
Abstract
Objective
The videolaryngostroboscopy parameters form (VLSP form) is a diagnostic tool for the collection of videolaryngostroboscopic basic findings through the evaluation of 12 parameters. The aim of the present study is to preliminarily investigate intra- and inter-rater reliability, validity and responsiveness of the VLSP form.
Methods
A study on a total amount of 160 forms for the evaluation of VLS basic findings was carried out. 80 forms were scored through the VLSP form and 80 with the Voice Vibratory Assessment with Laryngeal Imaging (VALI) form Stroboscopy (S) by four expert phoniatricians, that blindly scored the VLS recordings of 5 subjects without voice disorders and 5 patients with organic voice disorder before and after successful phonosurgery. Intra-rater and inter-rater analysis have been performed for both forms. The scores obtained through VLSP form and VALI form S have been compared to analyse concurrent validity, while VLSP scores before and after phonosurgery have been compared to analyse responsiveness. Finally, each rater annotated the “difficulty” in rating every parameter and its “importance” for the diagnosis.
Results
The VLSP form showed good inter- and intra-rater reliability. It showed a good accuracy for the documentation of changes of laryngeal anatomy and function after phonosurgery, similarly to the VALI form S. The 12 parameters of the VLSP form were judged “Slightly Important” in 28.3% of the samples, “Very Important” in 64.8% of the samples, “Not Difficult” in 73.1% of the samples.
Conclusions
The results of the present study suggest that the VLSP form is comparable to the VALI form S for the evaluation of videolaryngostroboscopic parameters and is a valid, reliable and reproducible diagnostic tool. It can help voice clinicians in the evaluation of VLS examinations and it allows for a punctual assessment of modifications in laryngeal anatomy and function in pathological conditions and after phonosurgery.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Videolaryngostroboscopy (VLS) is a basic investigation for the diagnosis of laryngeal diseases, using a stroboscopic light source and a microphone to visualize the oscillatory movements of the vocal folds [1]. It is particularly useful in the fields of phoniatrics [2] and laryngeal oncology [3]. Today videolaryngostroboscopy can be performed both through trans-oral approaches, using rigid-telelaryngoscopes, and through trans-nasal digital flexible endoscopes with good quality images. In 2001 the European Laryngological Society (ELS) published a basic Protocol for the assessment of dysphonia [4] which was updated together with the Union of European of Phoniatricians (UEP) in 2023 [5]; these guidelines considered VLS as a mandatory examination for a thorough assessment. In 2002 the Italian Society of Phoniatrics and Logopedics (SIFEL) introduced its multidimensional Protocol for the assessment of dysphonia [6] which follows the ELS guidelines; it contained a form for the collection of the VLS basic findings, which considered several parameters, including those codified by Hirano and Bless [1, 7] as the “Mucosal Wave” and the “Glottic Closure” and other parameters proposed by Bergamini and Ricci-Maccarini in the “SIFEL Protocol”, as the “Vocal Fold Motility” and the “Seat of Voice Source”, providing for a comprehensive evaluation tool for the videolaryngostroboscopic examination.
In 2018 this form was published with drawings, for helping voice clinicians in the evaluation of videolaryngostroboscopy basic findings [8]. This form, called “VLS Parameters (VLSP) form” (Fig. 1) provides scores for the evaluation of 12 parameters: (1) supraglottic framework behaviour, (2) seat of voice source, (3) vocal fold morphology, (4) vocal fold motility, (5) level of the vocal fold, (6) symmetry of glottic vibration, (7) periodicity of glottic vibration, (8) glottic closure, (9) profile of vocal fold edge, (10) amplitude of vocal fold vibration, (11) mucosal wave, (12) stops of vocal fold mucosa vibration.



VLS parameters form
The detailed description of each parameter is reported in the former publication [8]. Before completing the form, the voice clinician has to annotate the type of endoscope used for the examination, pitch, loudness and vocal register of the examined voice sample. These aspects give basic information for the correct evaluation of VLS.
In 2017 Poburka, Patel and Bless published two forms for the collection of basic findings of Videolaryngostroboscopy and High-Speed Videoendoscopy, called Voice Vibratory Assessment with Laryngeal Imaging (VALI) forms [9]. The VALI form Stroboscopy (VALI form S) provides scores for the evaluation of 11 parameters, similar to those contained in the VLSP form. They are: (1) glottal closure, (2) amplitude, (3) mucosal wave, (4) vertical level, (5) non vibrating portion, (6) supraglottic activity, (7) free edge contour, (8) phase closure, (9) phase symmetry, (10) regularity, (11) non vibratory observations. The 8th parameter “Phase Closure” contained in VALI form S provides for the evaluation of the duration of the closed phase of the glottic vibratory cycle compared to the open phase and this is correctly evaluated with High-Speed Videoendoscopy. The VALI form S has drawings for the illustration of the parameters, similarly to the VLSP form. Most of the parameters of the VALI form S are scored in percentage of deviation from normal; they do not include the parameters “Vocal Fold Motility” and “Seat of Voice Source”, that are contained in the VLSP form. The parameters of the VLSP form and of the VALI form S, with the similar parameters in the two forms, are shown in Table 1.
Materials and methods
Patients and procedures
In order to validate the VLSP form and to investigate its inter-and intra-rater reliability and reproducibility, a retrospective study on a total amount of 160 forms for the evaluation of VLS basic findings was carried out. 80 forms were scored through the VLSP form and 80 through the VALI form S. Four phoniatricians with over 10 years of experience in phonosurgery and laryngostroboscopic assessment were recruited to score 5 subjects without voice disorders (4 females, 1 male) and 5 patients (4 females, 1 male) with organic voice disorder before and after successful phonosurgery. Gender, age, vocal pitch and vocal register data, as well as diagnosis and phonosurgical procedures and the data of normal subjects are shown in Table 2. The raters were provided with an user manual that showed how to rate the VLS samples with the two forms. The raters were informed about age and gender of the subjects, type of endoscope used for VLS, vocal pitch (mean F0) and vocal register (1 modal, 2 falsetto), while were blinded to diagnosis and phonosurgical procedures. All the examinations were performed with a rigid 70° STORZ telelaryngoscope and a stroboscopic light Atmos L200 Endostroboscope; video files were saved and stored as WMV high quality videos. For the intra-rater reliability evaluations, the pre-operative VLS samples were re-evaluated one month later in a different order; raters were blind to both other raters scores and their own previous scores.
Most of the VALI form S parameters of are scored in percentage of deviation from normal, while most of the parameters of the VLSP form do not have a percentage scoring; in order to compare the scores of the two forms, each parameter’s possible scorings were associated to numbers and letters, as shown in Fig. 1.
Each parameter of the VLSP form and of the VALI form S was evaluated by the 4 raters who scored the parameter marking it on the form and annotating the “difficulty” in the evaluation of the parameter (0 not difficult, 1 slightly difficult, 2 very difficult). Each parameter of the VLSP form was also scored considering the “importance” for the diagnosis in each patient (0 not important, 1 slightly important, 2 very important).
Statistical analysis
Statistical analysis was carried out with GraphPad Prism software (Version 7.0, GraphPad Software, Inc, San Diego, CA). The D’agostino-Pearson normality test was used to verify Gaussian distributions of continuous variables.
For comparisons between groups, paired t-tests and Wilcoxon tests were used, as appropriate. Inter-rater reliability analysis was carried out with Fleiss K statistics, while for intra-rater reliability analysis Cohen K statistics were used. For the interpretation of k statistics, the guidelines provided by Landis and Koch were considered [9]: k < 0.00 = poor, k = 0.00–0.20 slight, k = 0.21–0.40 fair, k = 0.41–0.60 moderate, k = 0.61–0.80 substantial, k = 0.81–1.00 almost perfect agreement. An alpha of 0.05 was considered for statistical procedures.
Results
No significant differences were found regarding age, gender distribution, mean vocal pitch and vocal register between the group of normal subjects and the group of pathological cases. The scores of all the parameters of VLSP form and VALI form S in the subjects without voice disorder were “0” (normal), with perfect agreement between raters. No additional statistical analysis was therefore necessary To determine the intra-rater reliability of the VLSP form, Cohen K (CK) values were obtained by pooling the repeated ratings of each judge for all VLSP form parameters and all VALI form S parameters on the 5 patients with organic voice disorders. Regarding VLSP form parameters, Ck values of 0.97, 0.83, 0.89 and 0.96 were observed for the four raters, respectively; for VALI form S parameters, Ck values of 0.92, 0.86, 0.93 and 0.91 were observed for the four raters, respectively, suggesting almost perfect agreement for all four raters both in VLSP and in VALI S forms judgements.
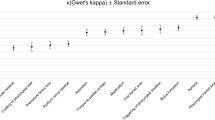
Concerning inter-rater reliability of the four raters assessing the five patients with organic voice disorders before surgery, Fleiss K (Fk) values showed substantial or almost perfect agreements for both VLSP and VALI S forms, as showed in Table 3.
For the responsiveness analysis of the VLSP form, each parameter’s score by each rater in pre- and post-operative conditions was compared. Since VLS parameters are complex and defined by combinations of numbers and letters, a statistical comparison test was not feasible. For this reason, an evaluation on post-surgical modifications was carried out for each parameter in order to establish whether an improvement occurred. For each patients who underwent phonosurgery and for each VSL parameter, the number of raters whose scores improved after phonosurgery was reported as fraction and percentage. Relevant modifications were found for each of the 5 pathological cases with almost perfect agreement in most of the parameters, as shown in Table 4. The percentages of Importance scores for each VLSP form parameter reported by the four raters (0 = not important; 1 = slightly important; 2 = very important) are shown in Table 5. The percentages of Difficulty scores in the evaluation of each parameter (scored as 0 = not difficult, 1 = slightly difficult, 2 = very difficult), both for VLSP form and VALI S form are shown in Table 6. The Fleiss K (Fk) coefficient calculated on Difficulty scores showed an overall good inter-rater reliability for all parameters, both in VLSP and in VALI S forms, ranging from k = 0.37 (fair agreement) to k = 1.0 (perfect agreement), as shown in Table 6.
Discussion
Reliability, validity and responsiveness of the VLSP have been analyzed for the first time. The results of this study regarding the validity, reliability and responsiveness of the VLSP form are similar to those reported in previous studies on VLS evaluation [11, 12]. In particular, VLSP form emerged as a good tool for detecting functional and anatomical changes after phonosurgery, with good inter-rater and intra-rater reliability. The availability of a “user manual” may help the rater, improving the agreement among raters. In the VLSP form the parameter “Vocal Fold Motility”, which is not contained in the VALI form S, allows for the evaluation of the position of the immobile vocal fold and the comparison between examinations before and after medialization laryngoplasty with injection laryngoplasty or thyroplasty, as in two cases presented in this study; also the recent ELS and UEP guidelines [5] recommend the use of the parameter “Motility” in the evaluation of VLS. The parameter “Seat of voice source” is also contained in the VLSP form and not in the VALI S form; it allows for the evaluation of the vibrating laryngeal voice source, which is not necessarily represented by the vocal folds. For instance, in supraglottic voice, vibration may occur between the ventricular bands. After a cordectomy, voice source might take place between a vocal fold and the contralateral ventricular band, as in one case presented in this study. The parameter “Vocal Fold Morphology” of the VLSP form is more comprehensive than the similar parameter of the VALI form S “Non Vibratory Observations”. In fact, it allows for the documentation of the atrophy of a vocal fold, as in 4 cases of this study and the vocal fold augmentation after injection laryngoplasty, in addition to the assessment of laryngeal lesions. The parameter “Glottic Closure” is more comprehensive than the similar parameter of the VALI form S because it provides for the documentation of the “slightly” or “very” incomplete glottic closure. The use of the VALI form S for this study suggested us to improve 4 parameters of the VLSP form, with a percentage score as in the VALI form S: the parameter 1 “Supraglottic Framework Behaviour” has now the specification of the degree of constriction in percentage; the parameter 8 “Glottic Closure” has been implemented with the specification of the degree of incomplete glottic closure in percentage; the parameters 10 “Amplitude of Vocal Fold Vibration” and 11 “Mucosal Wave” have been implemented with the specification of the degree in percentage as well (Fig. 1).
Concerning Importance ratings of VLSP form, all the 12 parameters were judged “slightly important” or “very important” by the four raters in the large majority of cases, suggesting that all the considered parameters can be considered relevant for the assessment of videolaryngostroboscopy.
Regarding Difficulty ratings, both VLSP form and VALI S form parameters were judged “not difficult” or “slightly difficult” by the raters in the large majority of cases; suggesting a good level of reproducibility for the two forms. In general, the scoring of VLSP form was considered slightly easier than VALI S form for all parameters by the raters, as shown in Table 6. The most marked difference between the two forms in terms of “Difficulty” was registered for parameter 3 of VLSP form (Vocal Fold Morphology), corresponding to the parameter 11 of the VALI S form (Non vibratory observations).
There are some limitations to this study. First, the number of videolaryngostroboscopic examinations in both subjects with and without voice disorders is limited, therefore the data provided should be considered as preliminary. Second, the raters involved in the study were expert phoniatricians, therefore it is not known whether reliability and concurrent validity scores apply to non-experts as well. Finally, no data on divergent validity have been provided. Further studies on larger samples of patients, involving both expert and non-expert raters are necessary.
Conclusions
A form for the collection of videolaryngostroboscopic parameters is a useful tool for the evaluation of the VLS examination. The VLSP form emerged as useful and comparable to the VALI form S for the evaluation of videolaryngostroboscopic basic parameters. In particular, the results of the present study suggest that VLSP form is a valid, reliable and responsive diagnostic tool. It can help the voice clinician in the evaluation of the videolaryngostroboscopic examination and it allows for the assessment of changes in laryngeal anatomy and function in pathological conditions and after phonosurgery.
References
Hirano M, Bless D (1993) Videostroboscopic examination of the larynx. Singular Publishing Group, INC., San Diego
Cornut G, Bouchayer M (1986) Apport de la vidéostroboscopie dans les indications de phonochirurgie. Acta Otorhinolaryngol Belg 40:436–442
Crosetti E, Pilolli F, Succo G (2012) Nuove strategie di stadi azione endoscopica nel carcinoma laringeo: la multistep endoscopy. Acta Otorhinolaryngol Ital 32:175–181
Dejonckere PH, Bradley P, Clemente P, Cornut G, Crevier-Buchman L, Friedrich G, Van De Heyning P, Remacle M, Woisard V, Committee on Phoniatrics of the European Laryngological Society (ELS) (2001) A basic Protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Eur Arch Otorhinolaryngol 258:77–82
Lechien JR, Geneid A, Bohlender JE, Cantarella G, Avellaneda JC, Desuter G, Sjogren EV, Finck C, Hans S, Hess M, Oguz H, Remacle MJ, Schneider-Stickler B, Tedla M, Schindler A, Vilaseca I, Zabrodsky M, Dikkers FG, Crevier-Buchman L (2023) Consensus for voice quality assessment in clinical practice: guidelines of the European Laryngological Society and Union of the European Phoniatricians. Eur Arch Otorhinolaryngol. https://doi.org/10.1007/s00405-023-08211-6. (Epub ahead of print. PMID: 37707614)
Ricci-Maccarini A, Lucchini E (2002) La valutazione soggettiva e obiettiva della disfonia. Official lecture at the XXXVI National Congress of the Italian Society of Phoniatrics and Logopedics (SIFEL). Acta Phon Lat 26:13–42
Bless DM, Hirano M, Feder RJ (1987) Videostroboscopic evaluation of the larynx. Ear Nose Throat J 66(7):289–296
Ricci-Maccarini A, Bergamini G, Fustos R (2018) Proposal of a form for the collection of videolaryngostroboscopy basic findings. Eur Arch Otorhinolaryngol 275:1927–1933
Poburka Bj., RR. Patel, Bless DN (2017) Voice-vibratory assessment with laryngeal imaging (VALI) form: reliability of rating stroboscopy and high-speed videoendoscopy. J. Voice 31(4):523.e1–513.e14
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33(1):159–174 (PMID: 843571)
Poburka BJ (1999) A new stroboscopy rating form. J Voice 13:403–413
Bonilha HS, Desjardins M, Garand KL, Martin-Harris B (2018) Parameters and scales used to assess and report findings from stroboscopy: a systematic review. J Voice 32(6):734–755. https://doi.org/10.1016/j.jvoice.2017.09.018. (Epub 2017 Nov 2)
Acknowledgements
The Authors acknowledge Dr. Erennio Natale for his contribution in the preparation of the forms for the raters.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that there is no conflict of interest.
Ethical approval
All procedures performed in this retrospective study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Presented at the PanEuropeanVoiceConference in Tallin on August 24th–27th, 2022.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ricci-Maccarini, A., Mozzanica, F., Fantini, M. et al. Validity, reliability and reproducibility of the VLS parameters form for the collection of videolaryngostroboscopic basic findings. Eur Arch Otorhinolaryngol 281, 2489–2497 (2024). https://doi.org/10.1007/s00405-024-08480-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-024-08480-9