
Abstract
The application of computed tomography (CT) is useful for the documentation of whole-body anatomical data on routine autopsy, virtual reconstruction of skeletal structure, objective measurements, and reassessment by repetitive analyses. In addition, CT data processing facilitates volumetric and radiographic density analyses. Furthermore, a recently developed automated analysis system markedly improved the performance and accuracy of three-dimensional (3D) reconstruction. The present study investigated virtual CT morphometry of lower limb long bones, including the femur, tibia, fibula, and first metatarsus, to estimate the sex and stature using postmortem CT data of forensic autopsy cases of Japanese over 19 years of age (total n = 259, 150 males and 109 females). Bone mass volumes, lengths, and total CT attenuation values of bilateral femurs, tibias, and fibulas correlated with the stature; however, the mean CT attenuation (HU) values showed age-dependent decreases. Correlations with the stature were similar for the lengths and mass volumes of the femur, tibia, and fibula (r = 0.77–0.85) but were higher for the mass volume of the first metatarsus (r = 0.77 for right and r = 0.58 for left). In addition, the ratio of the bone volume to the length of each bone showed the most significant sex-related differences (males > females with accuracy of 75.8–98.1 %). These findings indicate the usefulness of virtual CT morphometry of individual lower limb long bones, including volumetry, to estimate the sex and stature in identification.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Forensic anthropology is essential for identification of human remains and single bones, including estimation of the sex, age, and stature, combined with DNA analyses of sex and genetic polymorphisms [1–6]. Major anthropologic indicators include anatomy of the skull and pelvis for sex discrimination [7], the lengths of the upper and lower limb long bones for stature estimation [8], and developmental [9] and degenerative bone changes for age estimation [10]. In previous studies, however, sexual dimorphism related to the size and robusticity is also detected in the lengths, diameters, widths, and circumferences of the long bones of the upper and lower extremities, which are often recovered as dismembered body parts or skeletonized single bones [2, 11–13].
In the aforementioned process of forensic victim identification, radiology is useful to detect anatomical characteristics, specific pathologies of bones, and foreign bodies including surgical materials as well as in estimating the sex, age, and stature by anthropological procedures [14]. Besides conventional radiology, postmortem computed tomography (CT) is nowadays widely used in forensic routines [15]. Major advantages of CT in victim identification include virtual reconstruction of skeletal structures independent of the status of recovered human remains, even in cases of advanced decomposition or severe destruction by fire; reconstruction using three-dimensional (3D) volume rendering software on a workstation allows soft tissue to be removed without mechanical intervention or maceration [16, 17]. In addition, the application of CT is useful for the documentation of whole-body data on routine autopsy, virtual reconstruction of skeletal structure, objective measurements, and reassessment by repetitive analyses. Several studies demonstrated the successful application of virtual bone measurement using CT for stature and sex estimation [8, 15, 18–22]. Although the long bones of the lower limbs provide the most accurate stature estimates among different populations [23–31], up-to-date Japanese population data are limited owing to difficulty in mass human material collection [8]; thus, postmortem CT data analysis may contribute to updating the data. CT data processing also facilitates volumetric and radiographic density analyses of individual bones. Furthermore, a recently developed automated analysis system markedly improved the performance and accuracy of three-dimensional (3D) reconstruction [22].
Since previous studies suggested that the diameters or widths of long bones showed greater sex-related differences than bone lengths [2, 12, 32, 33], automated bone mass volume analysis may be useful for sex estimation, demonstrating the 3D size and robusticity of bones. Also, radiographic density analysis may provide identification data related to the robusticity of bones and age of subjects in the remains without postmortem decalcification. These parameters are not available in manual measurement.
From the abovementioned observations, the aim of the present study was to investigate the efficacy of virtual CT morphometry of lower limb long bones, especially volumetry and CT density analysis, to estimate the sex and stature using an automated 3D CT data analysis system in forensic autopsy cases of Japanese over adolescence.
Materials and methods
Postmortem CT data
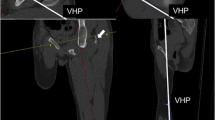
Postmortem CT scans were routinely performed immediately before autopsy within the framework of routine case work using a scanner (ECLOS; Hitachi Medical Co., Tokyo; 120 kVp, 200 mAs, 1.25 pitch factor, 2.5 × 4 mm collimation, and 16 × 1.25 mm section thickness). Serial forensic autopsy cases of Japanese of known sex, age, and stature without advanced decomposition, fracture, or destruction during a 3-year period from July 2010 to December 2013 were used: n = 259; 150 males of 19–95 (mean, 58.9; median, 52.0) years of age, and 109 females of 20–97 (mean, 59.6; median, 62.0) years of age. Demographic and anatomical data were collected from autopsy documents, including the sex, age, and stature. The cadaveric stature was measured in centimeters from the top of the head to the soles in a supine position on an autopsy table using a measuring tape [15].
CT data analysis
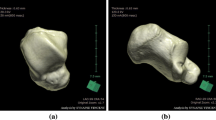
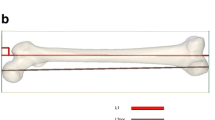
3D images of bilateral lower limb long bones, including the femur, tibia, fibula, and first metatarsus, were virtually reconstructed on the automated CT image analyzing system Volume Analyzer SYNAPSE VINCENT version 3 (FUJIFILM Medical Co., Ltd., Tokyo), identifying each bone shape based on the manufacturer’s graph-cut algorithm, which automatically estimates the CT value distribution and optimal boundary for region segmentation of the bones without users’ intervention [23, 34, 35]. The first metatarsus was chosen because it is a well-preserved foot bone in decomposed bodies and easy to identify when recovered separately [36]. Measured parameters were bone mass volume (cm3), maximum (max.) length (mm) (vertical distance between proximal and distal endpoints) (Supplementary Fig. S1), and the mean CT attenuation (HU) value and total CT attenuation (HU) value (mean HU × bone volume). The mean CT attenuation (HU) value was automatically provided for the whole extracted bone. Manual 3D measurement of the bone length was performed by three independent observers, and intraobserver and interobserver precisions were examined by applying three widely used precision estimates: the technical error of measurement (TEM), the relative technical error of measurement (rTEM), and the coefficient of reliability (R) [16]. Virtual measurements of the maximum bone length were compared with the manual measurements using skeletonized dry bone samples of the femur, tibia, and fibula (n = 7 for each) to examine the reliability. These measurements were repeated two times for each bone.
Comparison with previous stature estimation studies in Japanese
The present bone length measurements were applied to the stature estimation equations of previous studies involving Japanese for the femur and tibia by Hasegawa et al. [8], and the tibia and fibula by Yoshino et al. [33], and the results were compared.
Statistical analysis
The analyses were performed using Microsoft Excel, Statview (version 5.0, SAS Institute Inc.) and SPSS 17.0 (Statistical software package, Inc., Chicago, IL). The comparisons of measurement values between sexes were evaluated with unpaired t test analysis. The relationships between bone measurements and stature were determined by Pearson correlation analysis. The regression formulae and standard errors of estimate (SEE) were calculated by linear regression analysis for stature estimation. A p value <0.05 was considered significant. Bland-Altman method was performed to assess the agreement between the measured stature and estimated values using the above mentioned bone parameters. For sex estimation, the receiver operating characteristic (ROC) analysis was performed to estimate the cutoff points for each parameter of individual bones to compare the efficacy [12]. With the cutoff value, the accuracy of sex estimation was examined, dividing the number of cases identified by the total number of cases; cases above and below the cutoff values were estimated as males and females, respectively.
Results
Adequacy of virtual bone reconstruction
3D images of individual bones were virtually reconstructed on the automated CT image analyzing system two times in all cases. The reproducibilities of the extracted bone volume and CT density were 100.0 %. In manual measurements of bone lengths, intraobserver precisions were TEM = 0.149–1.316, rTEM < 1.5 %, and R > 0.95; interobserver precisions were TEM = 0.752–1.878, rTEM < 2.0 %, and R > 0.95 (Table 1). The differences between the virtual measurements using the volume analyzer and manual measurements of skeletonized dry bone samples of the femur, tibia, and fibula were 0–2 mm (errors within 0.005 % for each bone length).
Relationship with stature
Bone mass volumes (cm3), max. lengths (mm), and total CT values (HU) of the bilateral femurs, tibias, fibulas. and first metatarsus correlated with the stature in all cases (r = 0.42–0.85, SEE = 4.81–8.57, p < 0.0001), and also in males and females (r = 0.33–0.85, SEE = 4.17–6.64, p < 0.0001). Descriptive statistics of all bone parameters in males and females are shown in Table 2; each bone measurement and measured stature were greater in males than in females (p < 0.0001, except for the first metatarsal length with p = 0.03 and 0.04 for the left and right, respectively).
The correlations between max. bone lengths and the stature were positive and significant in all cases (r = 0.42–0.85, SEE = 4.81–8.57 cm, p < 0.0001), and also in males (r = 0.33–0.74, SEE = 4.72–6.49 cm, p < 0.0001) and females (r = 0.55–0.85, SEE = 4.17–6.64 cm, p < 0.0001); however, lower correlations with greater SEE were detected for the first metatarsus (r = 0.33–0.68, SEE = 5.79–8.57 cm, p < 0.0001) than for the other bones (r = 0.71–0.85, SEE = 4.17–5.35 cm, p < 0.0001) (Table 3 and Supplementary Fig. S2). Bone mass volumes showed correlations with the statures in all cases, and in males and females (r = 0.58–0.83, SEE = 4.93–6.15 cm, p < 0.0001); the correlation of the first metatarsus (r = 0.58–0 77, SEE = 5.70–6.15 cm, p < 0.0001) was higher than that for the length (Table 3 and Supplementary Fig. S2). Mean HU value showed an age-dependent decrease in all cases, and in males and females (r = −0.30 to −0.83, p = 0.0002 for male right femur and p < 0.0001 for the others), showing significant difference between females of <60 and >60 years of age (p < 0.0001, Fig. 1); however, total CT attenuation value (HU) correlated with the stature in all cases, and in males and females (r = 0.62–0.82, SEE = 5.02–6.04 cm, p < 0.0001) (Table 3 and Supplementary Fig. S2). There was a substantial right-left difference in max. length of the first metatarsus (r = 0.69, p < 0.0001); however, such bilateral asymmetry was not significant for the first metatarsal volume and each parameter of the other bones (r = 0.92–0.99, p < 0.0001). As above, correlations with the stature were similar for the lengths and mass volumes of the femur, tibia, and fibula but were higher for the mass volume of the first metatarsus without bilateral asymmetry, showing regression equations for stature estimation using bilateral data: 30.037 + (0.309 * max. femur length); 40.638 + (0.361 * max. tibia length); 36.392 + (0.368 * max. fibula length); and 123.607 + (2.151 * first metatarsal volume). When the sampling error was examined by random resampling and recalculation, reducing sample numbers to 100 and 50, the correlations between the stature and individual parameters (r values) did not show significant difference (<0.05).

Mean bone CT density with regard to age of the subject.F female, M male, A <60 years of age, B >60 years of age
The accuracy for stature estimation, as calculated from 95 % confidence evaluated by Bland-Altman method, was 24.2–73.9 % for individual bone max. length and was higher for the femur, tibia, and fibula (69.3–73.9 %) in all cases but lower when separately examined for males and females (52.9–67.3 %). The accuracy was lower for the first metatarsus (24.2 % for right and 29.1 % for left) in all cases, showing difference between males (24.7 % for right and 26.0 % for left) and females (55.7 % for right and 45.4 % for left). The accuracy for stature estimated from bone mass volume and total CT attenuation value was 40.1–71.9 and 29.3–69.6 %, respectively, for individual bones, and 61.3 and 60.5 % for mass volume of the right and left first metatarsus, respectively, in all cases, but lower when separately examined for males and females (42.0–54.6 %).
Comparison with previous stature estimation studies in Japanese
The accuracy of stature estimation, evaluated using the 95 % confidence interval, was 55.1–67.3 % for males and 26.4–40.2 % for females using the stature equation of Hasegawa et al. [8] for the femur and tibia; 40.3–48.6 % for males and 42.1—57.0 % for females using the stature equation of Yoshino et al. [33] for the tibia and fibula; and 60.4—66.4 % for males and 64.2—70.6 % for females using the present stature equation for the femur, tibia, and fibula (Table 4).
Sex-related difference
Sex-related difference was detected for all variables (p = 0.0018 for the max. length of the first metatarsus, and p < 0.0001 for the others; Table 5). The ratio of the bone volume to the length of each bone also showed significant sex-related difference (males > females; p < 0.0001). Cutoff values estimated for individual parameters to identify male and female bones are shown in Table 5 together with their accuracy. The accuracy to identify the sex was the highest for the ratio of bone mass volume to the max. length (75.8–91.6 % for males and 91.6–98.1 % for females), followed by total CT attenuation value (59.3–86.4 % for males and 84.0–95.1 % for females) and mass volume (75.3–85.7 % for males and 80.8–91.7 % for females), and then max. bone length (65.5–75.2 % for males and 74.8–80.2 % for females). In addition, the sex-related difference in mean CT attenuation value was detected in subjects over 60 years of age, showing the accuracy of 59.2–79.0 % for males and 80.4–96.4 % for females. When the sampling error was examined by random resampling and recalculation, reducing the sample number (75 males and 54 females), a sex-related difference was detected for all variables (p = 0.0001―0.041 for mean CT value of all bones, and p < 0.0001 for the others). The recalculated accuracy of sex discrimination did not show significant difference (<5.0 %) in all variables except for the ratio of the bone mass volume to the max. length in females and the total CT attenuation value in males (>10 %). Consistency rates of sex estimation using the combination of the parameters in males and females, respectively, were as follows: for the max. length and mass volume, 58.5 and 68.6 % for the femur, 60.0 and 69.2 % for the tibia, and 57.7 and 58.9 % for the fibula; for the mass volume and total CT attenuation value, 65.3 and 73.5 % for the femur, 52.7 and 64.5 % for the tibia, and 54.4 and 70.1 % for the fibula; and for the max. length, mass volume, and total CT attenuation value, 53.1 and 65.7 % for the femur, 66.0 and 72.0 % for the tibia, and 51.0 and 61.7 % for the fibula. Sex estimation using all bilateral long bones in males and females, respectively, was consistent in 46.7 and 59.6 % for the max. length and mass volume; in 54.7 and 66.1 % for the mass volume and total CT attenuation value; and in 37.3 and 41.3 % for the max. length, mass volume, and total CT attenuation value.
Discussion
The lower limb long bones of interest were readily reconstructed using automated CT data analysis system in the present study, as previously reported [23], and the accuracy and reproducibility of the measurements were established. All parameters of individual bone, including the length, volume, and CT density, correlated with body stature, showing sexual dimorphism, as previously reported for the bone length and diameter or width of long bones of the upper and lower extremities [2, 12, 32, 33]. These findings are consistent with the general concept of the lower limb long bone development depending on the hereditary factors and sex with ethnic and regional variations, modified by the influence of acquired factors [37], as well as the sex-related difference of cortical bone development [38], and degenerative changes in the elderly [39]. These bone statuses can be reflected in the mass volume and total CT attenuation value as indicators of the 3D size and robusticity in the remains without postmortem decalcification.
For the estimation of sex, the present study demonstrated the usefulness of volumetry and CT density of the lower limb long bones; the indicators involving these variables, including the mass volume and total CT attenuation value, were more effective for sex identification than the bone length. In addition, mean CT attenuation value of each bone also showed sex-related difference in the elderly subjects over 60 years of age. With regard to these parameters, however, individual subjects had varied sex-related characteristics, showing consistent results for all bilateral lower limb long bones in around 40 %. Among these parameters, the ratio of the mass volume to max. length was the most effective for sex estimation, showing the accuracies of 75.8–91.6 % for males and 91.6–98.1 % for females. The accuracies of these bone parameters were higher for females without bilateral asymmetry (over 90 % for the mass volume/max. length ratio) than for males (around 80–90 %), as previously reported [33, 36, 40–42], suggesting greater contribution of congenital factors to bone development during adolescence and aging-related degenerative changes in females [37, 39].
In the estimation of stature from separate single bones, the most common method is linear regression [43]. Since individual height is influenced by ethnicity and changes over time, it is recommended to use the updated regression formulae derived from the relevant population [44]. In the present study, the measurements of bilateral bones showed no significant difference for femur, tibia, and fibula, and the maximum lengths highly correlated with the stature both in males and female, as previously reported [45, 46]. However, the max. length of the first metatarsus showed lower correlations with the stature, involving substantial bilateral asymmetry. A previous study suggested a higher correlation with stature for the length of second metatarsus [47]; in the present study, however, for the first metatarsus, which is more easily identifiable when separately recovered, mass volume of the first metatarsus was a more adequate indicator for stature estimation than its max. length, suggesting the efficacy of CT volumetry. In stature estimation using individual bone parameters, the accuracies as estimated from 95 % confidence were higher (around 70 %) for mixed-sex groups than for male and female groups (around 60 %), as previously reported for foot measurements [1, 48], indicating that some skeletal variants are included both in males and females. This suggests that the accuracy of stature estimation is not improved by preliminary sex discrimination. Small intraobserver and interobserver deviations (<1.5 and <2 %, respectively) indicated the reliability of the virtual measurement, and a difference of <2 mm between the virtual and manual measurements using skeletonized dry bones is considered an acceptable range of error in forensic anthropology [49]. In postmortem measurement, a difference from antemortem statures (around 2.5-cm increase after death) should be taken in consideration [50]; however, comparisons with previous procedures for Japanese demonstrated the higher-level accuracy of the present procedure.
In conclusion, the observations of the present study described above suggest the usefulness of virtual CT morphometry of lower limb long bones to estimate the sex and stature in forensic identification, using virtual bone preparation for conventional osteometry, volumetry for estimating 3D size and robusticity, and CT value for degenerative changes and robusticity of intact bones for the elderly, especially in females, when compared with the updated ethnic population data. A rapid automated CT data analysis is practically useful to establish such population data using autopsy material.
References
Zeybek G, Ergur I, Demiroglu Z (2008) Stature and gender estimation using foot measurements. Forensic Sci Int 181:54. e1–5
Soni G, Dhall U, Chhabra S (2010) Determination of Sex from femur: discriminant analysis. J Anat Soc India 59:216–221
Duyar I, Pelin C (2003) Body height estimation based on tibia length in different stature groups. Am J Phys Anthropol 122:23–27
Aldegheri R, Agostini S (1993) A chart of anthropometric values. J Bone Joint Surg Br 75:86–88
Ozaslan A, Iscan MY, Ozaslan I, Tugcu H, Koc S (2003) Estimation of stature from body parts. Forensic Sci Int 132:40–45
Petrovečki V, Mayer D, Šlaus M, Strinović D, Škavić J (2007) Prediction of stature based on radiographic measurements of cadaver long bones: a study of the Croatian population. J Forensic Sci 52:547–552
Leopold D, Novotny V (1985) Sex determination from the skull and parts of the hip bone. Gegenbaurs Morphol Jahrb 131:277–285
Hasegawa I, Uenishi K, Fukunaga T, Kimura R, Osawa M (2009) Stature estimation formulae from radiographically determined limb bone length in a modern Japanese population. Leg Med (Tokyo) 11:260–266
Schmeling A, Olze A, Reisinger W, König M, Geserick G (2003) Statistical analysis and verification of forensic age estimation of living persons in the institute of legal medicine of the berlin university hospital charité. Leg Med (Tokyo) 5:S367–S371
Watanabe S, Terazawa K (2006) Age estimation from the degree of osteophyte formation of vertebral columns in Japanese. Leg Med (Tokyo) 8:156–160
Tatarek NE, Sciulli PW (2007) Anthropological analysis of the lower extremity determining sex, race, and stature from skeletal elements. In: Rich J, Dean DE, Powers RH (eds) In: forensic medicine of the lower extremity: human identification and trauma analysis of the thigh, Leg, and foot. The Humana Press Inc., Totowa, NJ, p 71
Saini V, Srivastava R, Rai RK, Shamal SN, Singh TB, Tripathi SK (2012) Sex estimation from the mastoid process among north indians. J Forensic Sci 57:434–439
Scheuer L (2002) Application of osteology to forensic medicine. Clin Anatomy 15:297–312
Rainio J, Lalu K, Ranta H, Penttilä A (2001) Radiology in forensic expert team operations. Leg Med (Tokyo) 3:34–43
Torimitsu S, Makino Y, Saitoh H, Sakuma A, Ishii N, Hayakawa M, Yajima D, Inokuchi G, Motomura A, Chiba F, Iwase H (2014) Stature estimation in Japanese cadevers based on pelvic measurements in three-dimensional multidetector computed tomographic images. Int J Legal Med 16:181–186
Jamaiyah H, Geeta A, Safiza MN, Khor GL, Wong NF, Kee CC, Rahmah R, Ahmad AZ, Suzana S, Chen WS, Rajaah M, Adam B (2010) Reliability, technical error of measurements and validity of length and weight measurements for children under two years old in Malaysia. Med J Malays 65:131–137
O’Donnell C, Iino M, Mansharan K, Leditscke J, Woodford N (2011) Contribution of postmortem multidetector CT scanning to identification of the deceased in a mass disaster: experience gained from the 2009 Victorian bushfires. Forensic Sci Int 205:15–28
Lorkiewicz-Muszyńska D, Kociemba W, Żaba C, Łabęcka M, Koralewska-Kordel M, Abreu-Głowacka M, Przystańska A (2013) The conclusive role of postmortem computed tomography (CT) of the skull and computer-assisted superimposition in identification of an unknown body. Int J Legal Med 127:653–660
Giurazza F, Vescovo RD, Schena E, Battisti S, Cazzato RL, Grasso FR, Silvestri S, Denaro V, Zobel BB (2012) Determination of stature from skeletal and skull measurements by CT scan evaluation. Forensic Sci Int 222:398. e1-398.e9
Torimitsu S, Makino Y, Saitoh H, Ishii N, Hayakawa M, Yajima D, Inokuchi G, Motomura A, Chiba F, Iwase H (2014) Stature estimation in Japanese cadavers using the sacral and coccygeal length measured with multidetector computed tomography. Leg Med (Tokyo) 16:14–19
Rodríguez S, González A, Simón A, Rodríguez-Calvo MS, Febrero-Bande M, Cordeiro C, Muñoz-Barús JI (2014) The use of computerized tomography in determining stature and sex from metatarsal bones. Leg Med (Tokyo) 16:252–257
Zaher JF, El-Ameen NFM, Seedhom AE (2011) Stature estimation using anthropometric measurements from computed tomography of metacarpal bones among Egyptian population. Egypt J For Sci 1:103–108
Hishmat AM, Michiue T, Sogawa N, Oritani S, Ishikawa T, Hashem MA, Maeda H (2014) Efficacy of automated three-dimensional image reconstruction of the femur from postmortem computed tomography data in morphometry for victim identification. Leg Med (Tokyo) 16:114–117
Ubelaker DH (1999) Sex, stature, and age. In: Human skeletal remains: excavation, analysis, interpretation. Third ed. Washington: Smithsonian Institution; p. 60-63
Allbrook D (1961) The estimation of stature in British and East African males: based on tibial and ulnar bone lengths. J Forensic Med 8:15–28
Yonhao W, Jiaying W, Bingcheng H (1979) Estimation of stature from long bones of Chinese male adults in south-west district. Acta Anat Sinica 10:1–6
Wilson RJ, Herrmann NP, Meadows LJ (2010) Evaluation of stature estimation from the database for forensic anthropology. J Forensic Sci 55:684–689
Taik MM, San MM (1972) Estimation of Burmese stature from long bones, Union Burma. J Life Sci 5:127–132
Dayal MR, Steyn M, Kuykendall KL (2008) Stature estimation from bones of South African whites. S Afr J Sci 104:124–128
Andou M (1923) Nihonjin (seijin) no shishikotsu no keisoku ni oite. Kokka igaku Zasshi (J Natl Med) 434:101–120 (in Japanese)
Fujii A (1960) On the relation of long bone lengths of limbs to stature. B Sch Phys Educ Juntendo Univ 3:49–61 (in Japanese with English abstract)
Yoshino M, Miyasaka S, Sato H, Seta S (1986) Estimation of stature from long bones based on somatometric analysis. Rep Natl Res Inst Police Sci Res Forensic Sci (Kashiwa) 39:201–207 (in Japanese with English abstract)
Jacob M, Avadhani R, Bindhu S (2013) Maximum femoral length and bicondylar width as a tool for sexual dimorphism. Indian J Res 2:185–186
Boykov YY, Jolly MP (2001) Interactive graph cuts for optimal boundary & region segmentation of objects in N-D images. Proc “Internation Conf Comput Vis” 1:105–112
Bello S, Andrews P (2006) The intrinsic pattern of preservation of human skeletons and its influence on the interpretation of funerary behaviours. In: Knüsel C, Gowland R (eds) The social archaeology of funerary remains. Oxbow Books, Oxford, pp 1–13
Humphrey LT (1998) Growth patterns in the modern human skeleton. Am J Phys Anthropol 105:57–72
Black TK 3rd (1978) A new method for assessing the sex of fragmentary skeletal remains: femoral shaft circumference. Am J Phys Anthropol 48:227–232
Khosla S, Amin S, Orwoll E (2008) Osteoporosis in men. Endocr Rev 29:441–464
Pandya A, Singel T, Akbari V, Dangar K, Tank K, Patel M (2011) Sexual dimorphism of maximum femoral length. Natl J Med Res 1:67–70
Vedapriya KA, Rajasree TK (2013) Determination of sex based on adult fibula. Int J Biol Med Res 4:3199–3209
Mountrakis C, Eliopoulos C, Koilias CG, Manolis SK (2010) Sex determination using metatarsal osteometrics from the Athens collection. Forensic Sci Int 200:178. e1–7
Krishan K, Kanchan T, Sharma A (2012) Multiplication factor versus regression analysis in stature estimation from hand and foot dimensions. J Forensic Leg Med 19:211–214
Singh S, Nair SK, Anjankar V, Bankwar V, Satpathy DK, Malik Y (2013) Regression equation for estimation of femur length in central Indians from inter-trochanteric crest. J Indian Acad Forensic Med 35:0971–0973
Pureepatpong N, Sangiampongsa A, Lerdpipatworakul T, Sangvichien S (2012) Stature estimation of modern Thais from long bones: a cadaveric study. Siriraj Med 64:22–25
Bhavna NS (2009) Use of lower limb measurements in reconstructing stature among shia Muslims. Internet J Biol Anthropol 2:86–97
Cordeiro C, Munoz-Baru’ JI, Wasterlain S, Cunha E, Vieira DN (2009) Predicting adult stature from metatarsal length in a Portuguese population. Forensic Sci Int 193:131. e1–131.e4
Giles E, Vallandigham PH (1991) Height estimation from foot and shoeprint length. J Forensic Sci 36:1134–1151
Stull KE, Tise ML, Ali Z, Fowler DR (2014) Accuracy and reliability of measurements obtained from computed tomography 3D volume rendered images. Forensic Sci Int 238:133–140
Trotter M, Gleser GC (1952) Estimation of stature from long bones of American whites and negroes. Am J Phys Anthropol 10:463–514
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hishmat, A.M., Michiue, T., Sogawa, N. et al. Virtual CT morphometry of lower limb long bones for estimation of the sex and stature using postmortem Japanese adult data in forensic identification. Int J Legal Med 129, 1173–1182 (2015). https://doi.org/10.1007/s00414-015-1228-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-015-1228-9