
Abstract
This study investigated the effects of head position on gain values during video head impulse tests (vHITs). Different head positions were used for vHIT of the horizontal semicircular canals of 20 healthy controls and 18 patients with unilateral vestibular loss (UVL), with head velocities ranging from 150°/s to 200°/s. Differences in vestibulo-ocular reflex gain in the control and patient groups according to head position (0° and 30° downward pitch) were analyzed. In the unaffected control group, the 30° pitched-down position resulted in a mean gain increase of up to 1.0 in both ears (right ear: 0.85 ± 0.26 for head-up and 1.05 ± 0.12 for head-down, p = 0.004; left ear: 0.75 ± 0.18 for head-up and 0.98 ± 0.16 for head-down, p < 0.001). In patients with UVL, the mean gains on the diseased side were 0.92 ± 0.16 in the head-up position and 0.82 ± 0.2 in the head-down position, at similar head velocities (p = 0.046). The pitched-down position also increased the asymmetry between ears in patients with UVL, at the same head velocity. A 30° head-down position can increase vHIT sensitivity, which resulted in increased mean gain in unaffected people and decreased mean gain in most of the patients with UVL in this study. This method may more effectively stimulate the horizontal semicircular canal. This vHIT modification may be helpful for more precisely evaluating vestibular function, thus reducing false-negative findings.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Halmagyi and Curthoys first described the head impulse test in 1988 [1]. The test evaluates semicircular canal function by interpreting the vestibulo-ocular reflex induced by stimulation of each canal according to different head rotational axes. The main pathologic finding of the head impulse test is the catch-up saccade, a compensatory mechanism of visual fixation in response to fast head movement in patients with reduced vestibulo-ocular reflex (VOR) [2, 3]. However, examiners may miss catch-up saccades during head movement (covert saccade), thus underscoring the need for more objective techniques to increase the sensitivity of the head impulse test. A scleral magnetic search coil was used to increase test sensitivity and obtain objective results, but the method was invasive and expensive to use in clinical settings. Recently, video-nystagmography (video head impulse test, vHIT) has become commercially available in clinical settings and has been shown to have similar findings to those of scleral magnetic search coil [4]. The vHIT is useful in patients with acute spontaneous vertigo, where the test helps to identify patients with reduced VOR gain [4]. Compared with the bedside head thrust test, the vHIT can detect both covert and overt saccades in a test. Furthermore, the vHIT can calculate the quantitative gain of eye velocity relative to head velocity. Development of a new device made the test more familiar and popular for evaluation of vestibular disorder in clinical settings.
Two parameters are generally used in the interpretation of vHIT results: vestibulo-ocular reflex (VOR) gain and catch-up saccade. However, there have been debates regarding interpretation of the parameters and test methods that could influence the test results. VOR gain can be influenced by test conditions such as target proximity, subject mental status, active or passive performance, subject age, stimulation velocity, goggle slippage, eye position, and head flexion/extension angle. Among these testing factors, we focused on head position. It is generally known that the head should be pitched down approximately 30° for effective stimulation of the horizontal semicircular canal (HSCC) due to the 30° upward tilt of the HSCC from the horizontal plane. Therefore, pitched-down position in the head impulse test might optimize the acceleration signal transduced exclusively through the HSCC. However, a previous study reported that the pitched-down head position did not affect HSCC stimulation because the strength of the stimulus decreased as a cosine function of head pitch [5]. However, recommendations regarding head position during testing (earth-horizontal naso-occipital axis or 30° head flexion) differ according to device manufacturer; it is possible that the borderline test results can be affected by head position, critically affecting normal or abnormal results [6–8]. Therefore, this study investigated the effect of head flexion on VOR gain during vHIT to identify the sources of discrepancies and the optimal vHIT methods. The results of this study may contribute to development of optimal methods for better vHIT results.
Subjects and methods
Subjects
Twenty healthy subjects (age 24–38 years, mean ± SD 28.4 ± 5.3 years, men/women 8/12) and 18 patients (age 27–64 years, mean ± SD 44.4 ± 13.4 years, men/women 10/8) with unilateral vestibular loss (UVL) were enrolled in this study (Table 1). The unaffected subjects did not have any history of vestibular disorder, vertigo or dizziness, posture or gait abnormalities, hearing impairment, and visual problems. They did not show any abnormalities on complete neuro-otologic examination and had normal caloric test results. Patients with UVL showed more than 25 % asymmetry in bithermal caloric tests. Their mean canal paresis value was 53.88 ± 16.69. Their final diagnoses were acute vestibular neuritis (10 cases), Meniere’s disease (six cases), and vestibular schwannoma (two cases) (Table 1).
All subjects provided their written informed consent to participate in this study. The study was approved by the Institutional Review Board of the principle author’s institute, where the patients were enrolled.
vHIT test with two different head-pitch angles
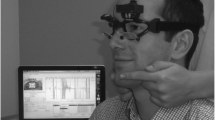
vHIT and bithermal caloric tests were performed on the same day. The tests were performed in the patient group 1–4 weeks after the onset of acute vertigo symptoms. VOR evaluation for HSCC was performed with an ICS Impulse system (Otometrics, Denmark) with its data acquisition software (OTOsuite Vestibular 1.00 Build 263). A high-speed camera (250 Hz), which captured the image of the right eye, and a gyroscope, which recorded the velocity of the head movements, were mounted on the goggles. The default software settings were used for the recordings. The subjects were asked to sit on a chair positioned 100 cm from a wall upon which a target for visual fixation was marked. Video goggles were placed properly on the face of the subjects to minimize slippage that might cause inaccurate data. The head thrust for HSCC stimulation was performed in two different head positions in each patient: (1) head-up: naso-occipital plane parallel to the earth-horizontal plane, and (2) head-down: a starting position of 30° pitched down (HSCC parallel to the earth-horizontal plane). We used a digital protractor to measure the 30° head angle. Rapid and passive movements of the head (head thrusts) were performed in the horizontal (yaw) plane towards a randomly chosen direction to reduce predictive saccades while the subject fixated on a dot located 100 cm away at eye height on the wall directly in front of the patient. The head velocities were between 150°/s and 200°/s. For data analysis, more than 20 impulses were delivered in each direction. The VOR mean gain used as the parameter of evaluation in this study was automatically calculated. The difference of mean VOR gain value between the two different test head positions was analyzed (Fig. 1).

Representative vHIT results in patients with unilateral vestibular loss. a The head-down position reveals larger gain asymmetry in a 43-year-old man with acute vestibular neuritis in his right ear. b The head-down position in a 52-year-old woman with Meniere’s disease in her left ear shows lower gain on the lesion side. Blue spot, gain on left ear with head-up position; Red spot, gain on right ear with head-up position; Violet spot, gain on left ear with head-down position; Orange spot, gain on right ear with head-down position
Statistical analysis
The results were analyzed using Fisher’s exact or Chi-square tests where appropriate (categorical variables), and paired or unpaired t tests (continuous variables) between two groups. Differences in the degree of gain before and after head flexion in individual subjects were evaluated by paired t test. Differences were considered significant if p < 0.05. All statistical analyses were performed using PASW for Windows, version 18.0 (SPSS, Inc., 2009; Chicago, IL, USA).
Results
Difference of VOR gain between the two test positions in unaffected participants
The mean peak head movement velocities in the right ears were 169.75 ± 12.82°/s and 170.75 ± 13.11°/s for the head-up and head-down positions, respectively. There was no significant difference in mean peak head movement velocity between the two positions (p > 0.05, Table 2). The mean gain values of the head-down position were significantly greater and closer to 1.0 than those of the head-up position in both sides (Table 1; Fig. 2a, b); the mean VOR gain values on the right and left sides for the head-down and head-up positions were 1.05 ± 0.12 and 0.98 ± 0.16 and 0.85 ± 0.26 and 0.75 ± 0.18, respectively (p = 0.004 and p < 0.001 for right and left sides, respectively). The gain values of both sides in the head-up position were more widely distributed than those of the head-down position; they also showed larger standard deviations (Fig. 2a, b). The results of vHIT showed no catch-up saccades in head-down and head-up positions.

Differences in mean gains between head-up and head-down positions in normal participants (a, b) and patients with unilateral vestibular loss (c, d). The mean gains on the right (a) and left (b) ears with the head-down position are closer to 1.0, compared to those in the head-up position (p = 0.004 and p < 0.001, respectively). The mean gains on the diseased side are decreased in the head-down position with similar head velocities (p = 0.046), but there are no gain differences on the healthy sides
Differences in VOR gain between two test positions in patients with UVL
The mean VOR gains on the affected sides were 0.82 ± 0.2 and 0.92 ± 0.16 in the head-down and head-up positions, respectively, with similar stimulating head velocities (p = 0.046, Table 2; Fig. 2c). In contrast, there was no significant difference in the mean VOR gain on the healthy side between the two positions (0.91 ± 0.13 head-up and 0.96 ± 0.16 head-down, p > 0.05, Table 2; Fig. 2d). In the graph of paired changes of gains on the affected sides (Fig. 3), every spot showed lower gains in the head-down position, except for three with gains of 1.04, 0.99, and 1.18 in the head-up position.

Individual gain traces in healthy participants (a) and patients with unilateral vestibular loss (b) with two different vHIT head positions
Low gain in the head-up position was observed in eight of 18 patients with UVL (44 %); however, the test sensitivity increased to 78 % (14/18) in the head-down position. The head-down position resulted in a false-negative rate drop to 15 % from 45 % in patients with UVL.
Correlation between vHIT VOR gain and caloric test canal paresis in patients with UVL
The canal paresis value on the bithermal caloric test tended to be inversely proportional to VOR gain on vHIT in patients in the head-down position (R 2 = 0.444, p = 0.003, Fig. 4a). In contrast, correlation between the gain and the canal paresis value was not significant in the head-up position (R 2 = 0.013, p = 0.648, Fig. 4b).

Correlation between VOR gain in vHIT with head-down (a) and head-up position (b) and canal paresis values in a bithermal caloric test of patients with unilateral vestibular loss. The graph shows the inverse correlation only in the head-down position (a)
Discussion
This study evaluated the effect of head-down position on the sensitivity of vHIT gain values. Our data suggest the following: (1) the head-down position in vHIT increased the gain close to 1.0 among people with normal vestibular function; (2) the gain on the lesion side in patients with UVL was more decreased in the head-down position than in the head-up position, despite no change in gain on the healthy side. Therefore, the results of this study suggest that the head-down position is optimal for more reliable gain values by more effectively stimulating the HSCC.
Shubert et al. [9] reported an increased head impulse test sensitivity of 71 % with a 30° head-down pitch, compared with the previously reported sensitivity values of 34–39 % [10, 11]. If the head impulse test is done with the neck in a neutral position (no cervical flexion), the head acceleration may be distributed to the vertical semicircular canals as well as the HSCCs [12]. As a result, peripheral vestibular afferents and central vestibular neurons of the intact HSCC are exposed to less acceleration and are, therefore, less likely to reach the inhibitory cutoff. Curthoys et al. also reported that the proportions and directions of acceleration affecting vertical canals can be read off and the maximal stimulation occurs in the HSCCs in a 21° pitched-down position [5]. In our study, there were 18 false-positive cases (healthy people incorrectly identified as having VOR gain under 0.8) in normal participants. The false-positive rate decreased to 15 % with head-down positioning. The variable gain values, high false-positive rate in normal participants, and high false-negative values in patients with UVL might be caused by insufficient head stimulation velocity (150°/s–200°/s) in our study. One study on the relationship between head stimulation velocity and gain, which reported that increasing head velocity could increase the gain higher, supports this idea [13]. Black’s study showed that the ipsilesional deficit and angular VOR asymmetry gradually increased with increasing head velocity [14]. The VOR asymmetry of patients with UVL significantly increases with higher acceleration [15]. However, stimulation with head velocities higher than 200°/s–250°/s may cause inaccurate gain values due to goggle slippage and wobble. This phenomenon is more frequent in Asian subjects. Because Asian noses are typically lower and flatter than Caucasian noses, goggles are more vulnerable slipping during high-velocity stimulation. The optimal head stimulation velocity that offered minimal goggle slippage was 150°/s–200°/s [6], which is also the lower limit of the stimulation range recommended by the manufacturer. In our study, the head velocity, ranging from 150°/s to 200°/s, was performed by a trained specialist, and cases outside this range were excluded. Despite the similar head velocity between the both groups in normal participants, the mean gains were increased around 1.0 in head-down position (0.85 ± 0.26 changed to 1.05 ± 0.12 on the right ear and 0.75 ± 0.18 to 0.98 ± 0.16 on the left ear). In the patients with UVL, the mean gain in only the diseased side was significantly decreased in head-down position (0.92 ± 0.16 to 0.82 ± 0.2, p = 0.046). The manufacturer’s recommended protocol suggests that head pitched-down position does not greatly increase the strength of the stimulus to the horizontal canals, since the strength of the stimulus decreases as a cosine function of head pitch. However, our results showed that the downward pitch could increase sensitivity with a head stimulation velocity of 150°/s–200°/s, which may be an alternative examination protocol. To optimize vHIT sensitivity with a velocity range of <200°/s, we recommend a 30° downward head pitch for HSCC stimulation.
The caloric test is considered the most useful method for identifying individuals with suspected peripheral UVL [16, 17]. However, the caloric stimulus is not physiological; its responses are mainly produced by thermally induced convection flow in the endolymph of the lateral semicircular canals [18]. Perez and Rama-Lopez [19] reported a clinical HIT specificity and sensitivity of 91 and 45 %, respectively, compared to caloric testing. Shubert et al. [9] compared caloric testing results to those of clinical head impulse testing in 176 patients presenting with vestibular disorder. The sensitivity of the clinical head impulse test for identifying vestibular hypofunction was 71 % for unilateral vestibular hypofunction and 84 % for bilateral hypofunction, with a specificity of 82 %. In this study, we collected data from 18 patients with acute vestibular symptoms and unilateral canal paresis greater than a 25 % cutoff in caloric tests (mean canal paresis value: 53.88 ± 16.69 %). Only the head-down position was significantly correlated with VOR gain in vHIT and canal paresis in caloric testing (R 2 = 0.444, p = 0.003, Fig. 4b). However, the linear correlation between the two tests disappeared in the head-up position (R 2 = 0.013, p = 0.648, Fig. 4a). This finding suggests that the gains in head-down condition more exactly reflected the canal paresis than those in head-up condition.
We also observed that the gains for leftward head impulses were lower than those for rightward head impulses in normal participants. Our finding is consistent with previous research that reported higher VOR gain in the adducting eye than in the abducting eye (in our case, the right eye for both rightward and leftward head impulses) when both eye movements were recorded during head impulse stimulation [20]. This is likely due to the shorter pathway to the abducting right eye after leftward head impulse (disynaptic) than to the adducting right eye after rightward head impulse because of an additional abducens internuclear neuron [21–25].
The results of this study show that head position during vHIT with a velocity of <200°/s can influence gain values. Placing the head in a pitched-down position can increase the vHIT sensitivity at this stimulation velocity. This method may be useful for evaluating vestibular function in patients with wide faces and low/flat noses, in which goggle slippage frequently occurs during high-velocity stimulation. To generalize the usefulness of this test method, prospective studies in larger populations with various facial structures should be performed with different stimulation velocities.
Conclusion
The head pitched downward at 30° during vHIT can provide more sensitive VOR gain values with a stimulation velocity of 150°/s–200°/s, possibly by providing an optimal acceleration signal induced exclusively through the HSCCs.
References
Halmagyi GM, Curthoys IS (1988) A clinical sign of canal paresis. Arch Neurol 45:737–739
Aw ST, Halmagyi GM, Black RA, Curthoys IS, Yavor RA, Todd MJ (1999) Head impulses reveal loss of individual semicircular canal function. J Vestib Res 9:173–180
Halmagyi GM, Aw ST, Cremer PD, Curthoys IS, Todd MJ (2001) Impulsive testing of individual semicircular canal function. Ann N Y Acad Sci 942:192–200
MacDougall HG, Weber KP, McGarvie LA et al (2009) The video head impulse test: diagnostic accuracy in peripheral vestibulopathy. Neurology 73:1134Y41
Curthoys IS, Blanks HI, Markham CH (1997) Semicircular canal functional anatomy in cat, guinea pig and man. Acta Otolaryngol 83:258–265
MacDougall HG, McGarvie LA, Halmagyi GM, Curthoys IS, Weber KP (2013) The video head impulse test (vHIT) detects vertical semicircular canal dysfunction. PLoS One 8(4):e61488
Jongkees LB, Maas JP, Philipszoon AJ (1962) Clinical nystagmography. A detailed study of electro-nystagmography in 341 patients with vertigo. Pract Otorhinolaryngol 24:65–93
Weber KP, MacDougall HG, Halmagyi GM, Curthoys IS (2009) Impulsive testing of semicircular-canal function using videooculography. Ann N Y Acad Sci 1164:486–491
Schubert MC, Tusa RJ, Grine LE, Herdman SJ (2004) Optimizing the sensitivity of the head thrust test for identifying vestibular hypofunction. Phys Ther 84(2):151–158
Harvey SA, Wood DJ (1996) The oculocephalic response in the evaluation of the dizzy patient. Laryngoscope 106:6–9
Harvey SA, Wood DJ, Feroah TR (1997) Relationship of the head impulse test and head-shake nystagmus in reference to caloric testing. Am J Otol 18:207–213
Tusa RJ, Grant MP, Buettner UW et al (1996) The contribution of the vertical semicircular canals to high-velocity horizontal vestibule-ocular reflex (VOR) in normal subjects and patients with unilateral vestibular nerve section. Acta Otolaryngol 116:507–512
Grane BT, Virre ES, Demer JL (1997) The human horizontal vestibulo-ocular reflex during combined linear and angular acceleration. Exp Brain Res 114(2):304–320
Black RA, Halmagyi GM, Thurtell MJ, Todd MJ, Curthoys IS (2005) The active head-impulse test in unilateral peripheral vestibulopathy. Arch Neurol 62(2):290–293
Sadeghi SG, Minor LB, Cullen KE (2006) Dynamics of the horizontal vestibuloocular reflex after unilateral labyrinthectomy: response to high frequency, high acceleration, and high velocity rotations. Exp Brain Res 175:471–484
Ferguson JH, Altrocchi PH, Brin M et al (1996) Assessment: electronystagmography. Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 46:1763–1766
Fife TD, Tusa RJ, Furman JM et al (2000) Assessment: vestibular testing techniques in adults and children. Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 55:1431–1441
Rohrmeier C, Richter O, Schneider M, Wirsching K, Fiedler I, Haubner F, Strutz J, Kühnel TS (2013) Triple test as predictive screen for unilateral weakness on caloric testing in routine practice. Otol Neurotol 34(2):297–303
Perez N (2003) Rama-Lopez J Head-impulse and caloric tests in patients with dizziness. Otol Neurotol 24(6):913–917
Weber KP, Aw ST, Todd MJ et al (2008) Inter-ocular differences of the horizontal vestibulo-ocular reflex during impulsive testing. Prog Brain Res 171:195Y8
Highstein SM, Holstein GR (2006) The anatomy of the vestibular nuclei. Prog Brain Res 151:157Y203
Chung J, Jung HJ, Kim CS, Kim YH (2014) A case of post-traumatic Meniere’s disease. Korean J Audiol 18(1):41–44
Yu KK, Choi CH, An YH, Kwak MY, Gong SJ, Yoon SW, Shim HJ (2014) Comparison of the effectiveness of monitoring Cisplatin-induced ototoxicity with extended high-frequency pure-tone audiometry or distortion-product otoacoustic emission. Korean J Audiol 18(2):58–68
Chung J, Jung HJ, Kim CS, Kim YH (2014) A Case of Post-Traumatic Meniere's Disease. Korean J Audiol 18(1):41–44
Shim DB, Song CE, Jung EJ, Ko KM, Park JW, Song MH (2014) Benign paroxysmal positional vertigo with simultaneous involvement of multiple semicircular canals. Korean J Audiol 18(3):126–130
Acknowledgments
This work was supported by “Industrial Core Technology Development Program of Biomedical Devices” funded by the Ministry of Trade, industry and Energy (MI, Korea). (10051518).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to disclose.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Financial disclosures
The authors have sources of financial support or funding to disclose.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Seo, Y.J., Park, Y.A., Kong, T.H. et al. Head position and increased head velocity to optimize video head impulse test sensitivity. Eur Arch Otorhinolaryngol 273, 3595–3602 (2016). https://doi.org/10.1007/s00405-016-3979-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-016-3979-4