
Abstract
The aim of this study was to introduce and discuss the method of preoperative radiological diagnosis to the congenital absence or atresia of the oval window (OW), and the method of surgical treatment. From July 2010 through August 2014, patients with normal external canal and tympanic membrane but conductive hearing loss underwent high resolution CT scan (HRCT). The multi-planar reformation (MPR), a post-processing protocol, was used. The patients with diagnosis of OW atresia and malformed stapes preoperatively underwent surgical treatment. The vestibular drilled-out and promontory drilled-out technique was used to reconstruct the ossicular chain. In the preoperative radiological diagnosis, six patients (ears) were noted to have congenital absence or atresia of the oval window with malformed facial nerve (class 4) and two patients (ears) were found to have footplate fixation (class 2). In the surgical treatment of eight ears, the malformed structure was identified and the ossicular chain reconstruction was made in six ears. The coronal HRCT CT imaging and the MPR post-processing technique can provide us practical and definite information for surgical treatment, especially in the discrimination of OW atresia and the fixed stapedal footplate. The promontory drill-out technique, fenestration in the bottom of the basal turn, provides us a new method in the hearing reconstruction when the area of OW was fully covered by malformed facial nerve. This technique was first reported in the literature.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Congenital absence or atresia of the OW is an uncommon embryologic defect. In addition, the defect is associated with an extraordinary anomalous development and malposition of the horizontal facial canal is rare uncommon. This malformation is characterized by the clinical presentation of conductive hearing loss, normal external ear canal, and normal middle ear cavity. Although the radiological diagnosis of congenital absence or atresia of the OW is not difficult on HRCT, the surgical correction is still difficult. In this study, we used HRCT and MPR techniques to detect patients with congenital malformation of the oval window and its related structure. According to the pre-operative radiological diagnosis, the surgical method was selected. The discussion was focused on the radiological diagnosis, surgical technique, and the Teunissen’s classified system [1].
Materials and methods
Cases enrolled
This is a retrospective study. From July 2010 through August 2014, patients with conductive hearing loss from our department were selected. All patients underwent CT scan and some diseases were excluded (otosclerosis, tympanosclerosis, otitis media, and atresia of external ear canal). The cases with malformation of the OW included two patients with unilateral conductive hearing loss and six patients with bilateral conductive hearing loss. Of the eight patients, four were male and four female, ranging in age from 7 to 30 years. All patients presented with congenital hearing problems, (see Table 1) and all malformations were confirmed by the surgery.
CT scan and surgical technique
The 128-channel multi-detector row CT scanner (Philips Brilliance iCT128) was used. The axial thin slice scanning was set at a collimation of 20 × 0.625 mm, with a pitch at 0.25 mm, horizon (FOV) at 150 mm × 150 mm, matrix at 1024 × 1024, voltage at 120 kV and current at 350 mA. All data were then transmitted to the EBW4 workstation for reconstruction of HRCT and MPR imaging. All primary surgeries were performed by the first author of this article. The incisions located at the posterior auricular and the tympanic cavity were inspected. The inspection was focused on the ossicular chain, oval window, and horizontal facial canal. According to the malformation of OW and related structure, the methods of the ossicular chain reconstruction were selected. The reconstructed materials were titanium TORP or platinum/titanium-piston. According to the 1995 guidelines of the Committee on Hearing and Equilibrium [2], the hearing results are recorded for both the pre- and post-operative AB-gap and AB-gap closure
Results
For the cases enrolled, Table 1 tabulated the radiological and surgical results. In fact, case 1 and cases 4–8 were bilateral malformation but only the ear underwent operation were listed in Table 1. According to the classification system of Teunissen and Cremers [1] (Table 2), six of the eight patients were classified as class 4. These six (cases 1, 2, 4, 5, 7, and 8) patients had absence or atresia of the OW and malformation of the stapes and facial nerve. Cases 3 and 6 had normal OW but a fixed stapedial footplate. Case 3 had malformation of facial nerve. According to the malformation of OW and facial nerve, the different methods of hearing reconstruction were selected in cases 1, 2, 3, 4, 6, and 7. The reconstruction was abandoned in case 5 and 8 because of the facial nerve overlaying the OW. None of the patients had facial nerve injury. The duration of follow-up ranged from 3 to 48 months.
Typical case
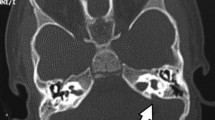
Case 1 (No. 2) Figure 1a (CT-MPR imaging) shows the OW tapering to a central depression (long black arrow) and facial nerve (short black arrow) located at the low position. Figure 1b is the picture of malformed OW and facial nerve seen during the operation. The atresia bone of OW was drilled out (Fig. 1c long-dotted black arrow) and the titanium-piston was implanted between the handle of malleus and the opened hole of OW (Fig. 1d short white arrow).

Long black arrow absence of oval window, short black arrow facial nerve, long-dotted white arrow partial long limb of incus, short white-dotted arrow handle of malleus, short white arrow titanium-piston, long black-dotted arrow bony plate of vestibular drilled partially
Case 2 (No. 4) Figure 2a is the pre-operative CT coronal image, Fig. 2b, c is the MPR imaging. The MPR imaging shows a thick bony plate tapering to a central depression (long black arrow) more clearly than the coronal imaging. Figure 2d shows the osseous OW atresia. The bony plate of OW was about 1 mm thick and was drilled out (Fig. 2e) with 0.5 mm diamond burr. The platinum/titanium-piston (Fig. 2f) was implanted between the long limb of incus and the opened hole of OW.

a CT coronal imaging, b, c CT-MPR imaging. Long black arrow absence of oval window, white short arrow facial nerve, long-dotted white arrow long limb of incus, short white-dotted arrow superstructure of stapes, short black arrow titanium and plastipore piston
Case 3 (No. 7) Figure 3a, b is the pre-operative CT MPR image, Fig. 3f is the post-operative MPR imaging. The osseous plate (long black arrow) of OW and the facial nerve located at the area of OW (short white arrow) can been seen. Figure 3d, e shows the position of promontory drilled out (long black arrow) and the implanted titanium-TORP between tympanic membrane and the hole of promontory. Figure 3f is the post-operative MPR imaging. The position of TORP with the column base inserted into the beginning of scala tympanic can be seen clearly.

Long black arrow atresia of OW, white short arrow facial nerve, long black-dotted arrow promontory drill-out, short black-dotted arrow round window, black short arrow the column base of titanium TORP. a Pre-operative CT-MPR imaging, long white arrow (L): handle of malleus; b pre-operative CT-MPR imaging, long white arrow (L): superstructure of stapes; c, d, e operative imaging; f post-operative CT-MPR imaging, long white arrow (L): titanium TORP inserted into the beginning of the scala tympanic
Case 4 (No. 3) Figure 4a is the pre-operative axial CT image, the facial nerve covered partial OW. Figure 4b is the MPR image, the footplate is normal in shape. Figure 4c is the 3D-reconstruction of ossicular chain, the stapes presented a mass and long limb of incus absence (Fig. 4b, c short black arrow). The pre-operative diagnosis was approved in the operation. The fixed footplate was mobilized and the titanium-TORP (long black-dotted arrow) was implanted between tympanic membrane and the footplate.

a Pre-operative axial CT imaging, b MPR imaging, c 3D-reconstruction of ossicular chain, d–f picture that we seen in the operation. The titanium-PORP was implanted in the micro hole of narrowed footplate. Long black arrow normal footplate in shape, short white arrow facial nerve, long white arrow absence of long limb of incus, short white-dotted arrow handle of malleus, short black arrow superstructure of stapes as a mass, long black-dotted arrow titanium-PORP, short white arrow facial nerve
Discussion
Embryology and question
The OW and stapes have different embryological origins. The stapes, together with the long limb of incus and handle of malleus, develops from Reichert’s cartilage of the second branchial arch during the fifth to sixth week. At the same time, The OW develops from a depression of the otic capsule during the seventh and ninth weeks. This depression forms the oval window (include annular ligament) and deep to the stapes footplate [3–6]. When the primitive stapes fails to fuse with the primitive vestibule, the oval window cannot develop, thereby resulting in its congenital absence [7, 8]. The facial bony canal coming from the otic capsule and the facial nerve tissue coming from the Reichert’s cartilage forms the fallopian canal during the tenth week. The developmental oval window, stapes, and facial nerve are clearly related both temporally and spatially. It is widely accepted that the displacement of the facial nerve may prevent the combination of the developing stapes and the underlying oval window [8, 9] (as cases 1, 4, 5, 7, and 8). In the Teunissen’s [1] Classification of congenital middle ear anomalies (Table 2), class 1 and class 2 include ears with congenital fixed stapes, class 4 with aplasia or severe dysplasia of the OW. In our study, class 4 represents deformity of the OW and facial nerve. This classification was based on the tympanic exploration. However, during surgery it is difficult to discriminate the atresia of OW coming from the otic capsule and the fixed footplate coming from the Reichert’s cartilage of the second branchial arch, as the Fig. 1b of case 1 in our paper (long black arrow). Regarding clinical surgery, the focus should be more on the pre-operative diagnosis. The coronal HRCT and the MPR post-processing technique provide us a practical method.
Pre-operative radiological diagnosis
Regarding the previous literature, the pre-operative diagnosis of the malformed OW is difficult and the exploratory tympanotomy is the only effective diagnosis method [10]. For the last decade, the HRCT and MPR post-processing technique has played an important role in the minor malformed structure pre-operatively. Zeifer et al. [7] reported the result of nine temporal bones in seven patients on high-resolution coronal CT scans. Seven ears showed complete lack of oval window formation and two showed partial absence of the oval window. Zeifer considered that the congenital absence of the oval window can be diagnosed on CT studies, especially on the coronal section. In horizontal section, Veillon et al. [11] considered whether the increased thickness of the footplate may be delineated in otosclerosis, chronic otitis media, malformation, when it measures 0.7 mm or more. Figure 2a of case 2 (No. 4) is the coronal CT, which shows a depressed atresia of OW and the low facial nerve without bony canal. Another radiological technique is the MPR (multi-planar reformation) imaging. This is a post-processing protocol. The imaging is created by reformation of the pixel with the result of showing total and fine ossicular chains within the same layer via multi-directional adjustment. Lane et al. [12] reported that the use of oblique planes of MPR can improved the CT diagnostic accuracy of the stapedial footplate-oval window complex. In comparison with the original 2D imaging, both resolution and contrasts are maintained [13, 14]. In showing OW and tapes, MPR imaging is more advantageous than the section plane [15]. Figure 1a of case 1 (No. 2) is an MPR imaging that shows the atresia of OW like a shape of “V” but no stapedial footplate. Figure 1c proved the atresia was a bony plate of vestibular, which was drilled out during the operation. The MPR imaging of Fig. 2b also indicated the thickened atresia plate more clearly than the coronal imaging of Fig. 2a. During the operation, the atresia plate was found to be the bony plate of vestibular but not the stapedal footplate (Fig. 2d), the thicken plate was approximately, 1 mm thick. Other cases (Nos. 1, 5, 7, and 8) are similar to case 1 (No. 2 see Table 1). Figure 4b of case 4 (No. 3) is MPR imaging that show an intact footplate (long black arrow). In the tympanic exploration, the footplate was found to be normal in shape but fixed. Regarding the cases we reported (class 4B, see Table 1), the radiological diagnosis of HRCT, especially the MPR imaging, can provide a practical and definite information for surgical treatment. In addition, these cases (class 4B cases) were all accompanied by a malformed facial nerve, which indicated malformation of OW as well, as Zeifer et al. [7] reported in his paper.
Surgical technique
The surgical treatment is difficult for the malformation of OW, especially in cases with malformed facial nerve. In the case with footplate fixation and facial nerve, no or partial covering the OW, the footplate can be mobilized with TORP implantation or drilled out with piston. However, it is unclear what occurs in cases when the facial nerve covers all of the OW or the footplate. The semicircular canal drill-out may be a choice but the hearing outcome is not satisfactory. Sterkers and Sterkers [16] reported a vestibular drilling technique with a satisfactory result. The fenestra was drilled above the facial never at the usual place of the Fallopian canal, just anterior to the ampulla of the lateral semicircular canal. A Teflon piston of either 0.6 or 0.4 mm was inserted in the vestibular cavity without traumatizing the utricule which is at 3 mm from the lateral wall of the vestibule. Plester [17] reported that in some cases, they encountered extreme difficulties in exposing the vestibule because of the overhanging facial nerve and the extremely narrow niche of the oval window, the promontorial window was created and the Guilford prosthesis hung from the handle of malleus was inserted into the vestibular scale. For the last years, Vibrant Soundbridge (VSB) implantation on the round window has been a new technique and may be a good choice [18–20]. Unlike Plester’s report about the placement of the piston through a promontory fenestra, we designed a new method of cochleostomy technique to reconstruct the hearing. The optimal fenestration located on the promontory wall (midpoint of the inferior margin of the oval window, anterior-inferior to the round window) for drilling to reach the bottom of the basal turn (case 3, Fig 3d). The bony of the hole was removed to the endosteum using a low-speed drill with a 1.0 mm diamond drill burr. Care was taken not to destroy the endosteum of the bony and the membranous labyrinth. When the fenestration had been created, a thin fascia was put on the bottom of fenestration, the distance from the tympanic membrane to the fascia was measured and an appropriate titanium-TORP was implanted between the tympanic membrane and the fenestration. Last, a small fat graft was used to seal around the bottom of TORP to prevent perilymph leak and a disc of cartilage was placed between the tympanic membrane and the top plate of TORP to prevent the extrusion of the prosthesis. The patient had no tinnitus, vertigo, and facial nerve paralysis. For our surgical technique, the position of the fenestration should be considered first. According to reports of Saunders and Fagan [21], the hole should be located at the midpoint of the inferior margin of the oval window and the distance from the inferior margin of the oval window to the superior margin of the hole should not exceed 0.3 mm in diameter to avoid damaging the spiral ligament and stria vascularis. Briggs et al. [22] reported that to avoid damage the basilar membrane and spiral ligament, the position of cochleostomy should be located at inferior, rather than anterior, to the round window to ensure scala tympani exploration. According to our experience in cochleostomy, if the fenestrated hole is located at anterior to the round window, the osseous spiral lamina and the scale vestibule can be seen sometimes. In case 3 in this paper, the cochlear structure covered by the endosteum should be the bottom of scala tympani and the spiral lamina located at the anterior part, but the cochlear structure was preserved well because of the entire endosteum.
Conclusion
Congenital absence or atresia of the oval window (OW), with or without malformed facial nerve is an uncommon embryologic defect. Preoperative diagnosis and surgical treatment is difficult. The coronal HRCT CT imaging and the MPR post-processing technique can provide us practical and definite information for surgical treatment, especially in the discrimination of OW atresia and the fixed stapedial footplate. The promontory drill-out technique, fenestration in the bottom of the scala tympani of the basal turn, provides us a new method in the hearing reconstruction when the OW was covered by a malformed facial nerve.
References
Teunissen EB, Cremers WR (1993) Classification of congenital middle ear anomalies: report on 144 ears. Ann Otol Rhinol Laryngol 102:606–612
(1995) Committee on Hearing and Equilibrium of guidelines for the evaluation of results of treatment of conductive hearing loss. American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc., Otolaryngol Head Neck Surg 113(3):186–187
Larsen WJ (1993) Development of the ears. In: Human embryology. Churchill Livingstone, New York, p 374
Strickland EM, Hanson JR, Anson BJ (1962) Branchial sources of auditory ossicles in man. I. Literature. Arch Otolaryngol 76:100–122
Hanson JR, Anson BJ, Strickland EM (1962) Branchial sources of the auditory ossicles in man. II. Observations of embryonic stages from 7 mm. to 28 mm. (CR length). Arch Otolaryngol 76:200–212
Mukerji SS, Parmar HA, Ibrahim M et al (2011) Congenital malformations of the temporal bone. Neuroimaging Clin N Am 21(3):603–619
Zeifer B, Sabini P, Sonne J (2000) Congenital absence of the oval window: radiologic diagnosis and associated anomalies. AJNR Am J Neuroradiol 21(2):322–327
Lambert PR (1990) Congenital absence of the oval window. Laryngoscope 100:37
Thomeer H, Kunst H, Verbist B et al (2012) Congenital oval or round window anomaly with or without abnormal facial nerve course: surgical results for 15 ears. Otol Neurotol 33(5):779–784
Su Y, Yuan H, Song YS et al (2014) Congenital middle ear abnormalities with absence of the oval window: diagnosis, surgery, and audiometric outcomes. Otol Neurotol 35(7):1191–1195
Veillon F, Riehm S, Emachescu B et al (2001) Imaging of the windows of the temporal bone. Semin Ultrasound CT MRI 22(3):271–280
Lane JI, Lindell EP, Witte RJ, De Lone DR, Driscoll CL (2006) Middle and inner ear: improved depiction with multiplanar reconstruction of volumetric data. Radiographics 26:115–124
Liu Y, Sun J, Guo Y et al (2014) Quality assessment of 3D-CTVR, MPR and section plane techniques in ossicular chain reconstruction in middle ear cholesteatoma. Comput Med Imaging Graph 38(8):696–701
Guo Y, Liu Y, Lu QH et al (2013) CT two-dimensional reformation versus three-dimensional volume rendering with regard to surgical findings in the preoperative assessment of the ossicular chain in chronic suppurative otitis media. Eur J Radiol 82(9):1519–1524 (Epub 1 May 2013)
Gong RZ, Chao BT, Liu K, Fan ZM, Wang HB, Chen QH et al (2004) CT multiplan reconstruction images of disorder of stapes. Zhonghua Er Bi Yan Hou Ke Za Zhi 39(5):265–268 (Chinese)
Sterkers JM, Sterkers O (1988) Surgical management of congenital absence of the oval window with malposition of the facial nerve. Adv Otorhinolaryngol 40:33–37
Plester D (1971) Congenital malformation of the middle ear. Acta Otorhinolaryngol Belg 25(6):877–884
ahrsdoerfer R (1980) Congenital malformations of the ear. Analysis of 94 operations. Ann Otol Rhinol Laryngol 89:348–352
Canale A, Dagna F, Cassandro C et al (2014) Oval and round window vibroplasty: a comparison of hearing results, risks and failures. Eur Arch Otorhinolaryngol 271(10):2637–2640
Zernotti ME, Arauz SL, Di Gregorio MF et al (2013) Vibrant Soundbridge in congenital osseous atresia: multicenter study of 12 patients with osseous atresia. Acta Otolaryngol 133(6):569–573
Saunders NC, Fagan PA (2006) Promontory drilling in stapedectomy: an anatomical study. Otol Neurotol 27(6):776–780
Briggs RJ, Tykocinski M, Stidham K et al (2005) Cochleostomy site: implications for electrode placement and hearing preservation. Acta Otolaryngol 125:870–876
Conflict of interest
All of the authors declare that they have no conflicts of interest concerning this article.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article

Cite this article
Yang, F., Liu, Y., Sun, J. et al. Congenital malformation of the oval window: experience of radiologic diagnosis and surgical technique. Eur Arch Otorhinolaryngol 273, 593–600 (2016). https://doi.org/10.1007/s00405-015-3597-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00405-015-3597-6