et al (2020) Clinical outcomes and Lens Constant Optimization of the Zeiss CT Lucia 602 Lens using a modified Yamane Technique. Clin Ophthalmol 14:3903–3912
Torii T, Tamaoki A, Kojima T et al (2020) Comparison of clinical outcomes between intracapsular implantation and intrascleral fixation using the same model of intraocular Lens. Clin Ophthalmol 14:3965–3974
Miura Y, Harada Y, Kiuchi Y (2020) Comparison of Different IOL Types in the Flanged IOL Fixation Technique. J Ophthalmol. ;2020
Rocke JR, McGuinness MB, Atkins WK et al (2020) Refractive outcomes of the Yamane Flanged Intrascleral haptic fixation technique. Ophthalmology 127:1429–1431
Mustafi D, Tom E, Messenger WB et al (2021) Outcomes of sutureless secondary intraocular lens fixation with haptic flanging in a cohort of surgically complex eyes. Graefes Arch Clin Exp Ophthalmol 259:1357–1363
Jujo T, Kogo J, Sasaki H et al (2021) 27-gauge trocar-assisted sutureless intraocular lens fixation. BMC Ophthalmol. ;21
Tokuhisa T, Watanabe T, Watanabe A et al (2022) Refractive error induced by intraocular lens tilt after intrascleral intraocular lens fixation. Int Ophthalmol 42:1213–1220
Malach DS, Guest JM, Adam C et al (2023) Intraocular Lens Formula Comparison of Flanged Intrascleral Intraocular Lens Fixation with double needle technique. Clin Ophthalmol 17:1–6
Noguchi S, Nakakura S, Noguchi A et al (2023) Relationship between Postoperative Anterior Chamber Depth and refraction based on the Haptic fix position in intraocular Lens Intrascleral fixation. J Clin Med 12:1815
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. ;6
Xia T, Martinez CE, Tsai LM (2020) Update on intraocular Lens formulas and calculations. Asia Pac J Ophthalmol (Phila) 9:186
Holladay JT (1997) Standardizing constants for ultrasonic biometry, keratometry, and intraocular lens power calculations. J Cataract Refract Surg 23:1356–1370
Yavuzer K, Evcimen Y (2019) Sutureless transconjunctival intrascleral intraocular lens fixation: the modified Yamane technique. Arq Bras Oftalmol 82:389–393
Suren E, Kalayci M, Cetinkaya E et al (2021) Evaluation of the Findings of Patients Who Underwent Sutureless Flanged Transconjunctival Intrascleral Intraocular Lens Implantation with or without Pars Plana Vitrectomy. J Ophthalmol. ;2021
Tang Y, Gao Y, Chu Y et al (2022) Modified Yamane technique with a 26-gauge needle: single corneal incision and simplified haptic insertion. J Cataract Refract Surg. ;48
Chung J, Bu JJ, Afshari NA Advancements in intraocular lens power calculation formulas. Curr Opin Ophthalmol [Internet]. 2022 [cited 2023 May 28];33:35–40. https://journals.lww.com/co-ophthalmology/Fulltext/2022/01000/Advancements_in_intraocular_lens_power_calculation.8.aspx
Kane Formula [Internet] [cited 2023 May 28]. https://www.iolformula.com/
Ryu S, Jun I, Kim TI et al (2021) Accuracy of the Kane Formula for Intraocular Lens Power Calculation in comparison with existing formulas: a retrospective review. Yonsei Med J 62:1117
Connell BJ, Kane JX (2019) Comparison of the Kane formula with existing formulas for intraocular lens power selection. BMJ Open Ophthalmol. ;4
Lu W, Hou Y, Yang H et al (2022) A systemic review and network meta-analysis of accuracy of intraocular lens power calculation formulas in primary angle-closure conditions. PLoS ONE. ;17
Wang Q, Jiang W, Lin T et al (2018) Accuracy of intraocular lens power calculation formulas in long eyes: a systematic review and meta-analysis. Clin Exp Ophthalmol 46:738–749
Wang Q, Jiang W, Lin T et al (2018) Meta-analysis of accuracy of intraocular lens power calculation formulas in short eyes. Clin Exp Ophthalmol 46:356–363
Kieval JZ, Al-Hashimi S, Davidson RS et al (2020) Prevention and management of refractive prediction errors following cataract surgery. J Cataract Refract Surg 46:1189–1197
Funding
No funding was received for this research.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Khowaja, A.H., Ghazanfar, A.S. & Tayyab, H. Accuracy of intraocular lens power calculation formulae for the Yamane technique of secondary fixation: a systematic review and meta-analysis. Graefes Arch Clin Exp Ophthalmol (2024). https://doi.org/10.1007/s00417-024-06603-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00417-024-06603-w