
Abstract
Purpose
To assess the efficacy and safety of oral saffron, a natural antioxidant, in treating mild/moderate age-related macular degeneration (AMD).
Methods
Randomised, double-blinded, placebo-controlled crossover trial of 100 adults (> 50 years) with mild/moderate AMD and vision > 20/70 Snellen equivalent in at least one eye. Exclusion criteria included confounding visual lesions, or significant gastrointestinal disease impairing absorption. Participants were given oral saffron supplementation (20 mg/day) for 3 months or placebo for 3 months, followed by crossover for 3 months. Participants already consuming Age-Related Eye Diseases Study (AREDS) supplements or equivalent maintained these. Primary outcomes included changes in best-corrected visual acuity (BCVA) and changes in multifocal electroretinogram (mfERG) response density and latency. Secondary outcomes included safety outcomes and changes in mfERG and BCVA amongst participants on AREDS supplements.
Results
Mean BCVA improved 0.69 letters (p = 0.001) and mean-pooled mfERG latency reduced 0.17 ms (p = 0.04) on saffron compared to placebo. Amongst participants on AREDS supplements, mean BCVA improved 0.73 letters p = 0.006) and mean-pooled mfERG response density improved 2.8% (p = 0.038). There was no significant difference in adverse event occurrence (p > 0.10).
Conclusion
Saffron supplementation modestly improved visual function in participants with AMD, including those using AREDS supplements. Given the chronic nature of AMD, longer-term supplementation may produce greater benefits.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Age-related macular degeneration (AMD) remains the most common cause of irreversible visual loss in the developed world, and its impact is predicted to rise as populations age [1]. Despite recent advances in the treatment of advanced disease, particularly neovascular AMD (nAMD) [2, 3], therapeutic options for the most common earlier forms of AMD remain limited. More than 10 years after the publication of the initial landmark, Age-Related Eye Diseases Study (AREDS), dietary modification and nutritional augmentation with AREDS-based supplements still remain the basis of AMD management [4, 5]. Various additions to these therapies have been trialled, but only the addition of lutein/zeaxanthin, two carotenoids that accumulate in retinal tissue, have been well validated [6].
Saffron (Crocus sativus) is a well-known Middle-Eastern spice that has been shown to possess significant antioxidant potential, and has been trialled as a therapy for a range of chronic degenerative diseases [7, 8]. Much of its antioxidant potential stems from the presence of a range of molecules within saffron that have significant chemical similarities to carotenoids [9]. As some carotenoids are known to be effective in treating AMD, it is plausible that other carotenoid molecules may also be effective therapies for AMD without the potential systemic side-effects of carotenoids such as beta-carotene. Saffron and its constituents also have no known significant side-effects at commonly consumed dosages, making it an attractive potential therapeutic for chronic conditions where long-term use may be required [10]. Preliminary investigations have suggested that saffron may be a useful treatment for AMD, however these studies may not have been adequately powered and standardised to assess efficacy [11, 12]. In an effort to better identify possible therapies for this increasingly burdensome condition, we investigated the role of saffron supplementation as a therapy for AMD.
Subjects & methods
A prospective, randomised, placebo-controlled, double blind crossover trial (Registered on Australian and New Zealand Clinical Trials Registry, June 2012, ACTRN 12612000729820) was conducted on 100 participants attending a single tertiary retinal clinic between January 2013 and March 2015. Power calculations indicated that such a sample provided 90% power to detect a difference of 15 nv·deg.−2 in N1P1 response densities on multifocal electroretinogram (mfERG) to a significance level of 0.05, and allowed for a drop-out rate of 10%. All participants provided written consent, and Institutional Ethical Review was obtained via the Sydney South-West Area Health Human Research Ethics Committee prior to study commencement. This research adhered to the tenets of the Declaration of Helsinki.
Inclusion/exclusion criteria
All participants underwent baseline dilated ophthalmic examination and general medical review to confirm the presence of AMD and to assess eligibility under the exclusion/inclusion criteria listed below. Inclusion criteria were as follows: (a) age greater than 50 years, (b) moderate severity AMD (defined as AREDS grade 2 or 3, Fig. 1) affecting at least one eye [13], c) best-corrected visual acuity (BCVA) better than 55 Early Treatment of Diabetic Retinopathy Study (ETDRS) letters (approximately 20/70 Snellen equivalent) in the eye(s) meeting criteria a and b) and (d) ability to provide written consent. Exclusion criteria were: (a) presence of any confounding visual lesion in the study eye(s), including neovascular AMD, proliferative diabetic retinopathy, macular hole or epiretinal membrane, prior macular off retinal detachment, uncontrolled glaucoma, significant corneal or lenticular opacities or active uveitis; (b) prior macular laser therapy for AMD or other retinal disorders; c) prior or current intravitreal pharmacotherapy and (d) gastric or hepatic disorders altering either absorption or metabolism of orally administered saffron. In participants in whom both eyes met eligibility criteria, both eyes were included in the analysis, with 167 eyes meeting inclusion/exclusion criteria.

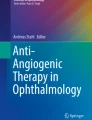
Matched fundus photo and multifocal electroretingram output. Top left: normal participant, middle left: fundus autofluorescence (FAF) showing normal trace, bottom left: normal multifocal electroretinogram (mfERG) output with normal peak height; top right: fundus image of a patient with age-related macular degeneration (AMD), showing central atrophy and drusen (arrow); middle right: FAF from AMD patient showing areas of atrophy (dark patches); bottom right: mfERG output from AMD patient showing decreased peak height
AMD
The diagnosis of AMD was confirmed by both dilated retinal examination by a retinal specialist (AC) and dilated retinal fundus photography (Zeiss Visucam NM/FA, Zeiss Industries, Dublin). Macular centred fundus photos (45°) were graded according to the AREDS trial criteria [13]. All participants also underwent baseline spectral domain optical coherence tomography (SD-OCT) and fundus autofluorescence (FAF). Where necessary, additional investigations, including fundus fluorescein angiography and indocyanine green angiography, were undertaken to evaluate potential exclusion criteria such as nAMD.
Randomisation & treatment
Following enrolment, all participants were consecutively randomised by a pre-determined computerised random-number generator sequence to receive either 20 mg saffron (treatment; S) or placebo (P) for 3 months (90 days) administered as an unlabelled oral capsule consumed once daily in the morning with meals. Both types of capsule were identical in colour and size, and provided in numbered containers. This dosage of saffron was chosen based on results from previously published pilot studies of saffron in AMD [11]. After the initial 3-month period, all participants crossed-over into the other arm and received treatment with the other intervention (saffron or placebo as appropriate) for a further 3 months. Compliance with treatment was assessed by interview at monthly visits.
Participants, study personnel and statistical analysts were masked to treatment allocation throughout the study period. Capsules were prepared by an independent contractor (Vitex Pharmaceuticals, Eastern Creek, NSW, Australia) who de-identified the containers in which capsules were provided prior to delivery to study personnel. Saffron was sourced from a single supplier who produces saffron at a single Australian location in a standardised method to reduce variability in supply. A single, unrelated researcher not in direct participant contact had access to the treatment code. Analysis was conducted by an independent statistician with no direct participant contact who was provided coded, de-identified information by study personnel, and then independently provided the study code by the sole researcher with this code.
Participants were requested to maintain their usual diet throughout the trial, and to continue on any supplements (including AREDS-based therapies) they had been consuming prior to study commencement. For sub-group analysis purposes, supplements were further subdivided into AREDS-based therapies (containing zinc, copper, Vitamin C, Vitamin E, but no beta-carotene or lutein-zeaxanthin), and separately also into a lutein-zeaxanthin supplement group.
Study protocol
All participants underwent monthly assessment for a period of 6 months. At each visit, complete ophthalmic examination was undertaken, including: (a) intraocular pressure (IOP) monitoring via Goldmann applanation tonometry, (b) adverse event monitoring, (c) standardised BCVA assessment in ETDRS letters and (d) colour fundus photography.
Additionally, at the baseline, 3- and 6-month visits, participants also underwent flicker perimetry (FP), microperimetry (MP), SD-OCT, FAF, lens grading using AREDS lens assessment criteria [14] and multifocal electroretinogram (mfERG) assessment. Electroretinography and perimetric examinations were performed prior to any investigations that may have affected photoreceptor response, such as fundus examination, colour photography, OCT, FAF or fundus photography.
Autofluorescence and optical coherence tomography
SD-OCT was conducted using a 19-line, 1024 A-scans per line scan via a Heidelberg Spectalis system (Heidelberg Industries, Heidelberg, Germany), and inbuilt Heidelberg licenced software with eye tracking and image recognition (Tru-Track and AutoRescan respectively) was employed to ensure continuity of the scan location. All scans were reviewed, recentred and resegmented as necessary by two independent graders, with any disputes adjudicated by a third, independent grader. Central macular thickness (CMT) was measured via SD-OCT within the central 1-mm ETDRS circle, and was defined as the distance between the Internal Limiting Membrane and Bruch’s Membrane.
FAF was conducted using a Heidelberg Spectralis FAF acquisition module, and hypoautofluorescence area (a measure of retinal atrophy size) was measured in mm2 using FAF images by two independent graders, with any disputes > 15% in the area being adjudicated by a third, independent grader.
Flicker perimetry
FP was conducted using a Medmont M7000 perimeter (Medmont Industries, Melbourne, Australia) in accordance with previously published methodology [15]. Briefly, the M700 is a bowl perimeter that presents Goldmann size III light-emitting diode stimuli with a maximum single point luminescence of 320 cd·m−2 and a background illumination of 3.2 cd·m−2. The automated flicker mode utilises a ZEST-fast Bayesian threshold logic, and tests participants using an array of 48-points at 1°, 3°, 6° and 10° from central fixation, with a duration of 800 ms−1 for flickering stimuli.
All participants initially received verbal instructions regarding test protocol and underwent a 2-min practice session in which non-flickering errors were highlighted and flickering responses received positive reinforcement as per previously published methodology. Following this, the test was conducted without operator involvement, and test reliability was ensured by blind-spot monitoring as well as non-flickering false-positives and flickering false-negatives randomly displayed throughout testing. A participant was retested if the rate of fixation loss, false negatives or false positives was more than 20%. Average sensitivities for the 1°, 3°, 6° and 10° rings were calculated at each time point, and the change in these values during the saffron and placebo phases were compared.
Microperimetry
MP was assessed undertaken with a Macular Assessment Integrity Analyser (MAIA, Centervue, Padova, Italy). The MAIA utilises a scanning light ophthalmoscope to perform fundus tracking, using the whole fundus as a reference. Participants were tested using an automated macular assessment protocol. Fixation was ensured via the use of a red circle target of 1° diameter, and stimuli were presented in a 4-2 strategy across an array of 37 points at 0°, 1°, 3° and 5° from central fixation. Throughout the test, Goldmann III stimuli are displayed across a dynamic range of 36 dB, with a background luminescence of 1.27 cd·cm2.
All participants were dilated with 1% tropicamide/2.5% phenylephrine prior to testing, and all received a standardised set of instructions regarding test performance prior to test commencement. Tests were conducted in a standardised, non-illuminated room, prior to any tests that may have affected photoreceptor response (such as fundus photos). Participants with false positive responses of > 25% were retested, and if these responses persisted, they were excluded from analysis.
Results were grouped into concentric rings at 1°, 3° and 5° from central fixation (rings 1–3 respectively) and analysed as the average sensitivity of each of these rings, as well as the overall average macular sensitivity.
Multifocal electroretinograms
Multifocal electroretinograms are an objective test of retinal function that measures retinal conduction, and were acquired using a VERIS™ Science (Veris) device following International Society for Electroretinogaphy in Vision (ISCEV) guidelines [16], with refractive error assessed by either using the patient’s own near glasses or by performing a subjective refraction for near and using this refraction in a trial frame. All participants’ pupils were maximally dilated to at least 7-mm diameter using 0.5% tropicamide and/or 2.5% phenylephrine, with the cornea anaesthetised with 0.4% oxybupivicaine hydrochloride. The mfERG data was acquired using a gold foil electrode. Test stimuli consisted of 103 scaled hexagons presented in a pseudorandom fashion at a rate of 75 Hz, using a luminance of 200 cd/m2 for the white hexagons and 1.0 cd/m2 for black hexagons. Fixation was ensured using a red fixation device, and recordings that contained blinks or other artefacts were not saved and were re-recorded. Signals obtained were band pass filtered from 10 to 100 Hz and amplified 100,000 times. Noise-contaminated segments were rejected and repeated.
The mfERG responses for the hexagons across the retina were separated into six concentric rings (rings 1 to 6) for data analysis. The first-order kernel responses were recorded according to the ISCEV guidelines [16]. The latencies and average response densities of the six concentric rings were measured (Fig. 1), with greater response density and lower latency indicative of better retinal function. The rings of 1–6 correspond to the foveola at 1°, 4°, 8°, 12°, 17°, and 22° radius of the stimulus, respectively according to the eccentricity, with the fixation target at the central 0.75°. The response amplitudes in each ring were measured between the first negative trough (N1) and the first positive peak (P1), yielding the N1P1 response densities (amplitudes per unit retinal area in nV/deg2). The P1 peak latencies (ms) of the positive waveform were also measured.
An initial full-field ERG was also conducted under ISCEV conditions [17] to exclude the presence of potential confounding retinal degenerative diseases that may have mimicked AMD.
Statistical analysis
The primary outcome was mean change in BCVA. Secondary outcomes included mean change in mfERG N1P1 response density, and mean change in mfERG latency, change in individual ring mfERG N1P1 response density and latency, mean change in flicker perimetry ring response, mean change in microperimetry ring response, and safety of saffron as compared to placebo. Incidence of serious adverse events (SAEs) was recorded and analysed between the two groups to assess this final outcome.
Additional exploratory analyses were also conducted to explore the effect of saffron on those participants already consuming other supplementation therapy, and the effect of baseline atrophy on response observed. Participants on AREDS supplementation (current best-practice treatment) were analysed to assess the efficacy of saffron in this subgroup.
Of the 100 participants enrolled, 97 completed both placebo and saffron supplementation (Fig. 2). A single participant withdrew soon after study commencement due to family illness, one participant died of urinary sepsis during the saffron supplementation phase after completing the placebo phase, and another participant withdrew due to travel difficulties during the placebo supplementation phase after completing the saffron phase. All participants enrolled in the study were included in the safety analysis. Efficacy analysis was conducted on an intention to treat basis; however, participants who developed confounding visual pathologies (nAMD, significant cataract, etc.) during one arm of the trial had their visual results (mfERG, FP, MP and BCVA) excluded from analysis in these arms. There were thus 95 participants in the placebo arm and 96 participants in the saffron arm who were analysed to assess the efficacy of saffron.

Flow diagram of participants within the trial
Given the hierarchical nature of data (cross-over study in two eyes for some patients, and across six rings for mfERG results) a linear mixed effects model was used to account for within patient, eye and ring correlations using the lme function in R package nlme. To combine mfERG results over all rings, a linear mixed effects model was fitted on the mfERG logarithm with a quadratic term for reduction of log (mfERG) by ring. The choice for taking the logarithm of mfERG results, and for using a quadratic term for reduction by ring, was made to ensure assumptions on residual values were not violated. The fixed effects were treatment only for BCVA and treatment, ring and ring squared for log (mfERG) and for latency. Random effects were chosen to minimise Akaike information criterion (AIC) and Bayesian information criterion (BIC) values.
Analysis of mfERG latency was also conducted both including and excluding ring 1, as this ring had significantly more variability than rings 2–6. This variability was suggestive of potential noise in the signal, and analysis with and without this ring gave similar results. Both results are presented below and the conservative results of all rings included are presented in the abstract.
All analyses were conducted using the software R: A Language and Environment for Statistical Computing version 3.2.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics of the cohort are displayed in Table 1. Fifty-one participants were male (52.6%), the mean age of participants was 73.9 years and 71 (73.2%) were already consuming AREDS supplements in both groups.
Vision
Mean BCVA improved by 0.69 ETDRS letters whilst on saffron compared to placebo (p = 0.001). For those participants already on best-practice supplementation (AREDS equivalent) mean BCVA improved 0.73 letters on saffron compared to placebo after 3 months (p = 0.006). There was no difference in the change in BCVA between AREDS grades (i.e. no difference in response between AREDS grades 2 and 3, p > 0.05).
Electroretinography
There was a trend toward improved mean pooled mfERG response density (2.1% improvement) whilst on saffron compared to placebo (p = 0.08). Individual ring response density changes were greater in rings 1, 2, 3, 5 and 6 whilst on saffron, and responses in ring 4 were greater on placebo; however, none of the individual ring response density changes were significant (p > 0.10 for all, Table 2).
For those participants already on best-practice supplementation (AREDS equivalent) mean pooled mfERG response density improved 2.8% on saffron compared to placebo (p = 0.04).
Mean pooled latency was 0.17 ms lower on saffron as compared to placebo (p = 0.04). Individual ring latency was lower for rings 3 and 6 on saffron (p < 0.05 for rings 3 and 6, p > 0.1 for all other rings, Table 2).
For those participants on AREDS supplements, mean pooled latency reduced 0.15 ms on saffron compared to placebo; however, this was not statistically significant (p = 0.12).
Central ring latency (ring 1) was significantly more variable than latency for rings 2–6. Excluding ring 1, mean pooled latency was 0.25 ms lower on saffron compared to placebo (p < 0.001), and for those participants also on AREDS supplements, mean pooled latency decreased 0.16 ms on saffron compared to placebo (p = 0.05).
There was no difference in the change of the mfERG response density or latency to saffron depending on the grade of AMD (i.e. no difference in response between AREDS grades 2 and 3, p > 0.05 for all).
Perimetry
Microperimetry results were not different between saffron or placebo for any of rings 1–3 (p > 0.10 for all). Flicker perimetry results were also not different between saffron or placebo for any of rings 1–4 (p > 0.10 for all).
Impact of anatomical and demographic factors
After adjusting for baseline CMT and FAF area, mean mfERG response density improved 2.3% on saffron compared to placebo (p = 0.05), mean mfERG latency was reduced by 0.19 ms on saffron compared to placebo (p = 0.03), and mean BCVA improved 0.70 letters on saffron compared to placebo (p = 0.001).
No association was found between FAF area and latency (p > 0.05); however, increased FAF area was associated with decreased mean pooled mfERG response density (p = 0.008).
No interaction was found between age and the effect of treatment on BCVA (p = 0.09), response density (p = 0.86) or latency (p = 0.58).
Safety
A total of 19 SAEs occurred during the trial, with ten occurring during the saffron supplementation phase and nine during placebo supplementation (Table 3).
No significant difference was observed in the rate of SAE occurrence between the two treatment arms (p > 0.10, two-sample t test). Mean change in IOP was 1.02 mmHg in the saffron phase and 1.13 mmHg in the placebo phase (p > 0.10, paired t-test) for change in IOP between the two groups.
Discussion
Oral saffron supplementation modestly assists in preserving retinal function in participants with AMD, and this benefit appears to extend to participants already consuming current best-practice therapy (beta-carotene free AREDS supplementation). Although the recent AREDS2 trial is a notable exception [6], few other studies investigating supplementation therapies in AMD have maintained participants on concurrent supplement therapies [18, 19]. This limits the generalizability of the results obtained, as patients in clinical practice are often already consuming supplements for moderate AMD [20]. Restricting concurrent supplement use also limits understanding of both potential therapeutic mechanisms of action and AMD pathophysiology, as it can be unclear whether different therapies are working on separate pathways or whether they are all targeting a single pathophysiological mechanism.
The most interesting finding of this trial was that there was a small but additive response in those participants consuming other antioxidant supplements, including beta-carotene free AREDS supplements. Although the mechanism by which saffron affects retinal tissue is still under investigation, reduction of oxidative stress is the most heavily investigated pathway [21]. Multiple constituents of saffron have been shown to reduce retinal oxidative stress in animal studies [22, 23], suggesting that there may be specific saffron constituents that are responsible for the results observed in our study. Whilst these are initial studies, they suggest that these constituents may be promising targets for future trials, and their benefits may be additive with existing therapies, potentially resulting in further reductions in AMD progression and visual loss.
Although electroretinography is not routinely used in the everyday clinical assessment of AMD, mfERG has successfully been utilised in AMD trials, including other trials of dietary supplementation [24, 25]. The major advantage of mfERG is that it is an objective functional assessment, meaning that it is less influenced by patient perceptions or other confounding factors than other, subjective functional tests. This allows for a more reliable measure of visual outcomes and may be highly specific in predicting visual loss over time [26, 27]. Responses represent ON and OFF-bipolar cell contributions plus smaller contributions from inner retina and photoreceptors, and thus the mfERG indicates function of the photoreceptors indirectly [28]. Previous studies of the mfERG in mild/moderate AMD have shown that compared to age-matched normal subjects, AMD sufferers have decreased amplitude/response density and increased latency [27, 29]. Changes in amplitude are thought to relate to loss of photoreceptor function, whilst alterations in latency have been suggested to reflect cellular dysfunction [30, 31]. As saffron supplementation improved both parameters, saffron may have a role in reducing cellular loss as well as stabilising photoreceptor function, although the short time frame of the study limits interpretation.
Microperimetry, which is a subjective measurement of retinal sensitivity at mesopic adaptation levels, may be mediated by both rod and cone photoreceptors. It was not found to show any difference between the two groups, suggesting that microperimetry in this study was not as sensitive as previous reports have suggested when comparing the techniques to matched normals [32]. Interestingly, flicker perimetry has previously been suggested to be less sensitive than mfERG at detecting altered retinal function in early AMD, and our results support this earlier finding [15].
There was no evidence that regular saffron supplementation is associated with increased safety risks to patients. The rate of cataract progression across the study was similar to that seen in major studies of cataract [33], as was the rate of nAMD development [5] although the study period is relatively short. Toxicological studies of saffron have suggested that saffron is not associated with serious side-effects at dosages below 5 g/daily, and the 20 mg/daily dose used in this study is well within such a therapeutic window [10]. It should be emphasised, however, that this study was not specifically designed to assess the safety of saffron supplementation, and as such, was not powered to detect potentially rare adverse events. Further research is thus needed to fully define the risk profile of saffron as a therapeutic substance.
Some limitations do apply to this study. The visual gain detected was statistically but not clinically significant, and this may relate to the relatively short follow-up period of our study, particularly given the slow progressive nature of AMD. It may therefore be that with more prolonged supplementation, a greater neuroprotective response would be observed, and longer duration trials may thus provide greater insight into this. Additionally, efficacy has also thus far only been tested at a single dosage, and further research is needed to fully define the dose-response relationship of saffron in AMD sufferers. Further, as there is no reliable biomarker available for testing to assess response or compliance with dosing, it was not possible to biologically monitor compliance with therapy, meaning compliance could only be assessed subjectively. Additionally, the lack of reliable biomarkers and the complex natural components in saffron mean than accurate measurement of the pharmacokinetics of saffron could not be assessed. As a result of this, the association between pharmacokinetics and pharmacodynamics for oral saffron remains unknown.
Saffron supplementation was both efficacious and safe in preserving retinal function in participants with AMD, although clinically the degree of response obtained with this short-term study was small. These effects were complementary with current best practice therapies, suggesting that further protection than is currently obtained may be gained for patients by using these substances in tandem. Given the rising number of individuals with AMD, and its propensity to lead to later irreversible visual loss, further, longer-duration studies are justified to more fully investigate the role of saffron and saffron-based therapies as treatments for AMD.
References
Klein R, Lee KE, Gangnon RE, Klein BE (2013) Incidence of visual impairment over a 20-year period: the Beaver Dam Eye Study. Ophthalmology 120:1210–1219
Rosenfeld PJ, Brown DM, Heier JS et al (2006) Ranibizumab for neovascular age-related macular degeneration. N Engl J Med 355:1419–1431
Brown DM, Kaiser PK, Michels M et al (2006) Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med 355:1432–1444
Chew EY, Clemons TE, Agron E et al (2013) Long-term effects of vitamins C and E, beta-carotene, and zinc on age-related macular degeneration: AREDS report no. 35. Ophthalmology 120:1604–1611
Age-Related Eye Disease Study Research Group (2001) A randomized placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E, beta carotene, and zinc for age-related macular degeneration and vision loss: AREDS report no. 8. Arch Ophthalmol 119:1417–1436
Age-Related Eye Disease Study 2 Research Group (2013) Lutein + zeaxanthin and omega-3 fatty acids for age-related macular degeneration: the age-related eye disease study 2 (AREDS2) randomized clinical trial. JAMA 2309:2005–2015
Purushothuman S et al (2013) Saffron pre-treatment offers neuroprotection to nigral and retinal dopaminergic cells of MPTP-treated mice. J Parkinsons Dis 3:77–83
Akhondzadeh S, Shafiee Sabet M, Harirchian MH et al (2010) A 22-week, multicenter, randomized, double-blind controlled trial of Crocus sativus in the treatment of mild-to-moderate Alzheimer's disease. Psychopharmacology 207:637–643
Bathaie SZ, Mousavi SZ (2010) New applications and mechanisms of action of saffron and its important ingredients. Crit Rev Food Sci Nutr 50:761–786
Mohamadpour AH et al (2013) Safety evaluation of Crocin (a constituent of saffron) tablets in healthy volunteers. Iran J Basic Med Sci 16:39–46
Falsini B et al (2010) Influence of saffron supplementation on retinal flicker sensitivity in early age-related macular degeneration. Invest Ophthalmol Vis Sci 51:6118–6124
Piccardi M et al (2012) A longitudinal follow-up study of saffron supplementation in early age-related macular degeneration: sustained benefits to central retinal function. Evid Based Complement Alternat Med 2012:429124
Age-Related Eye Disease Study Research Group (2001) The age-related eye disease study system for classifying age-related macular degeneration from stereoscopic color fundus photographs: the age-related eye disease study report number 6. Am J Ophthalmol 132(5):668–681
Age-Related Eye Disease Study Research Group (2001) The age-related eye disease study (AREDS) system for classifying cataracts from photographs: AREDS report no. 4. Am J Ophthalmol 131:167–175
Phipps JA, Dang TM, Vingrys AJ, Guymer RH (2004) Flicker perimetry losses in age-related macular degeneration. Invest Ophthalmol Vis Sci 45:3355–3360
Hood DC, Bach M, Brigell M et al (2012) ISCEV standard for clinical multifocal electroretinography (mfERG) (2011 edition). Doc Ophthalmol 124:1–13
McCulloch DL et al (2015) ISCEV standard for full-field clinical electroretinography (2015 update). Doc Ophthalmol 130:1–12
Murray IJ et al (2013) Lutein supplementation over a one-year period in early AMD might have a mild beneficial effect on visual acuity: the CLEAR study. Invest Ophthalmol Vis Sci 54:1781–1788
Souied EH, Delcourt C, Querques G et al (2013) Oral docosahexaenoic acid in the prevention of exudative age-related macular degeneration: the nutritional AMD treatment 2 study. Ophthalmology 120:1619–1631
Schleicher M, Weikel K, Garber C, Taylor A (2013) Diminishing risk for age-related macular degeneration with nutrition: a current view. Nutrients 5:2405–2456
Bisti S, Maccarone R, Falsini B (2014) Saffron and retina: neuroprotection and pharmacokinetics. Vis Neurosci 31:355–361
Chen L, Qi Y, Yang X (2015) Neuroprotective effects of crocin against oxidative stress induced by ischemia/reperfusion injury in rat retina. Ophthalmic Res 54:157–168
Ishizuka F et al (2013) Crocetin, a carotenoid derivative, inhibits retinal ischemic damage in mice. Eur J Pharmacol 703:1–10
Ma L, Dou HL, Huang YM et al (2012) Improvement of retinal function in early age-related macular degeneration after lutein and zeaxanthin supplementation: a randomized, double-masked, placebo-controlled trial. Am J Ophthalmol 154:625–634
Berrow EJ, Bartlett HE, Eperjesi F, Gibson JM (2013) The effects of a lutein-based supplement on objective and subjective measures of retinal and visual function in eyes with age-related maculopathy -- a randomised controlled trial. Br J Nutr 109:2008–2014
Ambrosio L et al (2015) The value of multifocal electroretinography to predict progressive visual acuity loss in early AMD. Doc Ophthalmol 131:125–135
Yavas GF, Kusbeci T, Inan UU (2014) Multifocal electroretinography in subjects with age-related macular degeneration. Doc Ophthalmol 129:167–175
Hood DC, Frishman LJ, Saszik S, Viswanathan S (2002) Retinal origins of the primate multifocal ERG: implications for the human response. Invest Ophthalmol Vis Sci 43:1673–1685
Yang S et al (2016) Photoreceptor dysfunction in early and intermediate age-related macular degeneration assessed with mfERG and spectral domain OCT. Doc Ophthalmol 132:17–26
Li J, Tso MO, Lam TT (2001) Reduced amplitude and delayed latency in foveal response of multifocal electroretinogram in early age related macular degeneration. Br J Ophthalmol 85:287–290
Gerth C et al (2003) Assessment of multifocal electroretinogram abnormalities and their relation to morphologic characteristics in patients with large drusen. Arch Ophthalmol 121:1404–1414
Wu Z, Ayton LN, Guymer RH, Luu CD (2014) Comparison between multifocal electroretinography and microperimetry in age-related macular degeneration. Invest Ophthalmol Vis Sci 55:6431–6439
Age-Related Eye Disease Study Research Group (2001) A randomized, placebo-controlled, clinical trial of high-dose supplementation with vitamins C and E and beta carotene for age-related cataract and vision loss: AREDS report no 9. Arch Ophthalmol 119:1439–1452
Acknowledgments
No authors have any conflicts of interest to declare. One previous researcher associated with this study who had no participant contact, was previously required to withdraw his involvement from the study due to a conflict of interest. This individual is not an author on this manuscript. Preliminary data from this study was presented at the Royal Australian College of Ophthalmologists Annual Congress, Melbourne, Victoria, Australia, November 2016.
Funding
No funding was received for this research. No funding was associated with the design, conduct or data analysis of this trial. Dr. Chang has previously acted as a consultant for Novartis, Bayer and Alcon.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organisation or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licencing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Broadhead, G.K., Grigg, J.R., McCluskey, P. et al. Saffron therapy for the treatment of mild/moderate age-related macular degeneration: a randomised clinical trial. Graefes Arch Clin Exp Ophthalmol 257, 31–40 (2019). https://doi.org/10.1007/s00417-018-4163-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-018-4163-x