
Abstract
The syndrome of pathological laughing and crying (PLC) is characterized by episodes of involuntary outbursts of emotional expression. Although this phenomenon has been referred to for over a century, a clear-cut clinical definition is still lacking, and underlying pathophysiological mechanisms are not well understood. In particular, it remains ill-defined which kind of stimuli—contextually appropriate or inappropriate—elicit episodes of PLC, and if the phenomenon is a result of a lack of inhibition from the frontal cortex (“top-down-theory”) or due to an altered processing of sensory inputs at the brainstem level (“bottom-up-theory”). To address these questions, we studied ten amyotrophic lateral sclerosis (ALS) patients with PLC and ten controls matched for age, sex and education. Subjects were simultaneously exposed to either emotionally congruent or incongruent visual and auditory stimuli and were asked to rate pictures according to their emotional quality. Changes in physiological parameters (heart rate, galvanic skin response, activity of facial muscles) were recorded, and a standardized self-assessment lability score (CNS-LS) was determined. Patients were influenced in their rating behaviour in a negative direction by mood-incongruent music. Compared to controls, they were influenced by negative stimuli, i.e. they rated neutral pictures more negatively when listening to sad music. Patients rated significantly higher on the CNS-LS. In patients, changes of electromyographic activity of mimic muscles during different emotion-eliciting conditions were explained by frontal cortex dysfunction. We conclude that PLC is associated with altered emotional suggestibility and that it is preferentially elicited by mood-incongruent stimuli. In addition, physiological reactions as well as behavioural changes suggest that this phenomenon is primarily an expression of reduced inhibitory activity of the frontal cortex, since frontal dysfunction could explain changes in physiological parameters in the patient group. We consider these findings being important for the clinical interpretation of emotional reactions of ALS patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pathological laughing and crying (PLC) or pseudobulbar affect (PBA) describes episodes of involuntary, often irresistible attacks of laughing and/or crying and is part of a large variety of neurological conditions, but most common in patients with amyotrophic lateral sclerosis (ALS) [5, 7, 9, 26]: some estimate that up to 50 % of this patient group, in particular those with bulbar deficits, are affected by this condition [15]. Although the first description of this phenomenon by Oppenheim and Siemerling dates back to the end of the nineteenth century [20], a clear-cut clinical definition is still lacking. PLC is commonly described as being preferentially provoked by inappropriate or incongruent stimuli [19, 22], while others claim that even unspecific stimuli, i.e. stimuli without any specific emotional quality for healthy subjects, account for PLC in patients [23]. Hartje [8] asserts that PLC represents a pattern of motor dysinhibition phenomena being provoked by unspecific stimuli or emerging spontaneously without being associated with any emotional changes.
As diverse as the definitions are the proposed theories about possible underlying pathomechanisms. Two main hypotheses are being discussed: The first one, also called “top-down” theory, has been proposed by Wilson [29] who hypothesized that phenomena of exaggerated or involuntary emotional expression were caused by lesions of the motor cortex. These lesions are supposed to result in a loss of voluntary control of functional brain stem regions controlling emotional expression. For almost a century, this theory was regarded as the best to explain the phenomena caused by PLC and PBA. The second, more recent theory claims that the brainstem response itself is impaired in patients with PLC, which in turn generates a pathological and exaggerated reaction to certain sensory stimuli [21]. This theory was proposed based on observations of different lesions such as stroke [5, 23], abscess [22], or tumours [24] in the pons, cerebellum, and brainstem. Additionally, one recent single photon emission computed tomography study showed decreased serotonin transporter density in the midbrain/pons of stroke patients with PLC [18]. Of note, this study only focussed on pons, midbrain, thalamus and hypothalamus, thus no conclusions can be drawn regarding possible alterations in other brain regions.
Surprisingly, although PLC is a common feature in ALS, only few studies exist targeting the phenomenon in this specific patient group in a systematic approach. One recent diffusion tensor imaging (DTI) study in ALS patients exhibiting PLC showed disruption of fiber tracts descending from the fronto-temporal cortex towards the pons [6]. In a neuropsychological study, McCullagh et al. [14] found that ALS patients with PLC show significant impairment in performing tasks related to frontal cortex function. In a more recent study, Olney et al. [19] report on ALS patients with PLC showing difficulties regulating their facial expression and their emotion voluntarily, which was interpreted as a result of impaired frontal cortex inhibitory activity.
In this psychophysiological study, we address the pathogenesis of PLC by exposing ALS patients to simultaneously presented visual and auditory stimuli, which were either emotionally congruent or incongruent. We designed this setting to systematically address the following questions:
-
(a)
Is PLC in ALS an exaggerated response to comparatively weak emotional stimuli or an inappropriate response to emotionally incongruent stimuli?
-
(b)
Is the phenomenon associated with a pathological modulation of emotional stimuli in a “bottom-up”-loop or is it due to reduced inhibition of emotional behaviour display due to frontal cortex dysfunction (“top-down”-loop)?
Materials and methods
Subjects
Ten patients with ALS and PLC/PBA (six males, mean age 64.0 ± 12.2 years, mean education years 14.0 ± 2.7) and ten healthy sex-, age- and education-matched controls (six males, mean age 65.8 ± 10.8 years, mean education years 13.2 ± 3.6; p = 0.73 for mean age; p = 0.84 for education years) were studied. Patients were recruited from the Department of Neurology of the University Hospital of Ulm, Germany. The patients had been diagnosed with ALS according to the revised El Escorial Criteria [4]. Initial symptoms (bulbar or spinal), site of onset (upper or lower extremity, proximal or distal, bulbar, trunk), ALS functional rating scale (ALS-FRS), and the age of the patient at disease onset were recorded as reported by the patients and their relatives and patients were clinically examined. The patients and controls included in this study had no history of other neurological or psychiatric disorders. All patients and controls had given written informed consent. All experiments were conducted according to the principles expressed in the Declaration of Helsinki. The study was approved by the Ethics Committee of the University Hospital of Ulm (No. 157/13).
Mean age at disease onset was 63.6 ± 10.5 years, mean ALS-FRS at the time of the study was 30.7 ± 10.2. Seven out of ten PLC patients showed a bulbar disease onset. Two patients (both with a bulbar onset) had died at the end of this study, with a total disease duration from symptom onset to death of 21 and 19 months, respectively. Table 1 gives an overview over the clinical data and psychological measures of the ALS patients and controls.
Neuropsychological testing
All patients and controls completed the Center of Neurologic Study Lability Scale for quantification of PLC (CNS-LS) [28] to quantify the occurrence of emotional lability. A score of 13 points was set as the cut-off for emotional lability, as suggested by Smith et al. [28]. To differentiate between pathological laughing and pathological crying, we split the CNS-LS into questions scanning for sadness (questions 1,3,6; maximum score 15; CNS-LS-neg-raw) and for laughing (questions 2,4,5,6; maximum score 20; CNS-LS-pos-raw) and determined the individual CNS-LS-pos and CNS-LS-neg percentage score (CNS-LS-pos/neg-raw divided by maximum score in this subscale times 100).
Screening for cognitive deficits mirroring frontal cortex function was performed by a board certified psychologist using the German version of the Edinburgh Cognitive and Behavioural ALS Screen (ECAS) [1, 12] in seven patients and all controls and with the Consortium to Establish a Registry for Alzheimer’ s Disease plus Scale (CERAD plus [17]) in three patients.
Experimental design
Subjects were seated in a darkened room 30 cm in front of a computer screen. They were shown pictures with three different emotional qualities (happy, sad, neutral). The pictures were chosen from the International Affective Picture System (IAPS), a standardized collection of emotional pictures [11]. The pictures depicted either human faces or objects and were balanced with respect to arousal while they varied on the valence scale. They appeared in a semi-randomized order, in which a neutral (N) picture was always separating a happy (H) from a sad (S) picture.
Each picture was presented for six seconds. In total, we presented a set of 40 pictures (10 happy, 10 sad, 20 neutral).
Mood induction and picture rating
Subjects were asked to rate the pictures according to their emotional quality for valence on a non-numeric scale while watching. The scale differentiated between the emotional qualities “unpleasant”/“inducing sadness” and “neutral-pleasant”/“inducing happiness”. For rating, subjects used a slide bar with a cursor on the rating scale. All subjects were capable of operating the bar.
While watching the pictures, subjects were listening to classical instrumental music sequences presented via headphones. As were the pictures, also the auditory stimuli were chosen from a standardized set of objectively validated happy and sad musical extracts with a duration of 30 s, respectively [16]. The musical pieces had been shown to robustly induce different mood states in normal subjects [16]. We chose ten pieces with either a happy or a sad character (five happy, five sad) and arranged them in two sets, one with the happy pieces and the other with the sad pieces. In the sets, the musical pieces appeared in randomized order.
In each subject, we performed two runs with 12 min duration, respectively, separated by at least 2 h and maximal 24 h. In the first run, subjects were evaluating the pictures while listening to the unpleasant musical pieces inducing sadness, in the second run, they were listening to the pleasant music inducing happiness (see “Appendix 1” for the list of musical excerpts).
Electrophysiological parameters
During mood induction, electrophysiological parameters were recorded with surface electrodes (for details see [13]). Heart rate (HR) was used as an index of valence [25] and Galvanic Skin Response (GSR) as an index of arousal [2, 10]. In addition, we recorded surface electromyogram (EMG) activity of mimic muscles to detect facial expression of emotion [27].
Heart rate
HR was acquired from electrodes attached to the right and left arm or leg, using the aforementioned amplifier. The signal was filtered from 0.5 to 15 Hz (time constant, 0.3 s). Data were expressed as the mean period duration in seconds between two heart beats during one picture episode (interstimulus interval from picture onset to onset of next picture, ISI).
Galvanic skin response
GSR was measured with electrodes fixed to the medial thenar and palm of the hand. The signal was bandpass-filtered from 0.016 to 10 Hz (time constant, 10 s). Galvanic skin response amplitudes were determined as the maximum conductance between 1 and 6 s after picture onset, relative to the EMG baseline at picture onset. For GSR, amplitudes of more than two standard deviations from the mean of each individual and trials with zero amplitude were discarded.
Facial EMG
We recorded surface EMG of the corrugator supercilii muscle, the orbicularis oris and the orbicularis oculi muscle. The electrodes were placed over the bellies of these muscles of either the left or the right side except for the corrugator supercilii muscle, where electrodes were placed between the eyebrows (Fig. 1). The EMG signal was externally rectified and bandpass-filtered (16–300 Hz; time constant, 0.01 s). The signal was given as the root mean square of the EMG signal in Volt (V) during ISI.

Experimental setup. Subjects rated affective quality (valence) of pictures presented on a computer screen using a slide bar while listening to classical music presented via headphones. During the experiment, we measured heart rate, galvanic skin response and facial muscular activity
Statistical analysis
The statistical analysis was performed with Statistical Package for the Social Sciences (SPSS) IBM, version 19.0. In the text, mean and standard deviation (SD) are given. A priori, data were analyzed for normal distribution using the Kolmogorov–Smirnov test, electrophysiological data were z transformed. Accordingly, analysis of variance was performed with in-between subject factor group and within subject factor demographics, induction behaviour (yes/no), neuropsychological and electrophysiological data, where the latter were corrected for emotional lability (CNS-LS, CNS-LS-pos, CNS-LS-neg) and cognitive performance (ECAS total). To determine differences between groups in rating behaviour according to affective quality of pictures, Scheffé post hoc analysis was performed.
Kendall–Tau correlation analyses were conducted to determine association of mood-induction and emotional lability (PLC) and the association of PLC sub-scores and picture rating behaviour of patients. A threshold of p < 0.05 (two-tailed) was used for statistical interference.
Results
Neuropsychological data
ALS patients scored significantly higher in the “overall” CNS-LS compared to healthy controls (18.1 ± 4.5 vs. 11.2. ± 3.3 points, F = 15.96, p < 0.01). Patients had a significantly higher CNS-LS-neg score compared to CNS-LS-pos (70.0 % vs. 37.5 %, F = 3.09, p = 0.01) and a significantly higher CNS-LS-neg compared to controls (F = 21.16, p < 0.01), while controls did not show a difference between the two scores (32.7 vs. 31.5 %).
The ECAS scores of seven patients and ten controls where above threshold for cognitive impairment [12], and all subjects were able to understand and perform the task accordingly.
Picture rating
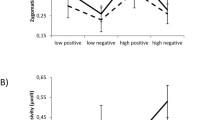
No clinically overt episodes of PLC were triggered during the experiment. For rating behaviour, both ALS patients and controls presented with a highly significant difference in the rating of pictures of different emotional content in both the happy and sad musical condition (F = 64.44, p < 0.01). In addition, PLC patients tended to rate neutral pictures accompanied by sad music more negatively, i.e. the difference between the rating of neutral and sad pictures in this group was less pronounced (post hoc Scheffé p = 0.03) than in controls. Regarding CNS-LS, we observed a significant correlation between CNS-LS score and mood induction for patients (r = 0.39, p = 0.04). For CNS-LS-pos, we found a correlation between the rating of positive pictures (r = 0.53, p < 0.01) and negative pictures (r = −0.34, p = 0.05), while for CNS-LS-neg, we observed a non-significant correlation with positive picture rating (r = −0.31, p = 0.07), but not with negative and neutral pictures. In other words, patients with a high positive score rated happy pictures more positively and negative pictures more negatively, while patients with a high negative score tended to rate positive pictures more negatively (Fig. 2). No significant effect could be observed for CNS-LS-pos and neutral pictures (r = −0.29, p = 0.097), nor for CNS-LS-neg and neutral (r = −0.14, p = 0.44) or sad pictures (r = 0.14, p = 0.42).

Mean values of picture ratings of ALS patients plotted against happy (upper row) and sad (lower row) CNS-LS sub-scores; x axis: CNS-LS score, y axis: picture rating; a happy pictures vs. CNS-LS-pos (r = 0.53, p < 0.01), b neutral pictures vs. CNS-LS-pos (p = 0.097, r = −0.29), c sad pictures vs. CNS-LS-pos (p = 0.05, r = −0.34), d happy pictures vs. CNS-LS-neg (p = 0.07, r = −0.31), e neutral pictures vs. CNS-LS-neg (r = −0.14, p = 0.44), f sad pictures vs. CNS-LS-neg (r = 0.14, p = 0.42)
Electrophysiological parameters
There was no significant difference between the two groups in the change of electrophysiological responses according to affective picture content. Group-differences in electrophysiological data were explained by frontal cortex function as expressed by the ECAS score (ANOVA corrected for ECAS score): EMG activity of the orbicularis oris muscle (F = 9.01, p < 0.01) and the orbicularis oculi muscle (F = 5.48, p = 0.036) and a non-significant trend for heart rate (F = 3.18, p = 0.096) and GSR (F = 2.95, p = 0.109) between the two musical conditions, while no difference could be observed for the corrugator supercilii muscle (F = 0.09, p = 0.77).
Discussion
Here, we systematically studied ALS patients suffering from PLC to find out whether episodes are elicited by contextually appropriate or inappropriate emotional stimuli, as there are controversial concepts on this issue [19, 22]. To address this question, an experimental set-up was designed with subjects confronted with visual and auditory stimuli of diverging emotional content simultaneously. We found that patients with PLC were more susceptible to mood-incongruent stimuli than controls. In particular, PLC patients rated pictures with a neutral content more negatively when listening to sad music. This mood induction in a negative direction was a consistent finding in PLC patients, but not in controls. We conclude that PLC is, thus, not induced by weak mood-congruent, but by mood-incongruent or contextually inappropriate stimuli. Also, our findings suggest that PLC is associated with enhanced emotional lability and is not only an involuntary motor activation of facial expression. We consider these findings being important for the clinical interpretation of emotional reactions of ALS patients.
It is another controversial question whether PLC is due to frontal cortex dysfunction with decreased inhibitory mechanisms or to altered processing of sensory stimuli, both of which would result in an exaggerated behavioural response. The PLC patients in our study did not exhibit an altered rating behaviour compared to controls when exposed to two emotionally equal stimuli. Thus, one may hypothesize that their reaction to sensory stimuli remained unaltered when there was no need for the emotion regulation system to suppress the answer to one stimulus to appropriately react to another. In contrast, patients were influenced in their behaviour when exposed to two stimuli of a diverging emotional content. This in turn may point to reduced inhibitory mechanisms, resulting in an exaggerated response to one stimulus and thus influencing the reaction to another simultaneously presented stimulus. Impaired voluntary suppression of emotional responses has been described before in ALS patients with PLC and has been interpreted as resulting from impairment of dorsal frontal brain structures [19]. When patients exhibit a clinically overt episode of PLC, this reduced inhibition might result in an exaggerated and contextually inappropriate emotional expression. We observed that PLC patients show an increased suggestibility when exposed to certain emotional stimuli, which in turn has an impact on their voluntary response. It may be hypothesized that this specific reaction is due to a lack of frontal inhibitory mechanisms in patients, resulting in specific behavioural alterations. In support of this, physiological changes in ALS patients, namely alterations of the surface EMG of facial muscles, were explained by frontal cortex function. Our findings are in line with a previous study reporting reduced ability of PLC patients on regulating their facial expression voluntarily [19]. We showed that altered facial expression in PLC is in fact related to frontal cortex function/dysfunction, by demonstrating that EMG changes of mimic muscles elicited by different emotional stimuli are closely related to cognitive performance and frontal function in PLC patients. This further supports the notion that the frontal cortex plays an important role in the pathophysiology of PLC. Recently, it could be convincingly shown in studies by Brettschneider et al. [3] that frontal changes, in particular of association fibres, exist neuropathologically in the majority of ALS patients.
We demonstrated that emotion regulation in PLC is altered at the behavioural as well as at the physiological level. To analyse changes in PLC at a third level of the emotion regulation system, i.e. the subjective level, patients and controls completed a standardized self-assessment questionnaire, the CNS-LS, to quantify the occurrence of emotional lability. We found that patients scored significantly higher on this scale compared to controls. In addition, we observed a significant correlation between CNS-LS and mood-induction. To differentiate between pathological laughing and pathological crying, we split the CNS-LS into questions scanning for sadness and happiness and found that these sub-scores did not only correlate with overall liability, but could in fact predict the direction of mood-induction in PLC patients. Remarkably, patients scored significantly higher on the CNS-LS-neg scale. Together with the fact that patients were influenced in their rating behaviour by sad musical pieces, this may suggest that patients with PLC are in general more sensitive to the negative component of emotion regulation. We conclude that the CNS-LS is a reliable instrument to detect emotional lability and PLC in patients with ALS. Yet, it does not sufficiently differentiate between pathological laughing and crying. We, therefore, suggest that the scale should be further sub-divided and possibly complemented by more specific questions.
One of the limitations of our study is the relatively small number of patients, which reduces the statistical power of our results and forbids general conclusions to a certain degree. Second, our findings are solely based on psychological and electrophysiological methods. While we could demonstrate specific alterations on different emotion regulating levels in our experimental setting, we could not show changes of functional connectivity between different brain regions.
To further support the hypotheses of involvement of frontal areas in the generation of PLC, additional methods, especially comprising fMRI protocols, should be applied. Standardized fMRI and resting-state protocols in patients with PLC might be able to verify alterations in specific frontal brain regions of these patients. Also, possible changes in connectivity of different functional areas of the brain, which we could not show using this protocol, might be revealed with fMRI and DTI techniques. In particular, it would be interesting to correlate psychophysiological and electrophysiological findings with MRI data. This in turn could help to further clarify the aforementioned concepts of the “top-down” and “bottom-up” theories in the pathogenesis of PLC and to support our hypothesis.
In summary, our study provides evidence that PLC/PBA in patients with ALS is an expression of altered emotional suggestibility. Patients with PLC are more prone to mood induction. In particular, they are easily influenced in their emotional response by mood-incongruent emotional stimuli. We showed that PLC involves alterations at the physiological, behavioural and subjective level of emotion regulation. Concerning underlying pathomechanisms, we hypothesize that PBA is related to frontal cortex dysfunction, in particular to reduced frontal inhibition, resulting in altered behavioural responses and physiological activity in PLC patients. Further studies combining imaging and psychophysiological techniques in larger cohorts will be needed to address the structural and pathophysiological mechanisms underlying PBA in different patient groups.
References
Abrahams S, Newton J, Niven E, Foley J, Bak TH (2014) Screening for cognition and behaviour changes in ALS. Amyotroph Lateral Scler Frontotemporal Degener 15(1–2):9–14. doi:10.3109/21678421.2013.805784
Bradley MM, Greenwald MK, Hamm AO (1993) Affective picture processing. In: Birbaumer N, Öhman A (eds) The structure of emotion. Hogrefe and Huber (publ.)
Brettschneider J, Del Tredici K, Toledo JB, Robinson JL, Irwin DJ, Grossman M, Trojanowski JQ (2013) Stages of pTDP-43 pathology in amyotrophic lateral sclerosis. Ann Neurol 74(1):20–38. doi:10.1002/ana.23937
Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron, Diseases (2000) El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 1(5):293–299
Dark FL, McGrath JJ, Ron MA (1996) Pathological laughing and crying. Aust N Z J Psychiatry 30(4):472–479
Floeter MK, Katipally R, Kim MP, Schanz O, Stephen M, Danielian L, Meoded A (2014) Impaired corticopontocerebellar tracts underlie pseudobulbar affect in motor neuron disorders. Neurology 83(7):620–627. doi:10.1212/WNL.0000000000000693
Gallagher JP (1989) Pathologic laughter and crying in ALS: a search for their origin. Acta Neurol Scand 80(2):114–117
Hartje W (2005) Störungen des emotionalen Verhaltens. In: Karnath HO, Hartje W, Ziegler W (eds) Kognitive Neurologie. Thieme, Stuttgart
Ironside R (1956) Disorders of laughter due to brain lesions. Brain 79(4):589–609
Lang PJ, Greenwald MK, Bradley MM, Hamm AO (1993) Looking at pictures: affective, facial, visceral, and behavioral reactions. Psychophysiology 30(3):261–273
Lang PJ, Bradley MM, Cuthbert BN (2008) International affective picture system (IAPS): affective ratings of pictures and instruction manual. Technical Report A-8. University of Florida, Gainesville
Lule D, Burkhardt C, Abdulla S, Bohm S, Kollewe K, Uttner I, Ludolph AC (2014) The Edinburgh cognitive and behavioural amyotrophic lateral sclerosis screen: a cross-sectional comparison of established screening tools in a German-Swiss population. Amyotroph Lateral Scler Frontotemporal Degener. doi:10.3109/21678421.2014.959451
Lule D, Kurt A, Jurgens R, Kassubek J, Diekmann V, Kraft E, Anders S (2005) Emotional responding in amyotrophic lateral sclerosis. J Neurol 252(12):1517–1524. doi:10.1007/s00415-005-0907-8
McCullagh S, Moore M, Gawel M, Feinstein A (1999) Pathological laughing and crying in amyotrophic lateral sclerosis: an association with prefrontal cognitive dysfunction. J Neurol Sci 169(1–2):43–48
Miller A, Pratt H, Schiffer RB (2011) Pseudobulbar affect: the spectrum of clinical presentations, etiologies and treatments. Expert Rev Neurother 11(7):1077–1088. doi:10.1586/ern.11.68
Mitterschiffthaler MT, Fu CH, Dalton JA, Andrew CM, Williams SC (2007) A functional MRI study of happy and sad affective states induced by classical music. Hum Brain Mapp 28(11):1150–1162. doi:10.1002/hbm.20337
Morris JC, Mohs RC, Rogers H, Fillenbaum G, Heyman A (1988) Consortium to establish a registry for Alzheimer’s disease (CERAD) clinical and neuropsychological assessment of Alzheimer’s disease. Psychopharmacol Bull 24(4):641–652
Murai T, Barthel H, Berrouschot J, Sorger D, von Cramon DY, Muller U (2003) Neuroimaging of serotonin transporters in post-stroke pathological crying. Psychiatry Res 123(3):207–211
Olney NT, Goodkind MS, Lomen-Hoerth C, Whalen PK, Williamson CA, Holley DE, Rosen HJ (2011) Behaviour, physiology and experience of pathological laughing and crying in amyotrophic lateral sclerosis. Brain 134(Pt 12):3458–3469. doi:10.1093/brain/awr297
Oppenheim H, Siemerling E (1886) Mitteilungen uber Pseudobulbarparalyse und akute Bulbarparalyse. Berl kli Woch, 46
Parvizi J, Anderson SW, Martin CO, Damasio H, Damasio AR (2001) Pathological laughter and crying: a link to the cerebellum. Brain 124(Pt 9):1708–1719
Parvizi J, Coburn KL, Shillcutt SD, Coffey CE, Lauterbach EC, Mendez MF (2009) Neuroanatomy of pathological laughing and crying: a report of the American Neuropsychiatric Association Committee on Research. J Neuropsychiatry Clin Neurosci 21(1):75–87. doi:10.1176/appi.neuropsych.21.1.75
Poeck K (1969) Pathological laughing and weeping in patients with progressive balbar palsy. Ger Med Mon 14(8):394–397
Pollack IF, Polinko P, Albright AL, Towbin R, Fitz C (1995) Mutism and pseudobulbar symptoms after resection of posterior fossa tumors in children: incidence and pathophysiology. Neurosurgery 37(5):885–893
Schandry R (1981) Psychophysiology: Körperliche Indikatoren menschlichen Verhaltens. US Psychologie, Urban und Schwarzenberg, Munchen Wien Baltimore
Schiffer R, Pope LE (2005) Review of pseudobulbar affect including a novel and potential therapy. J Neuropsychiatry Clin Neurosci 17(4):447–454. doi:10.1176/appi.neuropsych.17.4.447
Schwartz GE, Fair PL, Salt P, Mandel MR, Klerman GL (1976) Facial muscle patterning to affective imagery in depressed and nondepressed subjects. Science 192(4238):489–491
Smith RA, Berg JE, Pope LE, Thisted RA (2004) Measuring pseudobulbar affect in ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 5(Suppl 1):99–102. doi:10.1080/17434470410020058
Wilson SAK (1924) Some problems in neurology. II: pathological laughing and crying. J Neurol Psychopathol 4:299–333
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
The authors declare that they do not have any actual or potential conflicts of interest.
Appendix 1: List of musical excerpts
Appendix 1: List of musical excerpts
Composer | Title | |
|---|---|---|
Sad | Albinoni | Adagio in sol minor |
Bruch | Kol Nidrei | |
Grieg | Solveig’s song—Peer Gynt | |
Rodrigo | Concerto de Aranjuez | |
Sinding | Suite for violin & orchestra A minor | |
Happy | Bizet | Chanson du toreador—Carmen |
Mozart | Allegro—A little night music | |
Mozart | Rondo Allegro—A little night music | |
Strauß | Blue Danube | |
Strauß | Radetzky march |
Rights and permissions
About this article

Cite this article
Hübers, A., Kassubek, J., Grön, G. et al. Pathological laughing and crying in amyotrophic lateral sclerosis is related to frontal cortex function. J Neurol 263, 1788–1795 (2016). https://doi.org/10.1007/s00415-016-8201-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00415-016-8201-5