
Abstract
Major depressive disorder (MDD) and obesity are two serious public health problems. Although there have been some research on both, there have few studies on differences in obesity among MDD patients at different ages of onset. The study aims to evaluate the prevalence and factors associated with obesity in MDD patients at different ages of onset. This study totally recruited 1718 first-episode drug-naive MDD patients aged from 18 to 60 years. All subjects were divided into two subgroups: early adulthood onset (EAO, 18–45 years) and mid-adulthood onset (MAO, 45–60 years). Clinical symptoms of patients were evaluated using the 17-item Hamilton Depression Rating Scale (HAMD-17), Hamilton Anxiety Scale (HAMA), and Positive and Negative Syndrome Scale (PANSS) positive subscale. Baseline parameters including body mass index (BMI), blood pressure, and hematological biochemical parameters were assessed to investigate the association between these parameters and weight gain risk. The percentages of overweight and obesity patients with MDD in EAO group were 54.4% and 4.1%, respectively, and the percentages of overweight and obesity patients with MDD in MAO group were 60.4% and 2.8%, respectively. MDD patients in the MAO group had a longer duration of illness and higher scores in HAMD, HAMA, and PANSS positive subscale. They also had higher levels of thyroid stimulating hormone (TSH), anti-thyroglobulin (TgAb), fasting blood glucose (FBG), total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), systolic and diastolic blood pressures (SBP and DBP) levels. BMI did not differ significantly between the two groups. In the EAO group, statistically significant differences were found among normal weight, overweight and obese group in duration of illness, age of onset, TSH, TgAb, thyroid peroxidase antibody (TPOAb), free thyroxine (FT4), TC, triglycerides (TG), SBP and DBP. The TSH, TgTb and SBP were identified as risk factors for weight gain. In the MAO group, statistically significant differences were found among normal weight, overweight and obese group in TSH and FBG. The two indicators were identified as risk factors for weight gain. There were no significant differences in the weight of MDD patients at different ages of onset, while the factors that could potentially lead to obesity did show some differences.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Major depressive disorder (MDD) and obesity are two major public health problems that affect large numbers of people worldwide. For now, twelve-month prevalence of MDD is approximately 7% [1,2,3], and WHO estimates that by 2030, MDD will be the leading global disease and one of the leading causes of disability worldwide [4]. Meanwhile, in 2016, more than 1.9 billion adults worldwide were estimated to be overweight, and more than 650 million of them were obese [5]. It is worth noting that these two major public health problems tend to co-occur within individuals.
Several studies have shown that MDD and obesity have a bidirectional relationship [6]. They are interconnected through a vicious, mutually reinforcing cycle of adverse physiological adaptations [6, 7]. Studies have shown that obesity increases the risk of developing MDD, and in turn MDD further increases the likelihood of obesity. A recent US study reported that 43% patients with MDD were overweight or obese [8]. A meta-analysis involved 17,894 Chinese children and adolescents found that depression was more prevalent in subjects who were overweight or obese [9]. Adolescents with obesity reported 1.3 times higher risk of depression, and adolescents with depression had a 70% increased risk of being obese [10]. Different depression subtypes have different risk of being obese. A meta-analysis of observational studies reported that atypical depression is significantly associated with elevated BMI compared with melancholic depression [11].
Metabolic status is a major influencing factor in the interconnection of MDD and obesity. In an analysis of 30,337 obese individuals, the risk of depression was only slightly increased in obese individuals with good metabolic status compared to non-obese individuals, but the risk of depression was greater when obese individuals were associated with adverse metabolic conditions (e.g., hypertension, dyslipidemia, high C-reactive protein, or insulin resistance) [12]. However, the mechanisms underlying the association between depression and obesity remain controversial. A meta-analysis showed that one potential factor contributing to obesity in MDD was the use of antipsychotic drugs, but this still remains controversial [13, 14]. In a study of 1000 depressed patients, we found that only the use of mirtazapine was associated with weight gain through more than two years of follow-up [15]. However, in a meta-analysis of weight changes due to antidepressant use, Serretti and mandelli [14] suggested that although most antidepressants affect patients' weight, this effect is transient and negligible in the short term. In a large study involving 2545 subjects, depressive states, but not antidepressants, were found to be responsible for weight gain at 2-year follow-up [16]. Some common biological pathways exist in depression and obesity, such as genetics, alterations in systems involved in homeostatic adjustments and brain circuitries integrating homeostatic, mood regulatory responses and the gut microbiota [14, 17].
Among patients with MDD, differences in the age of first onset may have a differential impact on depressive symptoms. Adolescents with depression have a higher incidence of physical illness and an elevated risk of suicide during their lifetime [18]. In addition, the earlier age of onset of depression, the more severe their depressive symptoms, the more severe their cognitive impairment, and the less effective their antidepressant treatment [19]. Previous studies have found different brain imaging in patients with depression at different ages of onset. A meta-analysis showed that patients with early-onset depression had larger lateral ventricles and smaller amygdala and hippocampal volumes compared to healthy controls, unlike patients with late-onset depression [20]. Another study found that after the first episode of major depression, gray matter volumes in brain regions associated with mood regulation were reduced in drug-naïve adult patients, while gray matter volume changes differed between patients with early-onset and late-onset depression [21]. In a retrospective review, the early-onset late-lie depression had higher body mass index, greater risk of affective disorders in the family history, and poor treatment response [22]. It has been proposed that early-onset depression and late-onset depression differ phenomenologically. Low spirits and feelings of worthlessness were more frequently found in early-onset depression, they were sufficient discriminators to distinguish elderly subjects with early-onset depression and late-onset depression [23]. There is a large body of research on the differences in the age of depression onset, but no research on differences in body weight of depressed patients by age of onset, and even less research on factors associated with obesity in depressed patients by age of onset.
In light of these findings, the purpose of this study was to assess weight differences in MDD across age of onset and to explore factors associated with obesity in MDD. To avoid the effects of antidepressants on the weight of MDD patients, the subjects recruited for this study were untreated patients with first-episode MDD.
Methods
Subjects
This cross-sectional study was conducted at the psychiatric outpatient clinic of the First Hospital of Shanxi Medical University. A total of 1718 patients who met the diagnostic criteria for MDD were enrolled between 2015 and 2017. All subjects met the following inclusion criteria: (1) experienced an acute episode of MDD, as verified by two research psychiatrists based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV); (2) not receiving any antidepressant or other antipsychotic medication prior to the assessment; (3) the 17-item Hamilton Depression Rating Scale (HAMD, 17-item) score > = 24; (4) age between 18 and 60 years; (5) Han Chinese; and (6) able to understand the instructions of the clinical psychiatrist. Exclusion criteria included: (1) having a serious physical illness prior to study participation (see supplemental material); (2) having a history of drug or alcohol abuse (or dependence), as determined by self-reported substance use and medical records; (3) being pregnant or breastfeeding; and (4) being unwilling to participate.
This study was reviewed and approved by the Institutional Review Board of the First Hospital of Shanxi Medical University. All participants or their guardians signed a written informed consent form and had the right to decide whether to withdraw at any time if they wished.
Sociodemographic data and clinical measures
All patients were interviewed by two independent psychiatrists via the Structured Clinical Interview for DSM-IV (SCID-I/P). A self-designed questionnaire including age, gender, weight, marital status, age of depression onset, duration of illness, and education level was used to collect demographic information from the patients. In addition, based on previous studies and clinical experience, patients were divided into two groups in this study: early-adulthood onset (EAO, 18–45 years) and mid-adulthood onset (MAO, 45–60 years) [24]. The HAMD-17 was used to assess the severity of depressive symptoms. The Hamilton Anxiety Rating Scale (HAMA) was used to assess the severity of anxiety symptoms. The Positive and Negative Syndrome Scale (PANSS) positive subscale was used to assess psychotic symptoms. Two psychiatrists who were blinded to the clinical status of the participants attended training sessions on how to administer the HAMD-17, HAMA, and PANSS prior to the start of the study. After repeated assessments, the inter-rater correlation coefficients of the HAMD, HAMA, and PANSS scores were all greater than 0.8.
Physical and biochemical parameter measurements
Body mass index (BMI) was calculated from height and weight measurements, and the formula was weight (kg) divided by the square of height (m2). According to the diagnostic criteria of the Chinese Obesity Working Group, all patients were divided into normal weight group (BMI < 24 kg/m2), and overweight group (24 kg/m2 ≤ BMI < 28 kg/m2), and obese group (BMI ≥ 28 kg/m2) [25, 26]. After resting for at least 15 min, systolic and diastolic blood pressures (SBP and DBP) were measured on the left arm using an Omron digital sphygmomanometer. The final blood pressure value was the average of the two measurements.
Blood samples were collected from all patients after 12 h of fasting. Then all blood samples were sent to the laboratory center of the hospital within two hours after collection, and were assayed for the following parameter: total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), fasting blood glucose (FBG), thyroid stimulating hormone (TSH), free triiodothyronine (FT3), free thyroxine (FT4), anti-thyroglobulin (TgAb) and thyroid peroxidase antibody (TPOAb).
Statistical analysis
Data were statistically analyzed using the Statistical Package for Social Sciences (SPSS) version 22.0. The statistical comparison was performed using Mann–Whitney U test for continuous variables and chi-square (χ2) test for categorical variables. Kruskal–Wallis H test was used for outcome analyses as it is a rank-based non-parametric test that can be used to determine if there are statistically significant differences between two or more groups (normal weight group, overweight group, obese group) of an independent variable on dependent variables that are continuous, but not normally distributed. For those analyses in which the overall test was significant, pairwise comparisons were completed using the Mann–Whitney U test controlling for Type I error across tests with the Bonferroni adjustment. The variables for which p value was less than 0.5 were selected for the ordinal multivariate logistic regression analysis. Sex, marriage, and years of education were used as the most basic characteristics, and these variables may have an effect on clinical symptoms, and body weight. These factors were used as covariates with the aim of controlling for their potential impact on the observed association of Thyroid function, lipids, blood pressure and fasting blood glucose with obesity. P-values were two-tailed for all reported results, and the significance level was set at P < 0.05.
Results
Basic characteristics of patients grouped by age of MDD onset
As shown in Table 1, compared with the MAO group, the EAO group had higher proportion of males, higher level of education, lower rate of marriage, and shorter duration of depression (all P < 0.001).
The MAO group had significantly higher scores on the HAMD-17, HAMA, and PANSS positive subscale scores compared with the EAO group9 (all P < 0.05) (see Table 1).
The proportions of overweight and obese patients were 54.4% and 4.1%, respectively, in the EAO group, and 60.4% and 2.8%, respectively, in the MAO group. There was no significant difference in the proportion of normal weight, overweight and obese between the two groups, and no significant difference in BMI between the two groups (see Table 1).
Furthermore, there were significant differences in TSH, TgAb, FT3, FBG, TC, HDL-C, LDL-C, SBP and DBP between the two groups (all P < 0.05). Compared with the MAO group, the EAO group had lower values for TSH, TgAb, FBG, TC, LDL-C, SBP and DBP, but higher values for FT3 and HDL-C (all P < 0.05) (see Table 1).
Comparison of basic characteristics of different weigh groups within the EAO group
We compared clinical, physical and biochemical parameters between normal weight, overweight and obese (see Table 2). The Kruskal–Wallis H test found statistically significant difference in duration of illness (P = 0.040), age of onset (P = 0.012), TSH (P < 0.001), TgAb (P = 0.042), TPOAb (P = 0.003), FT4 (P = 0.031), TC (P = 0.008), TG (P = 0.021), SBP (P < 0.001) and DBP (P < 0.001) between the group of normal weight and the other two groups.
The Mann–Whitney U test found that the overweight group had a longer duration of illness (Bonferroni corrected P = 0.045), older age of onset (Bonferroni corrected P = 0.009) than the normal weight group. Besides, the overweight group had higher level of TSH (Bonferroni corrected P < 0.001), TgAb (Bonferroni corrected P = 0.036), TPOAb (Bonferroni corrected P = 0.003), TG (Bonferroni corrected P = 0.017), DBP (Bonferroni corrected P < 0.001) and SBP (Bonferroni corrected P < 0.001) than the normal weight group. The obese group had higher levels of TC (Bonferroni corrected P = 0.009) and DBP (Bonferroni corrected P = 0.023) than the normal weight group. The levels of TSH, FT4 and SBP in the obese group were higher than the overweight group (Bonferroni corrected PTSH = 0.012, PFT4 = 0.046, PSBP = 0.014) and the normal weight group (Bonferroni corrected PTSH < 0.001, PFT4 = 0.025, PSBP < 0.001).
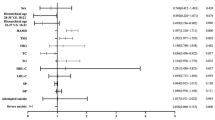
Using logistic regression, obesity in EAO group was associated with TSH (95% Cl: 1.083–1.250, P < 0.001, and OR = 1.164), TgAb (95% Cl: 0.999–1.00, P = 0.025, and OR = 0.999) and SBP (95% Cl: 1.008–1.048, P = 0.006, and OR = 1.028).
Comparison of basic characteristics of different weigh groups within the MAO group
A Kruskal–Wallis H test showed that there was a statistically significant difference in TSH and FBG between the different weight groups (P < 0.001) (see Table 3). Both TSH and FBG were significantly higher for the overweight group than for the normal weight group (Bonferroni corrected P < 0.001).
Using logistic regression, obesity in MAO group was associated with TSH (95% Cl: 1.072–1.347, P = 0.002, and OR = 1.202), and FBG (95% Cl: 1.028–1.953, P = 0.033, and OR = 1.417).
Discussion
In our study, both the early-adulthood onset MDD population and the mid-adulthood onset MDD population had higher numbers of overweight than normal weight and obese, respectively 54.4% and 60.4%. Nevertheless, we did not find difference in BMI between patients with depression at different ages of onset. This finding may differ from some previous studies. A previous study on depression and emotional eating found that younger depressed patients had a significant increase in BMI and waist circumference after 7 years of follow-up, while no such changes were found in older depressed patients[27]. This discrepancy may be due to the fact that our study included first-episode patients with depression, most of whom had a disease duration of less than 1 year, and no long-term effects of depression on body weight could be seen. In addition, the course of disease in mid-adulthood onset MDD group was longer than that in early adulthood onset depression group, and the duration of untreated disease could seriously affect the prognosis of patients [28,29,30], but it did not affect the body weight of patients.
There were differences in blood pressure and hematological biochemical parameters between the EAO and MAO groups. Blood pressure, thyroid stimulating hormone, lipids and fasting blood glucose were high in the MAO group. Blood pressure, lipids and fasting blood glucose are all indicators of metabolic syndrome. In a previous meta-analysis, it was found that the risk of metabolic syndrome in patients with depression decreased with age, with a higher risk of metabolic syndrome below 50 years of age as a cutoff [31]. Another study of elderly depressed patients in Iran found that metabolic syndrome did not increase with age [32]. The results of current studies on depressed patients of different ages with comorbid metabolic syndrome are inconsistent. Our study found high metabolic markers in patients with mid-adulthood onset MDD, which may be related to thyroid stimulating hormone. Studies have shown that thyroid stimulating hormone is a risk factor for various metabolic indicators. High level of thyroid stimulating hormone can directly affect lipid metabolism by binding to TSH receptors, and can also promote cholesterol synthesis and inhibit cholesterol removal [33]. Hepatic endoplasmic reticulum stress mediated by high levels of TSH also plays an important role in dyslipidemia and impaired glucose metabolism [34, 35], and TSH abnormalities can lead to thyroid dysfunction, which in turn can lead to hypertension, hyperglycemia, and dyslipidemia [36, 37]. Kim found that subclinical hypothyroidism increased the risk of metabolic syndrome about 7 times in adult depressive patients in Korea [38]. A number of studies have shown that thyroid stimulating hormone increases gradually with age [39,40,41]. Therefore, we hypothesized that the increase in fasting blood glucose, lipids, and blood pressure in patients with mid-adulthood onset MDD in the present study might be due to abnormalities in thyroid stimulating hormone.
In the present study, mid-adulthood onset depression patients had more severe depressive symptoms, anxiety symptoms, and psychotic symptoms than early adulthood onset depression patients. However, previous studies have shown that patients with early onset depression have more severe depressive symptoms and are more likely to have concomitant anxiety disorders [19, 42, 43]. In another large study by Park et al. [44], the authors did not find significant differences in HAMD and HAMA scores between MDD patients of different ages of onset. Nevertheless, we cannot ignore the role of thyroid stimulating hormone. High levels of thyroid stimulating hormone also play an important role in the clinical symptoms of depressed patients. A previous study has suggested that severe anxiety, depression, and psychotic symptoms, as well as old age and obesity, may be associated with elevated TSH levels [45,46,47]. A large study found a higher likelihood of depression in patients with subclinical hypothyroidism, and a subanalysis found that the geriatric group had a greater incidence of depression [48]. There are many common biological mechanisms between depression and subclinical hypothyroidism, such as disturbances in the hypothalamic-pituitary-adrenal axis, altered levels of hormones including growth inhibitors and 5-hydroxytryptophan [49]. There is a correlation between thyroid stimulating hormone level and psychotic symptoms. Schizophrenia is independently associated with hypothyroidism [50,51,52]. Liu found that serum thyroid stimulating hormone levels were independently associated with psychotic symptoms in patients with MDD [53]. In addition, depressed patients with co-morbid anxiety have higher thyroid stimulating hormone levels [54, 55]. Most of the current evidence on the relationship between thyroid stimulating hormone and psychotic and anxiety symptoms comes from observational cross-sectional studies. The underlying mechanisms remain largely unexplored.
A positive correlation between TSH and BMI was found in both the EAO and MAO groups. Many previous studies have found a significant relationship between BMI and thyroid stimulating hormone [37, 44, 56,57,58,59,60,61,62]. Previous studies have shown that subclinical hypothyroidism can cause changes in basal metabolic rate, leading to an increase in BMI, and that obesity can also affect thyroid function through mechanisms such as lipotoxicity and changes in adipokine and inflammatory cytokine secretion [63,64,65,66,67,68,69]. Although it has been demonstrated that thyrotropin is associated with basal metabolism and that elevated thyrotropin leads to increased body weight, lipids, blood glucose and blood pressure. However, there are differences in thyrotropin hormones and no differences in body weight in MDD patients of different ages of onset. We hypothesize that the influence of thyrotropin on body weight may decrease with age, and further studies are needed to investigate the exact mechanism.
Interestingly, a positive correlation between TgAb, SBP and weight can be found in the EAO group, while FBG was positively correlated with weight in the MAO group. Blood glucose and blood pressure as indicators of metabolic syndrome have been shown to be strongly associated with obesity [70,71,72,73,74]. In a large-scale study, a significant positive correlation was found between blood pressure and body weight in healthy people under 50 years of age, while this correlation was weaker in people over 50 years of age [75]. The results of this study are similar to our findings. However, there are still few studies on the relationship between body weight and blood glucose and blood pressure in different age groups, and even fewer in depressed patients. In addition, previous studies have found a positive correlation between anti-thyroglobulin and body weight, while the mechanism remains unclear [76].
Both men and women were at risk of obesity and depression bi-directionally. Depression can activate the hypothalamic-pituitary-adrenal axis and lead to accumulation of visceral fat through increasing the secretion of corticotrophin-releasing hormone, adrenocorticotropic hormone, and cortisol [77]. A previous study found a modest overlap of glucocorticoid receptor gene, the corticotrophin releasing hormone receptor gene, the serotonin 2A and 2C receptor genes, and the dopamine receptor D4 gene as the genetic risk factors that increase liability to both depression and obesity [7]. Depression and thyroid stimulating hormone interact with each other through the hypothalamic-pituitary-adrenal axis, growth inhibitors, and 5-hydroxytryptophan. In addition, TSH affects glycolipid metabolism by binding to thyroid stimulating hormone receptors, interfering with cholesterol synthesis and clearance, and mediating hepatic endoplasmic reticulum stress. In turn, changes in lipotoxicity, adipokine secretion, affect thyroid function. Therefore, there is an interaction between obesity, metabolism and TSH in depressed patients, and attention should be paid to all health indicators in depressed patients in order to inhibit the vicious circle. The mechanism of the influence of age of depression onset in this cycle needs to be further explored.
The present study still had some limitations. First, due to the cross-sectional design of this study, it is impossible to establish any causality between body weight and thyroid function, blood pressure and glucose. Second, because this study did not include healthy controls, the effect of depression on body weight cannot be clearly illustrated. Third, since this was a cross-sectional study, we cannot exclude the possibility that some of our patient subjects who verified as having depressive episode could be later diagnosed as with bipolar disorder. Finally, this study included patients with first-episode drug-naïve depression, which has some limitations in terms of clinical generalization. Future studies applying the research method of follow-up studies will further clarify the effects of different ages of onset on the body weight of MDD patients and the risk factors leading to obesity in MDD patients.
In conclusion, the age of onset of MDD does not cause differences in body weight, however, there are differences in the risk factors leading to obesity in patients with MDD at different ages of onset. Thyroid stimulating hormone abnormalities were a risk factor for obesity in all MDD patients. Fasting blood glucose abnormalities were risk factors for obesity in MDD patients with mid-adulthood onset, while anti-thyroglobulin and systolic blood pressures abnormalities were risk factors for obesity in MDD patients with early-adulthood onset.
Availability of data
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable requests.
References
Chand SP, Arif H (2023) Depression. In: StatPearls. StatPearls Publishing, St. Petersburg
Levinstein MR, Samuels BA (2014) Mechanisms underlying the antidepressant response and treatment resistance. Front Behav Neurosci 8:208. https://doi.org/10.3389/fnbeh.2014.00208
Kessler RC, Berglund P, Demler O et al (2003) The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA 289(23):3095–3105. https://doi.org/10.1001/jama.289.23.3095
Lépine JP, Briley M (2011) The increasing burden of depression. Neuropsychiatr Dis Treat 7(Suppl 1):3–7. https://doi.org/10.2147/NDT.S19617
World Health Organization (2021) Obesity and overweight. Newsroom. [Updated June 2021]. http://www.who.int/mediacentre/factsheets/fs311/en/
Mannan M, Mamun A, Doi S, Clavarino A (2016) Prospective associations between depression and obesity for adolescent males and females—a systematic review and meta-analysis of longitudinal studies. PLoS ONE 11(6):e0157240. https://doi.org/10.1371/journal.pone.0157240
Mannan M, Mamun A, Doi S, Clavarino A (2016) Is there a bi-directional relationship between depression and obesity among adult men and women? Systematic review and bias-adjusted meta analysis. Asian J Psychiatr 21:51–66. https://doi.org/10.1016/j.ajp.2015.12.008
Pratt LA, Brody DJ (2014) Depression and obesity in the U.S. adult household population, 2005–2010. NCHS Data Brief 167:1–8
Wang S, Sun Q, Zhai L et al (2019) The prevalence of depression and anxiety symptoms among overweight/obese and non-overweight/non-obese children/adolescents in china: a systematic review and meta-analysis. Int J Environ Res Public Health 16(3):340. https://doi.org/10.3390/ijerph16030340
Chao AM, Wadden TA, Berkowitz RI (2019) Obesity in adolescents with psychiatric disorders. Curr Psychiatry Rep 21(1):3. https://doi.org/10.1007/s11920-019-0990-7
Silva DA, Coutinho EDSF, Ferriani LO et al (2020) Depression subtypes and obesity in adults: a systematic review and meta-analysis. Obes Rev 21(3):e12966. https://doi.org/10.1111/obr.12966
Jokela M, Hamer M, Singh-Manoux A et al (2014) Association of metabolically healthy obesity with depressive symptoms: pooled analysis of eight studies. Mol Psychiatry 19(8):910–914. https://doi.org/10.1038/mp.2013.162
Milaneschi Y, Simmons WK, van Rossum EFC et al (2019) Depression and obesity: evidence of shared biological mechanisms. Mol Psychiatry 24(1):18–33. https://doi.org/10.1038/s41380-018-0017-5
Serretti A, Mandelli L (2010) Antidepressants and body weight: a comprehensive review and meta-analysis. J Clin Psychiatry 71(10):1259–1272. https://doi.org/10.4088/JCP.09r05346blu
Bet PM, Hugtenburg JG, Penninx BW, Hoogendijk WJ (2013) Side effects of antidepressants during long-term use in a naturalistic setting. Eur Neuropsychopharmacol 23(11):1443–1451. https://doi.org/10.1016/j.euroneuro.2013.05.001
Gibson-Smith D, Bot M, Milaneschi Y et al (2016) Major depressive disorder, antidepressant use, and subsequent 2-year weight change patterns in the Netherlands Study of Depression and Anxiety. J Clin Psychiatry 77(2):e144–e151. https://doi.org/10.4088/JCP.14m09658
Schachter J, Martel J, Lin CS et al (2018) Effects of obesity on depression: a role for inflammation and the gut microbiota. Brain Behav Immun 69:1–8. https://doi.org/10.1016/j.bbi.2017.08.026
Leone M, Kuja-Halkola R, Leval A et al (2021) Association of youth depression with subsequent somatic diseases and premature death. JAMA Psychiat 78(3):302–310. https://doi.org/10.1001/jamapsychiatry.2020.3786
Xiao L, Zhou JJ, Feng Y et al (2020) Does early and late life depression differ in residual symptoms, functioning and quality of life among the first-episode major depressive patients. Asian J Psychiatr 47:101843. https://doi.org/10.1016/j.ajp.2019.101843
Schmaal L, Veltman DJ, van Erp TG et al (2016) Subcortical brain alterations in major depressive disorder: findings from the ENIGMA major depressive disorder working group. Mol Psychiatry 21(6):806–812. https://doi.org/10.1038/mp.2015.69
Shen Z, Cheng Y, Yang S et al (2016) Changes of grey matter volume in first-episode drug-naive adult major depressive disorder patients with different age-onset. NeuroImage Clin 12:492–498. https://doi.org/10.1016/j.nicl.2016.08.016
Chae WR, Fuentes-Casañ M, Gutknecht F et al (2021) Early-onset late-life depression: association with body mass index, obesity, and treatment response. Compr Psychoneuroendocrinol 8:100096. https://doi.org/10.1016/j.cpnec.2021.100096
Heun R, Kockler M, Papassotiropoulos A (2000) Distinction of early- and late-onset depression in the elderly by their lifetime symptomatology. Int J Geriatr Psychiatry 15(12):1138–1142. https://doi.org/10.1002/1099-1166(200012)15:12%3c1138::aid-gps266%3e3.0.co;2-7
Sun QM, Zhang S, Xu YH, Ma J, Zhang YT, Zhang XY (2023) Depression severity partially mediates the association between thyroid function and psychotic symptoms in first-episode, drug-naive major depressive disorder patients with comorbid anxiety at different ages of onset. J Affect Disord 339:342–347. https://doi.org/10.1016/j.jad.2023.07.015
Ji CY, Working Group on Obesity in China (2005) Report on childhood obesity in China (1)—body mass index reference for screening overweight and obesity in Chinese school-age children. Biomed Environ Sci BES 18(6):390–400
Ji CY, Chen TJ, Working Group on Obesity in China (WGOC) (2013) Empirical changes in the prevalence of overweight and obesity among Chinese students from 1985 to 2010 and corresponding preventive strategies. Biomed Environ Sci BES 26(1):1–12. https://doi.org/10.3967/0895-3988.2013.01.001
Konttinen H, van Strien T, Männistö S et al (2019) Depression, emotional eating and long-term weight changes: a population-based prospective study. Int J Behav Nutr Phys Activ 16(1):28. https://doi.org/10.1186/s12966-019-0791-8
Sonawalla SB, Fava M (2001) Severe depression: is there a best approach? CNS Drugs 15(10):765–776. https://doi.org/10.2165/00023210-200115100-00003
Yang W, Xiao L, Yuan Z et al (2021) Anxiety and depression in patients with physical diseases and associated factors: a large-scale field survey in general hospitals in China. Front Psychiatry 12:689787. https://doi.org/10.3389/fpsyt.2021.689787
Montgomery SA, Gommoll CP, Chen C, Greenberg WM (2015) Efficacy of levomilnacipran extended-release in major depressive disorder: pooled analysis of 5 double-blind, placebo-controlled trials. CNS Spectr 20(2):148–156. https://doi.org/10.1017/S1092852914000273
Moradi Y, Albatineh AN, Mahmoodi H, Gheshlagh RG (2021) The relationship between depression and risk of metabolic syndrome: a meta-analysis of observational studies. Clin Diabetes Endocrinol 7(1):4. https://doi.org/10.1186/s40842-021-00117-8
Bakhtiari A, Hashemi M, Hosseini SR, Omidvar S, Bijani A, Khairkhah F (2018) The relationship between depression and metabolic syndrome in the elderly population: the cohort aging study. Iran J Psychiatry 13(4):230–238
Liu H, Peng D (2022) Update on dyslipidemia in hypothyroidism: the mechanism of dyslipidemia in hypothyroidism. Endocr Connect 11(2):e210002. https://doi.org/10.1530/EC-21-0002
Xu C, Zhou L, Wu K, Li Y, Xu J, Jiang D, Gao L (2019) Abnormal glucose metabolism and insulin resistance are induced via the IRE1α/XBP-1 pathway in subclinical hypothyroidism. Front Endocrinol 10:303. https://doi.org/10.3389/fendo.2019.00303
Zhou L, Ding S, Li Y et al (2016) Endoplasmic reticulum stress may play a pivotal role in lipid metabolic disorders in a novel mouse model of subclinical hypothyroidism. Sci Rep 6:31381. https://doi.org/10.1038/srep31381
Zhu Q, Jiang G, Lang X et al (2023) Prevalence and clinical correlates of thyroid dysfunction in first-episode and drug-naïve major depressive disorder patients with metabolic syndrome. J Affect Disord 341:35–41. https://doi.org/10.1016/j.jad.2023.08.103
Du FM, Kuang HY, Duan BH, Liu DN, Yu XY (2019) Effects of thyroid hormone and depression on common components of central obesity. J Int Med Res 47(7):3040–3049. https://doi.org/10.1177/0300060519851624
Kim MD, Yang HJ, Kang NR, Park JH, Jung YE (2020) Association between subclinical hypothyroidism and metabolic syndrome among individuals with depression. J Affect Disord 264:494–497. https://doi.org/10.1016/j.jad.2019.11.080
Límanová Z (2018) Thyroid disease in the elderly. Onemocnění štítné žlázy v seniorském věku. Vnitrni lekarsvi 64(11):993–1002
Biondi B, Cappola AR, Cooper DS (2019) Subclinical hypothyroidism: a review. JAMA 322(2):153–160. https://doi.org/10.1001/jama.2019.9052
Chen X, Zheng X, Ding Z et al (2020) Relationship of gender and age on thyroid hormone parameters in a large Chinese population. Arch Endocrinol Metab 64(1):52–58. https://doi.org/10.20945/2359-3997000000179
Zisook S, Lesser I, Stewart JW et al (2007) Effect of age at onset on the course of major depressive disorder. Am J Psychiatry 164(10):1539–1546. https://doi.org/10.1176/appi.ajp.2007.06101757
Yang F, Li Y, Xie D et al (2011) Age at onset of major depressive disorder in Han Chinese women: relationship with clinical features and family history. J Affect Disord 135(1–3):89–94. https://doi.org/10.1016/j.jad.2011.06.056
Park SC, Hahn SW, Hwang TY et al (2014) Does age at onset of first major depressive episode indicate the subtype of major depressive disorder?: the clinical research center for depression study. Yonsei Med J 55(6):1712–1720. https://doi.org/10.3349/ymj.2014.55.6.1712
Lang X, Hou X, Shangguan F, Zhang XY (2020) Prevalence and clinical correlates of subclinical hypothyroidism in first-episode drug-naive patients with major depressive disorder in a large sample of Chinese. J Affect Disord 263:507–515. https://doi.org/10.1016/j.jad.2019.11.004
Nuguru SP, Rachakonda S, Sripathi S et al (2022) Hypothyroidism and depression: a narrative review. Cureus 14(8):e28201. https://doi.org/10.7759/cureus.28201
Yang R, Du X, Li Z et al (2022) Association of subclinical hypothyroidism with anxiety symptom in young first-episode and drug-Naïve patients with major depressive disorder. Front Psychiatry 13:920723. https://doi.org/10.3389/fpsyt.2022.920723
Loh HH, Lim LL, Yee A, Loh HS (2019) Association between subclinical hypothyroidism and depression: an updated systematic review and meta-analysis. BMC Psychiatry 19(1):12. https://doi.org/10.1186/s12888-018-2006-2
Peng P, Wang Q, Lang XE, Liu T, Zhang XY (2023) Association between thyroid dysfunction, metabolic disturbances, and clinical symptoms in first-episode, untreated Chinese patients with major depressive disorder: undirected and Bayesian network analyses. Front Endocrinol 14:1138233. https://doi.org/10.3389/fendo.2023.1138233
Sharif K, Tiosano S, Watad A et al (2018) The link between schizophrenia and hypothyroidism: a population-based study. Immunol Res 66(6):663–667. https://doi.org/10.1007/s12026-018-9030-7
Davies NM, Holmes MV, Davey Smith G (2018) Reading Mendelian randomisation studies: a guide, glossary, and checklist for clinicians. BMJ (Clin Res Ed) 362:k601. https://doi.org/10.1136/bmj.k601
Freuer D, Meisinger C (2023) Causal link between thyroid function and schizophrenia: a two-sample Mendelian randomization study. Eur J Epidemiol 38(10):1081–1088. https://doi.org/10.1007/s10654-023-01034-z
Liu W, Wu Z, Sun M et al (2022) Association between fasting blood glucose and thyroid stimulating hormones and suicidal tendency and disease severity in patients with major depressive disorder. Bosnian J Basic Med Sci 22(4):635–642. https://doi.org/10.13705/bjbms.2021.6754
Zhao Y, Liu JC, Yu F et al (2023) Gender differences in the association between anxiety symptoms and thyroid hormones in young patients with first-episode and drug naïve major depressive disorder. Front Psych 14:1218551. https://doi.org/10.3389/fpsyt.2023.1218551
Yang W, Qu M, Jiang R et al (2022) Association between thyroid function and comorbid anxiety in first-episode and drug nave patients with major depressive disorder. Eur Arch Psychiatry Clin Neurosci. https://doi.org/10.1007/s00406-022-01457-x
Diniz MFHS, Beleigoli AMR, Benseñor IM et al (2020) Association between TSH levels within the reference range and adiposity markers at the baseline of the ELSA-Brasil study. PLoS ONE 15(2):e0228801. https://doi.org/10.1371/journal.pone.0228801
Al-Musa HM (2017) Impact of obesity on serum levels of thyroid hormones among Euthyroid Saudi adults. J Thyroid Res 2017:5739806. https://doi.org/10.1155/2017/5739806
Cho WK, Nam HK, Kim JH et al (2018) Thyroid function in Korean adolescents with obesity: results from the Korea National Health and Nutrition Examination Survey VI (2013–2015). Int J Endocrinol 2018:6874395. https://doi.org/10.1155/2018/6874395
Kang C, Liu J, Zheng Y et al (2023) Association of high BMI with subclinical hypothyroidism in young, first-episode and drug-naïve patients with major depressive disorder: a large-scale cross-sectional study. Eur Arch Psychiatry Clin Neurosci 273(1):183–190. https://doi.org/10.1007/s00406-022-01415-7
Babić Leko M, Gunjača I, Pleić N, Zemunik T (2021) Environmental factors affecting thyroid-stimulating hormone and thyroid hormone levels. Int J Mol Sci 22(12):6521. https://doi.org/10.3390/ijms22126521
Wang Y, Dong X, Fu C et al (2020) Thyroid stimulating hormone (TSH) is associated with general and abdominal obesity: a cohort study in school-aged girls during puberty in East China. Front Endocrinol 11:620. https://doi.org/10.3389/fendo.2020.00620
Lundbäck V, Ekbom K, Hagman E, Dahlman I, Marcus C (2017) Thyroid-stimulating hormone, degree of obesity, and metabolic risk markers in a cohort of Swedish children with obesity. Horm Res Paediatr 88(2):140–146. https://doi.org/10.1159/000475993
Walczak K, Sieminska L (2021) Obesity and thyroid axis. Int J Environ Res Public Health 18(18):9434. https://doi.org/10.3390/ijerph18189434
Nielsen TS, Jessen N, Jørgensen JO, Møller N, Lund S (2014) Dissecting adipose tissue lipolysis: molecular regulation and implications for metabolic disease. J Mol Endocrinol 52(3):R199–R222. https://doi.org/10.1530/JME-13-0277
Li C, Guan H, He Q et al (2021) The relationship between lipotoxicity and risk of extrathyroidal extension in papillary thyroid microcarcinoma. Endocrine 74(3):646–657. https://doi.org/10.1007/s12020-021-02809-8
Zhao M, Tang X, Yang T et al (2015) Lipotoxicity, a potential risk factor for the increasing prevalence of subclinical hypothyroidism? J Clin Endocrinol Metab 100(5):1887–1894. https://doi.org/10.1210/jc.2014-3987
Siemińska L, Wojciechowska C, Walczak K et al (2015) Associations between metabolic syndrome, serum thyrotropin, and thyroid antibodies status in postmenopausal women, and the role of interleukin-6. Endokrynol Pol 66(5):394–403. https://doi.org/10.5603/EP.2015.0049
Lai Y, Wang J, Jiang F et al (2011) The relationship between serum thyrotropin and components of metabolic syndrome. Endocr J 58(1):23–30. https://doi.org/10.1507/endocrj.k10e-272
Shao SS, Zhao YF, Song YF et al (2014) Dietary high-fat lard intake induces thyroid dysfunction and abnormal morphology in rats. Acta Pharmacol Sin 35(11):1411–1420. https://doi.org/10.1038/aps.2014.82
Jia WP, Xiang KS, Chen L, Lu JX, Wu YM (2002) Epidemiological study on obesity and its comorbidities in urban Chinese older than 20 years of age in Shanghai, China. Obes Rev 3(3):157–165. https://doi.org/10.1046/j.1467-789x.2002.00071.x
Vallée A, Perrine AL, Deschamps V, Blacher J, Olié V (2019) Relationship between dynamic changes in body weight and blood pressure: the ESTEBAN survey. Am J Hypertens 32(10):1003–1012. https://doi.org/10.1093/ajh/hpz096
Xie YJ, Ho SC, Su X, Liu ZM (2016) Changes in body weight from young adulthood to middle age and its association with blood pressure and hypertension: a cross-sectional study in Hong Kong Chinese women. J Am Heart Assoc 5(1):e002361. https://doi.org/10.1161/JAHA.115.002361
Mandai N, Akazawa K, Hara N et al (2015) Body weight reduction results in favorable changes in blood pressure, serum lipids, and blood sugar in middle-aged Japanese persons: a 5-year interval observational study of 26,824 cases. Glob J Health Sci 7(5):159–170. https://doi.org/10.5539/gjhs.v7n5p159
Thom G, Messow CM, Leslie WS et al (2021) Predictors of type 2 diabetes remission in the diabetes remission clinical trial (DiRECT). Diabet Med 38(8):e14395. https://doi.org/10.1111/dme.14395
Drøyvold WB, Midthjell K, Nilsen TI, Holmen J (2005) Change in body mass index and its impact on blood pressure: a prospective population study. Int J Obes 29(6):650–655. https://doi.org/10.1038/sj.ijo.0802944
Xia MF, Chang XX, Zhu XP et al (2019) Preoperative thyroid autoimmune status and changes in thyroid function and body weight after bariatric surgery. Obes Surg 29(9):2904–2911. https://doi.org/10.1007/s11695-019-03910-8
Dunbar JA, Reddy P, Davis-Lameloise N et al (2008) Depression: an important comorbidity with metabolic syndrome in a general population. Diabetes Care 31(12):2368–2373. https://doi.org/10.2337/dc08-0175
Acknowledgements
We are grateful to all the clinical physicians and nurses that participated in our current study and also to those research staff that contributed to the clinical assessments.
Funding
This work was supported by grants from the CAS International Cooperation Research Program (153111KYSB20190004) and funded by Tianjin Key Medical Discipline (Specialty) Construction Project (TJYXZDXK-033A).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Xiangyang Zhang, Xiaoen Liu, Xue Tian and Lina Wang. The first draft of the manuscript was written by Xiaoen Liu and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board (IRB) of the First Clinical Medical College, Shanxi Medical University (No. 2016-Y27). The patients/participants provided their written informed consent to participate in this study.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Liu, X., Tian, X., Wang, L. et al. Prevalence and associated factors of obesity in patients with major depressive disorder at different ages of onset. Eur Arch Psychiatry Clin Neurosci (2024). https://doi.org/10.1007/s00406-024-01766-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00406-024-01766-3