
Abstract
Background
To identify the etiology, pars plana vitrectomy results, culture results, and visual outcome of endophthalmitis in the pediatric age group.
Methods
Fifteen eyes of 15 consecutive pediatric patients who were treated and followed up for endophthalmitis between July 2011 and December 2012 were included in this study. Combined pars plana vitrectomy and intravitreal norvancomycin plus ceftazidime injection was performed on all 15 eyes. The vitreous samples were obtained by a standard pars plana vitrectomy. The specimens were sent to microbiology facility for gram staining, culturing, and sensitivity testing.
Results
The mean age of the patients was 5.3 ± 2.8 years (3–10 years). The mean follow-up time was 9.7 ± 1.5 months (7–12 months). Preoperatively, the visual acuities of the patients were as follows: light perception (n = 7), hand movements (n = 4), and counting fingers from 30 cm (n = 1), and these values were not available in three patients (n = 3). Postoperatively, the final best corrected visual acuity was 20/200 or better in six (40 %), counting of fingers in four (26.7 %), light perception to hand movements in two (13.3 %), and no light perception in one (6.7 %), with results being unavailable for two patients. Positive culture results were obtained from ten eyes (66.7 %). A single species was isolated in eight eyes, and multiple organisms were isolated in two eyes.
Conclusions
Penetrating ocular trauma was the most common cause of pediatric endophthalmitis in this consecutive series of endophthalmitis. Staphylococci and Streptococcus species were the most common isolated organisms. Patients with multiple organisms had poor visual recovery. Visual outcomes were poor in this series in spite of vitrectomy being performed immediately on all patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pediatric exogenous endophthalmitis is not uncommon, and may lead to devastating outcomes in a high percentage of cases in China. The condition can be a result of negligence of the guardian; however, some behavioral characteristics, such as attention deficit hyperactivity disorder (ADHD) symptoms in children may be associated with penetrating ocular injuries [1]. Unlike adults, children are usually delayed in seeing a doctor if they do not complain of pain or visual loss. Weinstein et al. [2] reported eight cases of culture-positive endophthalmitis in children in 1979. Seven of these cases occurred after trauma. Thordsen et al. [3] studied a consecutive series of pediatric endophthalmitis cases from a single institution over the last 10 years. They found that penetrating ocular trauma was the most common cause of pediatric endophthalmitis. Gram-positive species were the most common bacterial isolates. Moreover, endophthalmitis after trauma had a better prognosis than endophthalmitis resulting from other causes. To better understand more contemporary visual outcomes and the culture results of pediatric endophthalmitis after ocular trauma, we investigated a consecutive series of pediatric endophthalmitis cases after trauma from our institution over the last year.
Methods
Patients
The Eye & ENT Hospital of the Fudan University Review Board approved this retrospective review study. Pediatric endophthalmitis cases were identified by a computerized search for patients younger than 10 years of age who were treated for endophthalmitis at the Eye & ENT Hospital of Fudan University between July 2011 and December 2012. Medical records of each patient’s age, gender, initial visual acuity, treatment regimen, vitreous culture results, and visual acuity after surgery were obtained from inpatient charts. All of the patients underwent a standard pars plana vitrectomy.
Operation
All of the patients in the present study were treated with standard vitrectomy techniques and intravitreal antibiotics (vancomycin, ceftazidime, and/or amphotericin) as soon as the diagnosis was confirmed. Lensectomy was conducted simultaneously if there was a lesion on the lens. The mean follow-up time was 9.7 months (range: 7 to 12 months).
Culture methods
Ocular fluid specimens and wound cultures were obtained aseptically in the operating room. Vitreous samples were obtained by a standard pars plana vitrectomy. The specimens were sent to a microbiology facility for Gram staining, culturing, and sensitivity testing.
Statistical analysis
The statistical analyses consisted of the χ 2 test and Fisher’s exact test, where appropriate. Probability values <0.05 were considered statistically significant. All of the analyses were conducted with SPSS 17.0.
Results
Basic subject characteristics
As shown in Table 1, 15 pediatric endophthalmitis cases resulting from trauma were identified during the 18-month study period. Of these 15 cases, 13 cases (86.7 %) had penetrating corneal trauma, and two cases (13.3 %) had penetrating sclera trauma. The most common etiology of penetrating ocular trauma was scissors, which accounted for five of the 15 cases (33 %). Other etiologies included needles (three cases; 20 %), pencils (two cases; 13 %), rebars (two cases; 13 %), nails (one case; 7 %), plastic rods (one case; 7 %), and unknown etiology (one case; 7 %). The patients’ ages ranged from 3 to 10 years (mean 5.3 ± 2.8 years). A total of nine cases (60 %) were associated with hypopyon, ten cases (66.7 %) were associated with a lens lesion, and one case (7 %) was associated with retinal and choroidal detachment.
Culture results
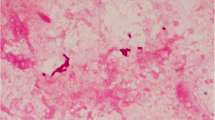
All of the cases were diagnosed and treated with standard vitrectomy within 24 h. In four cases (26.7 %), the formation of a ciliary body exudative membrane was found during the surgery. A vitreous biopsy was performed using the vitrectomy probe in all of the cases. The culture results are summarized in Table 1. Ten eyes (67 %) had positive vitreous cultures, a single bacterial species was isolated in eight eyes, and multiple organisms were isolated in two eyes.
Surgical results
Of all the patients in this consecutive series of pediatric endophthalmitis, 15 (100 %) achieved successful infection control. Preoperatively, the visual acuities of the patients were as follows: light perception (n = 7), hand movements (n = 4), and counting fingers from 30 cm (n = 1); values were not available in three patients (n = 3). All of the patients were treated with standard vitrectomy techniques and intravitreal antibiotics (norvancomycin, ceftazidime, and/or amphotericin) with a mean follow-up of 9.7 months (range 7–12 months). The final best-corrected visual acuities were 20/200 or better in six patients (40 %), counting fingers in four patients (26.7 %), light perception to hand movements in two patients (13.3 %), and no light perception in one patient (6.7 %). Results were not available in two patients. As shown in Table 2, visual outcome worse than counting fingers was attained in two children who had multiple organisms, compared with no children with a single bacterial species.
Discussion
In 1979, Weinstein et al. [2] reported a consecutive series of pediatric endophthalmitis from 1965 to 1976, and 86 % of the patients in that series had endophthalmitis secondary to ocular injuries. Thordsen et al. [3] also reported a consecutive series of 16 cases in 2008. They found that the most common cause of pediatric endophthalmitis was penetrating ocular trauma, which accounted for seven of 16 cases (44 %). Six cases (38 %) were associated with previous ocular surgery.
Here, we conducted a retrospective review of pediatric endophthalmitis, and found that all 15 cases occurred after a penetrating ocular trauma during an 18-month period. The most common etiologies of penetrating ocular trauma were scissors, needles, and pencils (67 %). An interesting study by Bayar et al. [1] also yielded the same results. They found that there was an association between penetrating eye injuries and inattentiveness, hyperactivity, oppositional defiant disorder, and conduct disorder in boys, as well as conduct disorder in girls.
The culture results in our series were also consistent with previous reports for the post-trauma cases. A total of ten of the 15 cases (67 %) were culture-positive, and all were gram-positive (seven Staphylococcus, one Streptococcus, one Staphylococcus and Streptococcus, and one Staphylococcus and fusarium). A single species was isolated in eight eyes, and multiple organisms were isolated in two eyes. In previous reports of post-traumatic endophthalmitis, culture-positive rates ranged from 44 to 75 %, and gram-positive organisms were predominant [2, 4, 5].
A poor prognosis was reported in previous reports [6–9], and 46.7 % (14/30) of the patients achieved final visual acuities of 20/200 or better. This result is similar to that found in the present study, in which 40 % (6/15) of patients achieved a final visual acuity of 20/200 or better. Essex et al. [9] reported that concomitant injuries may directly result in ocular damage that limits ultimate visual recovery. However, as shown in Table 2, patients with multiple ophthalmic injuries had a final visual acuity that was no worse than that in patients with a single ophthalmic injury (P > 0.05, Fisher’s exact test) in the present pediatric posttraumatic endophthalmitis series. Moreover, we found that patients with multiple organisms had a worse visual recovery than that in patients with a single species (P < 0.05, Fisher’s exact test). Polymicrobial infection and the virulence of the infecting microorganism indicated a poor prognosis [10].
The limitations of this study are as follows: (1) we evaluated the final visual acuity at a mean follow-up period of 9.7 months (range 7 to 12 months) after surgery; however, it is possible that some children may have achieved better vision after a longer time period, (2) because of the small sample size of pediatric endophthalmitis patients, some statistical analyses could not be performed, warranting more long-term follow-up studies in a larger number of patients, and (3) all patients were identified over a period of 18 months. It is possible to end up with etiology bias because of the short time of patients included.
In summary, penetrating ocular trauma was the most common cause of pediatric endophthalmitis in this consecutive series of endophthalmitis. Staphylococci and Streptococcus species were the most commonly isolated organisms. Patients with multiple organisms present had a poor visual recovery. Visual outcomes were poor in this series in spite of vitrectomy being immediately performed on all patients.
References
Bayar H, Coskun E, Öner V, Gokcen C, Aksoy U, Okumus S, Erbagci I (2015) Association between penetrating eye injuries and attention deficit hyperactivity disorder in children. Br J Ophthalmol 99:1109–1111
Weinstein GS, Mondino BJ, Weinberg RJ, Biglan AW (1979) Endophthalmitis in a pediatric population. Ann Ophthalmol 11:935–943
Thordsen JE, Harris L, Hubbard GB 3rd (2008) Pediatric endophthalmitis. A 10-year consecutive series. Retina 28:S3–S7
Alfaro DV, Roth DB, Laughlin RM, Goyal M, Liggett PE (1995) Paediatric post-traumatic endophthalmitis. Br J Ophthalmol 79:888–891
Alfaro DV, Roth D, Liggett PE (1994) Posttraumatic endophthalmitis. Causative organisms, treatment, and prevention. Retina 14:206–211
Peyman GA, Carroll CP, Raichand M (1980) Prevention and management of traumatic endophthalmitis. Ophthalmology 87:320–324
Puliafito CA, Baker AS, Haaf J, Foster CS (1982) Infectious endophthalmitis. Review of 36 cases. Ophthalmology 89:921–929
Brinton GS, Topping TM, Hyndiuk RA, Aaberg TM, Reeser FH, Abrams GW (1984) Posttraumatic endophthalmitis. Arch Ophthalmol 102:547–550
Essex RW, Yi Q, Charles PG, Allen PJ (2004) Post-traumatic endophthalmitis. Ophthalmology 111:2015–2022
Al-Rashaed SA, Abu El-Asrar AM (2006) Exogenous endophthalmitis in pediatric age group. Ocul Immunol Inflamm 14:285–292
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
National Natural Science Foundation provided financial support in the form of National Natural Science Foundation for Young Scholar of China (81300781) funding. The sponsor had no role in the design or conduct of this research.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Wu, H., Ding, X., Zhang, M. et al. Pediatric posttraumatic endophthalmitis. Graefes Arch Clin Exp Ophthalmol 254, 1919–1922 (2016). https://doi.org/10.1007/s00417-016-3330-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00417-016-3330-1