
Abstract
Purpose
During the second and the third trimesters of pregnancy and in the first 3 months following childbirth, about one-third of women experience urinary incontinence (UI). During pregnancy and after delivery, the strength of the pelvic floor muscles may decrease following hormonal and anatomical changes, facilitating musculoskeletal alterations that could lead to UI. Pelvic floor muscle training (PFMT) consists in the repetition of one or more sets of voluntary contractions of the pelvic muscles. By building muscles volume, PFMT elevates the pelvic floor and the pelvic organs, closes the levator hiatus, reduces pubovisceral length and elevates the resting position of the bladder. Objective of this review is to evaluate the efficacy of PFMT for prevention and treatment of UI during pregnancy and after childbirth and its effect on urinary system and supportive structures assessed by objective measurement techniques.
Methods
The largest medical information databases (Medline–Pubmed, EMBASE, Lilacs, Cochrane Library and Physiotherapy Evidence Database) were searched using the medical subject heading terms “pelvic floor muscle training”, “prevention”, “urinary incontinence”, “urinary stress incontinence”, “objective measurement techniques”, “pregnancy, “exercise”, “postpartum” and “childbirth” in different combinations.
Results and conclusions
Overall, the quality of the studies was low. At the present time, there is insufficient evidence to state that PFMT is effective in preventing and treating UI during pregnancy and in the postpartum. However, based on the evidence provided by studies with large sample size, well-defined training protocols, high adherence rates and close follow-up, a PFMT program following general strength-training principles can be recommended both during pregnancy and in the postnatal period.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Background
During the second and the third trimesters of pregnancy and in the first 3 months following childbirth, about one-third of women experience urinary incontinence (UI), which is the most common symptom associated with pelvic floor dysfunction [1]. During pregnancy and after delivery, the strength of the pelvic floor muscle (PFM) may decrease following hormonal and anatomical changes (both in the position of the pelvis and in the shape of the PFM), facilitating musculoskeletal alterations that could lead to UI. It is estimated that > 300% PFM strain is necessary for vaginal childbirth [2] and such effort exceeds the physiological limit that striated muscles can sustain, predisposing to muscles injuries. Indeed, several studies report that 20–26% of women show major injuries to the PFM after vaginal delivery (evaluated with ultrasound and MRI) [3,4,5]. Therefore, it seems plausible to compare vaginal delivery to a major sport injury. In the daily practice, more attention should be paid for prevention and treatment of its possible sequelae.
Urinary incontinence
According to the International Continence Society, UI is “a complaint of any involuntary leakage of urine” [6] and represents a common problem that deeply impacts the quality of life. The most common types of UI among women are:
-
(i)
stress urinary incontinence (SUI) unintentional urine leakage that happens when a physical movement or activity (e.g., sneezing, coughing, running, heavy lifting, childbirth) causes an increase in the abdominal pressure. Generally, it is caused by a loss of anatomical support of the urethrovesical junction (e.g., deficiency of the urethral sphincter, urethral hypermobility) (Fig. 1) and is the most commonly associated with pregnancy and postpartum period;
Fig. 1 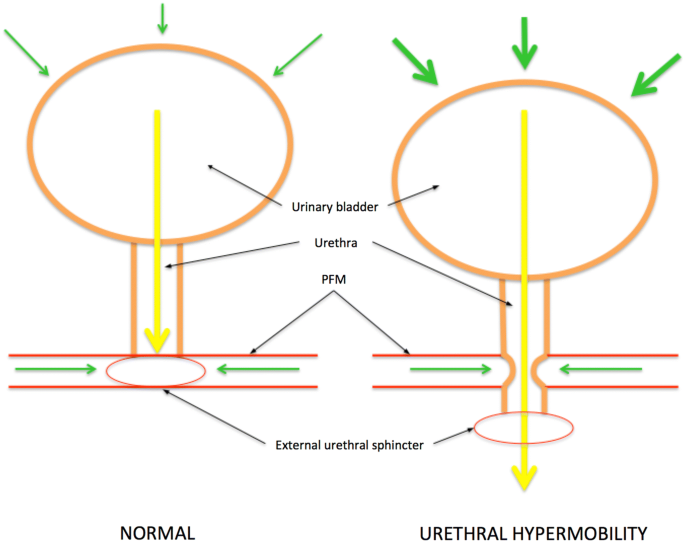
Urethral hypermobility refers to a condition that causes the urethra to drop below the pelvic floor muscles (PFM). When the support provided by the PFM is lost (e.g., after childbirth due to PFM damage), the bladder neck and the urethra may shift into a lower position, increasing the pressure on the bladder neck. If the pressure on the bladder exceeds the pressure on/in the urethra, leakage occurs
-
(ii)
urge urinary incontinence unintentional urine leakage usually associated with a sudden, strong need to void that can not be postponed. It is generally caused by an “overactive” bladder.

When patients experience both symptoms of stress and urge urinary incontinence, we face the condition that is called mixed urinary incontinence.
The prevalence of UI increases during pregnancy, especially in the second trimester, and gently decreases during the first postpartum year [7]. The overall prevalence (all types of UI) during pregnancy is estimated to be around 58% and SUI affects about 31–42% of women (nulliparous and multiparous) [8]. The percentage of persistence of UI in the first 3 months of the postpartum period is circa 30% [9]. Several factors are associated with postpartum UI, such as parity, age, maternal obesity, chronic lung disease, smocking, duration of the first and second stages of labor, type of delivery (spontaneous or operative), UI before or during pregnancy, high fetal weight and perineal trauma [10].
Effect of pregnancy, labor and type of delivery on PFM
The pathophysiology of UI during pregnancy, delivery and puerperium is multifactorial and still not fully defined. It involves hormonal changes, PFM and connective tissue modifications, bladder neck widening (due to the weight of both the uterus and the growing fetus) and anatomical injuries during delivery [11, 12]. Relaxin is a protein hormone which is produced during pregnancy. It is known to mediate the hemodynamic changes and to soften pelvic muscles and ligaments to prepare for delivery. Consequently, as the fetus grows and the uterus gains weight, PFM weakens [13]. In addition, constipation, which is a frequent complaint during pregnancy, may also increase the pressure on pelvic muscles [14]. During labor, PFM undergoes significant strain and the levator ani (the major muscle of the pelvic floor) has to distend at least five time its original size and to enlarge from 15–25 cm2 to 60–80 cm2, allowing the levator hiatus to widen during crowning [15].
A recent study conducted on animal models aimed to identify and quantify any architectural adaptations of PFM during pregnancy and to determine whether these changes occur also outside the pelvic floor. After harvesting pelvic muscles and tibialis anterior samples from mid- and late-pregnant rats and from 4- and 12-week postpartum rats, authors analyzed fiber length, physiologic cross-sectional area (typically used to determine the contraction properties of a muscle), sarcomere length and hydroxyproline content (for the evaluation of intramuscular collagen content). Changes in architectural design and an increase in collagen content were reported only in pelvic floor muscles. In particular, sarcomeres were added in series increasing fiber length. Hence, given the fact that muscle injury is generally related to excessive sarcomere strain, increased fiber length may represent a protective measure since the mechanical deformations that occur during parturition are distributed across a greater number of sarcomeres [16].
Although possible muscle adaptation, vaginal delivery represents a potential major risk factor for the onset of SUI and women who have had a vaginal delivery have a 2.5-fold increased risk when compared to those who had a cesarean section [17]. Several mechanisms may facilitate urine leakage (Fig. 2):

Effects of parturition on pelvic and urinary structures (B urinary bladder; V vagina, R rectum; PFM pelvic floor muscles)
-
(i)
perineal/pelvic injuries associated with vaginal delivery and prolonged abdominal pulling during fetal expulsion may be responsible for stretching and compression of the pelvic nerves, leading to ischemia, neurapraxia or compromised nerve function (pudendal nerve injury) [18];
-
(ii)
childbirth may weaken both the fascial structure and the connective tissue supporting the bladder neck and the urethra, promoting urethral hypermobility [19,20,21];
-
(iii)
any injuries of the levator ani during delivery may result in fibrosis and subsequentially may lead to a weakened pelvic floor [22].
Vacuum extraction, forceps delivery and perineal lacerations are all associated with pelvic floor disorders (including UI) up to 10 years after first delivery [23]. The effect of episiotomy in the prevention of postnatal UI, however, is still controversial [24]. In some countries, episiotomy represents a routine procedure, but in the majority of the cases, it is performed under obstetrical indication, such as fetal hypoxia and operative vaginal delivery (restricted approach). In a meta-analysis published in 2009, it was found that restricted episiotomy was associated with less perineal lacerations when compared to routine episiotomy, but no difference was found in the incidence of UI after delivery [25]. Similar results have been reported in other studies, which found no difference in UI and pelvic floor disorders incidence 3 months after delivery in primiparous women, suggesting that routine episiotomy does not protect against UI [26, 27]. On the other hand, Chang et al. [28] in a prospective study published in 2011 reported that the incidence of UI was significantly higher in women who had a vaginal delivery with episiotomy when compared to those who had a vaginal delivery without it. At the present time, there is no consensus on the possible protective role of elective/intrapartum cesarean delivery on long-term pelvic floor dysfunction. A recent systematic review on the impact of delivery route on pelvic floor disorders (including genital prolapse and UI) found that vaginal delivery is more likely to be associated with PFM injuries, increased bladder neck mobility and “ballooning” of the levator hiatus when compared to cesarean section [29].
Objective measurement techniques
Several authors tried to investigate the physiological changes of the bladder and the pelvic supportive structure during pregnancy through objective measurement techniques, but results are contradictory.
Urodynamic testing is not clinically useful during pregnancy because urinary symptoms generally begin early in pregnancy and do not correspond to urodynamic findings, but it may be helpful in identifying women who are more susceptible to postpartum pelvic floor disorders. Different investigators reported an increased bladder compliance (up to 1300 cc in the 8 month) and an increased bladder pressure at maximum capacity (ascribed to the enlarged uterus) in pregnant women studied with single- and multi-channel cystometry [30,31,32,33]. Pregnant women with SUI were found to have a reduced urethral length with lower closure pressure and diminished sphincter function at rest/stress when compared to continent pregnant women [32,33,34].
Perineal ultrasound (US) represents a simple, non-invasive, readily available and reproducible tool to evaluate bladder neck position and mobility, and it allows the evaluation of pelvic organs at rest and during straining. SUI is usually associated with post rotational descent of the proximal urethra and bladder neck hypermobility [35,36,37]. However, bladder neck mobility is also common in asymptomatic nonpregnant nulliparous women, with variable extent (from 4 to 32 mm during coughing and from 2 to 31 mm during Valsalva) [38]. The lack of an internationally accepted US definition for bladder neck hypermobility and the overlap between continent and incontinent US measurements represent major limitations in the use of perineal US in the diagnostic process. Several studies report that during pregnancy, the bladder neck is more caudal with increased mobility during Valsalva [34, 36, 39, 40]. King and Freeman reported that patients with postpartum SUI were more likely to have an increased mobility already antenatally when compared to continent postpartum women [35]. The same results were found by Dietz and Bennet, but no correlation with UI symptoms and US parameters was found [36]. In the study published by Pesschers and colleagues, both bladder neck position and mobility returned to antenatal values in most women at 6–10 weeks postpartum [39]. A widened resting angle of the bladder neck is another US feature that could be found during pregnancy. In the study published by Wijma et al. [41], the resting angle of the urethrovesical junction was already significantly increased at 12–16 weeks of pregnancy when compared to nonpregnant values (51.5° vs 44.5°) with further widening during pregnancy (up to 62°), indicating that the dynamic quality of the pelvic supportive structures is already weakened early in pregnancy. Notwithstanding, no correlation with UI was found.
2D and 3/4D translabial/transperineal US represents a highly valuable tool in evaluating levator ani function and morphology with good correlation with MRI in detecting major defects. Although it is a non-invasive, reproducible technique, carrying out the procedure requires a substantial learning curve. Increased hiatal area at rest and on Valsalva along with increased urethral mobility have been observed already in the third trimester of pregnancy by Sheck et al. [42].
Electrophysiologic tests Different studies used electromyography (EMG) and pudendal nerve terminal motor latency (PNTML) to evaluate possible neurogenic damages of PFM after delivery. EMG is generally used to asses the electrical activity of a striated muscle and PNTML measures the nerve conduction and allows the identification of pudendal nerve damage. It is well known that labor and vaginal delivery may cause partial denervation of the pelvic floor, especially in women delivering their first baby [43]. Different studies have observed an increased PNTML after childbirth, which was significantly associated with increased duration of the second stage of labor and high birth weight (> 4 kg), but not with forceps or vacuum delivery [44]. In the study published by Tetzschner et al., PNTML measurements were significantly increased in women with UI and a significant association with vacuum extraction was observed. No association was found with duration of the second stage of labor, birth weight, head circumference and epidural analgesia [45].
Pelvic floor muscle training (PFMT)
Pelvic floor muscle training (PFMT) consists in the repetition of one or more sets of voluntary contractions of the pelvic muscles. Frequency, intensity and progression of the exercises vary, depending on the protocol. At the present time, no standardized PFMT protocol exists. Generally, in a typical PFMT program, more sets of exercises are performed on different days of the week, for at least 6–8 weeks and after this initial phase, a maintenance program should be recommended to ensure long-term effects [46, 47]. The rationale of PFMT in the prevention/treatment of UI lay on several reasons. By building muscles volume, PFMT elevates the PFM and the pelvic organs, closes the levator hiatus, reduces pubovisceral length and elevates the resting position of the bladder. All this morphological changes contribute to improve the structural support of the pelvic floor and, during pregnancy, help in counteracting the increased intra-abdominal pressure caused by the developing fetus. In addition, a trained muscle besides being less prone to injury, has generally a greater reserve of strength so that injury to the muscle itself, or its nerve supply, does not cause sufficient loss of muscle function to reach the threshold where reduced urethral closure pressure results in leakage. Moreover, when damaged, it might be easier to retrain as the neural adaptation and the motor learning have already been assimilated [46]. PFMT may be delivered to women for both prevention and treatment of UI and may be started both during pregnancy and after childbirth.
Materials and methods
The largest medical information databases (Medline–Pubmed, EMBASE, Lilacs, Cochrane Library and Physiotherapy Evidence Database) were searched using the Medical Subject Heading (MeSH) terms “pelvic floor muscle training”, “prevention”, “urinary incontinence”, “urinary stress incontinence”, “objective measurement techniques”, “pregnancy, “exercise”, “postpartum” and “childbirth” in different combinations. The searches were updated regularly (date of last search: August 2018). Both meeting abstracts and full-length papers were included and the relative reference lists were systematically searched. After duplicates removal, the database searches resulted in 839 references. 124 articles were assessed for eligibility after the exclusion of some studies based on title, abstract and inclusion criteria and 41 papers were included in the study (Fig. 3). Recently, a Cochrane review on PFMT for prevention and treatment of urinary and fecal incontinence has been published [10]. Consequently, no meta-analysis was performed and only a narrative summary of results concerning antenatal and postnatal PFMT for prevention and treatment of UI is provided.

Flowchart of the search strategy
Results
PFMT during pregnancy
Twenty-five studies on PFMT started during pregnancy were identified. Ten trials were focused on the role of PFMT in the prevention of UI [48,49,50,51,52,53,54,55,56,57], four on the role of PFMT in the treatment of UI [58,59,60,61] and 11 both in the prevention and in the treatment of UI [48, 51, 62,63,64,65,66,67,68,69,70].
Concerning the first group of studies, continent pregnant women (both nulliparous and multiparous) were enrolled and PFMT was started at different weeks of gestation, ranging from 14 to 30 weeks of gestation. Different PFMT programs were followed with a significant heterogeneity in length, intensity and frequency of the training period (Table 1). Patients randomized to PFMT group were 62% less likely to experience UI in late pregnancy and in the early postpartum period, and were less likely to report UI 3–6 months after delivery [10]. Seven studies evaluated the severity of UI (episodes of UI, amount of urine leakage) and, although the high variability in the choice of measure, a general trend of a positive effect of PFMT was found [48,49,50, 52, 54, 56, 57]. In three studies, authors evaluated the continence of patients in late pregnancy and in the early postpartum period through a stress test (positive cough or pad test) and women randomized to PFMT were more likely to be continent when compared to the control group [50, 52, 55]. Concerning the long-term effect of PFMT, two studies evaluated continence at > 5 years and no difference was found in UI prevalence rate [50, 51], suggesting that PFMT is probably not effective at long term. However, these data could also be explained by subsequent pregnancies, stop in the exercises or, as shown in the study published by Morkved, women were performing similar PFMT protocols regardless of which group they had initially been randomized [51]. Only one study reported a general improvement in quality of life in the PFMT group [56].
The role of PFMT in the treatment of UI was evaluated in four studies [58,59,60,61]. In all studies, pregnant incontinent women were included (primiparous [60], multiparous [59], not stated [58, 61]). Also in this group of patients, PFMT protocols and follow-up intervals varied (Table 2). No difference was found in the prevalence of UI both in the early and in the late postnatal period [10]. Concerning the quality of life, only Cruz el al. [61] found an improvement in the PFMT group in late pregnancy.
Eleven trials reported PFMT for both prevention and treatment of UI during pregnancy [48, 51, 62,63,64,65,66,67,68,69,70]. Pregnant women with and without UI were recruited at different weeks of gestation (from 18 to 42 weeks of pregnancy). Different PFMT protocols were followed (Table 3). Overall, patients randomized to the PFMT group had a 26% lower risk to report UI in late pregnancy [10]. In the early and mid-postpartum periods, a significant difference in UI prevalence was found, favoring the PFMT group when compared to the control group. No difference was found in the late postnatal period [10]. Ko et al. [65] reported a statistically significant improvement in quality of life in the PFMT group at different time points (late pregnancy, mid- and late-postpartum). On the other hand, two other studies found no difference [63, 70]. Only one trial used the pad test to evaluate continence after PFMT and no difference was found between the two groups [70]. In addition, the PFMT group was shown not to be superior to the usual care group in terms of symptoms improvement: no differences were found at 3 and 12 months postpartum in frequency and amount of urine leakage [48, 62].
PFMT after childbirth
Fifteen studies on PFMT begun after childbirth were identified: five on the role of PFMT in the treatment of UI [71,72,73,74,75] and ten on the possible effect of PFMT on both prevention and treatment of UI in the postpartum period [76,77,78,79,80,81,82,83,84,85].
Concerning the role of PFMT in the treatment of UI in the postnatal period, the training was started 3 months or more after childbirth in all studies. Only incontinent women at 3 months or more after delivery were enrolled. Both primiparous and multiparous women were included. Different PFMT protocols were followed (Table 4). Postnatal PFMT was compared to standard discharge recommendations (including or not general information about PFMT) in all studies, except for two: Dumoulin et al. [73] introduced eight sessions of weekly relaxation massage in the control group and Kim et al. [74] allowed an 8-week unsupervised training. Patients randomized to PFMT group were less likely (about 22%) to experience UI symptoms in the late postnatal period (up to 12 months after delivery) [10]. A general reduction in severity of symptoms and episodes of UI was found, but given the different methods used to evaluate and report these, a solid statement can not be made [10]. Glazener et al. [72] reported a significant improvement in UI-related anxiety, but found no difference in the incidence of UI at 6-year follow-up. Regarding the quality of life, Dumoulin et al. [73] reported a significant improvement in the PFMT group, whereas Kim et al. [74] found no difference between the two groups.
Ten trials on the role of PFMT in both prevention and treatment of UI in the postnatal period were identified. In all studies, continent and incontinent women after spontaneous vaginal delivery were recruited. Chiarelli and Cockburn included only women who had an operative delivery (forceps or ventouse), or with fetal macrosomia (≥ 4000 g) (high-risk population for postpartum UI) [78]. Different PFMT protocols were followed (Table 5), but in three studies, no details were given concerning the training program [76, 77, 79]. In all studies, the control group received conventional discharge recommendations (including or not general information about PFMT), except in the study of Meyer et al. [77] where controls were specifically asked not to perform PFMT. No difference was found in UI prevalence up to 6 and 12 months after delivery [10]. Regarding frequency and amount of urine leakage, Sleep et al. [76] found no difference at 3 months postpartum between the two groups, whereas Liu et al. [81] reported less severe UI symptoms in the PFMT group. To evaluate continence during follow-up, some studies used the pad test: Hilde et al. [82] found no difference between the two groups at 6-month follow-up, whereas Wen et al. [80] reported that women randomized to PFMT group were less likely to be incontinent at 12-month follow-up.
Effect of PFMT on the urinary tract and on the pelvic supportive structure assessed by objective measurement techniques
Only few studies have investigated the effect of PFMT on the urinary tract and on the pelvic supportive structure by using objective measurement techniques.
In the study published by King and Freeman [35], 106 healthy nulliparous women were recruited antenatally for the evaluation of bladder neck mobility during pregnancy and in the postpartum period. A frequent US finding in the postnatal period is an increased mobility of the bladder neck with an increased angle of rotation at Valsalva. From the first visit at approximately 15–17 weeks, patients were regularly seen every 10 weeks during pregnancy with the last visit at 10–14 weeks postpartum. At each appointment, a perineal US was performed, to measure bladder volume and to evaluate bladder neck movement and rotation at rest and at Valsalva (which was standardized by using a modified sphygmomanometer). During the last visit, data on performance and frequency of postnatal pelvic floor exercises (PFEs) were recorded (“daily PFEs” = > 10 PFEs/day; “sometimes PFEs” = > 10 PFEs 2–3 times/week; “no PFEs” = less frequent than the previous). Persistent occasional SUI after delivery was reported in 18.4% of patients and de novo postpartum SUI in 3.9%, where women who performed postnatal PFEs were less likely to be incontinent (p = 0.02). The positive effect of postnatal PFEs on continence was even stronger in patients with antenatal bladder rotation > 10° at Valsalva (p = 0.003).
Another study which evaluated the effect of PFMT on bladder neck was recently published by Lekskulchai et al. [86]. In this case, PFMT was performed during pregnancy. 219 pregnant nulliparous women were enrolled and divided into two groups: 108 were randomized for antenatal PFMT (15 contractions, held for 5 s, performed three times after each meal) and 111 received routine antenatal care (control group). Patients were seen two times during pregnancy (second and third trimester) and two times in the postpartum period (at 3 and 6 months postpartum). At each visit, a transperineal US was performed to evaluate bladder neck position at rest and at Valsalva. Although, no significant difference between the two groups was found concerning urinary symptoms both during pregnancy and in the last postpartum visit, at 6 months postpartum the control group showed a greater bladder neck descent when compared to the intervention group (p = 0.003). In addition, in the subgroup of patients who had a vaginal delivery, the bladder neck descent was even greater in the control group when compared to women who regularly performed PFMT (p = 0.006).
In the study conducted by Dornowski et al. [87], 113 healthy pregnant women with and without SUI were recruited. Patients were divided into three groups: symptomatic women who underwent PFMT (group 1), asymptomatic women who underwent PFMT (group 2) and asymptomatic women without training (group 3). Group-supervised exercise sessions were held three times/week for 6 weeks and included a warm-up phase, an aerobic part with music, strength conditioning exercises and isolated PFM exercises. A surface EMG was performed before and after the 6-week training program. Three EMG measurements were taken: quick flicks (Q), static contractions (STA) and BASE/REST baselines before measurement and after 10-s contractions. Group 1 registered in most of the measured parameters the lowest values of PFM electrical activity but, during Q, group 1 showed the highest increase after training. If we consider that the electrical activity registered during Q reflects the ability of holding urine and/or stopping urine in case of increased intra-abdominal pressure (e.g., sneezing, coughing, running, heavy lifting, etc.), we can assume that PFMT improved the efficiency of PFM contraction.
Discussion
The use of PFMT in the treatment of UI in symptomatic women was first described by Kegel in 1948 [88]. PFMT protocols generally include five stages, all of them being essential and consequential: (i) information, (ii) posture correction, (iii) awareness stage and proprioceptive neuromuscular facilitation, (iv) strengthening programs and (v) perineal blockage before stress [89]. When to start it, how to perform it and by whom PFMT should be given represent three major variables that increase the heterogeneity of the findings and strongly impact the quality of the evidence.
PFMT could be recommended for primary, secondary or tertiary prevention. Primary prevention is done by preventing exposure to hazards and by increasing resistance to diseases or injuries before they occur. Secondary prevention aims to reduce the impact of a disease or injury that has already occurred, by detecting and treating it as soon as possible. Tertiary prevention consists of the treatment of symptoms of an on-going illness or injury that has lasting effects [90]. In the case of UI, given its multifactorial aetiology (compromised neural function, weakened PFM, decreased fascial support), it may be impractical to screen all patients to establish if the disease process is either absent or present, but still asymptomatic and in addition to that, at the present time, some clinical tests have still limited validity. Hence, especially in asymptomatic patients, the obtained results may be a combination of primary and secondary prevention effects. When to start a training protocol and to whom should offer it, still remain two highly debated topics. The 2017 Cochrane review concluded that antenatal PFMT in continent women may help in preventing the onset of UI in late pregnancy and postpartum. The efficacy of PFMT (both antenatal and postnatal) in treating UI remains uncertain [10].
Another specific problem when analyzing the effect of PFMT on UI is the high variability in training protocols, which are also often poorly described. In addition, the lack of a standardized PFMT protocol represents a major limitation to the transferability of study results. Indeed, intensity, frequency and type of exercise are the main factors which will set the effect size [91]. Several trials [50,51,52, 60, 65, 67, 73] follow the same PFMT protocol proposed by Bo et al. [92]. The authors suggest an “intensive training” that consists in the repetition of three sets of ten contractions at maximum intensity, held for 6 s, 3–4 times/week, which follows the general recommendations for strength training to increase the cross-sectional area of a muscle [93]. This type of protocol has been proven to be effective in reducing genital organs prolapse, too. Indeed, it builds muscle volume and thickness, reduces muscle length, closes the levator hiatus and elevates the resting position of the bladder and consequently also lifts the position of the bladder neck [94]. In different studies on PFMT effects, protocols with 1 weekly supervised session were considered intensive. However, if we consider that athletes who suffered major sport injuries are offered at least 2–3 physiotherapy sessions/week, the attention that is paid to PFM training appears suboptimal. In addition, low-dosage training may be a major reason for dropouts especially in patients who did not achieve satisfactory results and consequently are not motivated for new training periods at optimal dosage. Behavioral support is another aspect that should be taken into account when starting PFMT to ensure adherence, especially if the training protocol implies home exercises. Different adherence support strategies were mentioned in different studies (worksheets and exercise booklets, phone calls, individual tailoring and supervision, group setting), but only nine studies provided data about exercise behavior among patients included in both PFMT and control group [50, 51, 59, 64, 67, 70, 76, 78, 82]. Event if the collection of adherence data in both intervention and control groups could attenuate the difference between the two by changing the exercise behavior, it may also reduce the dropout rates in both groups.
A great heterogeneity was also found in the professional figure that provided the information about PMFT and supervised the training. Physiotherapists, nurses, midwives, obstetricians and general practitioners were generally involved, but no comparison was made between the effects of interventions given by different professionals.
Another topic of debate when discussing the benefits of PMFT is a possible lack of long-term effects. Few studies investigated the effect of PMFT over the years and all failed to demonstrate any benefit of PFMT when compared to the control group [48, 50, 51]. As any training program, it is plausible that its effect will decrease in time if not continued or if not followed by a maintenance program. Generally, muscle strength diminishes at a slower rate than that at which strength is gained through exercise. In a study published in 2004, it was shown that after cessation of exercising, muscle strength decreases by about 5–10% per week and this rate strictly depends on intensity and length of the training period [95]. An effective maintenance training protocol to slow down strength loss usually reduces frequency and volume of the exercises, but preserves the intensity of the previous training [96]. To date, no studies have investigated the minimum training that is necessary to maintain PFM strength after childbirth.
The paucity of studies which assessed the efficacy of PFMT through objective measurement techniques represents also another great limitation. As stated before, several tests still have reduced validity especially when performed during pregnancy, making the evaluation of PFMT effectiveness even harder.
Conclusions
Overall, the quality of the studies was low, mostly owing to poor reporting measurements, different training protocols and dosage in both interventional and control groups (in many cases usual care included also general information about PFMT) and small sample size (which may cause type two error). At the present time, there is insufficient evidence to state that PFMT is effective in preventing and treating UI in late pregnancy and in the postpartum. However, based on the evidence provided by studies with large sample size, well-defined training protocols, high adherence rates and close follow-up, a PFMT program following general strength-training principle like the one proposed by Bo et al. [92] can be recommended both during pregnancy and in the postnatal period. In addition, given the detrimental effect of PFM dysfunction on quality of life, more high-quality randomized controlled trials on the topic are needed and should represent a high priority in the field of urogynecology.
References
Swift SE (2000) The distribution of pelvic organ support in a population of female subjects seen for routine gynecologic health care. Am J Obstet Gynecol 183:277–285
Hoyte L, Damaser MS, Warfield SK et al (2008) Quantity and distribution of levator ani stretch during simulated vaginal childbirth. Am J Obstet Gynecol 199:198.e1–198.e5
DeLancey JO, Kearney R, Chou Q et al (2003) The appearance of levator ani muscle abnormalities in magnetic resonance images after vaginal delivery. Obstet Gynecol 101:46–53
DeLancey JOL, Low LK, Miller JM et al (2008) Graphic integration of causal factors of pelvic floor disorders: an integrated life span model. Am J Obstet Gynecol 199:610.e1–610.e5
Dietz PH, Lanzarone V (2005) Levator trauma after vaginal delivery. Obstet Gynecol 106:707–712
Abrams P, Cardozo L, Fall M et al (2003) The standardization of terminology of lower urinary tract function: report from the standardization sub-committee of the International Continence Society. Urology 61:37–49
Abrams P, Cardozo L, Wagg A, Wein A (eds) (2017) Incontinence, 6th edn. ICI-ICS, International Continence Society, Bristol, UK
Wesnes SL, Rortveit G, Bø K et al (2007) Urinary incontinence during pregnancy. Obstet Gynecol 109:922–928
Thom DH, Rortveit G (2010) Prevalence of postpartum urinary incontinence: a systematic review. Acta Obstet Gynecol Scand 89:1511–1522
Woodley SJ, Boyle R, Cody JD et al (2017) Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database Syst Rev 12:CD007471
Sievert KD, Amend B, Toomey PA et al (2012) Can we prevent incontinence? ICI-RS 2011. Neurourol Urodyn 31:390–399
Herbert J (2009) Pregnancy and childbirth: the effects on pelvic floor muscles. Nurs Times 105:38–41
Day J, Goad K (2010) Recovery of the pelvic floor after pregnancy and childbirth. Br J Midwifery 18:51–53
Marshall K, Thompson K, Walsh D et al (1998) Incidence of urinary incontinence and constipation during pregnancy and post-partum: survey of current findings at the Rotunda Lying-in hospital. Br J Obstet Gynaeco 105:400–402
Svabik K, Shek K, Dietz H (2009) How much does the levator hiatus have to stretch during childbirth? BJOG 116:1657–1662
Alperin M, Lawley DM, Esparza MC et al (2015) Pregnancy-induced adaptations in the intrinsic structure of rat pelvic floor muscles. Am J Obstet Gynecol 213:191.e1–191.e7
Rortveit G, Daltveit AK, Hannestad YS et al (2003) Urinary incontinence after vaginal delivery or cesarean section. N Engl J Med 348:900–907
Smith ARB, Hosker GL, Warrell DW (1989) The role of pudendal nerve damage in the aetiology of genuine stress incontinence of urine in women. BJOG 96:29–32
Peschers U, Schaer G, Anthuber C et al (1996) Changes in vesical neck mobility following vaginal delivery. Obstet Gynecol 88:1001–1006
Falconer C, Blomgren B, Johansson O et al (1998) Different organization of collagen fibrils in stress-incontinent women of fertile age. Acta Obstet Gynecol Scand 77:87–94
Norton PA (1993) Pelvic floor disorders: the role of fascia and ligaments. Clin Obstet Gynecol 36:926–938
Dimpfl T, Jaeger C, Muelller-Felber W et al (1998) Myogenic changes of the levator ani muscle in premenopausal women: the impact of vaginal delivery and age. Neurourol Urodyn 17:197–205
Handa VL, Blomquist JL, McDermott KC et al (2012) Pelvic floor disorders after vaginal birth: effect of episiotomy, perineal laceration, and operative birth. Obstet Gynecol 119:233–239
Hartmann K, Viswanathan M, Palmieri R et al (2005) Outcomes of routine episiotomy: a systematic review. JAMA 293:2141–2148
Carroli G, Mignini L (2009) Episiotomy for vaginal birth. Cochrane Database Syst Rev 1:1
Klein MC, Gauthier RJ, Jorgensen SH et al (1992) Does episiotomy prevent perineal trauma and pelvic floor relaxation? Online J Curr Clin Trials. Doc No 10
Sartore A, De Seta F, Maso G (2004) The effects of mediolateral episiotomy on pelvic floor function after vaginal delivery. Obstet Gynecol 103:669–673
Chang SR, Chen KH, Lin HH et al (2011) Comparison of the effects of episiotomy and no episiotomy on pain, urinary incontinence, and sexual function 3 months postpartum: a prospective follow-up study. Int J Nurs Stud 48:409–418
de Araujo CC, Coelho SA, Stahlschmidt P et al (2018) Does vaginal delivery cause more damage to the pelvic floor than cesarean section as determined by 3D ultrasound evaluation? A systematic review. Int Urogynecol J 29:639–645
Muellner SR (1939) Physiological bladder changes during pregnancy and the puerperium. J Urol 41:691–695
Iosif S, Ingemarsson I, Ulmsten U (1980) Urodynamic studies in normal pregnancy and in puerperium. Am J Obstet Gynecol 137:696–700
Iosif S, Ulmsten U (1981) Comparative urodynamic studies of continent and stress incontinent women in pregnancy and in the puerperium. Am J Obstet Gynecol 140:645–650
Van Geelen JM, Lemmens WAJG et al (1982) The urethral pressure profile in pregnancy and after delivery in healthy nulliparous women. Am J Obstet Gynecol 144:636–649
Meyer S, Bachelard O, DeGrandi P (1998) Do bladder neck mobility and urethral sphincter function differ during pregnancy compared with during the nonpregnant state. Int Urogynecol J Pelvic Floor Dysfunct 9:397–404
King JK, Freeman RM (1998) Is antenatal bladder neck mobilty a risk factor for postpartum stress incontinence. Br J Obstet Gynaecol 105:1300–1307
Dietz HP, Bennett MJ (2003) The effect of childbirth on pelvic organ mobility. Obstet Gynecol 102:223–228
Jundt K, Scheer L, Schiessl B et al (2010) Incontinence, bladder neck mobility, and sphincter ruptures in primiparous women. Eur J Med Res 15:246–252
Reed H, Freeman RM, Waterfield A et al (2004) Prevalence of bladder neck mobility in asymptomatic nonpregnant nulliparous volunteers. Br J Obstet Gynaecol 111:172–175
Pesschers UM, Schaer G, DeLancey J et al (1997) Levator ani function before and after childbirth. Br J Obstet Gynaecol 104:1004–1008
Toozs-Hobson P, Balmforth J, Cardozo L et al (2008) The effect of mode of delivery on pelvic floor functional anatomy. Int Urogynecol J 19:407–416
Wijma J, Weis-Potters AE, de Wolf BTHM et al (2003) Anatomical and functional changes in the lower urinary tract following spontaneous vaginal delivery. Br J Obstet Gynaecol 110:658–663
Shek KL, Kruger J, Dietz HP (2012) The effect of pregnancy on hiatal dimensions and urethral mobility: an observational study. Int Urogynecol J 23:1561–1567
Allen RE, Hosker GL, Smith AR et al (1990) Pelvic floor damage and childbirth: a neurophysiological study. Br J Obstet Gynaecol 97:770–779
Sultan AH, Kamm MA, Hudson CN (1994) Pudendal nerve damage during labor: prospective study before and after childbirth. Br J Obstet Gynaecol 101:22–28
Tetzschner T, Sorensen M, Jonnson L, Lose G, Christansen J (1997) Delivery and pudendal nerve function. Acta Obstet Gynecol Scand 76:324–331
Bø K (2004) Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct 15:76–84
Mørkved S, Bø K (2014) Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: a systematic review. Br J Sports Med 48:299–310
Sampselle CM, Miller JM, Mims BL et al (1998) Effect of pelvic muscle exercise on transient incontinence during pregnancy and after birth. Obstet Gynecol 91:406–412
Stothers L (2012) A randomized controlled trial to evaluate intrapartum pelvic floor exercise as a method of preventing urinary incontinence (Abstract). J Urol 167(4 Suppl):106
Reilly ETC, Freeman RM, Waterfield MR et al (2002) Prevention of postpartum stress incontinence in primigravidae with increased bladder neck mobility: a randomised controlled trial of antenatal pelvic floor exercises. BJOG 109:68–76
Mørkved S, Bø K, Schei B et al (2003) Pelvic floor muscle training during pregnancy to prevent urinary incontinence: a single-blind randomized controlled trial. Obstet Gynecol 101(2):313–319
Gorbea Chavez V, Velazquez Sanchez MdP, Kunhardt Rasch JR (2004) Effect of pelvic floor exercise during pregnancy and puerperium on prevention of urinary stress incontinence [Efecto de los ejercicios del piso pelvico durante el embarazo y el puerperio en la prevencion de la incontinencia urinaria de esfuerzo]. Ginecol Obstet Mex 72:628–636
Gaier L, Lamberti G, Giraudo D (2010) Pelvic floor muscle training during pregnancy to prevent urinary pelvic floor dysfunctions (Abstract). Neurourol Urodyn 29:64–65
Barakat R, Pelaez M, Montejo R et al (2011) Exercise during pregnancy improves maternal health perception: a randomized controlled trial. Am J Obstet Gynecol 204:402.e1–402.e7
Kocaoz S, Eroglu K, Sivaslioglu AA (2013) Role of pelvic floor muscle exercises in the prevention of stress urinary incontinence during pregnancy and the postpartum period. Gynecol Obstet Invest 75:34–40
Pelaez M, Gonzalez-Cerron S, Montejo R et al (2014) Pelvic floor muscle training included in a pregnancy exercise program is effective in primary prevention of urinary incontinence: a randomized controlled trial. Neurourol Urodyn 33:67–71
Sangsawang B, Sangsawang N (2016) Is a 6-week supervised pelvic floor muscle exercise program effective in preventing stress urinary incontinence in late pregnancy in primigravid women?: a randomized controlled trial. Eur J Obstet Gynecol Reprod Biol 197:103–110
Skelly J, Rush J, Eyles P, et al (2004) Postpartum urinary incontinence: regional prevalence and the impact of teaching pelvic muscle exercises to pregnant women with UI (Abstract number 552). In: 34th Annual Meeting of the International Continence Society and the International Urogynecology Association, Paris
Woldringh C, van den Wijngaart M, Albers-Heitner P et al (2007) Pelvic floor muscle training is not effective in women with UI in pregnancy: a randomised controlled trial. Int Urogynecol J Pelvic Floor Dysfunct 18:383–390
Dinc A, Kizilkaya Beji N, Yalcin O (2009) Effect of pelvic floor muscle exercises in the treatment of urinary incontinence during pregnancy and the postpartum period. Int Urogynecol J Pelvic Floor Dysfunc 20:1223–1231
Cruz C, Riesco ML, Zanetti M (2014) Supervised pelvic floor muscle training to treat urinary incontinence during pregnancy: a randomized controlled trial (Abstract number 403). Neurourol Urodyn 33:867–868
Hughes P, Jackson S, Smith P et al (2011) Can antenatal pelvic floor exercises prevent postnatal incontinence (Abstract). Neurourol Urodyn 20:447–448
Dokmeci F, Bayramov S, Tur BS et al (2008) Pelvic floor muscle training during pregnancy: a randomized single-blind controlled study on improvement of antenatal and postpartum lower urinary tract symptoms (Abstract). J Pelvic Med Surg 14:304
Bø K, Haakstad LA (2011) Is pelvic floor muscle training effective when taught in a general fitness class in pregnancy? A randomised controlled trial. Physiotherapy 97:190–195
Ko PC, Liang CC, Chang SD et al (2011) A randomized controlled trial of antenatal pelvic floor exercises to prevent and treat urinary incontinence. Int Urogynecol J 22:17–22
Frumenzio E, Giovannozzi S, Pietropaolo A et al (2012) Results of a prospective randomised study: role of pelvic-perineal rehabilitation in post-partum incontinence recovery (Abstract number 4). Neurourol Urodyn 31(S1):S3
Stafne S, Salvesen K, Romundstad P et al (2012) Does regular exercise including pelvic floor muscle training prevent urinary and anal incontinence during pregnancy? A randomised controlled trial. BJOG Int J Obstet Gynaecol 119:1270–1280
Miquelutti MA, Cecatti JG, Makuch MY (2013) Evaluation of a birth preparation program on lumbopelvic pain, urinary incontinence, anxiety and exercise: a randomized controlled trial. BMC Pregnancy Childbirth 13:154
Assis LC, Bernardes JM, Barbosa AM et al (2015) Effectiveness of an illustrated home exercise guide on promoting urinary continence during pregnancy: a pragmatic randomized clinical trial (Portuguese). Rev Bras Ginecol Obstet 37:460–466
Fritel X, de Tayrac R, Bader G et al (2015) Preventing urinary incontinence with supervised prenatal pelvic floor exercises: a randomized controlled trial. Obstet Gynecol 126:370–377
Wilson PD, Herbison GP (1998) A randomized controlled trial of pelvic floor muscle exercises to treat postnatal urinary incontinence. Int Urogynecol J Pelvic Floor Dysfunct 9:257–264
Glazener CM, Herbison GP, Wilson PD et al (2001) Conservative management of persistent postnatal urinary and faecal incontinence: a randomised controlled trial (Extended electronic version). BMJ 323:1–5
Dumoulin C, Lemieux MC, Bourbonnais D et al (2004) Physiotherapy for persistent postnatal stress urinary incontinence: a randomized controlled trial. Obstet Gynecol 104:504–510
Kim EY, Kim SY, Oh DW (2012) Pelvic floor muscle exercises utilizing trunk stabilization for treating postpartum urinary incontinence: randomized controlled pilot trial of supervised versus unsupervised training. Clin Rehabil 26:132–141
Ahlund S, Nordgren B, Wilander EL et al (2013) Is home-based pelvic floor muscle training effective in treatment of urinary incontinence after birth in primiparous women? A randomized controlled trial. Acta Obstet Gynecol Scand 92:909–915
Sleep J, Grant A (1987) Pelvic floor exercises in postnatal care. Midwifery 3(4):158–164
Meyer S, Hohlfeld P, Achtari C et al (2001) Pelvic floor education after vaginal delivery. Obstet Gynecol 97:673–677
Chiarelli P, Cockburn J (2002) Promoting urinary continence in women after delivery: randomised controlled trial (extended electronic version). BMJ 324:1–6
Ewings P, Spencer S, Marsh H et al (2005) Obstetric risk factors for urinary incontinence and preventative pelvic floor exercises: cohort study and nested randomized controlled trial. J Obstet Gynaecol 25:558–564
Wen X-H, Shi S-Q, Wang J-Y (2010) Pelvic muscles exercise for postpartum stress urinary incontinence. China Pract Med 5:72–73
Liu X-B (2011) Pelvic floor muscle training for prevention and treatment of postpartum urinary incontinence clinical observation. Guide China Med 9:21–22
Hilde G, Stær-Jensen J, Siafarikas F et al (2013) Postpartum pelvic floor muscle training and urinary incontinence: a randomized controlled trial. Obstet Gynecol 122:1231–1238
Kou J-L, Dang L-J, Feng X-Q (2013) Clinical study on the treatment of postpartum rehabilitation to improve the pelvic floor function. Med Innov China 10:55–57
Peirce C, Murphy C, Fitzpatrick M et al (2013) Randomised controlled trial comparing early home biofeedback physiotherapy with pelvic floor exercises for the treatment of third-degree tears (EBAPT trial). BJOG 120:1240–1247
Frost A, Trankel D, Shannon M (2014) The efficacy of written and verbal pelvic floor exercise discharge instructions in reducing urinary incontinence among postpartum patients (Abstract). J Womens Health Phys Ther 38:40
Lekskulchai O, Wanichsetakul P (2014) Effect of pelvic floor muscle training (PFMT) during pregnancy on bladder neck descend and delivery. J Med Assoc Thail 97:S156–S163
Dornowski M, Sawicki P, Wilczyńska D et al (2018) Six-week pelvic floor muscle activity (sEMG) training in pregnant women as prevention of stress urinary incontinence. Med Sci Monit 24:5653–5659
Kegel AH (1948) Progressive resistance exercise in the functional restoration of the perineal muscles. Am J Obstet Gynecol 56:238–248
Bourchier AP, Dentz JP, Grosse D (1999) Aims of pelvic floor rehabilitation, selection of patients. In: Appell RA, Bourchier AP, La Torre F (eds) Pelvic floor dysfunction Investigations & conservative treatment. Casa Editrice Scientifica Internazionale, Rome, pp 201–210
Hensrud DD (2000) Clinical preventive medicine in primary care: background and practice: 1. Rationale and current preventive practices. Mayo Clin Proc 75:165–172
Imamura M, Abrams P, Bain C et al (2010) Systematic review and economic modelling of the effectiveness and cost-effectiveness of non-surgical treatments for women with stress urinary incontinence. Health Technol Assess 14:1–188
Bø K, Hagen RH, Kvarstein B et al (1990) Pelvic floor muscle exercise for the treatment of female stress urinary incontinence. III. Effects of two different degrees of pelvic floor muscle exercises. Neurourol Urodyn 9:489–502
Haskell WL (1994) Dose-response issues from a biological perspective. In: Bouchard C, Shephard RJ, Stephens T (eds) Physical activity, fitness, and health. Human Kinetics Publishers, Champaign, pp 1030–1039
Braekken IH, Majida M, Engh ME et al (2010) Morphological changes after pelvic floor muscle training measured by 3-dimensional ultrasonography: a randomized controlled trial. Obstet Gynecol 115:317–324
Fleck SJ, Kraemer WJ (2004) Designing resistance training programs, 3rd edn. Human Kinetics Publishers, Champaign
Kraemer WJ, Ratamess NA (2004) Fundamentals of resistance training: progression and exercise prescription. Med Sci Sports Exerc 36:674–688
Author information
Authors and Affiliations
Contributions
IS: Protocol/project development, Data analysis, Manuscript writing/editing. SS: Data collection or management, Data analysis. MM: Data collection or management. FN: Data collection or management. RM: Protocol/project development. DC: Protocol/project development.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Rights and permissions
About this article

Cite this article
Soave, I., Scarani, S., Mallozzi, M. et al. Pelvic floor muscle training for prevention and treatment of urinary incontinence during pregnancy and after childbirth and its effect on urinary system and supportive structures assessed by objective measurement techniques. Arch Gynecol Obstet 299, 609–623 (2019). https://doi.org/10.1007/s00404-018-5036-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00404-018-5036-6