
Abstract
Objectives
The few voxel-wise lesion-symptom mapping (VLSM) studies aimed at identifying the anatomy of executive function are limited by the absence of a model and by small populations. Using Trail Making Test (TMT) and verbal fluency and a model of their architectures, our objective was to identify the key structures underlying two major executive processes, set-shifting and strategic word search.
Methods
We applied a validated VLSM analysis to harmonized cognitive and imaging data from 2009 ischemic stroke patients as a part of the Meta VCI Map consortium. All contrast analyses used an adjusted threshold with 2000 Freedman–Lane permutations (p ≤ 0.05).
Results
The TMT parts A and B were associated with structures involved in visual-spatial processing, the motor system, the frontal lobes, and their subcortical connections. Set-shifting depended on the left dorsomedial frontal region. Both semantic and phonemic fluency tests depended on verbal output abilities and processing speed with similar slopes in different languages. The strategic search process depended on Broca’s area, F2 and related tracts, temporal and deep regions. Lastly, the lesion map of set-shifting did not overlap with those of strategic word search processes.
Interpretation
Our results identify the anatomical substrates of two main executive processes, revealing that they represent only a specific subpart of previously reported structures. Finally, our results indicate that executive functions depend on several specific, anatomically separable executive processes mainly operating in various parts of the frontal lobes.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Action speed and executive functions make critical contributions to adaptive processes and human activities, and are often significantly impaired in brain diseases [1]. These higher order processes influence lower level automatic cognitive processes, enabling them to cope with non-routine situations [2] and to improve efficiency in routine situations [3]. In clinical practice, these functions are typically assessed using the well-known Trail Making Test (TMT) parts A and B (TMTA: joining numbers in ascending order; TMTB: joining numbers and letters alternately, i.e., set-shifting) and verbal fluency tests (giving as many names of a given category as possible in a set time) [3, 4]. These tests involve the executive process per se (i.e., set-shifting for TMTB and lexical–semantic strategic search for verbal fluency), but also ‘peripheral’ processes (visual-spatial–motor processes for TMT; lexical–semantic linguistic processes for verbal fluency) (supplement Table 1). Identifying the specific anatomy of executive processes, therefore, requires a model of their functional organization, specifying the links between executive and peripheral processes and their measures. Translating this model into lesion-symptom mapping (LSM) analysis makes it possible to adjust executive test performance for peripheral processes, and thus identify the specific anatomy of executive processes.
Recently, voxel-wise LSM (VLSM) studies have shown that performance in these tests depends on many brain regions. TMTB performance has been examined in six VLSM studies attributing performance to variable lesions in the frontoparietal region and deep left hemisphere [5,6,7,8,9], although these results are subject to debate [6, 10, 11]. The adjustment for peripheral sensorimotor processes has been performed in only three studies [5, 8, 9], which concluded that different left-hemisphere structures were involved: the rostral anterior cingulate gyrus [9], the insula [5], the external capsule and the corona radiata [8]. VLSM studies of verbal fluency tests have demonstrated the role of left-side lesions of the inferior frontal gyrus (F3), striatum, thalamus, insula, temporopolar region, and a large number of tracts [9, 12,13,14,15,16,17,18]. The two studies that controlled for language abilities reported contrasted results with extensive left-hemisphere damage [9] or a failure to identify a region specifically associated with the strategic word search process [12].
Overall these controversial results are probably due to the lack of adjustment for peripheral processes in many studies and the limited sample size of several studies resulting in variable coverage of key structures. Thus, the brain areas dedicated to task-specific control processes (i.e., set-shifting in the TMTB, and strategic searching in a verbal fluency task) have not been identified. Moreover, it remains unclear whether the brain areas dedicated to these specific control processes overlap, which would be expected if a single amodal control system underlies executive functions [2]. This second point is fundamental because it determines the functional architecture of executive functions.
By taking advantage of the very large multicenter dataset produced by the MetaVCI map consortium [19] with a harmonized cognitive assessment [4, 20], the objective of the present study was to identify the brain structures dedicated to two major executive processes, set-shifting and strategic word search, based on the structures subtending performance in the TMT and verbal fluency tests and to describe their interrelationships.
Methods
Population
We performed a large-scale lesion-symptom mapping study of pooled and harmonized individual patient data (brain imaging and cognitive assessments) from the Meta VCI Map consortium [19]. As reported previously [19], the Meta VCI Map multicenter dataset consists of individual data from cohorts of patients with ischemic stroke, with infarct segmentation data on acute MRI (diffusion-weighted imaging [DWI] or T2-weighted fluid-attenuated inversion recovery [FLAIR]) showing the symptomatic infarcts, and cognitive assessment data recorded within 15 months of the index stroke (including at least one measure of demographically adjusted TMT and verbal fluency, for the purposes of the present study). Five cohorts (Bundang VCI [21], Hallym VCI [21, 22], GRECogVASC-infarct subgroup [23], PROCRAS [24], and STROKDEM [25]) met these criteria for the present study (supplemental Fig. 1). Along with the data on TMT performance (completion time and, if available, the error rate) and semantic and phonemic fluencies, we analyzed data on confrontation naming, if available. We then excluded patients with missing data for age and educational level. All data were previously pooled, anonymized, and processed in a previous multicenter study [19] by the Utrecht coordinating center. The present analyses were performed at the study’s coordinating center (Picardie Jules Verne University; Amiens, France). The ethical and institutional approvals required by local regulations had been obtained for all Meta VCI Map cohorts.
Cognitive and imaging assessments
The cognitive assessment comprised the country-specific adaptation of the NINDS-Canadian Stroke Network harmonization standards battery [4]. The TMTB used numbers and letters (Roman or Korean letters depending on the country) [22,23,24, 24, 25]. The TMTA involves visuospatial search, visual identification, visuomotor processes, and sustained attention; in addition, the TMTB involves rapid switching between number and letter series. The semantic fluency test used the category “animals”, while the phonemic fluency test used items with a frequency matched to that in the harmonization standards battery [22, 24]. The Boston naming test was available in four cohorts (Bundang VCI and Hallym VCI [21, 22], GRECogVASC [23, 26], and PROCRAS [24]). Performance analysis was based on a validated method [27] that provides Z scores adjusted for age and education (i.e., adjusted for demographics). These analyses were carried out by the investigators of each cohort, using norms of each country.
Lesion-symptom mapping
Using previously validated methods [19, 28, 29], VLSM was performed on voxels lesioned in at least four patients. The data were analyzed using NiiStatV9 (https://www.nitrc.org/projects/niistat/), running with Matlab R2018b (https://in.mathworks.com/products/matlab.html) and SPM12 (http://www.fil.ion.ucl.ac.uk/spm/). Analyses were computed using the general linear model.
First, we analyzed demographically adjusted performance (Z scores) in all tests. The dependent variables were Z scores of completion times for parts A and B of the TMT, and semantic and phonemic fluencies. The naming score was analyzed as a guide to structures associated with verbal output and is described in the online supplement (Supplement Fig. 3 and Table 3). The threshold was adjusted using the false discovery rate and p < 0.001 was considered statistically significant. The potential effect of the time interval between MRI and cognitive assessment on VLSM results was addressed by two sets of analyses (Supplement results 2.2.) which yielded negative results, thus indicating that the time interval and its variation between subjects did not account for our findings.
Second, additional subtraction contrast analyses were used to identify structures associated with executive processes, set-shifting, and strategic word search (Supplement Table 2). Using NiiStat, all the contrast analyses used an adjusted threshold with 2000 Freedman–Lane permutations and p ≤ 0.05. Set-shifting (i.e., the process required to switch between digit and letter series in a time-constrained task) was analyzed by subtracting the TMTA completion time from the TMTB completion time in VLSM analysis. A sensitivity analysis was performed using an ANOVA with the test part (TMTA, TMTB) as the within-subject factor and the presence (present, absent) of a lesion in the TMTB–TMTA contrast map as the between-subject factor.
Regarding fluency performance, phonemic fluency minus semantic fluency contrast analysis was used to determine whether or not some structures were specifically associated with a given fluency test. The identification of brain structures associated with strategic word search was based on our previously validated model of the functional architecture of verbal fluency [12, 30]. This model posits that fluency production involves three main types of process operating in common: (1) linguistic processes, namely semantic and output lexico-phonological processes (common to externally triggered oral expression, such as those involved in the naming task), (2) a general attentional activation process that accelerates processing speed (which is purposely assessed using a simple non-verbal task, the TMTA), and (3) a strategic (i.e., cue-based, unusual) search process [12, 30]. The main advantage of this model is that the key structures underlying the strategic search process can be identified by a VLSM analysis of fluency production with a contrast analysis subtracting structures associated with naming and processing speed. The validity of this model in this multi-ethnic population was first verified (Supplement 2.1): it showed that fluency production depends on verbal output abilities and processing speed (Fig. 1), with strikingly similar slopes in different languages (Supplement Fig. 2). Then structures associated with strategic word search were examined using two subtraction contrast analyses ([phonemic fluency]–[TMTAt and naming], [semantic fluency]–[TMTAt and naming]). A sensitivity analysis was performed using two ANOVAs (semantic word search, phonemic word search) with the test as a within-subject factor (naming, TMTA and semantic fluency for semantic word searching; naming, TMTA and phonemic fluency for phonemic word searching) and the presence (present, absent) of a lesion in the semantic or phonemic contrast maps as the between-subject factor.

Associations (Z scores) between semantic fluency and naming (left) and between phonemic fluency (right) and naming, as a function of the speed (blue: normal; red: impaired) in the TMTA. Notice that fluency production is closely related to naming abilities and processing speed
Statistical analyses
All statistical analyses were performed using SAS® software (version 9.4, SAS Institute, Cary, NC). The threshold for statistical significance was set to p ≤ 0.05, unless otherwise indicated.
Results
Characteristics of the study population
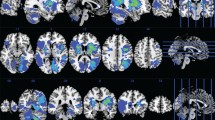
We included 2009 patients (Table 1) from the 5 cohorts (Bundang VCI: n = 758, GRECogVASC-infarct: n = 296, Hallym VCI: n = 643, PROCRAS: n = 175, STROKEDEM: n = 137) which are detailed in Supplement Table 2. The patients’ demographic and clinical characteristics (Table 1; Supplement Table 2) were typical of a hospital-based stroke population. Pre-stroke cognitive impairment (defined as an Informant Questionnaire on Cognitive Decline score > 3.38 [31]) was observed in 18.9% of the participants. Most of the imaging data were recorded in the first 2 weeks after the stroke. DWI was used most frequently for infarct segmentation. The cognitive assessment was usually performed 2 to 6 months after the stroke. The infarct distribution (Fig. 2) was similar in the two hemispheres, with a high level of brain lesion coverage: 1,556,726 of the 1,817,478 voxels (85.6%) in the Montreal Neurological Institute template were damaged in 4 or more patients. and were therefore included in the analyses. Only the distal part of the anterior cerebral artery territories, the posterobasal part of temporal lobes, the midbrain and the medulla oblongata could not be included in the analyses, due to damage observed in fewer than four patients. Furthermore, the lesion distribution was not significantly associated with age or educational level (p > 0.05 for both).

Lesion overlap in at least 4 of the 2009 patients (left-side structures are shown on the left of the figure)
VLSM analyses
The TMT
The demographically adjusted test completion time
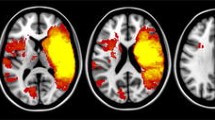
The completion times for the TMTA and TMTB were associated with a very large number of structures (Fig. 3a; Table 2; Supplement Table 3); the latter were characterized by slight overall right prominence (52.7% of the significant voxels) for the TMTA and left prominence for the TMTB (64.7% of the significant voxels). The TMTA and TMTB both involved regions underlying visual-spatial processing (the occipital, temporal and parietal lobes, the optic radiations and their connections, including the inferior longitudinal fasciculus (ILF) and the inferior occipitofrontal fasciculus (IOFF)), the motor system (precentral, corticospinal, and internal capsule), the frontal lobes (three frontal lateral gyri and, for the TMTB, the dorsomedial area) and their subcortical connections (the frontostriatal and thalamofrontal tracts).

A VLSM analysis of demographically adjusted scores (left-side structures are shown on the left of the figure). 3a (upper). The completion times in the TMTA (in blue) and TMTB (in red) (overlapping in purple). 3b (lower). Semantic fluency (in blue) and phonemic fluency (in red) (overlapping in purple). TMT Trail Making Test
Structures specific for set-shifting: the TMTB minus TMTA contrast analysis
The contrast analysis revealed small foci of 626 voxels specifically associated with the TMTB (Fig. 4; Table 2). The voxels were mainly located in the left dorsomedial frontal region, involving the subgenual and pregenual anterior cingulate gyrus (Brodmann area [BA] 24), the adjacent areas (BA 32 and the superior part of BA 11), the adjacent corpus callosum, and the frontostriatal tract.

Contrast analysis of the TMTB completion time minus the TMTA completion time: VLSM findings and sensitivity analysis of the lesion effect within this contrast map on TMT performance (Z score) showing the disproportionate effect of the lesion on TMTB (left-side structures are shown on the left of the figure). TMT Trail Making Test
The sensitivity analysis (Fig. 4.) showed (1) a significant effect of lesion within this contrast map (p = 0.003) due to an overall slowing in lesioned patients (lesion present: − 1.29 ± 0.16; lesion absent: − 0.81 ± 0.05), (2) a significant effect (p = 0.0001) of the test part, due to a slower time in the TMTB (− 1.39 ± 0.09) than in the TMTA (− 0.704 ± 0.87), and (3) most importantly, a significant lesion × test part interaction (p = 0.0001), related to the expected disproportionate slowing in the TMTB by lesioned patients.
Phonemic and semantic fluency tests
Demographically adjusted fluency production
Both fluency tests were associated with many structures in the left hemisphere (Fig. 2b; Table 3; Supplement Table 5), including the three frontal lateral gyri (F1, F2, and F3) and their frontostriatal, thalamofrontal, and aslant tracts; the temporal lateral gyri (T1, T2, and T3, especially the polar part); the parietal lobe (the inferior and superior lobuli, and the precuneus); central regions (including the rolandic operculum and the corticospinal tract); and the insula. The deep lesions mainly involved the striatum, thalamus, corpus callosum, and many tracts (including the arcuate, uncinate, ILF, and IOFF).
We checked the three tasks with a strong linguistic component (naming and both fluency tests) in the 1836 right-handed patients: these checks gave similar results (data not shown).
Structures specific for semantic and phonemic searching:
This analysis failed to find any structures differentially associated with fluencies.
Structures specific for strategic word search: fluency minus naming and TMTA contrast analysis
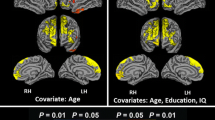
The subtraction contrast VLSM analyses (Fig. 5; Table 3) revealed clusters of voxels specifically associated with fluency tests; the voxels were mainly located in Broca area (Brodmann area [BA] 44 and 45), F2 (BA 46) and related tracts (the uncinate, aslant, frontostriatal and thalamofrontal tracts), temporal regions (mainly centered on T1, and especially BA 22), and deep regions (the striatum, pallidum, thalamus, arcuate, corpus callosum, corticospinal and internal capsule, ILF, and IOFF).

Semantic fluency (in blue) and phonemic fluency (in red) minus naming and TMTA contrast: VLSM findings and sensitivity analysis of the lesion effect within this contrast map showing the disproportionate effect of the lesion on fluency (left-side structures are shown on the left of the figure). TMT Trail Making test
The sensitivity analyses showed congruent results, with a disproportionate effect of the presence of a lesion within the contrast maps in each fluency test (Fig. 5). For the semantic word search, the significant effect of test (p = 0.0001) was due to worse performance for fluency (− 1.007 ± 0.03) than in the TMTA (− 0.878 ± 0.06) and naming (− 0.694 ± 0.04); the lesion effect (p = 0.0001), to worse overall performance (present: − 1.052 ± 0.06; absent: − 0.667 ± 0.03). Most importantly, the lesion x test interaction (p = 0.001) was due to the disproportionate decrease in fluency (relative to the two other tests) when a lesion was present in the semantic contrast maps. For the phonemic word search, the significant effect of test (p = 0.0001) was due to worse performance for fluency (− 0.760 ± 0.04) than for naming (− 0.478 ± 0.05; TMTA: − 0.752 ± 0.07). The lesion effect was not significant (lesion present: − 0.736 ± 0.07; absent: − 0.591 ± 0.04 p = 0.07). Most importantly, the lesion × test interaction (p = 0.0001) was due to the disproportionate decrease in fluency (relative to the two other tests; p < 0.05 for both) when a lesion was present in the phonemic contrast maps.
Lastly, the maps for set-shifting did not overlap with those for strategic word search processes (Figs. 4 and 5).
Discussion
This study of a very large, multi-ethnic meta-cohort with a harmonized battery was designed to reveal the anatomical substrates of two major executive processes, set-shifting and strategic word search, assessed using the two most commonly used executive tests and to investigate the functional architecture of control processes.
Our results extend previous findings [5,6,7,8,9, 32] and show that the TMT completion time is associated with a very large number of structures in both hemispheres. The TMT’s anatomical substrate included regions involved in visuospatial processing (the occipital, temporal, and parietal lobes, optic radiations, and their connections, such as the ILF and the IOFF) and required for visual scanning, reading, and visuomotor guidance [33]. The substrate also involved the motor structures (the precentral, corticospinal, and internal capsule) needed to quickly draw connecting lines. Lastly, the substrate included some of the frontal lateral regions (F1, F2, F3) and their subcortical connections (the frontostriatal and thalamofrontal tracts); these are all especially involved in the temporary maintenance of information [34, 35] and processing speed [33, 36, 37]. Our anatomical findings show that the attentional component needed to accelerate TMT completion [5,6,7,8,9, 32] cannot be identified from the completion time because it also reflects many sensorimotor components [3, 33, 38]. Interestingly, the regions associated with TMTA completion time included the right frontostriatal and orbital parts of F3, which have been previously associated with motor speed and sustained alertness, respectively [33]. The large size of the TMT anatomical substrate explains why it is highly vulnerable to brain lesions in general [3] and stroke in particular [20, 23, 39]. According to the subtraction contrast analysis, the anatomical substrate of set-shifting mainly depended on the left dorsomedial frontal region and especially the subgenual and pregenual anterior cingulate gyrus (BA 24) and adjacent areas (BA 32 and the superior part of BA 11). This result is at odds with the previously reported role of the insula, external capsule, center semiovale, and parietal lesions [5,6,7, 9,10,11]. Given the large population size in our study, this discrepancy cannot be attributed to insufficient power. Our finding is congruent with the known role of the pregenual anterior cingulate gyrus in the suppression of automatic actions and the control of voluntary action, which require the coordination of processes associated with sustained attention and motor timing [40, 41]. Thus, our result indicates that disproportionate slowing for TMTB (relative to TMTA) indicates a lesion in the left pregenual anterior cingulate gyrus or its callosal connections.
Our present results also document the processes recruited during fluency tests and their anatomical substrates. The close relationships (with very similar slopes) between verbal fluency production, verbal output abilities (indexed by confrontation naming), and processing speed (indexed by the TMTA) in different ethnic groups confirm our previous findings in stroke patients [12] and monolingual and bilingual controls [12, 30]. These findings support our model that performance of a verbal fluency task involves three types of processes operating in common: (1) linguistic processes, namely semantic and output lexico-phonological processes, (2) a general attentional activation process that accelerates processing speed, and (3) a strategic (i.e., cue-based, unusual) search process [12]. The present results enable us to interpret the contrast of fluency minus both naming and processing speed in terms of the anatomy of strategic word search process. The anatomical substrates for the fluency tests both involved the left frontal lateral lobe and their tracts (frontostriatal, thalamofrontal, and aslant tracts), the temporal lobe (T1, T2, and T3 especially at the polar part), the parietal lobe (both inferior and superior lobulus, precuneus), the insula, and central regions (including rolandic operculum and corticospinal tract). The lesions of deep structures mainly involved the striatum, thalamus, corpus callosum, and various tracts (including the arcuate, uncinate, ILF, and IOFF). Our findings extend the results of previous VLSM studies highlighting left-side lesions in F3, the temporal and temporopolar regions, striatum, thalamus, insula, and a large number of white matter tracts [12,13,14,15,16,17,18]. Furthermore, the large cohort studied here enables us to document the anatomical substrate of processes underlying the two fluency tests. The very similar anatomies for these two tests contrast with the previously reported prominent roles of F3 in phonemic fluency and temporal structures in semantic fluency [12, 14, 15, 18]. The prominent involvement of temporopolar structures in semantic fluency was expected, given their involvement in verbal semantic [12, 42]. Our present results showed that phonemic fluency is also associated with temporopolar structures. Further analyses of this topic between and within languages could be useful but are beyond the scope of this study. Our study is the first to describe the anatomical substrate of the strategic word search process, as our previous study of 358 patients failed to identify it. These findings strongly suggest that strategic lexical searching with both semantic and phonemic cues is performed by Broca’s area and T1 and requires connecting tracts (the uncinate, aslant, frontostriatal, and thalamofrontal tracts).
Furthermore, our results have major implications for the functional architecture of executive functions. They indicate that control processes are anatomically separable from lower level processes (i.e., visuomotor processes for TMT, and verbal output for fluency) and this supports the hypothesis of separable executive processes [43]. Our results also show that (1) the anatomical substrates of the two executive processes (set-shifting and strategic word search) did not overlap, and therefore (2) executive functions depend on several specific, anatomically separable executive processes rather than a single amodal control system. This interpretation is consistent with previous reports of selective impairments in executive processes, as assessed with similar binary decision tasks [44,45,46]. The only previous study to generate VLSM maps for various executive tests in a smaller population with predominantly frontal lesions showed a slight overlap between perseverative errors in TMTB and modified card sorting test but not for phonemic fluency [9]. These congruent results indicate that executive functions depend on many specific, anatomically separable executive processes operating primarily in various parts of the frontal lobes.
Our study has several limitations. First, the executive function assessment involved two tests only and did not encompass other well-known tests. However, these two tests are known to capture most of the executive impairment due to stroke [39] and so were, thus, the only ones of this type included in the harmonized stroke battery [4]. Interestingly, the two tests also capture the most executive impairment due to Alzheimer’s disease—another major cause of cognitive impairment [47,48,49]. Nevertheless, this limitation did not prevent us from finding non-overlapping anatomical substrates for executive processes, and therefore does not undermine the study’s main conclusions. Second, the analyses focused on lesion effect and not on other imaging factors that also contribute to cognitive deficit, albeit to a lower extent [29]. Third, the consortium pooled cohorts of patients with some differences in age and education, time interval of cognitive assessment and testing (due to language differences). However, this was controlled for by the use of age- and education-adjusted norms, by additional analyses excluding the role of time on VLSM results, and by additional analyses showing the striking similarities in the relationship between fluency and naming across countries. More importantly, these differences did not prevent important findings from being obtained. Fourth, cohort studies on post-stroke cognitive impairment tend to be selective. For example, patients who are most severely affected, such as severe aphasics or hemiplegic, are often underrepresented in more demanding research protocols. Fifth, cognitive trajectories after stroke differ between patients and may change over time. Therefore variation in timing of assessment might influence our results. Sixth, our pooled sample only includes Caucasian and Asian patients; thus, generalizability to other ethnicities remains undetermined.
Our study also has several strengths, including a very large population, the use of a normalized, harmonized assessment, and previously validated models of executive processes. This has enabled us to validate their functional architecture and identify the anatomical substrates of two main executive processes, revealing that they represent only a specific subpart of previously reported structures.
Data availability
Data sharing is not applicable to this article as no new data were created in this study.
References
Godefroy O, Azouvi P, Robert P et al (2010) Dysexecutive syndrome: diagnostic criteria and validation study. Ann Neurol 68:855–864. https://doi.org/10.1002/ana.22117
Shallice T, Burgess P (1991) Higher-order cognitive impairments and frontal lobe lesions in man. Frontal lobe function and dysfunction. Oxford University Press, New York, NY, US, pp 125–138
Godefroy O, Martinaud O, Narme P et al (2018) Dysexecutive disorders and their diagnosis: a position paper. Cortex J Devoted Study Nerv Syst Behav 109:322–335. https://doi.org/10.1016/j.cortex.2018.09.026
Hachinski V, Iadecola C, Petersen RC et al (2006) National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 37:2220–2241. https://doi.org/10.1161/01.STR.0000237236.88823.47
Varjačić A, Mantini D, Levenstein J et al (2018) The role of left insula in executive set-switching: lesion evidence from an acute stroke cohort. Cortex J Devoted Study Nerv Syst Behav 107:92–101. https://doi.org/10.1016/j.cortex.2017.11.009
Kopp B, Rösser N, Tabeling S et al (2015) Errors on the trail making test are associated with right hemispheric frontal lobe damage in stroke patients. Behav Neurol. https://doi.org/10.1155/2015/309235
Miskin N, Thesen T, Barr WB et al (2016) Prefrontal lobe structural integrity and trail making test, part B: converging findings from surface-based cortical thickness and voxel-based lesion symptom analyses. Brain Imaging Behav 10:675–685. https://doi.org/10.1007/s11682-015-9455-8
Anziano M, Mouthon M, Thoeny H et al (2023) Mental flexibility depends on a largely distributed white matter network: causal evidence from connectome-based lesion-symptom mapping. Cortex J Devoted Study Nerv Syst Behav 165:38–56. https://doi.org/10.1016/j.cortex.2023.04.007
Gläscher J, Adolphs R, Damasio H et al (2012) Lesion mapping of cognitive control and value-based decision making in the prefrontal cortex. Proc Natl Acad Sci USA 109:14681–14686. https://doi.org/10.1073/pnas.1206608109
Chan E, MacPherson SE, Robinson G et al (2015) Limitations of the trail making test part-B in assessing frontal executive dysfunction. J Int Neuropsychol Soc JINS 21:169–174. https://doi.org/10.1017/S135561771500003X
Nishimura A, Sutoko S, Kiguchi M et al (2022) Projection of damaged visual and language regions on low trail making test part-B performance in stroke patients. Front Neurol. https://doi.org/10.3389/fneur.2022.853942
Godefroy O, Aarabi A, Dorchies F et al (2023) Functional architecture of executive processes: evidence from verbal fluency and lesion mapping in stroke patients. Cortex 164:129–143. https://doi.org/10.1016/j.cortex.2023.03.013
Baldo JV, Schwartz S, Wilkins D, Dronkers NF (2006) Role of frontal versus temporal cortex in verbal fluency as revealed by voxel-based lesion symptom mapping. J Int Neuropsychol Soc JINS 12:896–900. https://doi.org/10.1017/S1355617706061078
Biesbroek JM, Lim J-S, Weaver NA et al (2021) Anatomy of phonemic and semantic fluency: a lesion and disconnectome study in 1231 stroke patients. Cortex 143:148–163. https://doi.org/10.1016/j.cortex.2021.06.019
Schmidt CSM, Nitschke K, Bormann T et al (2019) Dissociating frontal and temporal correlates of phonological and semantic fluency in a large sample of left hemisphere stroke patients. NeuroImage Clin. https://doi.org/10.1016/j.nicl.2019.101840
Thye M, Szaflarski JP, Mirman D (2021) Shared lesion correlates of semantic and letter fluency in post-stroke aphasia. J Neuropsychol 15:143–150. https://doi.org/10.1111/jnp.12211
Cipolotti L, Xu T, Harry B et al (2021) Multi-model mapping of phonemic fluency. Brain Commun 3:fcab232. https://doi.org/10.1093/braincomms/fcab232
Chouiter L, Holmberg J, Manuel AL et al (2016) Partly segregated cortico-subcortical pathways support phonologic and semantic verbal fluency: a lesion study. Neuroscience 329:275–283. https://doi.org/10.1016/j.neuroscience.2016.05.029
Weaver NA, Kuijf HJ, Aben HP et al (2021) Strategic infarct locations for post-stroke cognitive impairment: a pooled analysis of individual patient data from 12 acute ischaemic stroke cohorts. Lancet Neurol 20:448–459. https://doi.org/10.1016/S1474-4422(21)00060-0
Lo JW, Crawford JD, Desmond DW et al (2019) Profile of and risk factors for poststroke cognitive impairment in diverse ethnoregional groups. Neurology 93:e2257–e2271. https://doi.org/10.1212/WNL.0000000000008612
Lim J-S, Kim N, Jang MU et al (2014) Cortical hubs and subcortical cholinergic pathways as neural substrates of poststroke dementia. Stroke 45:1069–1076. https://doi.org/10.1161/STROKEAHA.113.004156
Yu K-H, Cho S-J, Oh MS et al (2013) Cognitive impairment evaluated with vascular cognitive impairment harmonization standards in a multicenter prospective stroke cohort in Korea. Stroke 44:786–788. https://doi.org/10.1161/STROKEAHA.112.668343
Barbay M, Taillia H, Nédélec-Ciceri C et al (2018) Prevalence of poststroke neurocognitive disorders using national institute of neurological disorders and Stroke-Canadian stroke network, VASCOG criteria (vascular behavioral and cognitive disorders), and optimized criteria of cognitive deficit. Stroke 49:1141–1147. https://doi.org/10.1161/STROKEAHA.117.018889
Aben HP, Reijmer YD, Visser-Meily JM et al (2018) A role for new brain magnetic resonance imaging modalities in daily clinical practice: protocol of the prediction of cognitive recovery after stroke (PROCRAS) study. JMIR Res Protoc. https://doi.org/10.2196/resprot.9431
Bournonville C, Hénon H, Dondaine T et al (2018) Identification of a specific functional network altered in poststroke cognitive impairment. Neurology 90:e1879–e1888. https://doi.org/10.1212/WNL.0000000000005553
Godefroy O, Leclercq C, Roussel M et al (2012) French adaptation of the vascular cognitive impairment harmonization standards: the GRECOG-VASC study. Int J Stroke Off J Int Stroke Soc 7:362–363. https://doi.org/10.1111/j.1747-4949.2012.00794.x
Godefroy O, Gibbons L, Diouf M et al (2014) Validation of an integrated method for determining cognitive ability: Implications for routine assessments and clinical trials. Cortex J Devoted Study Nerv Syst Behav 54:51–62. https://doi.org/10.1016/j.cortex.2014.01.016
Arnoux A, Toba MN, Duering M et al (2018) Is VLSM a valid tool for determining the functional anatomy of the brain? Usefulness of additional Bayesian network analysis. Neuropsychologia 121:69–78. https://doi.org/10.1016/j.neuropsychologia.2018.10.003
Puy L, Barbay M, Roussel M et al (2018) Neuroimaging determinants of poststroke cognitive performance: the GRECogVASC study. Stroke 49:2666–2673. https://doi.org/10.1161/STROKEAHA.118.021981
Kassir R, Roussel M, Abboud H (2023) Godefroy O (2023) Verbal fluency in bilingual Lebanese adults: is the prominent language advantage due to executive processes, language processes, or both? Appl Neuropsychol Adult. https://doi.org/10.1080/23279095.2023.2234536
Jorm AF (1994) A short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): development and cross-validation. Psychol Med 24:145–153. https://doi.org/10.1017/s003329170002691x
Turken A, Whitfield-Gabrieli S, Bammer R et al (2008) Cognitive processing speed and the structure of white matter pathways: convergent evidence from normal variation and lesion studies. Neuroimage 42:1032–1044. https://doi.org/10.1016/j.neuroimage.2008.03.057
Ouin E, Roussel M, Aarabi A et al (2022) Poststroke action slowing: Motor and attentional impairments and their imaging determinants. Evidence from lesion-symptom mapping, disconnection and fMRI activation studies. Neuropsychologia. https://doi.org/10.1016/j.neuropsychologia.2022.108401
Roussel M, Dujardin K, Hénon H, Godefroy O (2012) Is the frontal dysexecutive syndrome due to a working memory deficit? Evidence from patients with stroke. Brain J Neurol 135:2192–2201. https://doi.org/10.1093/brain/aws132
Collette F, Van der Linden M (2002) Brain imaging of the central executive component of working memory. Neurosci Biobehav Rev 26:105–125. https://doi.org/10.1016/s0149-7634(01)00063-x
Duering M, Zieren N, Hervé D et al (2011) Strategic role of frontal white matter tracts in vascular cognitive impairment: a voxel-based lesion-symptom mapping study in CADASIL. Brain 134:2366–2375. https://doi.org/10.1093/brain/awr169
Périn B, Godefroy O, Fall S, de Marco G (2010) Alertness in young healthy subjects: an fMRI study of brain region interactivity enhanced by a warning signal. Brain Cogn 72:271–281. https://doi.org/10.1016/j.bandc.2009.09.010
Godefroy O, Roussel M, Despretz P et al (2010) Age-related slowing: perceptuomotor, decision, or attention decline? Exp Aging Res 36:169–189. https://doi.org/10.1080/03610731003613615
Roussel M, Martinaud O, Hénon H et al (2016) The behavioral and cognitive executive disorders of stroke: the GREFEX study. PLoS ONE. https://doi.org/10.1371/journal.pone.0147602
Kerns JG, Cohen JD, MacDonald AW et al (2004) Anterior cingulate conflict monitoring and adjustments in control. Science 303:1023–1026. https://doi.org/10.1126/science.1089910
Donoso M, Collins AGE, Koechlin E (2014) Human cognition. Foundations of human reasoning in the prefrontal cortex. Science 344:1481–1486. https://doi.org/10.1126/science.1252254
Mummery CJ, Patterson K, Price CJ et al (2000) A voxel-based morphometry study of semantic dementia: relationship between temporal lobe atrophy and semantic memory. Ann Neurol 47:36–45
Posner MI, Petersen SE (1990) The attention system of the human brain. Annu Rev Neurosci 13:25–42. https://doi.org/10.1146/annurev.ne.13.030190.000325
Godefroy O, Lhullier C, Rousseaux M (1996) Non-spatial attention disorders in patients with frontal or posterior brain damage. Brain J Neurol 119(Pt 1):191–202. https://doi.org/10.1093/brain/119.1.191
Godefroy O, Rousseaux M (1996) Binary choice in patients with prefrontal or posterior brain damage. A relative judgement theory analysis. Neuropsychologia 34:1029–1038. https://doi.org/10.1016/0028-3932(96)00012-7
Godefroy O, Cabaret M, Petit-Chenal V et al (1999) Control functions of the frontal lobes. Modularity of the central-supervisory system? Cortex J Devoted Study Nerv Syst Behav 35:1–20. https://doi.org/10.1016/s0010-9452(08)70782-2
Godefroy O, Martinaud O, Verny M et al (2014) The dysexecutive syndrome of Alzheimer’s disease: the GREFEX study. J Alzheimers Dis JAD 42:1203–1208. https://doi.org/10.3233/JAD-140585
Godefroy O, Bakchine S, Verny M et al (2016) Characteristics of Alzheimer’s disease patients with severe executive disorders. J Alzheimers Dis JAD 51:815–825. https://doi.org/10.3233/JAD-150971
Andriuta D, Roussel M, Barbay M et al (2018) Differentiating between Alzheimer’s disease and vascular cognitive impairment: is the “memory versus executive function” contrast still relevant? J Alzheimers Dis JAD 63:625–633. https://doi.org/10.3233/JAD-171097
Acknowledgements
We thank Hugo J. Kuijf and Lei Zhao for their contribution to imaging data harmonization of the Meta VCI Map project data. We thank Olivia K.L. Hamilton, Irene M.C. Huenges Wajer, Bonnie Y.K. Lam, Adrian Wong, and Xu Xin as members of the Meta VCI Map neuropsychology working group for their advice on neuropsychological data harmonization. We thank Hassan Berrissoul and Astrid Causel for assistance with organizational aspects and Quentin Legendre for help with MRI data management in the GRECogVASC study.
Funding
The curation and harmonization of individual participant data in Meta VCI Map consortium was supported by Vici Grant 918.16.616 from ZonMW to GJB. The GRECogVASC study has been funded by Amiens University Hospital and by a grant from the French Ministry of Health (DGOS R1/2013/144). Funding for the PROCRAS study was obtained through ZonMw as part of the ‘TopZorg’ project in 2015 (grant # 842003011).
Author information
Authors and Affiliations
Consortia
Contributions
OG, MR, FD, RK, and AA were responsible for study concept and design. OG and AA were responsible for VLSM analyses. OG, MR, FD, RK, and AA drafted the manuscript. All authors revised the manuscript critically for important intellectual content. All authors gave final approval for submission. Cohort-specific contributions: KJL, BJK, and HJB were responsible for the Bundang VCI cohort. HJB: data collection and data interpretation. BJK and KJL: data collection. JSL, ML, and KHY were responsible for the Hallym VCI cohort. JSL: data collection and data interpretation. ML and KHY: data collection. OG, MR. and AA were responsible for the GRECogVASC cohort, study design and data collection. HPA and PLMK were responsible for the PROCRAS cohort study design and data collection. RB, TD, RL were responsible for the STROKDEM cohort study design, data collection and analysis. NAW, JMB, GJB were responsible for the curation and harmonization of individual participant data in Meta VCI Map consortium (www.metavcimap.org).
Corresponding author
Ethics declarations
Conflicts of interest
Godefroy, NA Weaver, M Roussel, F Dorchies, R Kassir, JM Biesbroek, KJ Lee, HJ Bae, BJ Kim, HJBae, JS Lim, M Lee, KH Yu, H P Aben, P LM de Kort, R Bordet, R Lopes, T Dondaine, GJ Biessels, and A Aarabi: none related to this study.
Ethical standard
The ethical and institutional approvals required by local regulations had been obtained for all Meta VCI Map cohorts.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Appendix
Appendix
GRECogVASC study group:
Olivier Godefroy, MD, PhD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Martine Roussel, PhD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Mélanie Barbay, MD, PhD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Sandrine Canaple, MD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Chantal Lamy, MD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Claire Leclercq, MD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Audrey Courselle-Arnoux, MD (Department of Neurology and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Sandrine Despretz-Wannepain (Department of Neurology, University Hospital of Amiens, France);
Pascal Despretz (University of Lille, INSERM CIC-IT 807, France); Hassan Berrissoul (University Hospital of Amiens, France);
Carl Picard (Department of Biostatistics and medical research, University Hospital of Amiens, France);
Momar Diouf (Department of Biostatistics and medical research, University Hospital of Amiens, France);
Gwénolé Loas, MD, PhD (Department of Psychiatry and Laboratory of Functional Neurosciences, University Hospital of Amiens, France);
Hervé Deramond, MD (Department of Radiology, University Hospital of Amiens, France);
Hervé Taillia, MD (Department of Neurology, Val de Grace Hospital, Paris, France);
Anne-Emmanuelle Ardisson (Department of Neurology, Val de Grace Hospital, Paris, France);
Claudine Nédélec-Ciceri, MD (Department of Neurology, Hospital of La Rochelle, France);
Camille Bonnin, PhD (Department of Neurology, Hospital of La Rochelle, France);
Catherine Thomas-Anterion, MD, PhD (Department of Neurology, University Hospital of St Etienne, France);
Francoise Vincent-Grangette (Department of Neurology and CMRR, University Hospital of St Etienne, France);
Jérome Varvat, MD (Department of Neurology, University Hospital of St Etienne, France);
Véronique Quaglino, PhD (Department of Psychology and Laboratory CRPPCO, University of Amiens, France);
Hélène Beaunieux (Department of Psychology, University of Caen, France);
Christine Moroni (Department of Psychology, University of Lille, France);
Audrey Martens-Chazelles (Department of Neurology, Hospital of Creil, France);
Stéphanie Batier-Monperrus (Department of Neurology, Hospital of Epinal, France);
Cécile Monteleone & Véronique Costantino (Department of Neurology, Hospital of Ajaccio, France;
Eric Theunssens (Institut de logopédie, Haute Ecole de Liège, Belgium).
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Godefroy, O., Weaver, N.A., Roussel, M. et al. Architecture and anatomy of executive processes: evidence from verbal fluency and Trail Making Test in 2009 stroke patients. J Neurol 271, 6147–6159 (2024). https://doi.org/10.1007/s00415-024-12541-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-024-12541-8