
Abstract
Estimation of age at death is important in forensic investigations of unknown remains. There have been several reports on applying the degree of osteophyte formation—an age-related change in the vertebral body—for age estimation; however, this method is not yet established. This study investigated a method for age estimation of modern Japanese individuals using osteophytes measured on CT images. The sample included 250 cadavers (125 males) aged 20–95 years. The degree of osteophyte formation was evaluated as score O (0–5 points), and the degree of fusion of the osteophytes between the upper and lower vertebrae was evaluated as score B (0–2 points). Age estimation equations were developed using regression analyses with seven variables, determined by scores O and B, and the equation with the smallest standard error of estimate (SEE) was obtained when the number of vertebrae with score O ≥ 2 was used as the explanatory variable. Age estimation with SEE of about 10 years was possible even when partial vertebrae with a high degree of osteophyte formation were used, showing its potential for practical application. The cutoff value for age estimation was established using the receiver operating characteristic curve analysis, wherein good results were obtained for all variables (area under the curve ≥ 0.8). The combination of the estimation equation and the cutoff value can narrow the range of age estimates.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Estimation of age at death is part of determining the biological profile of the deceased and is crucial in the forensic investigation of unknown remains. Various parts of the bone such as diaphyseal length, cranial suture, pubic symphysis, fourth rib, and ilium auricular surface have been used for age estimation; however, the accuracy of these common age estimation methods depends on the experience level and knowledge of the observer [1]. Moreover, it is currently difficult to estimate the age of a deceased, middle-aged adult with a high degree of accuracy [2, 3]. As the aging population grows, further research on age estimation methods to be applied for relatively older age groups will be soon required.
It is widely known that osteophytes of the vertebral column develop with age and represent one of the most common age-related changes [4]. Several studies have examined the relationship between osteophytes and age and have shown a significant correlation between osteophyte formation and age [5,6,7,8,9,10,11,12]. However, the first study to apply this to an age estimation equation was published recently, in 2006, by Watanabe et al. [13]. In the previous study, the degree of osteophyte formation in the vertebral column was evaluated by palpation at the time of autopsy on a 4-point scale and used as the osteophyte formation index to examine its correlation with age. Subsequently, Praneatpokgrang et al. measured the length of osteophytes from the second cervical vertebra to the fifth lumbar vertebra, scored each vertebra on a scale of 0–5, and reported an age estimation formula using the average value [14]. However, the age estimation method using vertebrae is not yet a well-established method, as there has been a very limited number of published reports, and some reports indicate that it is ineffective for estimating age by regression equation or narrowing age estimate due to its large variability [8].
Globally, postmortem computed tomography (PMCT) is increasingly being utilized in forensic departments to assist in forensic autopsies [15,16,17]. This has resulted in the increasing use of CT images in the field of forensic anthropology. The use of CT images enables rapid, non-destructive observation of the bone without requiring any preparation. Moreover, the bone structure can be clearly observed, making it possible for relatively inexperienced examiners to perform bone examinations [18, 19]. Furthermore, it is possible to create multiplanar reconstructed (MPR) images and three-dimensional images, providing more information than conventional radiographic examinations [20]. CT is considered a potential tool in forensic anthropology and has been reported to be beneficial for several bone sites, including the sternum, medial end of the clavicle, cranial suture, and pelvic bones; however, there is no previous reports of age estimation with osteophytes using CT images [21,22,23,24,25,26]. This study aimed to determine the presence and extent of vertebral osteophytes in an adult Japanese population and to use this data to develop an age estimation method for this particular population.
Materials and methods
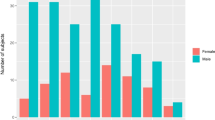
We reviewed data of 250 subjects with known age and sex (125 males, aged 20–95 years, mean 51 ± 22 years, the number of cadavers aged 20–29 = 23, aged 30–39 = 18, aged 40–49 = 16, aged 50–59 = 16, aged 60–69 = 16, aged 70–79 = 20, aged 80–89 = 12, aged 90–95 = 4; 125 females, aged 20–91 years, mean 52 ± 21 years, the number of cadavers aged 20–29 = 20, aged 30–39 = 18, aged 40–49 = 17, aged 50–59 = 17, aged 60–69 = 17, aged 70–79 = 18, aged 80–89 = 15, aged 90–91 = 2) who underwent PMCT and subsequent forensic autopsy at the Department of Legal Medicine at our University in Japan, between December 2009 and August 2016. All subjects belonged to Japanese or Northeast Asian ethnicities. Whole-body CT was performed before an autopsy in all cases, and subjects were excluded if their history included conditions or events, which could possibly affect the vertebrae, such as spinal injuries, multiple traumas, burn injuries, severe decomposition, congenital malformations, known diseases that could affect bone observations, and an atypical number of vertebrae.
PMCT was performed using a 16-row detector CT system (Eclos; Hitachi, Ltd., Tokyo, Japan). The scanning protocols were as follows: collimation, 1.25 mm; reconstruction interval, 1.25 mm; tube voltage, 120 kV; tube current, 200 mA; and rotation time, 1 s. Image data were processed on a workstation (Synapse Vincent; Fujifilm Medical, Tokyo, Japan) to obtain MPR images. The thoracic and lumbar vertebrae were observed using a bone kernel reconstruction, a window width of 1,500 Hounsfield units (HU), and a window level of 450 HU. The degree of osteophytes and bridging of each vertebra was scored according to the following methodology: the upper and lower surfaces of each vertebral body were observed in a plane parallel to the upper and lower vertebral body planes, respectively; the length of the perpendicular line from the most prominent osteophyte to the edge of the vertebral body limb in each plane “measurement o” was measured and classified as 0 to 5; and the score O was defined as the degree of osteophyte formation (Fig. 1, Table 1). The vertebrae were also observed on sagittal and coronal sections, and the degree of fusion between the vertebrae and osteophytes above the observed vertebrae was classified from 0 to 2, with score B indicating the degree of bridging (Fig. 2, Table 1). For all vertebral bodies in the thoracic and lumbar spine, the two scores, O and B, were measured and used to establish seven variables (Table 2). All subjects were evaluated by the same observer. To estimate intraobserver errors of scores O and B, 30 randomly selected subjects were re-evaluated by the same observer 6 months after the first evaluation. To estimate interobserver error, the same 30 subjects were also evaluated by a second observer.

Postmortem computed tomography images for measuring score O. a Sagittal section image of the vertebral body. The osteophytes are observed in the plane of the white dashed line in each thoracic and lumber spinal body; b the length of the perpendicular line from the most prominent osteophyte to the edge of the vertebral body limb was defined as “measurement o” in each axial or oblique axial plane defined in Fig. 1a

Postmortem computed tomography images for measuring score B. a No osteophytic fusion (bridging) or no close approximation (proximity) between upper and lower osteophytes (score B = 0); b proximity is observed, but bridging is not complete (score B = 1); c bridging between the upper and lower vertebral bodies is complete (score B = 2)
Statistical analyses were performed using the statistical software R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria. ISBN 3–900,051-07–0, URL http://www.R-project.org/) and Ekuseru-Toukei 2015 (Social Survey Research Information Co., Ltd., Tokyo, Japan). Cohen’s kappa analysis was used to examine inter-observer errors, and 0.80–1.0 indicated an almost perfect agreement [27, 28]. Descriptive statistics were performed for each variable. After the analysis of variance, Student’s t-test was used to compare the mean values between the sexes. The correlations between age at death and each variable were assessed using Pearson’s product-moment correlation coefficient, and the coefficient of determination (R2) was calculated. The standard error of estimate (SEE) was calculated to evaluate the validity of the regression equation.
Receiver operating characteristic (ROC) curve analysis was used to set the cutoff value of the variables in age estimation. To determine the most appropriate cutoff value for answering the question “above or below a certain age,” the range of 30–80 years and above was divided into eleven 5-year intervals, and ROC analysis was conducted for each age for all seven variables. The ROC curve represents a plot of the “false positive proportion” on the x-axis and the “true positive proportion” on the y-axis. The accuracy of the cutoff value was measured by the area under the curve (AUC); the larger the value of the AUC, the better the efficacy of the measurement in estimation. A test with perfect accuracy, or sensitivity and specificity of 100%, has an AUC value of 1, and when the variable is a perfectly random predictor, the AUC is 0.5. The AUC results were defined as follows: excellent, 0.9–1; good, 0.8–0.9; fair, 0.7–0.8; poor, 0.6–0.7; and finally, failed for AUC values between 0.5 and 0.6 [29, 30]. As a cutoff value, the one with the largest Youden’s index was adopted [31].
Moreover, P-values < 0.05 were considered statistically significant.
This study was approved by the Ethics Committee of our university. The requirement for informed consent from the next of kin was waived.
Results
The κ coefficients for intraobserver error were as follows; score O was 0.998 for the upper vertebral column, 0.998 for the lower, and 0.983 for score B, and those for interobserver error were as follows: score O was 0.995 for the upper vertebral column, 0.992 for the lower, and 0.954 for score B, wherein all values were above 0.9, indicating almost perfect agreement.
The results of the descriptive statistics for each variable are shown in Table 3. Although the degree of osteophyte formation and bridging was slightly higher in males, there was no significant difference between the sexes.
The results of the simple regression analysis with each variable as the explanatory variable and age as the objective variable are shown in Table 4. The SEE for both males and females was the smallest in the single regression analysis with O( +) as the explanatory variable, and it was < 10 years old (males, y = 2.924x + 27.394, SEE 9.884 years; females, y = 3.007x + 30.681, SEE 9.546 years).
The results of the ROC analysis are shown in the Supplementary Material Table 1. All variables showed excellent or good AUC values for all age groups, with several being above 0.95, indicating useful cutoff values. The P values were all < 0.01.
For example, if O(max) was 5, the regression equation would estimate the age range to be 59.7–79.9 years for males and 63.3–83.2 years for females. If the same value was used as the cutoff value obtained in the ROC analysis, it is determined to be ≥ 60 years for males (sensitivity 0.898; specificity 0.868) and ≥ 70 years for females (sensitivity 0.778; specificity 0.854). In addition to this, if O(-) was 1, it is estimated to be ≥ 65 years for males (sensitivity 0.872; specificity 0.814) and ≥ 75 years for females (sensitivity 0.808; specificity 0.838), and it may be possible to narrow the range of estimated ages by using different explanatory variables together.
Discussion
Single regression analysis in our study showed each variable using score O for both males and females and showed an age estimation equation with a SEE of about 10 to 11 years old, with O( +) showing the smallest SEE. O( +) had SEEs of < 10 years old, and it was considered to be effective. Previous studies have considered the length and degree of osteophytes for scoring and performing regression analysis; the number of vertebrae with obvious osteophytes was not considered [13, 14]. Our study is a first-of-a-kind report using a method that evaluates the number of vertebrae with osteophytes and shows it is useful in practice owing to its feasibility. O(maxL) is the least complicated evaluation method, as it only measures the length of the most developed osteophyte of the five lumbar vertebrae observed. The SEE of both males and females was relatively good at about 10.3 years, considering that the difference in SEE was less than 1 year compared with the smallest SEE (O( +)). The SEE of B(sum) was relatively large, about 14 years old, and each estimating equation using variables from score O was more useful.
ROC analysis showed excellent or good results for all variables with excellent results in about 77% (118/154) and results with AUC > 0.95 in 44% (68/154). While the other variables tended to have generally lower AUCs with age, B(sum) did not show a decrease in AUC values with increasing age for both males and females. B(sum) was found to be relatively more useful for estimating age after middle age, as high AUC values of 0.88 or higher for males and 0.9 or higher for females were obtained for all classes after age 40, and the highest AUC values were obtained for females aged 75 or older and 80 or older.
In this study, the SEE obtained using the regression equation using O( +) (males: 9.884 years; females: 9.546 years) is better than the SEE reported in the previous Japanese study (males, 12.6 years; females, 11.9 years) and comparable or slightly better than the SEE examined for Thai skeletal specimens (males, 10.275 years; females, 9.813 years) [13, 14]. In a previous study on Japanese people, the scoring method was subjective, and reproducibility was not examined. However, this study solved such issues by measuring the osteophytes scoring more objectively using CT images with high reproducibility. To observe the whole vertebral body as a skeletal specimen after soft tissue removal, as in the Thai method, is time-consuming and not feasible in clinical settings; further, it is ethically difficult to collect prospective data. Conversely, CT can obtain whole-body data quickly, and soft tissue can be easily removed with less ethical difficulty; thus, CT can be particularly useful for estimating the age at death by the vertebral body.
Praneatpokgrang et al. reported several regression equations for each vertebral body, except for the atlas, in the cervical, thoracic, and lumbar spine [14]. This is useful when the spine is completely preserved, or at least one of the cervical, thoracic, or lumbar spine is completely preserved.
However, the vertebral body is expected to be easily separated and partially missing owing to postmortem changes. This is often a problem in forensic anthropology. In addition to O( +), which had the smallest SEE among the variables in this study, O(sum) and O( −) require a complete thoracolumbar spine, and O(sumL) requires a complete lumbar spine to remain. On the other hand, O(max), O(maxL), and B(sum) may be used for age estimation even when only some of the vertebrae remain. If the osteophyte formation in the partially discovered skeleton is mild, it cannot be used because the undiscovered vertebrae may have advanced osteophytes, but if only one discovered vertebra has a maximum value of 5, an age estimate of about 10 years SEE is possible. Furthermore, if multiple vertebrae are fused and remain in a single mass, the regression equation using B(sum) can be used to narrow down the estimated age using a cutoff value.
Although very few reports have focused on setting the cutoff values for age estimation using ROC analysis, it may allow narrowing the range of estimated ages when used in conjunction with regression equations [32]. In this study, all variables showed good or excellent results, and it was also shown that it is possible to set excellent cutoff values with an AUC of 0.9 or higher, even for cadavers > 70 years. Although the Lamendin method was considered to be one of the most accurate age estimation methods for deceased persons > 40 years old, it has been reported to have the disadvantage of underestimating age with a mean error of about 19 years in elderly persons with periodontal disease [33, 34]. Even the iliac auricular surface, which can estimate the age of relatively older adults, cannot be used to classify people > 60 years [35]. This study is the first to provide cutoff values for age estimation at 5-year intervals for people aged ≥ 60 years, which strongly suggests that it is useful for estimating the age of the elderly, which is considered relatively difficult and may be particularly useful in forensic anthropology for the contemporary aging population.
Limitations
This study was conducted using data from modern adult Japanese, and other populations were not examined. Moreover, cross-validation was not performed, and the performances of the regression equation and the cutoff value may have been overestimated. Known diseases and obvious trauma were excluded, but chronic spine pathologies may not have been ruled out. It is known that osteophyte formation is also affected by microtrauma, environmental factors such as occupational and labor loads, and bone formation, which is influenced by various factors such as nutritional status. However, it was difficult to analyze these occupational and environmental factors in detail because of the lack of sufficient antemortem information as a characteristic of forensic autopsy cases. [4, 36, 37]. A prospective study is necessary for quantitative evaluation, although it seems difficult to carry out at present. Moreover, the cervical spine was not evaluated in this study due to the metal artifacts associated with dental treatment, which is considered an additional limitation.
Conclusion
This is the first study to use CT images of vertebral osteophytes to calculate both a regression equation and a cutoff value for age estimation. The results show that assessment of vertebral osteophytes by postmortem CT could be useful for estimating age at death in Japanese adults, especially in the older population.
Data availability
Not applicable.
Code availability
Not applicable.
References
Cunha E, Baccino E, Martrille L, Ramsthaler F, Prieto J, Schuliar Y, Lynnerup N, Cattaneo C (2009) The problem of aging human remains and living individuals: a review. Forensic Sci Int 193:1–13. https://doi.org/10.1016/j.forsciint.2009.09.008
Franklin D (2010) Forensic age estimation in human skeletal remains: current concepts and future directions. Leg Med 12:1–7. https://doi.org/10.1016/j.legalmed.2009.09.001
Thevissen PW, Galiti D, Willems G (2012) Human dental age estimation combining third molar(s) development and tooth morphological age predictors. Int J Legal Med 126:883–887. https://doi.org/10.1007/s00414-012-0755-x
Prescher A (1998) Anatomy and pathology of the aging spine1Dedicated. 1. Eur J Rad 27:181–195. https://doi.org/10.1016/S0720-048X(97)00165-4
Stewart TD (1958) The rate of development of vertebral osteoarthritis in American whites and its significance in skeletal age identification. Leech 28:144–151
Snodgrass JJ (2004) Sex differences and aging of the vertebral column. J Forensic Sci 49:458–463. https://doi.org/10.1520/JFS2003198
Chanapa P, Yoshiyuki T, Mahakkanukrauh P (2014) Distribution and length of osteophytes in the lumbar vertebrae and risk of rupture of abdominal aortic aneurysms: a study of dry bones from Chiang Mai, Thailand. Anat Cell Biol 47:157–161. https://doi.org/10.5115/acb.2014.47.3.157
Listi GA, Manhein MH (2012) The use of vertebral osteoarthritis and osteophytosis in age estimation. J Forensic Sci 57:1537–1540. https://doi.org/10.1111/j.1556-4029.2012.02152.x
Kasai Y, Kawakita E, Sakakibara T, Akeda K, Uchida A (2009) Direction of the formation of anterior lumbar vertebral osteophytes. BMC Musculoskelet Disord 10:4. https://doi.org/10.1186/1471-2474-10-4
Kacar E, Unlu E, Beker-Acay M, Balcik C, Gultekin MA, Kocak U, Eroglu S, Yucel A (2017) Age estimation by assessing the vertebral osteophytes with the aid of 3D CT imaging. Aust J Forensic Sci 49:449–458. https://doi.org/10.1080/00450618.2016.1167241
Van der Merwe AE, Işcan MY, L’abbé EN (2006) The pattern of vertebral osteophyte development in a South African population. Int J Osteoarchaeol 16:459–464. https://doi.org/10.1002/oa.841
Snodgrass JJ (2004) Sex differences and aging of the vertebral column. J Forensic Sci 49:JFS2003198-6
Watanabe S, Terazawa K (2006) Age estimation from the degree of osteophyte formation of vertebral columns in Japanese. Leg Med 8:156–160. https://doi.org/10.1016/j.legalmed.2006.01.001
Praneatpolgrang S, Prasitwattanaseree S, Mahakkanukrauh P (2019) Age estimation equations using vertebral osteophyte formation in a Thai population: comparison and modified osteophyte scoring method. Anat Cell Biol 52:149–160. https://doi.org/10.5115/acb.2019.52.2.149
Dirnhofer R, Jackowski C, Vock P, Potter K, Thali MJ (2006) VIRTOPSY: Minimally invasive, imaging-guided virtual autopsy. Radiographics 26:1305–1333. https://doi.org/10.1148/rg.265065001
Makino Y, Yokota H, Nakatani E, Yajima D, Inokuchi G, Motomura A, Chiba F, Torimitsu S, Uno T, Iwase H (2017) Differences between postmortem CT and autopsy in death investigation of cervical spine injuries. Forensic Sci Int 281:44–51. https://doi.org/10.1016/j.forsciint.2017.10.029
Leth PM (2009) Computerized tomography used as a routine procedure at postmortem investigations. Am J Forensic Med Pathol 30:219–222. https://doi.org/10.1097/PAF.0b013e318187e0af
Dedouit F, Telmon N, Costagliola R, Otal P, Joffre F, Rougé D (2007) Virtual anthropology and forensic identification: report of one case. Forensic Sci Int 173:182–187. https://doi.org/10.1016/j.forsciint.2007.01.002
Zech WD, Hatch G, Siegenthaler L, Thali MJ, Lösch S (2012) Sex determination from os sacrum by postmortem CT. Forensic Sci Int 221:39–43. https://doi.org/10.1016/j.forsciint.2012.03.022
Flach PM, Gascho D, Schweitzer W, Ruder TD, Berger N, Ross SG, Thali MJ, Ampanozi G (2014) Imaging in forensic radiology: an illustrated guide for postmortem computed tomography technique and protocols. Forensic Sci Med Pathol 10:583–606. https://doi.org/10.1007/s12024-014-9555-6
Grabherr S, Cooper C, Ulrich-Bochsler S, Uldin T, Ross S, Oesterhelweg L, Bolliger S, Christe A, Schnyder P, Mangin P, Thali MJ (2009) Estimation of sex and age of “virtual skeletons”–a feasibility study. Eur Radiol 19:419–429. https://doi.org/10.1007/s00330-008-1155-y
Barrier P, Dedouit F, Braga J, Joffre F, Rougé D, Rousseau H, Telmon N (2009) Age at death estimation using multislice computed tomography reconstructions of the posterior pelvis. J Forensic Sci 54:773–778. https://doi.org/10.1111/j.1556-4029.2009.01074.x
Chiba F, Makino Y, Motomura A, Inokuchi G, Torimitsu S, Ishii N, Sakuma A, Nagasawa S, Saitoh H, Yajima D, Hayakawa M, Odo Y, Suzuki Y, Iwase H (2013) Age estimation by multidetector CT images of the sagittal suture. Int J Legal Med 127:1005–1011. https://doi.org/10.1007/s00414-013-0883-y
Tangmose S, Jensen KE, Lynnerup N (2013) Comparative study on developmental stages of the clavicle by postmortem MRI and CT imaging. J Forensic Rad Imaging 1:102–106. https://doi.org/10.1016/j.jofri.2013.05.008
Chiba F, Makino Y, Motomura A, Inokuchi G, Torimitsu S, Ishii N, Kubo Y, Abe H, Sakuma A, Nagasawa S, Saitoh H, Yajima D, Hayakawa M, Miura M, Iwase H (2014) Age estimation by quantitative features of pubic symphysis using multidetector computed tomography. Int J Legal Med 128:667–673. https://doi.org/10.1007/s00414-014-1010-4
Monum T, Makino Y, Prasitwattanaseree S, Yajima D, Chiba F, Torimitsu S, Hoshioka Y, Yoshida M, Urabe S, Oya Y, Iwase H (2020) Age estimation from ossification of sternum and true ribs using 3D post-mortem CT images in a Japanese population. Leg Med 43:101663. https://doi.org/10.1016/j.legalmed.2019.101663
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174. https://doi.org/10.2307/2529310
McHugh ML (2012) Interrater reliability: The kappa statistic. Biochem Med 22:276–282. https://doi.org/10.11613/bm.2012.031
Obuchowski NA (2003) Receiver operating characteristic curves and their use in radiology. Radiology 229:3–8. https://doi.org/10.1148/radiol.2291010898
Metz CE (1978) Basic principles of ROC analysis. Semin Nucl Med 8:283–298. https://doi.org/10.1016/s0001-2998(78)80014-2
Youden WJ (1950) Index for rating diagnostic tests. Cancer 3:32–35. https://doi.org/10.1002/1097-0142(1950)3:1%3c32::AID-CNCR2820030106%3e3.0.CO;2-3
Sakuma A, Saitoh H, Suzuki Y, Makino Y, Inokuchi G, Hayakawa M, Yajima D, Iwase H (2013) Age estimation based on pulp cavity to tooth volume ratio using postmortem computed tomography images. J Forensic Sci 58:1531–1535. https://doi.org/10.1111/1556-4029.12175
Baccino E, Ubelaker DH, Hayek LA, Zerilli A (1999) Evaluation of seven methods of estimating age at death from mature human skeletal remains. J Forensic Sci 44:931–936
Foti B, Adalian P, Signoli M, Ardagna Y, Dutour O, Leonetti G (2001) Limits of the Lamendin method in age determination. Forensic Sci Int 122:101. https://doi.org/10.1016/s0379-0738(01)00472-8
Lovejoy CO, Meindl RS, Pryzbeck TR, Mensforth RP (1985) Chronological metamorphosis of the auricular surface of the ilium: a new method for the determination of adult skeletal age at death. Am J Phys Anthropol 68:15–28. https://doi.org/10.1002/ajpa.1330680103
Kim DK, Kim MJ, Kim YS, Oh CS, Shin DH (2012) Vertebral osteophyte of pre-modern Korean skeletons from Joseon tombs. Anat Cell Biol 45:274–281. https://doi.org/10.5115/acb.2012.45.4.274
Schmeling A, Olze A, Reisinger W, Geserick G (2005) Forensic age estimation and ethnicity. Leg Med 7:134–137. https://doi.org/10.1016/j.legalmed.2004.07.004
Author information
Authors and Affiliations
Contributions
All authors contributed to the study’s conception and design. Material preparation and data collection were performed by Fumiko Chiba, Go Inokuchi, Yumi Hoshioka, Yohsuke Makino, Suguru Torimitsu, Rutsuko Yamaguchi, and Hirotaro Iwase. The first measurement was performed by Fumiko Chiba, and the second by Mei Kono. The first draft of the manuscript was written by Fumiko Chiba, and all authors have commented on previous versions of the manuscript. All authors have read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
This study complies with the current laws of the country in which it was performed, and this study protocol was approved by the ethics committee of Chiba University.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Chiba, F., Inokuchi, G., Hoshioka, Y. et al. Age estimation by evaluation of osteophytes in thoracic and lumbar vertebrae using postmortem CT images in a modern Japanese population. Int J Legal Med 136, 261–267 (2022). https://doi.org/10.1007/s00414-021-02714-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-021-02714-9