
Abstract
The objectives of this work were to validate two published methods for subadult age estimation based on measurements of the pars lateralis, and to develop a new method based on a wider set of measurements using the Granada Osteological Collection. The pars lateralis of 127 individuals from 6 months prenatal to 4 years of age were measured, taking 6 measurements of the body, the anterior synchondrosis and the condyle. Length and width were used to validate the published methods. Regression functions using age as the independent variable were calculated using each of the six measurements taken, and functions for age estimation were obtained through classical calibration. Functions for calculation of the 95% confidence interval of the estimates were obtained through linear regression using the estimation errors. In the validation of the previous methods, one method showed a linear tendency of the differences, which can be attributed to a circularity in reasoning in the original work. In the other method, a tendency towards overestimation was found, which can be attributed to the limitations of the method itself. The new functions have a consistency rate of 92.2% to 97.1%; the functions derived from all measurements are useful from 6 months prenatal to 2 years of age. Moreover, the functions obtained are applicable to incomplete pars lateralis, allowing for age estimation in a wide set of contexts and providing straightforward age estimates with their respective margin of error.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In recent years, several studies have contributed to refining methods of sex and age estimation in subadult skeletal remains. Although there is consensus in that methods based on dental development are the most reliable [1,2,3], it is desirable that a wide “toolbox” of methods be available in order to encompass a wide range of forensic and archaeological settings where the recovery of fragmented and isolated skeletal elements is usual. Thus, a diverse array of skeletal elements from a growing number of documented skeletal collections has been studied to assess morphological changes [4] and metric variation of cranial [5, 6] and postcranial skeletal elements [7,8,9].
Regarding the metric variation of the skull, the occipital bones and specifically the pars basilaris has received special attention, especially by virtue of its relatively late fusion with the rest of the skull and its compact nature, resistant to taphonomic factors [5, 10,11,12]. In its immediate anatomical vicinity, the pars lateralis has also been the subject of studies [6, 10, 11, 13], which reveal its potential for age determination in infant individuals. However, we believe that these studies did not exploit the full potential of the pars lateralis as only two measurements were applied: length and width (with slight differences in their definition depending on the author—see [14]), which are based on the posterior and lateral margins of the bone, prone to destruction by taphonomic factors. The first aim of this paper is to validate two of the methods derived from the pars lateralis, namely the ones proposed by Fazekas and Kósa [11] and Smith et al. [6], both of which use the same set of measurements. The second and main purpose is to provide a method for subadult age determination from pars lateralis measurements with four practical aspects in mind. First, we seek to employ clearly referenced measurements of different components of the bone that will allow for the use of incomplete elements. Second, we intend the method to be easy to apply, allowing for age estimations using a caliper and straightforward calculations. Third, we aim to provide specific formulae for situations in which the sex of the individual can be assessed, and general formulae for cases in which sex cannot be known. Finally, we propose a simple method for determining the 95% confidence interval of each estimate, in order to provide all the necessary information on the reliability of the estimates.
Materials and methods
Sample
The pars lateralis of 186 individuals were measured from the Granada Osteological Collection of Identified Infants and Young Children, composed at the time of this study of 241 individuals of known sex and age, ranging from 5 months of gestation to 8 years, most of whom were younger than 1 year [15]. Cases with pathologies that could eventually influence skull development (anencephaly, hydrocephalus) and cases with no recorded age at death were eliminated from the analysis, leaving a total of 127 individuals: 55 females and 72 males (Table 1).
Measurements
The measurements taken were as follows, using a digital caliper and registering up to 0.1 mm:
-
1.
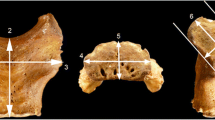
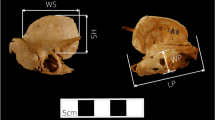
Maximum length (Fig. 1a). The greatest distance measured between the anterior and posterior interoccipital synchondroses [11]. Typically, the measurement involves the lateral margin of the jugular branch of the anterior intraoccipital synchondrosis, and the region between the posterior and lateral laminae of the posterior intraoccipital synchondrosis. If any bony projection is found, it should be included in the measurement (Fig. 1b).
-
2.
Maximum width (Fig. 1a). The greatest distance measured between the medial and lateral margins of the posterior interoccipital synchondrosis [11]. The measurement should be made with the caliper parallel to the main plane of the bone to ensure the maximum measurement, considering morphological variations due to bone development (Fig. 1c).
-
3.
Length of the anterior synchondrosis (Fig. 2). The maximum distance measured between the jugular and condylar branches of the anterior intraoccipital synchondrosis.
-
4.
Width of the anterior synchondrosis (Fig. 2). Maximum measurement taken on an axis perpendicular to the length. The measurement should be taken with the caliper parallel to the anterior surfaces of the synchondrosis to measure the maximum width regardless of whether it is on the jugular or condylar branch.
-
5.
Length of occipital condyle (Fig. 3a). Maximum dimension of the condyle taken in the anteroposterior axis. If a ridge is present, it should be included in the measurement (Fig. 3b).
-
6.
Width of the occipital condyle (Fig. 3a). Maximum measurement of the condyle in an axis perpendicular to the length. It is convenient to take it with the caliper parallel to the surface of the condyle to measure the maximum dimension.

a Location of the length (1) and width (2) of the pars lateralis. Panels b and c show the procedures for recording length and width when exostoses or variants in shape are found

Location of the length (3) and width (4) of the anterior synchondrosis of the pars lateralis

a Location of the length (5) and width (6) of the condyle. Panel b shows the procedure for recording length when a distinct rim is found
By default, all available pars lateralis were measured regardless of their side; however, due to poor preservation, not all measurements could be taken on all bones. The left element was selected for the analysis; to verify whether the left and right elements were interchangeable when the left measurement could not be taken, the measurements of both sides were compared using Student's t-test for paired samples.
To estimate the intra- and interobserver error, repeat measurements were performed several days after the original measurements on a random sample of 43 individuals, both by the original investigator (GF) and by one of us (JIO). These measurements were evaluated using the concordance correlation coefficient (CCC) [16] interpreted using the criteria suggested by McBride [17]. CCC calculations were performed using the DescTools package in the R 3.6.2 statistical environment [18].
Validation of previous methods
The effectiveness of the methods proposed by Fazekas and Kósa [11] and by Smith et al. [6]—both based on the length and width of the pars lateralis—on the Granada skeletal collection was tested in different ways owing to the difference in procedures employed by each method. Fazekas and Kósa [11] provide reference tables with the ranges of measurements attributable to each age, grouped in intervals of half a lunar month (2 weeks). Therefore, in this case, age was estimated for those individuals whose measures of length and width of the pars lateralis were within the range covered by the original method. As the age distribution of the measured individuals (Table 1) departs from normality, the estimates were compared with the chronological age of the official records using the Wilcoxon test for paired samples. The median and interquartile range of the differences between estimates and real age were calculated, and the number of overestimated and underestimated cases was counted.
The analysis carried out by Smith et al. [6] on the Lisbon and Spitalfields skeletal collections provides a set of linear functions for age estimation, accompanied by their respective mean standard errors which, when multiplied by two, provide 95% confidence intervals for age estimates. Therefore, in addition to determining the age of the remains from the Granada collection from length and width using the corresponding linear functions, the 95% confidence interval of the estimates was calculated. A concordance rate for each function was calculated as the percentage of individuals whose real age fell within the 95% confidence interval of the estimate. As with the Fazekas and Kósa method, the comparison between the actual ages and the point estimates was performed using a Wilcoxon test for paired samples, the number of overestimated and underestimated cases were counted, and the median and interquartile range of the differences with the point estimates were calculated.
Regression functions
Graphical inspection of the data (Figs. 4 and 5) suggests that the best relationship between age and measurements is logarithmic, so a linear regression of each measurement as a function of the logarithm of age was performed, with the resulting equations having the following general form:

Logarithmic relationship between the length of the pars lateralis and gestational age

Linearized relationship between the length of the par lateralis and gestational age, showing distinct departures from linear tendency in black
Once the regression equations were calculated, they were transformed to solve for age, so that the general form of the estimating equations is as follows:
This classical calibration procedure was preferred to the calculation of regression equations, using age as the dependent variable because of the bias this introduces in the residuals, and which has been widely documented [19].
Prior to performing the regression analysis, a graphical inspection of the relationship between the measurements and the logarithm of age was performed to detect deviations from homoscedasticity, and to determine the age intervals in which the linear relationships held in order to avoid behaviours in the data that alter the slope of the regression. The equations were calculated from the gestational age (GA) of the individuals, calculated by adding 280 days to the postpartum chronological age. Thus, prenatal individuals had ages less than 280 days. To obtain the age in years of the individuals analysed, 280 days must be subtracted from the age value obtained, and then divide the resulting number of days by 365. Regression equations were performed for all individuals, and for individuals of each sex separately, with ANCOVA testing of the difference between their slopes. The graphical representation of the data was performed with the ggplot2 package [20], and all statistical analyses were performed in the R 3.6.2 environment [18].
Error of the estimate and internal validation
The standard error of the regression coefficient behaves as a variation in the slope that oscillates about the mean of the independent variable—in this case, the logarithm of age. Therefore, the standard errors (and resulting confidence intervals) of the estimates widen as they move away from the mean and must be calculated for each case. There are formulae available both for estimating values of the dependent variable from the linear regression equation [21] and for values of the independent variable solved from the transformed equation [22]. However, for practical purposes, we opted in this study to provide linear regression equations of the margin of error on the estimated age for each formula. This allows us to quickly calculate the 95% confidence interval of the point estimate of age obtained from the formula by employing equations with the following general form:
The formulae for calculating the error were obtained from the confidence intervals of the age estimates of each formula, using the investr package [22] in the R 3.6.2 environment [18]. In addition, for comparative purposes, the mean standard error (MSE) of each age estimation formula was calculated using the confidence intervals.
Internal validation of the models was carried out by applying them on the original data. The age estimates were considered in concordance with the real age of the individuals if the latter fell within the 95% confidence interval of the estimate. A concordance rate was calculated as the percentage of individuals with concordant age estimates.
Results
Comparison of the measurements of left and right elements yielded results indicating no evidence (t = 0.205, df = 170, p = 0.838 for condyle length) to weak evidence (t = 1.739, df = 156, p = 0.084 for synchondrosis length) for asymmetry between the sides, so the left pars lateralis was used by default, turning to the right element if the left was absent or could not be measured due to poor preservation. This resulted in the number of elements for each measurement shown in Table 2. The results for intra- and interobserver error (Table 3) show a concordance of more than 95%, thus being substantial to near perfect for all measures.
The results obtained for the validation of the methods proposed by Fazekas and Kósa [11] and by Smith et al. [6] are shown in Table 4. In the Fazekas and Kósa method, significant differences were found for maximum length but not maximum width. However, graphical examination of the differences (Fig. 6a–b) showed a tendency to overestimate prenatal ages, and to underestimate ages around the moment of birth. Moreover, a distinct linear tendency was observed in the differences. Applying the method proposed by Smith et al. [6] to the Granada pars lateralis data, strong evidence was found for a tendency towards overestimation of the point estimates, but high consistency rates were found when the 95% confidence interval was considered (Table 4; Fig. 6c–d).

Differences between estimated age and real age found when applying the methods of Fazekas and Kósa [11] for length (a) and width (b) and Smith et al. [6] for length (c) and width (d) to the Granada skeletal collection. Dots represent the point estimates of age; lines represent the 95% confidence interval of the estimates. Points below the horizontal lines represent underestimates; points above the horizontal lines represent overestimates
Graphical inspection of the relationship between the logarithm of age and measurements yielded several deviations from linearity, recorded from 2 years of age (GA = 1010) for maximum length, maximum width, and the widths of the synchondrosis and the condyle (Fig. 5 ). Therefore, the range of predicted ages was restricted to 2 years for these measurements, and to 4 years (GA = 1740) for the remaining measurements.
Regression functions
The formulae for estimating age based on the regression functions obtained are shown in Table 5, together with their coefficient of determination (R2), their concordance rate, and the formula to obtain the error for each case. All models presented R2 greater than 0.8; the lowest concordance rate (92.2%) corresponds to the formula for condyle length in male individuals.
The formulae are applied calculating the division of the difference between the measurement and the intercept (a) by the slope (b) and using this result as the exponent for the base of the natural logarithm (e). For example, in the case of measuring a synchondrosis length of 12.4 mm, the application of the general formula (Table 5, formula 3) yields a gestational age of the following:
The margin of error to be considered for the 95% confidence interval of this estimate is as follows:
Therefore, the 95% estimate of gestational age is 341 to 781 days, that is, between two and 16.7 months. In case narrower confidence intervals are desired, the standard error can be obtained using an approximation to the t distribution, by dividing the error obtained by the formula by two.
The sex-specific regressions and formulae show R2 indices and concordance rates similar to the general formulae, and the formulae for male individuals yield a narrower confidence interval. For example, application of the formula for male individuals (Table 5, formula 9) to the above example yields a GA of 529 ± 183 days. The formulae for female individuals showed wider confidence intervals: application of the corresponding formula (Table 5, formula 15) to the above example yields a GA of 592 ± 269 days. In formulae derived from three measurements (synchondrosis length, condyle length, and condyle width), moderate evidence was found for a difference in slopes between males and females (Table 5; Fig. 7a). Although in the other formulae this difference is statistically non-existent (Fig. 7b), it is advisable to employ the specific formulae whenever possible.

Differences between the slopes for male and female individuals, exemplified through the functions for condylar length (a, significant) and maximum length (b, non-significant)
Discussion
As for the validation of the methods obtained by other authors, apart from the fact that the method proposed by Fazekas and Kósa [11] does not provide margins of error, the linear tendency observed upon graphical inspection deserves more attention. A close reading of the original work [11] reveals that, owing to possible reporting errors, the skeletal material was not grouped according to reported gestational age but rather according to size (pp. 30–31). This leads to a circularity in the reasoning by which the size of the skeletal element is used to estimate age through a method where the age of the reference sample is also an estimate based on size. Therefore, not only the methods based on pars lateralis but all methods proposed by Fazekas and Kósa [11] should be considered unreliable.
The application of the method proposed by Smith et al. [6] on the Granada skeletal sample showed a systematic overestimation in the point estimates. We believe the main reason for this is to be found in the method, which is based on dividing the growth curve into intervals that can reasonably be fit to a straight line. In this study, we decided to use the logarithmic model for several reasons. In the first 5 years after birth, growth is best described as a “decaying polynomial”, departing negatively from a linear rate with time [23]. It is desirable to fit singular models into this pattern, and for the period considered we found that a logarithmic model was appropriate. Also, the cut-off point between one function and the next is based on the behaviour of the dataset and can be of limited use for ages near the age limit between each linear model, where substantial overlap between measurement values can be found. This notwithstanding, the method proposed by Smith et al. [6] shows a considerable concordance between estimated age and real age when the 95% confidence interval is considered, effectively validating the method through the Granada skeletal collection. It should be noted, however, that the mean standard errors (MSE) calculated using the confidence intervals of the methods proposed in this work are substantially lower than the ones calculated by Smith and colleagues (i.e., 65 days = 0.18 years vs. 0.37 years for length, and 74 days = 0.20 years vs. 0.40 years for width).
The results obtained for intra- and interobserver error of the new measurements proposed show a very high degree of agreement. This suggests a high applicability, always assuming careful reading of the descriptions and the graphical guides (Figs. 1, 2 and 3) prior to taking the measurements. The regression functions obtained on the entire set of measurements have the following features:
-
The formulae corresponding to maximum length, maximum width, anterior synchondrosis width, and condyle width can be applied to the remains of individuals between 6 months of gestation (GA = 184 days) and 2 years (GA = 1010 days).
-
The formulae for anterior synchondrosis length and condyle length can be applied to individuals between 6 months gestation and 4 years (GA = 1740 days).
-
All formulae are applicable to isolated pars lateralis elements; in addition, in cases where the pars lateralis is fused with the occipital squama but not with the pars basilaris, it is still possible to apply the formulae for the anterior synchondrosis and the condyle.
-
If adequate (morphological or molecular) indicators of the sex of the individual are available, it is advisable to apply the sex-specific formulae.
It should be noted that the confidence intervals increase rapidly with the estimated age; in most of the formulae, the error exceeds 1 year in estimates beyond their range of applicability. However, the errors of the formulae for the length of the condyle exceed one year for age estimates of 1 year or less, being therefore not applicable in general. For the length of the synchondrosis, this error is 1 year in age estimates of a little more than 1 year, so they are useful for individuals of up to 2 years reducing the confidence interval to less than 95%. Even considering these limitations, we find it important to present these formulae as potential tools for isolated or fragmented pars lateralis elements.
Regarding accuracy testing, we chose to include the entire sample for the regression analysis, privileging sample size over the practical convenience of retaining a test sample. Thus, the only measures of accuracy we can offer are the result of the concordance rates detailed in Table 5. Furthermore, the applicability of the method proposed in this work on other populations remains an open issue. Nutrition, disease, and genetic factors all influence growth rates in different stages of infancy and childhood, being nutrition a crucial factor during the first few years [24]. These factors depend on socioeconomic status and population history, and this should be considered in the analysis of the samples that were inevitably drawn from peoples who lived and died in a variety of circumstances. The validation of these formulae in populations from a variety of contexts will be crucial in the determination of their applicability, and in their eventual calibration for other realities. Moreover, the validation and comparison will allow us to determine if the patterns found in this study can be generalized or are peculiarities of the sample, as for example the apparent faster growth of the pars lateralis in males as reflected in a higher slope in the regression formulae.
Finally, this is admittedly a fairly simple approach to the matter at hand considering recent developments, as for example geometric morphometrics [25], transition analysis [26] and Bayesian calibration [27, 28]. However, in many cases, these studies usually require considerable statistical expertise or specific software. A balance should be sought between the accuracy of the methods, their sophistication, and their applicability.
Data availability
The dataset generated and analysed during the current study are available from the corresponding author on reasonable request.
References
AlQahtani SJ, Hector MP, Liversidge HM (2010) Brief communication: the London atlas of human tooth development and eruption. Am J Phys Anthropol 142:481–490. https://doi.org/10.1002/ajpa.21258
García-Mancuso R (2014) Congruencia entre edad esquelética y desarrollo dentario en una muestra osteológica con edad cronológica documentada. Rev Argentina Antropol Biológica 16:103–109
Irurita Olivares J, Alemán Aguilera I, Viciano Badal J, De Luca S, Botella López MC (2014) Evaluation of the maximum length of deciduous teeth for estimation of the age of infants and young children: proposal of new regression formulas. Int J Legal Med 128:345–352. https://doi.org/10.1007/s00414-013-0903-y
Cardoso HFV, Gomes J, Campanacho V, Marinho L (2013) Age estimation of immature human skeletal remains using the post-natal development of the occipital bone. Int J Legal Med 127:997–1004. https://doi.org/10.1007/s00414-013-0818-7
Irurita Olivares J, Alemán Aguilera I (2017) Proposal of new regression formulae for the estimation of age in infant skeletal remains from the metric study of the pars basilaris. Int J Legal Med 131:781–788. https://doi.org/10.1007/s00414-016-1478-1
Smith DEM, Humphrey LT, Cardoso HFV (2021) Age estimation of immature human skeletal remains from mandibular and cranial bone dimensions in the postnatal period. Forensic Sci Int 327:110943. https://doi.org/10.1016/j.forsciint.2021.110943
Cardoso HFV, Spake L, Humphrey LT (2017) Age estimation of immature human skeletal remains from the dimensions of the girdle bones in the postnatal period. Am J Phys Anthropol 163:772–783. https://doi.org/10.1002/ajpa.23248
Cardoso HFV, Vandergugten JM, Humphrey LT (2017) Age estimation of immature human skeletal remains from the metaphyseal and epiphyseal widths of the long bones in the post-natal period. Am J Phys Anthropol 162:19–35. https://doi.org/10.1002/ajpa.23081
Picó Pérez C, Irurita Olivares J, Alemán Aguilera I (2017) Validation methods of Fazekas and Kósa and Molleson and Cox for age estimation of the ilium in Western Mediterranean non-adult population: proposal of new regression formulas. Int J Legal Med 131:789–795. https://doi.org/10.1007/s00414-016-1475-4
Redfield A (1970) A new aid to aging immature skeletons: development of the occipital bone. Am J Phys Anthropol 33:207–220. https://doi.org/10.1002/ajpa.1330330206
Fazekas IG, Kósa F (1978) Forensic fetal osteology. Akadémiai Kiadó, Budapest
Scheuer L, MacLaughlin-Black S (1994) Age estimation from the pars basilaris of the fetal and juvenile occipital bone. Int J Osteoarchaeol 4:377–380. https://doi.org/10.1002/oa.1390040412
Thornton R, Edkins AL, Hutchinson EF (2020) Contributions of the pars lateralis, pars basilaris and femur to age estimations of the immature skeleton within a South African forensic setting. Int J Legal Med 134:1185–1193. https://doi.org/10.1007/s00414-019-02143-9
Scheuer L, Black S (2004) The juvenile skeleton. Academic Press, San Diego
Alemán I, Irurita J, Valencia AR, Martínez A, Lõpez-Lázaro S, Viciano J, Botella MC (2012) Brief communication: the Granada osteological collection of identified infants and young children. Am J Phys Anthropol 149:606–610. https://doi.org/10.1002/ajpa.22165
Lin LI-K (1989) A concordance correlation coefficient to evaluate reproducibility. Biometrics 45:255–268. https://doi.org/10.2307/2532051
McBride GB (2005) A proposal for strength-of-agreement criteria for Lin’s concordance correlation coefficient. Hamilton, New Zealand
R Development Core Team (2019) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna. https://www.R-project.org/
Aykroyd RG, Lucy D, Pollard AM, Solheim T (1997) Regression analysis in adult age estimation. Am J Phys Anthropol 104:259–265. https://doi.org/10.1002/(sici)1096-8644(199710)104:2%3C259::aid-ajpa11%3E3.0.co;2-z
Wickham H (2016) ggplot2: elegant graphics for data analysis. Springer-Verlag, New York
Lucy D (2005) Introduction to statistics for forensic scientists. Wiley, Chichester
Greenwell BM, Schubert Kabban CM (2014) investr: an R Package for inverse estimation. R J 6:90–100
Cameron N (2022) The pattern of human growth. In: Cameron N, Schell LM (eds) Human growth and development, 3rd edn. Academic Press, San Diego, pp 1–22
Stinson S (2012) Growth variation: biological and cultural factors. In: Stinson S, Bogin B, O’Rourke D (eds) Human biology: an evolutionary and biocultural perspective. Wiley, Hoboken, pp 587–635
Braga J, Treil J (2007) Estimation of pediatric skeletal age using geometric morphometrics and three-dimensional cranial size changes. Int J Legal Med 121:439–443. https://doi.org/10.1007/s00414-007-0170-x
Tangmose S, Thevissen P, Lynnerup N, Willems G, Boldsen J (2015) Age estimation in the living: transition analysis on developing third molars. Forensic Sci Int 257:512.e1-512.e7. https://doi.org/10.1016/j.forsciint.2015.07.049
Konigsberg LW, Frankenberg SR (2013) Bayes in biological anthropology. Am J Phys Anthropol 152:153–184. https://doi.org/10.1002/ajpa.22397
Ferrante L, Skrami E, Gesuita R, Cameriere R (2015) Bayesian calibration for forensic age estimation. Stat Med 34:1779–1790. https://doi.org/10.1002/sim.6448
Funding
Gonzalo Figueiro received partial financial support from the Comisión Sectorial de Investigación Científica, Universidad de la República, Uruguay (2019 Academic Mobility and Exchanges Programme).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Research involving Human Participants and/or Animals
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Figueiro, G., Irurita Olivares, J. & Alemán Aguilera, I. Age estimation in infant skeletal remains by measurements of the pars lateralis. Int J Legal Med 136, 1675–1684 (2022). https://doi.org/10.1007/s00414-022-02867-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-022-02867-1