
Abstract
Methylone is a synthetic derivative of cathinone. It is sold principally on the Internet in powder form under the name «bath salts». Deaths following consumption are very rare. This report details the first case of a death in France (a 21-year-old man), following ingestion of methylone during an evening with friends. Anoxia was observed at the time of autopsy. Toxicological analyses highlighted a consumption of methylone and cannabis. However, biological analyses showed an absence of ethanol, cocaine, amphetamines, and opiate derivatives. Likewise, no medications were found. High concentrations of methylone were found in the peripheral blood (3.13 mg/L) and in the central blood (6.64 mg/L). Its presence in the gastric contents provides evidence that the substance was taken orally. The dosage of δ9-tetrahydrocannabinol (THC) suggests a recent cannabis consumption (THC 12.9 μg/L, THC-COOH 29.3 μg/L, 11-OH-THC 4.9 μg/L). This case illustrates that the consumption of methylone, which has a reputation of being less «powerful» than ecstasy, is not without its dangers.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Methylone is a synthesized compound from the cathinone family. Cathinone is an alkaloid from the leaves of the Khat plant (Catha edulis) [1]. The synthetic derivatives of cathinone form part of the new psychoactive substances (NPS) and are sold primarily on the Internet as «bath salts» or «plant food», with the label «not for human consumption» [2]. They have been known as «legal highs» and seen as a legal alternative to amphetamines. The drugs most frequently found are mephedrone and methylone in Europe [3], and α-pyrrolidinopentiophenone (PVP), 3,4-methylenedioxypyrovalerone (MDPV), and pentedrone in the USA [4]. The majority of cathinones are ingested or nasally insufflated, but because of their hydrosolubility, they can also be injected [3, 5]. Being thermolabile, they are probably not smokable. Since mid-2010, cathinones have been circulating under their proper names, but sometimes sold as ecstasy (methylenedioxymethamphetamine (MDMA)) or amphetamines [6]. In France, all cathinone derivatives have been classified as narcotics since the 27th of July 2012. This is the first time in France that an entire family of chemicals, and not just a list of compounds, has been classified as narcotics.
Methylone is a ketonic compound very close in structure to ecstasy, also called bk-MDMA. Considering the structure of methcathinone (beta-keto-methamphetamine) (Fig. 1), and specifying the presence of a methylenedioxy bridge as a prefix, it can also be called Methylene-Dioxy-MethCathinone (MDMC).

Chemical structures of methylone, MDMA, and methcathinone
Methylone, synthesized in 1996 by P. Jacob and A. Shulgin as an antidepressant and antiparkinsonian drug [7], appeared in the Netherlands at the end of 2004 as a recreational drug, in liquid form, under the name «explosion» [8]. It was one of the first substances in this family to be sold on the Internet [3, 8], labeled «room odorizer» and packaged in plastic tubes containing 5 ml of liquid, with no indication of the composition, at a price ranging from €10 to €15 ($13 to $20) [8].
Methylone is a product generally consumed in a party setting and used for its psychostimulant effects similar to those of cocaine, amphetamines, and MDMA. The immediate effects (euphoria, disinhibition, empathy, happiness, increased energy, and heightened senses) can be accompanied by short-term «secondary» effects, above all when a large dose has been taken. These effects are linked to the sympathomimetic toxicity of the product and include raised blood pressure, irregular heart beat (tachycardia, arrhythmia), mydriasis, hyperthermia with dehydration, vertigo, nausea, and convulsions [1]. Trismus, muscle cramps, and the sensation of increased strength can also be observed. Methylone is sold in powder form, either alone, or blended with caffeine, or with another compound from the same family. One dose corresponds on average to 100 to 250 mg [3].
Acute intoxication caused by methylone, other cathinones, MDMA and amphetamines, and their derivatives can lead to an irregular heart beat which can result in acute respiratory distress. We are reporting on the first case of a death in France linked to the consumption of methylone and cannabis.
Case report
A 21-year-old man took cannabis and methylone during a night out. The first symptoms described by the patient were breathing difficulties accompanied by polypnea. His friends placed him in the water of a nearby children’s paddling pool. His condition did not improve, and the emergency services were contacted. When the emergency medical service arrived, medical staff found the patient in cardiopulmonary arrest. For a period of 30 min, maximum effort was made to resuscitate the patient, but without success. A cardiac arrest was noted as well as a pupillary mydriasis, and a trismus of the masseter muscles with intubation difficulties and a general stiffness of the body.
While at the scene investigators seized the substance the victim had consumed, a powder which had been sold to him as ecstasy and had been circulating during the evening.
Autopsy
The autopsy was performed within 24 h of death. The external examination of the body did not reveal any signs of blows or injuries, and there were no external lesions. The needle puncture in the vein of the left arm was as a result of the resuscitation and was not linked to the injection of toxic substances. There were no lesions of perforation of the nasal septum. Thanatological features were livid cyanosis, conjunctival hyperemia, and subpalpebral petechiae. Rigor mortis had reached its maximum level in the lower part of the body and was disappearing from the upper part. There was no sign of putrefaction.
During the autopsy, signs of anoxia were discovered: the blood was fluid, dark and incoagulable; pulmonary congestion was observed with heavy lungs (745 g for the right lung, 685 g for the left) and pleural Tardieu ecchymoses. No macroscopic abnormalities were observed during dissection of the organs. The opening of the stomach revealed liquid contents and petechial suffusion of the mucosa. The pericardium showed petechiae on the front and rear surfaces of the left ventricle, consistent with resuscitation maneuvers.
The autopsy report concluded that death was due to respiratory distress that could have been provoked by the absorption of a toxic substance or toxic substances.
Samples were taken from different biological liquids (central blood, peripheral blood, bile, vitreous humor) as well as the gastric contents.
Toxicological analyses
Analysis methods
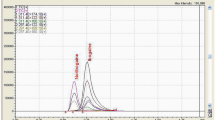
Methylone was first identified in the whole blood, urine, bile, and gastric content by a screening method of liquid chromatography coupled to a diodes array detector (HPLC/DAD). A liquid-liquid extraction was performed in a trisolvent mixture (chloroform/isopropanol/n-heptane; 60:14:26 v/v) in a base mode with prazepam as internal standard. The sample volume was 2 mL for whole blood, 1 mL for urine, 0.1 mL for bile, and 0.5 mL for homogenized gastric content. Methylone was identified with its retention time and its UV spectra. Then, a specific method was developed to quantitate methylone in the different biological liquids by liquid chromatography coupled with tandem mass spectrometry (LC/MS-MS). A deproteinization of 250 μL of sample with methanol-ZnSO4, 7H2O 0.2 M (1/4 v/v) was performed with addition of methylone-d3 as internal standard, followed by an online extraction on the Strata-X column (Phenomenex) with a mobile phase consisting of 2 mM ammonium formate. The chromatographic separation was performed on an analytical column Kinetex PFP (Phenomenex), with a gradient using a mobile phase A (0.2 % formic acid 2 mM ammonium formate buffer) and a mobile phase B (0.2 % formic acid 2 mM ammonium formate in methanol/acetonitrile 70/30 (v/v)). The detection was performed with an API 3200 Qtrap (AB Sciex), in MRM mode, with two transitions for methylone (m/z 209 → m/z 161 and m/z 209 → m/z 133) and one for methylone-d3 (m/z 212 → m/z 164). Methylone and methylone-d3 were supplied by LGC standards (Molsheim, France) as 1.0 and 0.1 mg/mL reference standard solutions, respectively. A calibration curve was carried out with drug-free whole blood spiked at six concentration points (10, 25, 50, 100, 150, and 200 μg/L). The method was validated in whole blood according to the French accreditation committee (COFRAC), document SH GTA 04: repeatability, reproducibility, accuracy, linearity, limit of quantification, and carry-over. Matrix effects were measured. The coefficients of variation (CV) of the repeatability (five times the same day) and reproducibility (five different days) assays and the inaccuracy were below 5 %. The limit of quantification was 1.5 μg/L. No matrix effects were highlighted after spiking and extraction of six different whole bloods (CV <3 %). The absence of carry-over was verified. The method was linear up to 1000 μg/L. Selectivity studies were performed with close compounds such as amphetamines (amphetamine, metamphetamine, MDMA, MDA, MDEA, MBDB), other cathinones (butylone, MDPV, MDPBP, 4-methylethcathinone, mephedrone), and methoxetamine. The cannabinoids were measured in the blood by LC/MS-MS after liquid-liquid extraction with hexane/ethyl acetate (90/10 v/v). The other narcotics (cocaine, opiates, amphetamines, and related substances) were measured in the blood by gas chromatography coupled with mass spectrometry (GC/MS) after liquid-liquid extraction with chloroform/isopropanol (90/10 v/v) and derivation. The blood and urine were screened for buprenorphine by GC/MS after liquid-liquid extraction and derivation. The measurement for the concentration of ethanol, along with other alcohols such as methanol and isopropanol, in the blood and urine was carried out by head-space gas chromatography coupled with detection by flame ionization (HS/GC/FID). Screening for medication in the blood and urine was carried out according to the trisolvent liquid-liquid extraction previously described and injected in both HPLC/DAD and GC/MS systems. The powder seized by the investigators was analyzed by HPLC/DAD.
Results
The analysis of the peripheral blood and the urine showed an absence of alcohol and medication. Screening for the narcotics generally looked for revealed an absence of opiates, cocaine and benzoylecgonine, and amphetamines (amphetamine, methamphetamine, MDMA, MDA, MBDB, and MDEA). Nevertheless, it showed the presence of cannabinoids: THC 12.7 μg/L, THC-COOH 29.3 μg/L, 11-OH-THC 4.9 μg/L.
One substance appeared in the screening plots HPLC/DAD and GC/MS, in the blood and in the urine. This substance showed the same spectral characteristics and an identical retention time to the product seized by the investigators. This product was identified as methylone and measured in different biological liquids (Table 1).
The product seized by the investigators was a shiny, white, fine-grained powder. The only organic molecule present was methylone, with a degree of purity of 83.3 %.
Discussion
Methylone is a newly synthesized product from the cathinone family which can be bought on the Internet, but also sold illegally during evenings out. It acts on monoamine systems in the same ways as MDMA: inhibition of the reuptake of noradrenaline, dopamine, and serotonin and increase of the release of these same neurotransmitters from the intra-cellular storage vesicles [9, 10]. In spite of these similarities, the subjective symptoms observed from these two drugs are not completely identical according to users’ forums: the effects of methylone are different and not as strong. According to Alexander Shulgin, it has «an almost antidepressant action, pleasant and positive, but not the unique magic of MDMA» [8]. This product is considered by users as not very dangerous. Four cases of death attributed to methylone have been reported in the USA [11–13]. All subjects were young: three men, two of them aged 23 (cases 1 and 3), and one 19-year-old (case 4), as well as a 19-year-old woman (case 2). These subjects died in spite of quick medical attention, with maximum resuscitation. Clinical findings ante-mortem include common symptoms, such as an irregular heartbeat developing quite quickly after the taking of methylone (cases 2 and 3), and a hyperthermia superior to 39.9 °C (cases 1, 2, and 3). Respiratory distress was observed (cases 1 and 4), and a stiffness of the body (case 2). Only case 3 described convulsions. In our case, it was respiratory difficulties which were foremost, accompanied by trismus, stiffness of the body, and supposed hyperthermia (placed in the water of a paddling pool).
The autoptic findings in these cases [11, 12] do not show any specific observation, with the exception of an anatomical (case 4: bicuspid aortic valve) and pathophysiological variant (case 1: moderate hypertrophy of the left ventricle and obesity) which were not linked to the occurrence of death. An anatomopathological examination carried out on case 4 highlighted congestion and a pulmonary edema with symptoms of respiratory distress [12]. These same pulmonary findings were observed at the macroscopic level in our case.
As far as the toxicological analyses are concerned (Table 2), cases 1 to 4 show a post-mortem concentration of methylone in the peripheral blood of between 0.56 and 3.3 mg/L [11, 13]. Among these four cases, we can differentiate between quicker deaths and slower deaths: one subject died a short time after receiving medical attention and taking the product (case 2). He had a concentration of 3.3 mg/L. Case 1 died 24 h after admission to the emergency department, with a post-mortem concentration of 0.84 mg/L; case 3 died quickly after receiving medical attention, but several hours after the start of symptomatology (concentration 0.56 mg/L). Case 4 died quickly after receiving medical attention, but the time span between the taking of methylone and death is not known (concentration 0.67 mg/L). In our case, death came quite quickly after consumption. As a result, there was a high blood concentration of 3.1 mg/L, similar to case 2. It should be noted that case 4, considered a rapid death after the onset of symptoms, had a sudden malaise while jogging. The physical effort could have played a role in bringing about death. In all the cases cited, there is no other substance that could have interfered in the occurrence of death. Inthree3 cases, medication was found in therapeutic concentrations in the blood: case 1 dextromethorphan; case 2 lamotrigine; case 3 midazolam, lorazepam, and fentanyl. In our case, the toxicological analyses showed a recent consumption of cannabis, but this did not play a role in bringing about death. Cases 1 and 3 show very high methylone concentrations in the gastric contents (12 and 4.5 mg/L, respectively), which provides evidence of oral consumption of the substance. It is the same for the case which we describe 57.3 mg/L.
Methylone can also play an indirect role in bringing about death. Case 5 is that of a young woman who was found drowned after voluntarily going for a swim following consumption of a substance [14]. The autopsy concluded that the cause of death was drowning. The high methylone concentration in the blood (3.4 mg/L, peripheral and central blood) enabled the authors to consider that intoxication by methylone had led to an inability to reach the shore. The toxicological analyses also showed consumption of cannabis (THC 3.2 μg/L, THC-COOH 110 μg/L). A driver of a motor vehicle who had an accident following a driving error (case 6), died of his injuries [15]. He had a concentration of methylone of 0.73 mg/L and of MDPV of 0.06 mg/L in the central blood [15] and had consumed cannabis (THC 15 μg/L, THC-COOH 118 μg/L). Similarly, methylone played a role in bringing about the death of a 16-year-old boy (case 7), who had a history of heart disease and asthma [16]. The concentration of methylone was lower: 0.27 mg/L [16].
On the other hand, there are cases of deaths which have been classed as having a non-toxic cause despite the subjects having consumed methylone [13]. Concentrations in the central blood varied between 0.06 and 1.1 mg/L (Table 2) for two deaths caused by a firearm (38-year-old man and 35-year-old woman) and one death by drowning (21-year-old woman). The concentrations in the peripheral blood were not indicated.
In the cases published, it can be observed that the concentrations of methylone in the central blood are superior or equal to those in the peripheral blood, with a ratio varying between 1.0 and 1.2 (n = 4) [11, 13, 14]. Our case shows a higher ratio (2.1), suggesting that phenomena for redistribution could exist, as described for MDMA [17] .
Conclusion
We describe the first case of a death in France following ingestion of methylone. Death occurred with respiratory difficulties at the forefront, despite rapid medical attention. During autopsy, indirect signs of anoxia were noted. The concentration of methylone in the peripheral blood was very high and quite similar to that in another case when death occurred rapidly after ingestion. Methylone is considered as being responsible for the death. As seen in the literature, there seems to be an overlap between the post-mortem blood concentrations of those whose death was attributed to the consumption of methylone (0.56 to 3.3 mg/L) and those whose death was not of toxic origin (0.06 to 1.1 mg/L). However, the comparison is made difficult by the absence of blood concentrations in the peripheral blood for the deaths of non-toxic origin. The concentrations in the central blood superior to those in the peripheral blood (ratio from 1.0 to 1.2 in the literature and 2.1 in our case), suggest the existence of phenomena for post-mortem redistribution.
References
Tekulve K, Alexander A, Tormoehlen L (2014) Seizures associated with synthetic cathinone exposures in the pediatric population. Pediatr Neurol 51(1):67–70
Prosser JM, Nelson LS (2012) The toxicology of bath salts: a review of synthetic cathinones. J Med Toxicol Off J Am Coll Med Toxicol 8(1):33–42
López-Arnau R, Martínez-Clemente J, Abad S, Pubill D, Camarasa J, Escubedo E (2014) Repeated doses of methylone, a new drug of abuse, induce changes in serotonin and dopamine systems in the mouse. Psychopharmacology (Berl) 231(16):3119–29
Uralets V, Rana S, Morgan S, Ross W (2014) Testing for designer stimulants: metabolic profiles of 16 synthetic cathinones excreted free in human urine. J Anal Toxicol 38(5):233–41
Baumann MH, Partilla JS, Lehner KR (2013) Psychoactive “bath salts”: not so soothing. Eur J Pharmacol 698(1–3):1–5
Warrick BJ, Wilson J, Hedge M, Freeman S, Leonard K, Aaron C (2012) Lethal serotonin syndrome after methylone and butylone ingestion. J Med Toxicol Off J Am Coll Med Toxicol 8(1):65–8
Jacob P, Shulgin A (1996) Novel n-substituted-2-amino-3’,4’-methylene-dioxypropiophenones - WO1996039133A1
Bossong MG, Van Dijk JP, Niesink RJM (2005) Methylone and mCPP, two new drugs of abuse? Addict Biol 10(4):321–3
Sogawa C, Sogawa N, Ohyama K, Kikura-Hanajiri R, Goda Y, Sora I et al (2011) Methylone and monoamine transporters: correlation with toxicity. Curr Neuropharmacol 9(1):58–62
Nagai F, Nonaka R, Satoh Hisashi Kamimura K (2007) The effects of non-medically used psychoactive drugs on monoamine neurotransmission in rat brain. Eur J Pharmacol 559(2-3):132–7
Pearson JM, Hargraves TL, Hair LS, Massucci CJ, Frazee CC, Garg U et al (2012) Three fatal intoxications due to methylone. J Anal Toxicol 36(6):444–51
Carbone PN, Carbone DL, Carstairs SD, Luzi SA (2013) Sudden cardiac death associated with methylone use. Am J Forensic Med Pathol 34(1):26–8
Cawrse BM, Levine B, Jufer RA, Fowler DR, Vorce SP, Dickson AJ et al (2012) Distribution of methylone in four postmortem cases. J Anal Toxicol 36(6):434–9
McIntyre IM, Hamm CE, Aldridge L, Nelson CL (2013) Acute methylone intoxication in an accidental drowning – a case report. Forensic Sci Int 231(1-3):e1–3
Marinetti LJ, Antonides HM (2013) Analysis of synthetic cathinones commonly found in bath salts in human performance and postmortem toxicology: method development, drug distribution and interpretation of results. J Anal Toxicol 37(3):135–46
Kovács K, Tóth AR, Kereszty EM (2012) A new designer drug: methylone related death. Orv Hetil 153(7):271–6
Baselt RC (2008) Disposition of toxic drugs and chemicals in man. Édition : 8. Foster City, Ca: Biomedical Publications
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Barrios, L., Grison-Hernando, H., Boels, D. et al. Death following ingestion of methylone. Int J Legal Med 130, 381–385 (2016). https://doi.org/10.1007/s00414-015-1212-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00414-015-1212-4