
Abstract
Purpose
This study aimed at determining the importance of an elective neck dissection (END) in case of a cN0 laryngeal or hypopharyngeal carcinoma after (chemo) radiation.
Methods
Retrospective review was made of patients treated in a single tertiary center between 2002 and 2014. Influence of an END in case of a cN0 salvage laryngectomy on complications, recurrence-free survival and disease-specific survival was assessed. Inclusion criteria: squamous cell carcinoma and cN0 neck. Exclusion criteria: second primary tumor in the head and neck, a total laryngectomy because of a dysfunctional larynx, or a previously performed neck dissection.
Results
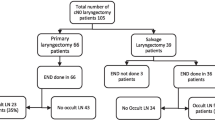
Of the 86 included patients, 27 (31%) underwent an END, of which 1 had occult metastasis (4%). Of the remaining 59 patients (69%) without an END, 3 developed a regional recurrence (5%). The overall survival was significantly higher for patients who had an END (p = 0.037). The incidence of complications was not significantly different between the two groups.
Conclusions
In light of the limited complications of an END and the poor prognosis of regional recurrence after previous (chemo)radiotherapy and a (pharyngo)laryngectomy, we advise consideration of an END at the time of a salvage laryngectomy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The treatment of laryngeal and hypopharyngeal cancer preferably consists of organ preservation using (chemo) radiation. A laryngectomy is performed in case of cartilage destruction and/or extralaryngeal growth, a dysfunctional larynx and when tumors recur after (chemo) radiation.
Performing an elective neck dissection (END) of a negative (N0) neck during salvage laryngectomy is controversial. Based on the rarity of occult neck metastasis, the lack of impact on regional cancer control and the morbidity of neck dissections, several retrospective studies argue against an END [1,2,3,4,5]. However, other studies show an improved survival after an END for advanced local disease [6]. Others advise an END for recurrent stage T3–T4 [7, 8] and supraglottic tumors due to the higher rate of occult metastasis [7,8,9].
In literature, the incidence of occult lymph node metastasis in recurrent laryngeal carcinomas ranges from 0 to 28% [1, 2, 4,5,6,7,8,9,10,11,12]. Patients with a supraglottic tumor [7,8,9] or advanced local disease (i.e., stage T3–T4) [6,7,8] at initial presentation, have a higher rate of occult metastasis. The decision analysis model of Weiss et al. [13] for primary squamous cell carcinoma (SCC) of the head and neck area advises an END if the risk of neck metastasis is over 20%. A more recent model of Hilly et al. [3] concludes that an END is not warranted during salvage laryngectomy after chemoradiation based on the regional recurrence rate and survival rates. Furthermore, the more extensive surgery due to the END could increase morbidity and complication rate [1, 2, 4]. The national guideline of the Dutch Head and Neck surgery committee advises a watchful waiting policy in case of initial negative lymph nodes and no clinical evidence of lymph node metastasis during the local recurrence [14].
Given the controversy in literature, this study aims to determine whether an END should be performed during salvage (pharyngo) laryngectomy. Therefore, we evaluated the influence of an END on the recurrence-free and disease-specific survival and compared the complication rate between patients with and without END during salvage surgery.
Materials and methods
We describe a retrospective study of patients who underwent a salvage (pharyngo) laryngectomy because of a recurrent tumor after primary (chemo) radiation. Patients treated in the period 2002–2014 were reviewed. Permission to conduct this study was received from the Medical Ethics Committee of our institution. Cases were identified using our EPD. Inclusion criteria were a recurrent SCC in the larynx or hypopharynx after (chemo) radiation and a clinical/radiological/cytological negative neck at the time of the recurrence after (chemo) radiation. Before surgery, patients underwent at least one of the following to stage the neck: CT, MRI, PET or ultrasound with fine needle aspiration biopsy (UGFNAB). UGFNAB and CT demonstrated comparable accuracy [15]. The imaging modality choice is based on tumor location and T stage. A neck was considered cN0 if no pathological lymph nodes were found during imaging and/or physical examination, or if detected nodes were cytologically benign. Only patients with curative treatment intention were included. Patients were excluded in case of a second primary tumor in the head and neck area, a total laryngectomy because of a dysfunctional larynx, or a previously performed neck dissection. The decision to perform salvage surgery with or without unilateral/bilateral END was taken after discussion in the multidisciplinary head and neck oncology team, which in principle follows the national guideline of the Dutch Head and Neck surgery committee. However, this decision was sometimes changed pre- or peroperatively by the surgeon.
The following information was collected for included patients: TNM staging and tumor location of primary and recurrent tumor, primary treatment, preoperative imaging, details of surgery and END, postoperative complications, pathology results, tumor recurrence location and date, locoregional control and survival. Initial and recurrent laryngeal tumors were classified by the TNM Classification of Malignant Tumors (8th edition, 2016). When the TNM classification was lacking, tumors were staged retrospectively based on the EPD.
Both unilateral and bilateral ENDs were performed; the choice between selective and modified radical was based on the tumor size and tumor location. In some cases only an END of level VI was performed, see Table 1. When primary closure of the pharyngolaryngeal defect was not possible, a pectoralis major flap or jejunum interposition was used.
All patients were followed up to January 2017, or until date of death. Follow-up time was measured from date of salvage laryngectomy to date of death or date of last follow-up. Recurrences after salvage laryngectomy, laryngopharyngectomy or partial laryngectomy were confirmed by multiple imaging modalities, physical examinations and biopsies.
Statistical analyses were performed using IBM SPSS Statistics 24. A statistical significance level of 5% was used. Descriptive statistics were compared using the Pearson Chi square test in case of categorical variables. When the number of events was < 5, Fisher’s exact test was used. The Kaplan–Meier method was used for survival analysis, the independent T test for comparing mean age and the non-parametric test (Mann–Whitney) for comparing median follow-up time. The disease-specific survival (DSS) was defined as no mortality due to the laryngeal or hypopharyngeal tumor. Recurrence-free survival (RFS) was defined as no local, regional or distance recurrence.
Results
Patients
86 patients treated with a salvage (total or partial) (pharyngo) laryngectomy were included. All patients were cN0 at time of salvage surgery. The majority of the study population was male (84%). The mean patient age at the time of surgery was 65 (range 41–86) years. Of the 86 patients reviewed, initial tumor location was distributed as follows: 53 patients (62%) glottic carcinoma, 25 patients (29%) supraglottic carcinoma, 6 patients (7%) hypopharyngeal carcinoma (all piriform sinus) and 2 patients (2%) subglottic carcinoma. Tumor recurrences were staged T1N0 in 9 patients, T2N0 in 24 patients, T3N0 in 23 patients and T4N0 in 31 patients. 73 patients (85%) underwent a total laryngectomy, 7 patients (8%) underwent a total laryngectomy with pharyngectomy and 6 patients (7%) underwent a partial laryngectomy.
No statistically significant difference in patient characteristics of gender, cT stage (T1–2 or T3–4), cN stage (N0 or N+), location of initial radiotherapy (larynx or larynx and neck), mean overall follow-up and preoperative imaging (CT, MRI or PET) was found for patients with ENDs compared to those without. We did find a statistically significant difference between the groups with and without END for initial tumor localization (glottic, supraglottic, subglottic and hypopharyngeal), rT stage (T1–2 or T3–4) and initial radiation vs. chemoradiation. See Table 1.
Initial treatment of the tumor consisted of radiotherapy for 77 patients, while for 9 patients radiotherapy was combined with cisplatin or cetuximab. Patients received different radiation doses depending on tumor location and size, and total radiation dose was 58–70 Gy. Patients treated with radiotherapy combined with cisplatin or cetuximab had significantly more advanced tumors (cT3–T4N+), positive lymph nodes and subglottic or hypopharyngeal primary locations. 48 patients (56%) received bilateral neck radiotherapy; total dose was 46–51 Gy. Patients who received radiotherapy of the neck had significantly more advanced T stages, more initial positive lymph nodes, more often a supraglottic, subglottic or hypopharyngeal carcinoma and received concurrent cisplatin or cetuximab more frequently than patients who only underwent radiation of the primary site (p = 0.000, p = 0.002, p = 0.000, p = 0.004, respectively). Imaging performed before salvage laryngectomy included CT of the neck (62 patients), ultrasound of the neck (49 patients), PET (5 patients) and/or MRI of the neck (3 patients).
All patients with a primary tumor recurrence were staged cN0. An END was performed on 31% of patients (27/86) at the time of the salvage laryngectomy. Of the performed ENDs, 21 were unilateral and 6 bilateral. 1 patient had occult lymph node metastasis (4%). This patient initially had a T3 supraglottic tumor without positive lymph nodes and was treated with radiotherapy on the central and lateral neck. The patient died few days after surgery due to a dehiscence in the neck with necrosis and major bleeding.
Oncological outcome
Follow-up ranged from 8 days to 147 months. Median follow-up time was 26 months. For the whole cohort, the 5-year OS rate was 47%, while the 5-year OS rate was 62% for patients with an END and 41% for patients without (p = 0.037). The 5-year DSS was 81% for patients with an END and 59% for patients without an END. (p = 0.114). See Fig. 1. The 5-year RFS rate was 74% for patients with an END and 59% for patients without (p = 0.280). 3 patients had a primary lung carcinoma or metastasis due to the laryngeal carcinoma. No evidence of local or regional recurrence was observed on the CT scan of these patients and no further examination was performed given their poor condition. As no distinction between lung metastasis and primary tumor could be made, these patients were excluded from the disease-specific survival analysis.

Kaplan–Meier survival plot for disease-specific survival with elective neck dissection or no elective neck dissection. p value = 0.114 for disease-specific survival
13 patients developed a local recurrence, 3 patients a regional recurrence and 5 patients a distant metastasis. 1 patient developed a local and regional recurrence simultaneously and 3 patients developed a local and distant metastasis simultaneously. 1 local plus regional recurrence and 3 local plus distant recurrences were included in the local recurrence group for the analysis. Hence, total local recurrence rate was 20% (17/86). Local recurrence rate was 11% in the patients who underwent an END (3/27) and 24% for patients who did not undergo an END (14/59) (p = 0.246).
Furthermore, 4 patients had a regional failure, of which 2 had an ipsilateral recurrence, 1 a contralateral recurrence and 1 a bilateral recurrence. 1 patient with a locoregional recurrence was excluded from the analysis because of the local recurrence. See Table 2 for patient characteristics. Regional recurrence occurred in 5% (3/59) of the patients without END and no regional recurrences occurred in the group of patients with END (p = 0.549). Distance metastasis rate was 6% (5/86) for the total group, of which 3% (2/59) was for patients with END and 11% (3/27) for those without END (p = 0.176). Some patients had a recurrence in multiple sites.
A univariate analysis showed no significant difference between no recurrence and (regional) recurrence for the prognostic factors gender, initial tumor site, TNM stage, treatment with (chemo)radiation, radiotherapy on the neck and type of surgery of differentiation grade. See Table 3.
Complications
In total 36% (31/86) of patients developed a postoperative complication. Complications included 20 patients with a pharyngocutaneous fistula, 9 patients with postoperative bleeding and 7 patients with wound infection. See Table 4. Complication rate was comparable between patients with and without an END (37% vs 36%). 7 patients had more than one complication.
Discussion
This study compares outcomes in patients who underwent salvage surgery with or without END. There is no consensus in literature regarding in which cases an END should be performed. The value of an END is determined by the influence on OS and RFS, rate of occult lymph node metastasis and morbidity of an END.
OS was significantly better when an END was performed; DSS and RFS showed no significant difference. Hence, the question is why there is a difference between OS and DSS. Typical head and neck cancer patients have comorbidities and an unhealthy lifestyle including smoking and alcohol consumption, potentially leading to only the fit (ter) patients being selected for an END. Multiple studies, including Freiser et al.’s largest retrospective research to date (125 patients), showed no improved survival after an END [1, 4, 7, 12]. In contrast, a study by Hilly et al. showed that an END in case of advanced tumor stage (T3–T4) had significant impact on the disease-free and OS. In this study the percentage of regional recurrences was the same (8%) after a total laryngectomy with or without END [6]. This means that the ENDs did not have an impact on the regional recurrence rate. In our population, advanced tumor stage (T3–T4) did not influence survival rate, possibly explained by the low number of included patients with END.
The decision to perform an END could be based on the risk of occult lymph node metastasis. In this study only 1 patient had an occult metastasis (4%), which is low compared to literature, in which a wide spread variance (0–28%) is reported [1, 2, 4,5,6,7,8,9,10,11,12]. This variance can be explained by differences in study populations, e.g., patient characteristics, treatment modalities, number of included patients and preoperative radiological imaging. The patient with the occult metastasis in our study initially presented with a T3N0M0 supraglottic tumor. Postoperative pathological examination showed laryngeal cartilage invasion, perineural growth and possibly vaso-invasive growth. Previous research showed a significantly higher risk of occult metastasis in case of cartilage invasion and perineural invasion [7]. However, this conclusion was based on 3 patients with occult lymph node metastasis and, similar to our population with only 1 patient with occult metastasis, which is too few to judge.
In literature, a higher percentage of occult metastasis is reported in case of advanced recurrent tumors (T3–4) [7, 8] and supraglottic tumors compared to small tumors (T1–T2) and other sub locations [7,8,9]. Also, patients with radiation of the larynx and neck for an initial N+ neck had significantly more occult metastasis compared with an N0 neck [11]. In a study of Freiser et al. [12] occult lymph nodes in the neck were significant negative predictors for the OS and disease-free survival. Given the low rate of occult metastasis in our study, no definite conclusion about prognostic factors for occult metastasis can be drawn.
According to Weiss et al. [13], it is advisable to perform an END in case of more than 20% positive occult lymph nodes for a primary SCC in the head and neck area. Reflecting on our results, it is advisable to not perform an END based on the 20% limit. A possible explanation for identifying only 1 patient with occult metastasis is the extensive neck investigations in our institution. Often a CT of the neck is combined with a UGFNAB, and the cytology defines whether a suspected lymph node is malignant or benign. Some studies did not mention pre-operative examination of the neck in their methods [7, 11], leaving it unclear how the neck was staged negative. Other studies performed a combination of CT, MRI and / or PET [2, 9, 12] or only a CT [1, 4, 10]. Pezier et al. [5] used CT or MRI and UGFNAB of the neck when indicated. It is remarkable that they also found a low occult lymph node metastasis rate of 4%. The question is whether a low occult lymph node metastasis rate can be attributed to UGFNAB.
In our study, no significant difference in number of complications between patients with or without an END was found. A total complication rate of 36% for the total population is quite high, but still below the range found in literature (43–66%) [2, 4, 12]. Some studies show significantly more complications in case of salvage laryngectomy with (unilateral or bilateral) END [1, 2, 4]. Increased complication rate makes performing an END less attractive, especially given the fact that the benefits in terms of survival are doubtful. Freiser et al. [12] found a significant higher rate of complications (wound complications) after chemoradiation. In contrast, in our study, patient and tumor characteristics (gender, tumor location and size) and treatment modalities (type of surgery, pre-operative treatment with radiotherapy of chemoradiation) did not have a significant influence on the complication rate. A possible reason for the lack of differences in complication rate between patients with or without END could be patient selection, i.e., fit (ter) patients were selected for an END.
The national guideline of the Dutch Head and Neck surgery committee advises watchful waiting in case of initial negative lymph nodes. 1 of the 2 patients with an ipsilateral regional recurrence had initially a positive lymph node (treated with radiotherapy on the larynx and neck). The number of patients is too small to judge if the advice of the guideline can be supported (50% of regional recurrences with initial N+ and 50% with initial N0).
When performing an END, a choice needs to be made between performing unilaterally or bilaterally. In our study, 27 ENDs were performed, of which 6 were bilateral and 21 unilateral. In total 3 patients had a regional recurrence, of which 2 were ipsilateral and 1 bilateral. Likely, the 2 ipsilateral recurrences could have been avoided by performing an ipsilateral END. The reason for performing a (unilateral or bilateral) selective or modified radical END was not always properly documented and the decision for the type of an END was based on the tumor size and location. Next to this, surgeon’s preferences played a role. Since our study population is very heterogeneous and the performed bilateral ENDs are uncommon, it is not possible to draw a definitive conclusion about performing an ipsilateral or bilateral END.
This study has some limitations. Because of the retrospective design, data may not be complete. The population is heterogeneous in terms of tumor characteristics (location and TNM), preoperative treatment (radiotherapy dose and location, type of chemoradiation) and surgical techniques (type of salvage surgery and ENDs), which can lead to differences in the long-term follow-up. Furthermore, the patient characteristics between the groups with and without END are significantly different, which causes bias in comparison. The reason for (not) performing an END was not always documented. The complications after a total laryngectomy with or without END were determined from registration of complications in the medical file. It is possible that complications were not always adequately recorded; hence the reported complication rate could be lower than reality.
We know patients have a poor prognosis after a second recurrence. Often patients opt out of further treatment, since they have a long history of treatments for this kind of cancer. The question is whether an END is justified by the potential benefit in terms of OS and RFS.
Concluding, we found that patients with a recurrent, lymph node negative, laryngeal or hypopharyngeal carcinoma after primary (chemo) radiation who had salvage (pharyngo) laryngectomy combined with an END had a significantly higher OS than patients without an END. Despite this being a reasonably large retrospective study, the DSS and RFS were not significantly better. 3 of the 59 patients (5%) who did not undergo an END, potentially would have benefitted from an END. 1 patient benefitted from the END because an occult metastasis was found. In light of the limited complications of ENDs and the poor prognosis of regional recurrence after previous radiotherapy and a (pharyngo) laryngectomy, we advise to consider an END at the time of the salvage laryngectomy. A prospective randomized study with a significant number of cases with similar tumor locations and sizes and pre-operative treatment is necessary to determine the effect of an END at the time of a salvage laryngectomy on survival, recurrences, complications and occult metastasis. This could provide a more definite answer, complementing the so-far conducted retrospective studies.
References
Deganello A, Meccariello G, Bini B et al (2014) Is elective neck dissection necessary in cases of laryngeal recurrence after previous radiotherapy for early glottic cancer? J Laryngol Otol 128(12):1089–1094
Basheeth N, O’Leary G, Sheahan P (2013) Elective neck dissection for no neck during salvage total laryngectomy: findings, complications, and oncological outcome. JAMA Otolaryngol Head Neck Surg 139(8):790–796
Hilly O, Stern S, Horowitz E, Leshno M, Feinmesser R (2013) Is there a role for elective neck dissection with salvage laryngectomy? A decision-analysis model. Laryngoscope 123(11):2706–2711
Bohannon IA, Desmond RA, Clemons L, Magnuson JS, Carroll WR, Rosenthal EL (2010) Management of the N0 neck in recurrent laryngeal squamous cell carcinoma. Laryngoscope 120(1):58–61
Pezier TF, Nixon IJ, Scotton W et al (2014) Should elective neck dissection be routinely performed in patients undergoing salvage total laryngectomy? J Laryngol Otol 128(3):279–283
Hilly O, Gil Z, Goldhaber D et al (2015) Elective neck dissection during salvage total laryngectomy—a beneficial prognostic effect in locally advanced recurrent tumours. Clin Otolaryngol 40(1):9–15
Yao M, Roebuck JC, Holsinger FC, Myers JN (2005) Elective neck dissection during salvage laryngectomy. Am J Otolaryngol 26(6):388–392
Wax MK, Touma BJ (1999) Management of the N0 neck during salvage laryngectomy. Laryngoscope 109(1):4–7
Koss SL, Russell MD, Leem TH, Schiff BA, Smith RV (2014) Occult nodal disease in patients with failed laryngeal preservation undergoing surgical salvage. Laryngoscope 124(2):421–428
Farrag TY, Lin FR, Cummings CW et al (2006) Neck management in patients undergoing postradiotherapy salvage laryngeal surgery for recurrent/persistent laryngeal cancer. Laryngoscope 116(10):1864–1866
Amit M, Hilly O, Leider-Trejo L et al (2013) The role of elective neck dissection in patients undergoing salvage laryngectomy. Head Neck-J Sci Spec 35(10):1392–1396
Freiser ME, Ojo RB, Lo K et al (2016) Complications and oncologic outcomes following elective neck dissection with salvage laryngectomy for the N0 neck. Am J Otolaryngol 37(3):186–194
Weiss MH, Harrison LB, Isaacs RS (1994) Use of decision-analysis in planning a management strategy for the stage N0 neck. Arch Otolaryngol 120(7):699–702
Dutch Workgroup Head and Neck tumors, Netherlands Comprehensive Cancer Organisation (IKNL) (2010) Guideline laryngeal carcinoma, version 3.0
Takes RP, Righi P, Meeuwis CA et al (1998) The value of ultrasound with ultrasound-guided fine-needle aspiration biopsy compared to computed tomography in the detection of regional metastases in the clinically negative neck. Int J Radiat Oncol Biol Phys 40(5):1027–1032
Acknowledgements
No acknowledgment of grant support and of individuals who were of direct help in the preparation of the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Bernard, S.E., Wieringa, M.H., Meeuwis, C.A. et al. Elective neck treatment during salvage (pharyngo) laryngectomy. Eur Arch Otorhinolaryngol 276, 1127–1133 (2019). https://doi.org/10.1007/s00405-018-5257-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-018-5257-0