
Abstract
The majority of homicides in the world are caused by firearms and a good understanding of gunshot wounds is important for the forensic pathologist. We have analyzed all 315 homicides by gunshots in Denmark during 1992–2016 with focus on information relevant to forensic pathologists. Of the 1417 homicides in Denmark in 1992–2016, 315 (22.2%) had gunshot trauma as the primary homicide method. During 1992–2016, there has been a significant decrease in the number of gunshot homicides overall, of homicides committed with hunting weapons, and of domestic gunshot homicides. Most victims (70.5%) and offenders (93.7% of homicides with known offenders) were males. Male victims were significantly younger than female victims. Most victims were killed with handguns (43.8%) or shotguns (41.0%). Compared to all other weapons, the victims killed with shotguns had fewer entry wounds, a higher New Injury Severity Score (NISS), and a higher proportion of contact/close-range entry wounds. The head (58.1%) and thorax (46.7%) were often injured, with injuries to the head being more common in contact/close-range entry wounds. The results show that gunshot injuries in homicides are different from suicides and accidents and clearly are affected by the homicide type, the sex of the victim, and the weapon used and that these entities are intertwined. Our findings provide an evidence-based foundation for use in death investigations and for policy development in the area of interpersonal violence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The majority of homicides in the world are caused by firearms and a good understanding of gunshot wounds is important for the forensic pathologist [1,2,3]. The homicide rate has been reduced in western countries, including Denmark, since the 1990s [4]. The latest study of gunshot homicides in Denmark was twenty years ago and featured only part of the country [5].
Careful examination of gunshot wounds and the related injuries can provide information about the type of firearm used, the direction of fire, and range of fire, which is useful for determining the cause and manner of death and provides important information to a criminal investigation [6,7,8].
In this study, we will provide data on all gunshot homicides in Denmark during 1992–2016, focusing on information relevant to forensic pathologists.
Materials and methods
From the databases of the three departments of forensic medicine in Denmark, we identified all homicides in the period 1992–2016 [4]. The average population size in Denmark was 5.41 (5.16–5.71) million people [4]. Homicides with gunshot trauma as the primary homicide method were selected for further analysis.
For each homicide, we registered general information about the homicide, the victim, and the offenders in one database, including weapon type. The homicides were grouped based on the typology of the European Homicide Monitor [9]. In a second database, we registered every injury on the skin and in organs using the Abbreviated Injury Scale (AIS) framework with localizers [10,11,12]. We added detailed information about the cause of injury, range of fire, exit wounds, and the trajectories of gunshot wounds, as seen during surgery and/or autopsy. One author (AHT) has completed the AIS training program and collected all the data. From the AIS data, we retrieved the number of gunshot wounds in each victim, the Injury Severity Score (ISS), and New Injury Severity Score (NISS). As ISS is known to underestimate the severity of penetrating injuries [13], we only report categorical data of NISS. The normal grouping of NISS is “minor (1–3),” “moderate (4–8),” “serious (9–15),” “severe (16–24),” and “critical (25–75)” [14]. To better suit the homicide victim population that has few victims with low scores, we define three NISS categories: “low (1–24),” “medium (25–44),” and “high (45–75).”
We registered the data electronically in EpiData (EpiData Association, 2010, Odense, Denmark. http://www.epidata.dk) with double entry of the AIS data. We exported the data to Stata (StataCorp. 2015, Stata Statistical Software: Release 14. College Station, TX: StataCorp LLC) and Rstudio (RStudio Team (2015), RStudio: Integrated Development for R. RStudio, Inc., Boston, MA; http://www.rstudio.com/) for statistical analysis and data visualization.
We analyzed annual data with linear regression, using lm() in R. We fitted models allowing for different regression lines using lm(number ~ year). For differences between groups (e.g., difference in mean age between female and male victims), we used permutation tests of 100,000 permutations. For each permutation, we permuted the sex and calculated the mean difference between the two groups (the null). Contingency tables were tested with chi-square test.
The study has been approved by the Danish Data Authority.
Results
Gunshot homicides
Of the 1417 homicides in Denmark in 1992–2016, 315 (22.2%) had gunshot trauma as the primary homicide method. Other homicide methods contributed to the death in 3 (1.0%) of those homicides, two with sharp force trauma and one with overrunning by a car.
Gunshot trauma contributed to death in 2 (0.2%) of the remaining 1102 homicides with a primary homicide method other than gunshot trauma, one sharp force trauma, and one housefire.
The 315 gunshot trauma homicides were committed in 277 events, distributed in 246 events with one victim and 31 events with multiple victims (69 victims total, 2–3 victims per event).
There was an overall average of 12.6 (4–19) gunshot homicides per year, but the number has shown a significant decrease over the years, with a reduction of 0.32 homicides per year (linear regression: P < 0.01, F = 12.9, R2 = 0.36) (Supplementary Figure 1).
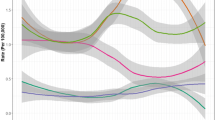
The gunshot homicide rate was 0.23 per 100,000, 0.33 per 100,000 for males, and 0.14 per 100,000 for females, with a significant annual decrease of 0.007 per year (linear regression: P < 0.001, F = 17.6, R2 = 0.43) (Fig. 1). The decrease was significant for female victims (linear regression: slope =−0.007, P < 0.001, F = 21.8, R2 = 0.49) but not for male victims (linear regression: slope =−0.006, P = 0.09, F = 3.2, R2 = 0.12).

The annual gunshot homicide rate (per 100,000) for 1992–2016
The victims and the offenders
Most victims were males (222 males (70.5%) and 93 females (29.5%)). The mean age of the victims was 35.4 years (0–87, sd=16.0) (Supplementary Figure 2) and showed male victims (mean = 33.6 years (0-81, sd=14.0)) to be significantly younger than female victims (mean = 39.7 years (1–87, sd=19.4)) (permutation test, P < 0.01).
The offender’s sex was known in 288 (91.4%) homicides, with the majority of those (270 (93.7%)) having only male offenders. In 39 (13.5%) of the homicides with known offender sex, there were multiple offenders, and none were female only. Female single offenders only killed males and 66.7% of those were intimate partner homicides. Male offenders killed intimate partners in only 24.4% of cases.
There were 237 homicides (204 homicide events) with one offender, where the age and sex of the offender were known. The mean age of these offenders was 37.1 years (14–88, sd=14.5), 37.2 years (14–88, sd=14.6) for males and 32.4 years (18–51, sd=11.0) for females (Supplementary Figure 3), with no significant difference between the sexes (permutation test, P < 0.35).
The weapons and location
Most victims were killed with handguns or shotguns (Fig. 2 and Table 1). Hunting weapons (shotguns and hunting rifles (including .22 rifles)) were used in 56.0% of homicides with female victims and in 34.7% with male victims. Hunting weapons were used in 55.5% of domestic homicides and 24.4% of homicides in relation to other criminal activity (criminal milieu and robbery). In 3.5% of homicides, two or more weapons were used.

Type of weapon related to the sex of the victim. The bars show the number of homicides for each main group
There was a significant annual reduction in the number of homicides committed with hunting weapons (linear regression: slope: −0.42, P < 0.001, F = 56.4, R2 = 0.70), but not in homicides committed with other weapons (linear regression: slope = 0.10, P = 0.26, F = 0.014, R2 = 0.06) (Fig. 3).

The annual number of gunshot homicide victims grouped by hunting weapons (shotgun and hunting rifle) and all other types of firearms
The weapon was on the scene in 116 (40.0%) of the homicides. Of those with a weapon present, only 20 (17.2%) were with a single victim having only one gunshot wound without the perpetrator committing suicide.
The majority of homicides occurred in an inside location (65.4%) (Supplementary Figure 4). Of victims killed outside, 87.4% were males and 22.3% were in a vehicle.
The gunshot wounds
There were 762 gunshot entry wounds, of which 600 (78.4%) were on the head, neck, thorax, or abdomen. Entry wounds with multiple elements from the same discharge of a shotgun were counted as only one wound. The mean number of gunshot wounds on the victims was 2.4 (1–27, median=1), 2.6 (1–27, median=2) for males and 2.0 (1–11, median=1) for females, with no significant difference of the mean between the sexes (permutation test, P < 0.07). In 51.1% of the victims, there was only one gunshot wound.
The number of gunshot wounds in victims killed with shotguns was significantly lower (mean =1.6 (1–5, median=1)) compared with all other weapons (mean = 3.0 (1–27, median = 2)) (permutation test, P < 0.001) (Table 1).
The head (58.1%) and thorax (46.7%) were the most common regions for gunshot entry wounds (Fig. 4 and Supplementary Figure 5). The extremities had gunshot entry wounds in 33.3% of gunshot homicide victims. The majority of victims had entry wounds at the front of the body (83.5%), while fewer had at the back (34.6%) (Supplementary Figure 5).

Distribution of gunshot entry wounds relative to all 315 gunshot homicides, i.e., the percentage of victims that had at least one gunshot wound in a given area. Due to their mobility, the extremities have not been separated into front and back
Of the 600 gunshot entry wounds to the head, neck, thorax, and abdomen, 50.2% had a trajectory with a posterior element, 28.5% with an anterior element, and 21.3% with no front-back element (Fig. 5). The most common trajectory for gunshot wounds seen on the victims during surgery and/or autopsy was posterior-right-inferior (9.3%) followed by posterior-left-inferior (7.7%).

Trajectories for gunshot wounds in the three planes relative to the victim’s front and back, as seen during surgery and/or autopsy. The bars show the relative distribution of trajectories in each plane for the 600 gunshot entry wounds to the head, neck, thorax, and abdomen. Due to the curvatures of the body, it is possible to have an anterior trajectory on the front of the body and vice versa. “---” means no direction in a given plane
The pathological range of fire was determined by the pathologists responsible for each autopsy. Contact range was determined by soot and gunpowder being restricted to the internal wound (and immediate vicinity in loose contact wounds), while close range was determined by soot and/or gunpowder surrounding the external wound. Absence of soot and gunpowder indicated distant range or indeterminate range depending on other findings and available case information [15]. Most of the entry wounds (68.7%) were in the range group distant range/indeterminate range, but for shotguns, contact/close range was more common (60.0%) (Table 1 and Supplementary Figure 6). In domestic homicides, about half of the entry wounds were contact/close range, while distant range/indeterminate range made up the majority of entry wounds in other homicide types (Supplementary Figure 7). A single contact gunshot wound was the only gunshot wound in 16 victims (5.0%). Contact/close-range gunshot wounds were more often to the head (84.0%/49.8%) than distant range/indeterminate range (33.5%/19.6%) (Supplementary Figures 8–10).
Typology/motives
The largest group of homicides with male victims was in the criminal milieu (33.8%) (Fig. 6 and Supplementary Figure 12 and Supplementary Table 1). All 22 victims killed in legal intervention were males. Most female victims (89.2%) were killed in domestic homicides, often by their current or previous intimate partner (71.0%).

Homicide type related to the sex of the victim. The bars show the number of homicides for each main group
There was a significant annual reduction in the number of domestic homicides (linear regression: slope −0.25, P < 0.001, F = 20.4, R2 = 0.47) but not in criminal milieu (linear regression: slope: 0.00, P = 0.99, F = 0.00, R2 = 0.00) or the group of other types of homicides (linear regression: slope: −0.07, P = 0.27, F = 1.28, R2 = 0.05) (Supplementary Figure 13).
Trauma scores and organ injuries
Table 1 shows the distribution of the New Injury Severity Score (NISS) in relation to weapon type. In NISS, 59.9% of male victims were in “high” vs. 66.7% of the female victims. Of victims killed with shotguns, 76.0% were in NISS “high” vs. 52.2% for all other victims combined (chi-sq = 18.76, df = 2, P < 0.001) (Supplementary Figure 14).
The brain and lungs (including hemo- and pneumothorax) were the organs that most often had injuries (Fig. 7).

Distribution of injuries to organ systems, relative to all 315 gunshot homicides, i.e., the percentage of victims that have at least one injury in a given organ
The most common primary cause of death was trauma to the nervous system (49.8%) followed by trauma to the cardiovascular system (36.5%). Signs of exsanguination (sparse lividity, pale organs and/or a decreased amount of blood in the vessels) were found in 66.4% of the victims.
Discussion
Globally, most homicides are caused by firearms, but with great regional differences, based on the availability of firearms in the community and the prominent homicide types [1, 3, 16,17,18,19,20,21,22,23,24,25,26]. As a general rule, countries with a high homicide rate will have a high proportion of gunshot homicides [1]. In parts of Central America with annual homicide rates of up to 80 per 100.000, gunshot homicides make up to three-quarters of homicides [1].
Only a small proportion of homicide events had multiple victims, most of those within families. Denmark has been spared the mass shooting events with double-digit homicide victims experienced in other countries during terrorist attacks and school shootings [27,28,29].
Most gunshot homicide victims and offenders were male which is similar to other countries [1, 3]. The male victims were significantly younger than the female victims, which also is part of a global trend [1, 3].
The reduction in the annual gunshot homicide rate is part of a general trend for all the four most common homicide types in Denmark [4, 11, 12]. When grouped by weapon type the reduction only affected hunting weapons. The weapon type, the homicide type, and the victim sex are intertwined, with a large proportion of domestic homicides involving female victims and hunting weapons. It is well described that reduced or impaired access to firearms in private homes leads to both fever gunshot homicides and suicides [1, 3, 16,17,18,19,20,21,22,23, 30].
Private possession of a firearm requires a permit in Denmark. The most recent drastic change in The Danish Firearms Act was in 1986 where smooth-bore shotguns were added to the list of weapons requiring a permit [31, 32]. It is unclear what the effect of this change in Danish legislation has had on the number of gunshot homicides, as it predates our study period and we do not have access to weapon ownership statistics.
Although the majority of victims were killed in an inside location, the proportion was much lower than for homicides in general [4, 12].
When trying to determine the manner of death in a deceased, the number of gunshot entry wounds, the localization of gunshot wounds, and the range of fire are important parameters to evaluate [7, 8, 33,34,35,36]. It is very rare to have multiple gunshot wounds in suicides [7, 8, 33,34,35,36,37], while about half of the homicide victims in our study had multiple gunshot wounds. Our findings in regard to the number of gunshot wounds in general in homicide victims are similar to many other studies [7, 8, 33,34,35,36,37,38]. The number of gunshot wounds in homicides is related to the type of weapon, with shotguns and hunting rifles causing fewer wounds due to the limited number of cartridges loaded at one time and their relative lethality per shot [7, 39]. Our findings on trauma scores confirm that victims shot with shotguns and hunting rifles were much more likely to be in the NISS group “high (45–75)” than those shot with other weapons (Table 1 and Supplementary Figure 14).
Most suicidal gunshot wounds are to the head or chest and rarely involve the back of the body and extremities [7, 35, 36]. While the majority of the homicide victims also had gunshot entry wounds to the head or chest, we found that one in three had gunshot entry wounds to the back of the body and one in three had gunshot entry wounds to the extremities, areas with a clear difference compared to suicides [7, 35, 36]. We did not find the same clear overrepresentation of left-sided entry wounds as Maiden et al. found in their study from Israel, where compulsory military service was stated as a contributing factor [40].
Suicidal gunshot wounds are almost exclusively fired from contact range and only very seldom from distant/intermediate range, while accidental gunshot wounds show variation in ranges, depending on whether they are self-inflicted or not [7, 16, 33, 34, 36, 41]. Two-thirds of gunshot entry wounds in our study showed no evidence of being contact or close range, which almost entirely precludes suicide during an investigation (Table 1 and Supplementary Figure 6) [7, 33, 34]. On the other hand, only very few homicide victims had a single contact range gunshot wound, the hallmark of suicidal gunshot wounds [7, 16, 33, 34, 36, 41]. Contrary to other homicide types, about half of the entry wounds in domestic homicides were contact/close range, most likely reflecting the more personal nature of these homicides and the common use of shotguns, which are less effective at long range [7, 33, 34].
As most gunshot entry wounds were to the front of the body, it is not surprising that many trajectories had a posterior element. The proportion of trajectories with a posterior element is not as high as Maiden et al. found, but that study only included gunshot homicides with injuries to the thorax and abdomen, and not neck and face [40]. Homicides feature dynamic situations with possible movement between the victim and offender, so the trajectories tend to be more varied than in the stable conditions of suicides [35, 36, 42].
One in three male gunshot homicide victims were killed in a criminal milieu compared to only one in ten for all homicides in Denmark during 1992–2016 [4]. Gunshot homicides are more common in the criminal milieu and those tend almost exclusively to have male victims [1,2,3, 9].
The organ injuries in gunshot homicides are of course linked to the localization of the gunshot wounds and to the risk of a fatal outcome. The brain and thoracic organs were most commonly injured, reflecting their critical function [38, 40]. Compared to homicides by penetrating sharp force trauma, the cranium is especially vulnerable to gunshot trauma due to the amount of transmitted energy in gunshots [12, 39].
The results show that gunshot injuries in homicides are different from suicides and accidents and clearly are affected by the homicide type, the sex of the victim, and the weapon used and that these entities are intertwined. Our findings provide an evidence-based foundation for use in death investigations and for policy development in the area of interpersonal violence.
Data Availability
Not applicable.
Code availability
Not applicable.
References
(UNODC) TUNOoDaC. Global study on homicide 2019. Vienna: The United Nations Office on Drugs and Crime (UNODC) 2019
Mc Evoy C, Hideg G (2017) Global Violent Deaths 2017: Time to Decide. Small Arms Survey Graduate Institute of International and Development Studies Geneva: small arms survey
Global Burden of Disease Injury C, Naghavi M, Marczak LB, Kutz M, Shackelford KA, Arora M et al (2018) Global mortality from firearms, 1990-2016. JAMA 320(8):792–814. https://doi.org/10.1001/jama.2018.10060
Thomsen AH, Leth PM, Hougen HP, Villesen P, Brink O (2019) Homicide in Denmark 1992-2016. Forensic Sci Int Synergy 1:275–282. https://doi.org/10.1016/j.fsisyn.2019.07.001
Hougen HP, Rogde S, Poulsen K (2000) Homicide by firearms in two Scandinavian capitals. Am J Forensic Med Pathol 21(3):281–286
Denton JS, Segovia A, Filkins JA (2006) Practical pathology of gunshot wounds. Arch Pathol Lab Med 130(9):1283–1289. https://doi.org/10.1043/1543-2165(2006)130[1283:PPOGW]2.0.CO;2
Molina DK, DiMaio V, Cave R (2013) Gunshot wounds: a review of firearm type, range, and location as pertaining to manner of death. Am J Forensic Med Pathol 34(4):366–371. https://doi.org/10.1097/PAF.0000000000000065
Cave R, DiMaio VJ, Molina DK (2014) Homicide or suicide? Gunshot wound interpretation: a Bayesian approach. Am J Forensic Med Pathol 35(2):118–123. https://doi.org/10.1097/PAF.0000000000000085
Ganpat SM, Granath S, Hagstedt J, Kivivuori J (2011) Homicide in Finland, the Netherlands and Sweden: a first study on the European homicide monitor data
Gennarelli TA, Wodzin E (2008) Association for the advancement of automotive M. Abbreviated injury scale 2005: update 2008. Barrington, Ill.: Association for the Advancement of Automative Medicine
Thomsen AH, Villesen P, Brink O, Leth PM, Hougen HP (2020) Improved medical treatment could explain a decrease in homicides with a single stab wound. Forensic Sci Med Pathol 16:415–422. https://doi.org/10.1007/s12024-020-00246-z
Thomsen AH, Hougen HP, Villesen P, Brink O, Leth PM (2020) Sharp force homicide in Denmark 1992-2016. J Forensic Sci 65(3):833–839. https://doi.org/10.1111/1556-4029.14244
Rowell SE, Barbosa RR, Diggs BS, Schreiber MA, Trauma Outcomes G, Holcomb JB et al (2011) Specific abbreviated injury scale values are responsible for the underestimation of mortality in penetrating trauma patients by the injury severity score. J Trauma 71(2 Suppl 3):S384–S388. https://doi.org/10.1097/TA.0b013e3182287c8d
Stevenson M, Segui-Gomez M, Lescohier I, Di Scala C, McDonald-Smith G (2001) An overview of the injury severity score and the new injury severity score. Inj Prev 7(1):10–13. https://doi.org/10.1136/ip.7.1.10
Knight B, Saukko PJ (2016) Knight’s forensic pathology, 4th edn. CRC Press, Taylor & Francis Group, Boca Raton
Junuzovic M, Rietz A, Jakobsson U, Midlov P, Eriksson A (2019) Firearm deaths in Sweden. Eur J Pub Health 29(2):351–358. https://doi.org/10.1093/eurpub/cky137
Santaella-Tenorio J, Cerda M, Villaveces A, Galea S (2016) What Do We know about the association between firearm legislation and firearm-related injuries? Epidemiol Rev 38(1):140–157. https://doi.org/10.1093/epirev/mxv012
Doucette ML, Crifasi CK, Frattaroli S (2019) Right-to-carry laws and firearm workplace homicides: a longitudinal analysis (1992-2017). Am J Public Health 109(12):1747–1753. https://doi.org/10.2105/AJPH.2019.305307
Lee LK, Fleegler EW, Farrell C, Avakame E, Srinivasan S, Hemenway D, Monuteaux MC (2017) Firearm laws and firearm homicides: a systematic review. JAMA Intern Med 177(1):106–119. https://doi.org/10.1001/jamainternmed.2016.7051
Jeffery A, Hulewicz B, Langlois N, Little D, Ellis P (2007) Firearm fatalities in Western Sydney 1994-2003. Forensic Sci Med Pathol 3(4):252–257. https://doi.org/10.1007/s12024-007-0035-0
Hepburn LM, Hemenway D (2004) Firearm availability and homicide: a review of the literature. Aggress Violent Behav 9(4):417–440. https://doi.org/10.1016/s1359-1789(03)00044-2
Siegel M, Ross CS, King C 3rd (2013) The relationship between gun ownership and firearm homicide rates in the United States, 1981-2010. Am J Public Health 103(11):2098–2105. https://doi.org/10.2105/AJPH.2013.301409
Siegel M, Negussie Y, Vanture S, Pleskunas J, Ross CS, King C 3rd (2014) The relationship between gun ownership and stranger and nonstranger firearm homicide rates in the United States, 1981-2010. Am J Public Health 104(10):1912–1919. https://doi.org/10.2105/AJPH.2014.302042
Ptaszynska-Sarosiek I, Filimoniuk K, Cwalina U, Niemcunowicz-Janica A (2016) Review of fatal gunshot cases in the files of the Department of Forensic Medicine in Bialystok, Poland, in the years 1964-2015. Arch Med Sadowej Kryminol 66(4):211–219. https://doi.org/10.5114/amsik.2016.68097
Chmieliauskas S, Laima S, Fomin D, Jurolaic E, Jasulaitis A, Stasiuniene J, Characiejus D, Utkus A (2019) Homicide victims and mechanisms in Lithuania from 2004 to 2016. J Forensic Legal Med 65:27–31. https://doi.org/10.1016/j.jflm.2019.04.010
Khoshnood A (2019) Holding Sweden hostage: firearm-related violence. Forensic Sci Res 4(1):88–93. https://doi.org/10.1080/20961790.2019.1570665
Sollid SJ, Rimstad R, Rehn M, Nakstad AR, Tomlinson AE, Strand T et al (2012) Oslo government district bombing and Utoya island shooting July 22, 2011: the immediate prehospital emergency medical service response. Scand J Trauma Resusc Emerg Med 20:3. https://doi.org/10.1186/1757-7241-20-3
Tresson P, Touma J, Gaudric J, Pellenc Q, Le Roux M, Pierret C et al (2017) Management of vascular trauma during the paris terrorist attack of november 13, 2015. Ann Vasc Surg 40:44–49. https://doi.org/10.1016/j.avsg.2016.09.011
Kalesan B, Lagast K, Villarreal M, Pino E, Fagan J, Galea S (2017) School shootings during 2013-2015 in the USA. Inj Prev 23(5):321–327. https://doi.org/10.1136/injuryprev-2016-042162
Gjertsen F, Leenaars A, Vollrath ME (2013) Mixed impact of firearms restrictions on fatal firearm injuries in males: a national observational study. Int J Environ Res Public Health 11(1):487–506. https://doi.org/10.3390/ijerph110100487
Thomsen JL, Albrektsen SB (1991) An investigation of the pattern of firearms fatalities before and after the introduction of new legislation in Denmark. Med Sci Law 31:162–166
Justitsministeriet. Danish Firearm Act (2019)
Molina DK, Wood LE, DiMaio VJ (2007) Shotgun wounds: a review of range and location as pertaining to manner of death. Am J Forensic Med Pathol 28(2):99–102. https://doi.org/10.1097/01.paf.0000257415.82728.d7
Molina DK, DiMaio VJ, Cave R (2013) Handgun wounds: a review of range and location as pertaining to manner of death. Am J Forensic Med Pathol 34(4):342–347. https://doi.org/10.1097/PAF.0000000000000048
Druid H (1997) Site of entrance wound and direction of bullet path in firearm fatalities as indicators of homicide versus suicide. Forensic Sci Int 88(2):147–162
Karger B, Billeb E, Koops E, Brinkmann B (2002) Autopsy features relevant for discrimination between suicidal and homicidal gunshot injuries. Int J Legal Med 116:273–278
Maghin F, Antonietti A, Farina D, Benedetti P, Verzeletti A (2019) A case of suicide by double gunshot wounds to the head: the ability to act after the first shot. Int J Legal Med 133(5):1469–1476. https://doi.org/10.1007/s00414-019-02085-2
Castro-Espicalsky TL, Costa ST, Santiago BM, Freire AR, Daruge Junior E, Prado FB et al (2020) Craniofacial injuries by firearms projectiles: an analysis of 868 deaths in the five regions of Brazil. J Forensic Legal Med 69:101888. https://doi.org/10.1016/j.jflm.2019.101888
Stefanopoulos PK, Mikros G, Pinialidis DE, Oikonomakis IN, Tsiatis NE, Janzon B (2019) Wound ballistics of military rifle bullets: An update on controversial issues and associated misconceptions. J Trauma Acute Care Surg 87(3):690–698. https://doi.org/10.1097/TA.0000000000002290
Maiden NR, Hiss J, Gips H, Hocherman G, Levin N, Kosachevsky O, Vinokurov A, Zelkowicz A, Byard RW (2016) An analysis of the characteristics of thoracic and abdominal injuries due to gunshot homicides in Israel. J Forensic Sci 61(1):87–92. https://doi.org/10.1111/1556-4029.12901
Karger B, Billeb E, Koops E (2002) Accidental firearm fatalities. Forensic and preventive implications. Int J Legal Med 116(6):350–353. https://doi.org/10.1007/s00414-002-0337-4
Suwanjutha T (1988) Direction, site and the muzzle target distance of bullet in the head and neck at close range as an indication of suicide or homicide. Forensic Sci Int 37(3):223–229. https://doi.org/10.1016/0379-0738(88)90188-0
Funding
Asser Hedegård Thomsen has received funding from Brødrene Hartmanns Fond (A26707).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
ESM 1
(DOCX 802 kb)
Rights and permissions
About this article

Cite this article
Thomsen, A.H., Leth, P.M., Hougen, H.P. et al. Gunshot homicides in Denmark 1992–2016. Int J Legal Med 135, 1507–1514 (2021). https://doi.org/10.1007/s00414-021-02548-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-021-02548-5